
Abstract
Objective
The study aimed to develop and validate messages for a mobile phone text-based intervention to enhance human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) risk reduction among long-distance truckers (LDTs) in Kenya.
Methods and methodology
Initially, key facts and updates on HIV/AIDS risk reduction were extracted from existing guidelines and packaged into short messages targeted for LDTs. Subsequently, a panel of interdisciplinary experts was purposively sampled and invited through individual emails to participate in the e-Delphi exercise. The study involved three phases: formative research, intervention development, and content validation. Two rounds of the e-Delphi exercise were conducted. A consensus threshold of above 75% was adopted. A Fleiss’ kappa (K) statistic was computed to assess the interrater reliability levels in each round of the e-Delphi exercise.
Results
Most experts were of Kenyan citizenship, 21 (88%), except for one Ugandan and two South Africans. A total of 56 items were rated by 24 experts in round one. Out of the 56 items rated in round one, 50 achieved a consensus above 75%. Based on feedback from specific experts in round one, six items were amended, and an extra one was formulated. In round two, seven items were rated. The seven items achieved a consensus level of 98.21%, meaning a third round was unnecessary.
Conclusion
Given the multi-dimensional inputs from the interdisciplinary panel of experts, the text-based intervention is considered a valid tool for promoting HIV/AIDS risk reduction among LDTs. Considering the substantive approval of the intervention from the panel of experts, a short message service-based digital delivery platform will be used in the implementation phase. We recommend regular updates of the intervention, as the evidence is expected to grow and evolve further.
Introduction
Currently, sub-Saharan Africa is witnessing a steep decline in new human immunodeficiency virus (HIV) infections, according to the most recent Joint United Nations Programme on HIV/AIDS (UNAIDS) report. 1 However, evidence shows this outcome may not be true in certain key population groups. 1 One such population is the long-distance truckers (LDTs). Briefly, LDTs are understood to be among the populations that continue to face chronic neglect from HIV prevention programmes in the region. In addition, LDTs exhibit high-risk sexual networks with female sex workers (FSWs), whose risk of HIV is also high.2,3 Besides, LDTs’ irregular work schedules often do not align with the routine operating hours of most mainstream healthcare facilities along their transit routes. 4 Therefore, over time, LDTs have become hard to reach with essential HIV/acquired immunodeficiency syndrome (AIDS) risk reduction services such as HIV testing, sexually transmitted infection (STI) screening and treatment, and pre-exposure prophylaxis (PrEP), among others. Consequently, an HIV burden of 14.34%, almost five times that of the general population, has been reported among LDTs in the region. 5
With the critical need for the HIV/AIDS risk reduction interventions targeted for LDTs in mind, it is crucial to understand how best healthcare providers can develop and implement them. As such, there have been substantial recommendations for consistent HIV/AIDS risk reduction interventions delivered through mobile phone platforms to hard-to-reach mobile populations like the LDTs.6–8 However, due to an overburdened and underfunded healthcare system, adopting such interventions among the LDTs in most sub-Saharan African countries, including Kenya, has been suboptimal. Indeed, more recently, mobile phone-based text messaging education was recommended to correct existing misconceptions, misunderstandings, and negative attitudes towards HIV/AIDS risk reduction among LDTs using the Northern Corridor Highway in Kenya. 9
Risk reduction messages on HIV/AIDS are evidence-based facts made to guide the prevention of new infections.1,10 The body of evidence on HIV/AIDS prevention is constantly evolving. For instance, more recent approaches such as PrEP and U=U (undetectable viral load = untransmissible HIV infection) are among the latest risk reduction strategies that the UNAIDS is strongly advocating for. 1 Therefore, the most recent guidelines and experts should be consulted when developing HIV/AIDS risk reduction messages. 11 As such, evidence recommends involving the consumers of the intervention during the development of the risk reduction messages.11–13 That way, the researcher can overcome the disconnect that may occur when the consumers of the intervention are not involved, most likely leading to unacceptability and poor outcomes of the HIV/AIDS risk reduction messages.
As part of the development process of the risk reduction messages, validation has to be done to gauge their suitability and credibility. Previous studies have involved several experts with relevant experience in the area of interest.11–13 This approach helps gather experts’ views, perceptions, and suggestions on improving the intervention messages before they are rolled out to the target population. 14 Previously, experts were invited to physical meetings to offer their views when validating the interventions. 14 However, with the recent emergence of electronic-based technology platforms, researchers prefer using electronic (e-Delphi) techniques to gather expert views during validation. 14 Different from other methods of intervention validation, an e-Delphi technique enables expert anonymity, iterative feedback, and statistical strength in consensus. 15
While text-based messaging offers a promising platform through which LDTs can be remotely reached with HIV/AIDS risk reduction updates, it is still not clear what would be the most suitable content. Therefore, the current study leveraged expert opinions to develop and validate mobile phone text-based messages on HIV/AIDS risk reduction targeting LDTs in Kenya. Subsequently, the validated intervention messages would be implemented through a short message service (SMS)-based digital delivery platform to the LDTs.
Methods and methodology
Study design
The standard Delphi approach informed the study design, with several rounds of expert opinions until a consensus was reached. Unlike the traditional Delphi technique, where experts have had physical meetings to validate a tool, the current study leveraged electronic mail. Here, experts were allowed to rate items’ suitability for HIV/AIDS risk reduction. In addition, experts were asked to share feedback on areas where they felt improvement was needed.
The recommended threshold of 75% median agreement levels in specific items informed the choice of consensus level. 16 However, there appear to be dissenting opinions on the actual consensus levels, and a higher consensus threshold is recommended for quality outcomes. 17 As such, the current study adopted a consensus threshold of above 75% agreement levels.
Study phases
Three phases of the study were implemented between April and June 2024. Details of the study phases are outlined below.
Phase 1: formative research
As part of a larger ongoing study, formative research was conducted to collect qualitative feedback on preferred intervention content and delivery modes from LDTs and healthcare providers. Briefly, the LDTs were directly involved in the in-depth interviews during the formative research in the qualitative arm of the study. Specifically, the qualitative arm was anchored on two questions: (a) what are the existing behaviour change communication strategies for HIV/AIDS risk reduction among LDTs in Kenya? (b) What are the existing barriers to HIV/AIDS risk reduction among LDTs in Kenya? 18 As such, the findings from the qualitative arm, especially on the preferred content and mode of delivery, were essentially a contribution of the LDTs who had directly participated in in-depth interviews. Indeed, the findings from the formative research would later inform the number of items across various categories of the HIV/AIDS risk reduction as well as a mobile phone platform, given the tight work schedules and constant mobility nature of LDTs. Besides, the formative research also involved a systematic review and meta-analysis of HIV/AIDS risk reduction interventions targeted for LDTs. 19 The findings from the systematic review and meta-analysis strongly supported mobile phone text-based approaches in remotely reaching the hard-to-reach LDTs with HIV/AIDS risk reduction messages. 19
Phase 2: developing the intervention
The researcher assembled several guidelines and training manuals on various HIV/AIDS risk reduction themes to formulate targeted text-based items for the LDTs. The guidelines included PrEP, post-exposure (PEP), HIV testing, antiretroviral therapy (ART) treatment and care, STI screening and treatment, and the Kenya National Key Population manual.20–22 Subsequently, seven items were developed on PrEP, six on HIV testing, 12 on ART treatment and care, 15 on PrEP, seven on PEP, and lastly, 10 on STI screening and treatment, making a total of 57.
A Swahili version of the 57 items was created using standard translation tools. Besides, a native Swahili speaker with formal linguistic and public communication training in Kiswahili was engaged to enhance the accuracy of the Swahili version of the 57 items. Subsequently, a separate bilingual speaker was engaged to back-translate the Swahili version in English to ensure the validity of the translated items. Besides, a male peer educator familiar with healthcare needs for LDTs assessed the items to ensure the language used was non-stigmatizing and culturally appropriate.
Phase 3: content validation
The third phase involved validating the initially developed 56 items and adding a new one using an e-Delphi exercise. The exercise was undertaken in two rounds. A summary of the three phases is given in Figure 1.
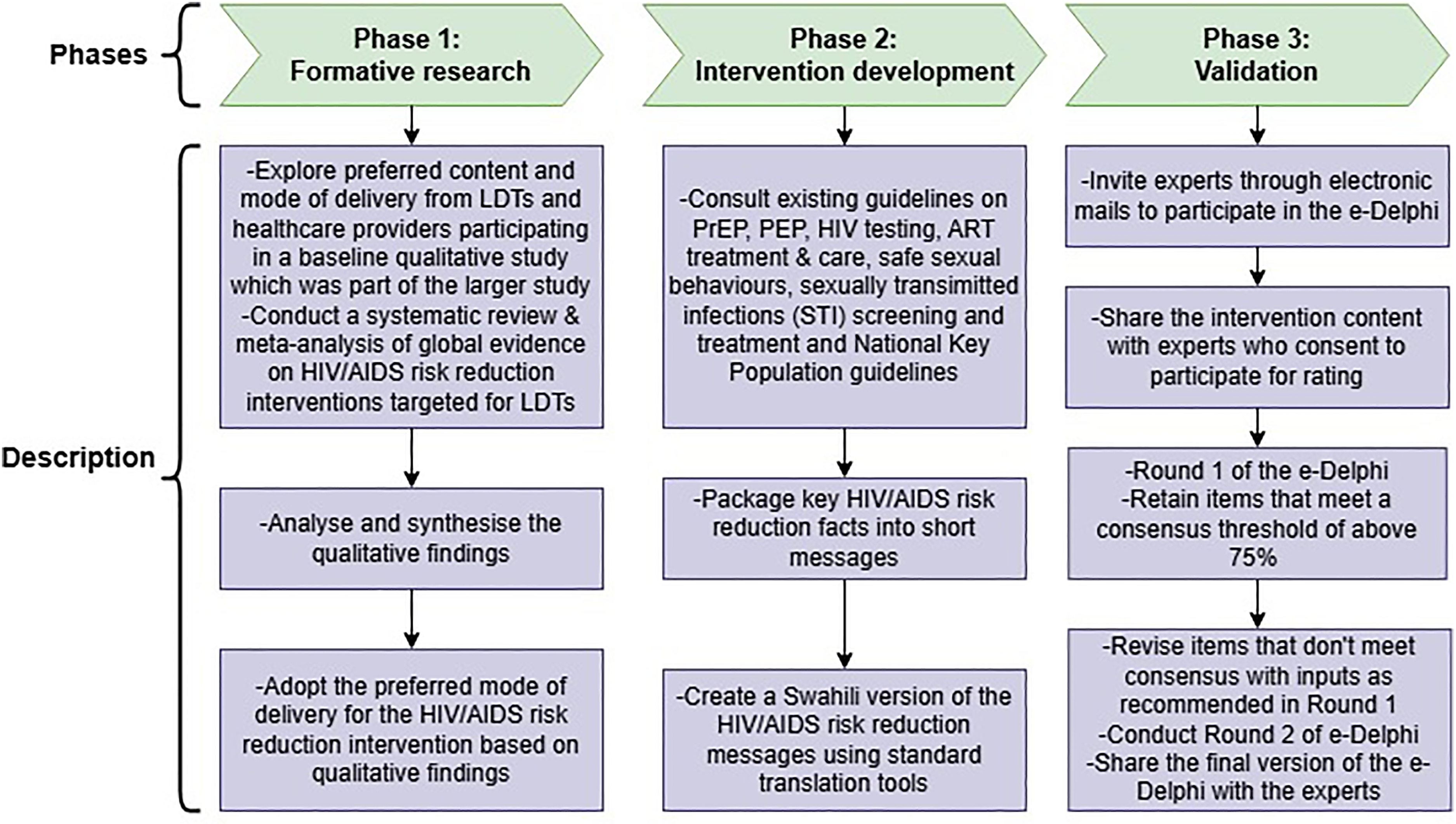
Summary of the three study phases.
Study participants
A total of 35 experts were purposively sampled based on their experience in HIV/AIDS risk reduction among key population groups in May 2024. Specifically, the experts had to be researchers or healthcare providers from various sub-Saharan African countries of diverse professional backgrounds. Expectedly, the participants were individuals with a wealth of experience in behavioural intervention research or extensive involvement in HIV/AIDS risk reduction programmes for LDTs. Invitations to participate in the study were sent to the experts through electronic mail (email). Out of the 35 invited experts, 24 replied, consenting to participate. Those who did not respond to the invitation emails were left out.
Sample size
Evidence of a universally accepted sample size calculation formula for e-Delphi exercises is limited. 23 As such, a sample size of between 20 and 30 participants is considered adequate in concluding consensus in the e-Delphi rounds. 23 This is so especially when the panel of experts is homogenous and possesses a substantial level of uniformity in their expertise. Therefore, a sample size of 24 was purposively deemed suitable for the study, considering that the panel of experts was relatively homogenous and were all healthcare professionals in HIV/AIDS prevention for LDTs.
Eligibility criteria
For potential inclusion in the panel of experts, one had to: (a) be a healthcare provider of HIV/AIDS risk reduction services to LDTs or other key population groups; (b) be a researcher with evidence of published work on HIV/AIDS prevention among LDTs or other closely related key population groups such as FSWs; (c) access to an email account; and (d) consent to participate. Providers of semi-skilled services, such as peer educators who distribute condoms to LDTs and had no formal training in clinical sciences, were excluded.
Participation and informed consent
Generally, the panel of experts involved researchers or healthcare providers drawn from non-governmental organization-based and Ministry of Health, Kenya health facilities. The researchers, who were predominantly the first authors of open-source publications on HIV/AIDS studies among LDTs, and their contact email addresses were selected. Subsequently, an initial email was sent to them containing an electronic version of the informed consent in the form of a Google form link. At this point, only a brief highlight of the study was given, requesting to return the electronically signed informed consent form if they were willing to participate. On the other hand, the healthcare providers were conveniently sampled physically or through phone calls during the formative research phase to share their emails, through which an electronic version of the informed consent would be shared with them. After all participants had given informed consent, the iterative rounds of the e-Delphi exercise were started. The informed consent form used in this study is provided in Supplemental File 1.
Procedures
In round one, an electronic version of the tool, a brief description of the study, and instructions on how to complete it were sent as a Google form link to individual experts. Specifically, experts were required to rate the items based on clarity, relevance, coherence, and sufficiency in HIV/AIDS risk reduction. A Yes option indicated a positive rating, whereas a No option indicated a negative rating. A Yes option was scored with one, and a No option with zero. In addition, experts had the opportunity to share feedback on areas they felt needed improvement.
After round 1, the researcher made the necessary adjustments to items that had not met the required threshold as guided by experts. Subsequently, round 2 followed, allowing the experts to rate the amended items further and offer feedback on areas that needed necessary adjustments. The recommended criterion (all items must have achieved a percentage of agreement above 75) for closing the e-Delphi in round 2 was considered. 16
Statistical analysis
The researcher computed overall percentage agreement levels based on the experts’ ratings of the specific items. Further, to assess the interrater reliability levels in each round of the e-Delphi exercise, a Fleiss’ kappa (K) statistic was computed. 24 Here, a Fleiss’ K of <0.00 indicated poor agreement, 0.00–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement, and 0.81–1.0 perfect agreement. A p-value below 0.05 depicted significance in the Fleiss’ K agreement levels.
Design and digital implementation plan for the mobile phone text-based intervention
Several prerequisites had to be implemented to secure a digital platform through which the validated intervention would be delivered to the end-users (LDTs). Initially, the researcher registered a digital text messaging platform called TD_Educator (meaning truck driver educator) with a bulk messaging company called Text.SMS. 25 Briefly, the digital text messaging platform falls under the first taxonomy (digital health interventions for persons) of the World Health Organization classification of digital interventions in health. 26 The intervention is further sub-classified under the first category, targeted communications to persons. 26
Subsequently, the digital text messaging platform (TD_Educator) was formally registered with the Government of Kenya and authorized to share the messages with the LDTs. The bulk text messaging platform (TD_Educator) would enable the archiving and scheduling of the messages for sending at a later time. The TD_Educator platform was set in such a way that scheduled messages would be sent on Mondays, Wednesdays, and Fridays of every week. Considering the varying length of the intervention items and the total number (57 unique messages), it was envisaged that the messages would be shared for at least 24 weeks. One message (English version) would be sent at 7 a.m. and the other (Swahili version) at 5 p.m. on the three select days of the week. The weekly messages would only be sent once without being repeated at a later date. This timing was based on the feedback gathered from LDTs at formative research, which indicated that this was the best time for them to read and comprehend the messages uninterrupted amidst their busy schedule. The bulk message application and registration certificates are given in Supplemental File 2.
Results
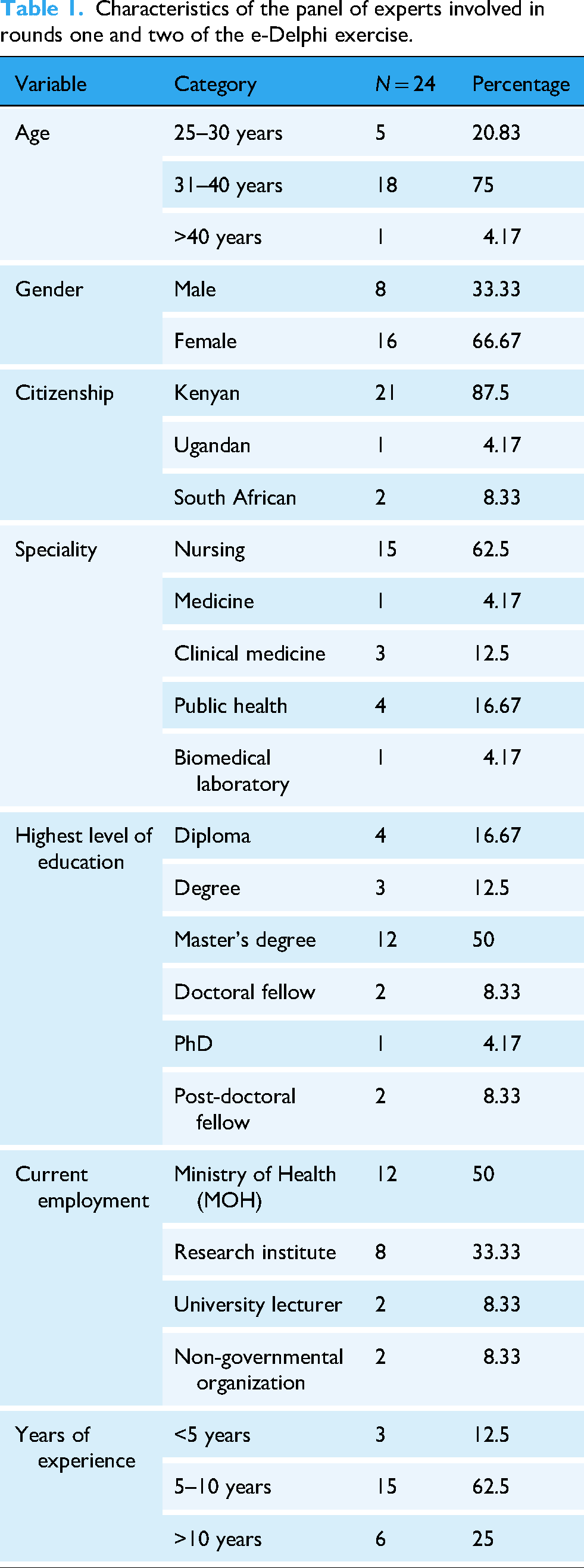
Characteristics of the panel of experts who participated in the e-Delphi exercise
A total of 24 experts took part in rounds one and two of the e-Delphi technique. Most participants were of Kenyan citizenship, 21 (88%), except for one Ugandan and two South Africans. Most of the experts were of the female gender, 16 (66.67%); were aged between 31 and 40 years, 18 (75%); had a background in nursing, 15 (62.5%); and had work experience between 5 and 10 years, 15 (62.5%). Half the experts worked at various HIV/AIDS service delivery units at the Ministry of Health. A detailed summary of the experts’ characteristics is given in Table 1.
Characteristics of the panel of experts involved in rounds one and two of the e-Delphi exercise.
Round one of the e-Delphi exercise
A total of 56 intervention items were rated by 24 experts in round one. The items were spread across various HIV/AIDS risk reduction themes. The themes included sexual behaviours (condom use, sexual partner reduction, and alcohol/substance use), HIV testing, PrEP, PEP, ART care, and STIs. Almost a quarter of the intervention items were on PrEP, 14 (25%), and the least was on HIV testing, 6 (10.71%). The items on HIV testing had the highest level of consensus at 98.61%, followed by STIs at 98.33% and PrEP coming last at 89.58%. In all sections of the intervention items, at least one item did not meet the set criteria of above 75% consensus, except for HIV testing and STIs. Out of the 56 messages, six had a consensus of 75% and below, meaning substantial changes and a second round of validation were needed. Almost all the other 50 intervention items were retained in content, except for a few minor grammatical changes. Based on experts’ recommendations, an extra item on PrEP was developed and taken for validation in round two, together with the initial six that had not met the set consensus in round one. Overall, the consensus was 93.82% in round one. Furthermore, a Fleiss’ K of 0.41, p = 0.001 indicated moderate agreement among the experts in round one. A summary of the e-Delphi outcome of round one is given in Table 2.
Round one of the e-Delphi exercise.

Revisions made to specific items based on expert recommendations
Specific intervention items were revised based on expert recommendations. A summary of the items in their initial format and after revision is given in Table 3.
Summary of the items revised based on expert recommendations.

Round two of the e-Delphi exercise
Round two involved rating the above seven intervention items from the panel of 24 experts. All intervention items attained a 100% consensus except for three, which was 95.8%. Overall, a consensus of 98.21% was achieved in round 2, indicating that a consensus was reached and a third round was unnecessary. Also, a Fleiss’ K of 0.62, p = 0.005 was attained, affirming substantial interrater agreement levels. Eventually, the final intervention content was shared with the experts. However, a response was unnecessary, given that they had already rated all the items above the required threshold of 75% in rounds one and two. A summary of the outcomes of the round two e-Delphi exercise is given in Table 4. A list of the initial draft and the 57 validated items in both English and Swahili versions is given in Supplemental File 3.
Round two of the e-Delphi exercise.

Discussion
Generally, 57 items on HIV/AIDS risk reduction were rated, attaining consensus based on the set threshold of above 75%. Besides, the expert qualitative inputs were critical in enhancing the content of the risk reduction text messages. This outcome indicates that the intervention's content is valid based on expert judgement. Furthermore, this is evidence that the intervention package was relevant in addressing key HIV/AIDS risk reduction areas in the target population. Notably, the intervention aligns with the recent UNAIDS call to reach vulnerable and hard-to-reach populations with more current and up-to-date risk reduction messages. 1 The goal is to promote optimal uptake of HIV/AIDS risk reduction services such as PrEP among LDTs.
The choice of an electronic platform for the Delphi exercise is understood to have enhanced the efficiency of the whole process. The rapid growth of internet use among healthcare professionals in recent years has significantly promoted electronic platforms for information sharing, such as emails. 14 As a result, this approach possibly enhanced the efficiency of the exercise while enabling multi-dimensional inputs from experts of diverse backgrounds. Indeed, the validation exercise attracted 24 multi-national experts with distinct backgrounds in various health disciplines. Agreeably, this is a considerable level of multi-disciplinary inclusivity of experts. Evidence shows that multi-disciplinary inclusivity is critical in e-Delphi exercises.14,27 Arguably, this level of inclusivity shows that the issues addressed in the intervention are of priority importance in promoting HIV/AIDS risk reduction among LDTs. As such, the intervention can be adopted to enhance HIV/AIDS risk reduction across diverse populations of LDTs in the region.
On the contrary, although 24 experts participated in this study, most of them (88%) were from Kenya. The concentration of the panel of experts from a particular country may introduce a key limitation in geographical diversity, which may affect contextual interpretations of the findings. 28 Agreeably, while Kenya shares various epidemiological similarities with other countries in the region, the insights generated by the experts may not fully capture the heterogeneity of experiences and implementation challenges across board. 28 As such, future studies should engage a more geographically diverse panel of experts to broaden the generalizability of findings.
The peers held varied consensus levels across different categories of the HIV/AIDS risk reduction items. For instance, the highest consensus levels were on HIV testing items at 98.61% and the lowest on PrEP items at 89.58% in round one. Understandably, the phase at which peers acquire current updates on HIV/AIDS risk reduction may vary, depending on one's level of education and profession, among many other factors. It can be argued that evidence on HIV testing may not be rapidly evolving as compared to the more recent PrEP. 22 Since the introduction of PrEP, more and more updates have surfaced. This assertion is corroborated by the opinions received from specific experts that the researcher needed to consult more current guidelines on PrEP. Agreeably, while the researcher had used the pre-existing guidelines when developing the formative text messages, more updates were already in place, barely 2 months before the validation exercise had begun. As a result, experts may achieve considerably lower consensus levels in the more rapidly evolving areas, such as PrEP, than in HIV testing.27,29 Also, given this outcome, we opine the need for regular updates to this intervention from time to time as the evidence is expected to grow and evolve further. 27 Equally important, similar updates are also needed for healthcare providers to keep them in touch with the current evidence on HIV/AIDS risk reduction.
The experts found it convincing to have more HIV/AIDS risk reduction items in certain areas, such as PrEP. The use of PrEP in the prevention of HIV infections is a relatively new area. While this approach has proven success rates of almost 100%, much about it is unknown among vulnerable populations like LDTs.9,30 Therefore, the researcher developed most of the items on PrEP with the presumption that LDTs had no pre-existing knowledge in that specific area. Indeed, one expert recommended adding an extra item on PrEP, highlighting the emphasis carried by the items in that category.
The experts agreeing on packaging the intervention as an SMS delivered through mobile phone platforms underscores its relevance as the most suitable mode of delivery to the hard-to-reach LDTs.8,9 The choice of the mobile platform was also informed by feedback from LDTs in the formative qualitative phase of a larger study as their preferred mode of delivery. Mobile phone platforms have proven efficient in remotely reaching hard-to-reach populations such as LDTs with HIV/AIDS risk reduction messages.9,31 Furthermore, mobile phone platforms are known to enhance confidentiality and privacy on HIV/AIDS risk reduction messages among hard-to-reach populations while at the same time creating demand for existing services such as PrEP, PEP, and HIV testing, among many others. Eventually, these efforts will contribute to the collective UNAIDS goal of ending new HIV infections and AIDS by 2030.
Notably, while this study focuses on content development and validation, this may not guarantee the success of the intervention. The ultimate success primarily depends on the acceptability of the HIV/AIDS risk reduction messages to the LDTs. Therefore, plans include pre-testing the messages for clarity, cultural relevance, and resonance. Thereafter, an implementation, followed by evaluation of the messages will be done to ensure that the intervention is not only informed by evidence but also contextually appropriate.
Lastly, the e-Delphi exercise involved only two rounds of expert engagement. In contrast, other studies have reported three rounds of the e-Delphi exercise, where the last round involves sharing the final content of the validation exercise.14,32 Nonetheless, while we still had the last step of sharing the final content with the experts, we did not find it fitting the definitions of an e-Delphi round, where rating and further consensus are needed.
Strengths and limitations
The involvement of multi-disciplinary experts in the e-Delphi exercise is considered a strength, given their multi-dimensional inputs, which enhanced the credibility of the intervention. It is also understood that consulting widely on resource materials such as existing guidelines and training manuals for developing the risk reduction text messages enhanced the quality of the intervention. However, given the constantly evolving evidence on specific aspects of HIV prevention, such as PrEP, the validity of the intervention may weaken over time, needing extensive revisions in the future.
Conclusions
The text-based intervention is considered a valid tool for promoting HIV/AIDS risk reduction among LDTs. The validation exercise attracted immense support from key experts, emphasizing the critical role of HIV/AIDS risk reduction messages for the vulnerable and hard-to-reach LDTs. Given the substantive approval of the intervention items from the panel of experts, an SMS-based delivery platform will be used in the implementation phase. For future studies, we recommend regularly consulting the most current updates during the development of similar interventions, as the evidence is expected to grow and evolve further.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251353287 - Supplemental material for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique
Supplemental material, sj-docx-1-dhj-10.1177_20552076251353287 for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique by Cyrus Mutie, Kawira Kithuci, John Gachohi and Grace Mbuthia in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251353287 - Supplemental material for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique
Supplemental material, sj-docx-2-dhj-10.1177_20552076251353287 for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique by Cyrus Mutie, Kawira Kithuci, John Gachohi and Grace Mbuthia in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251353287 - Supplemental material for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique
Supplemental material, sj-docx-3-dhj-10.1177_20552076251353287 for A mobile phone text-based intervention to enhance HIV/AIDS risk reduction among long-distance truckers in Kenya: Development and validation using an e-Delphi technique by Cyrus Mutie, Kawira Kithuci, John Gachohi and Grace Mbuthia in DIGITAL HEALTH
Footnotes
Acknowledgement
We are grateful for the multi-disciplinary panel of experts for their support and collaboration during e-Delphi exercise.
Ethical considerations
Ethical approval was granted by the ethical review committee of Jomo Kenyatta University of Agriculture and Technology (JKUAT), JKU/ISERC/02317/1256. The study was also licensed by the National Commission for Science, Technology, and Innovation, Kenya (NACOSTI), NACOSTI/P/24/33837. More approvals were obtained from Busia (ADM 15/27 Vol.1/151) and Kajiado (KJD/CC/ADM/45 VOL.V (4)) counties in Kenya.
Consent for publication
All information used in the development of the manuscript is fully anonymized and does not contain any identifying details of study participants. Therefore, publication consent was not applicable.
Author contributions
CM conceived the study and methodology, performed administration, data collection, software, and analysis, and wrote the original draft. KK, JG, and GM conceived the study and methodology, supervised the study, and writing and reviewing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets and other relevant material used in the development of the current study findings are available upon request from the corresponding author.
Guarantor
CM.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.