
Abstract
Background
While mobile (m)-health interventions offer a promising platform through which the vulnerable long-distance truckers (LDTs) can be remotely reached with current human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) risk reduction updates, their use is limited in Kenya.
Objective
The study aimed to establish the effect of a short message service (SMS)-based mHealth intervention in enhancing HIV/AIDS risk reduction among LDTs in Kenya.
Methods and Methodology
This was a pre-posttest quasi-experimental study involving a control site (Namanga) and an intervention site (Busia), each comprising 189 LDTs. At baseline, a pre-test was done to assess existing HIV/AIDS risk levels. In Phase 2, an SMS-based mHealth intervention comprising 57 items was developed and implemented using a digital platform (TD_Educator) over a six-month period. Eventually, a post-test was conducted to evaluate the effect of the intervention. A two-proportion Z-test and a Cochran-Armitage test were used to compare the proportions of HIV/AIDS risk levels between the two study arms, utilising the R statistical software. A Cramér's V test was also used to calculate the effect size of the intervention.
Results
Slightly more than half, 202 (53.44%) of the LDTs were at moderate HIV/AIDS risk levels, 106 (28.04%) at high-risk levels, and 70 (18.52%) at low-risk levels at baseline. Post-intervention, statistically significant (χ2 = 72.25, df = 1, p < 0.001) higher proportions (50.62%) of low HIV/AIDS risk levels were observed in the intervention arm (Busia), an indication of a shift from high to lower risk levels following the BCC intervention, unlike the control arm (χ2 = 0.84, df = 2, p = 0.657). Overall, the intervention had a moderate effect, with a Cramér's V of 0.3 (χ² = 28.214, df = 2, p < 0.001), in enhancing HIV/AIDS risk reduction.
Conclusion
The mHealth intervention is considered effective in enhancing HIV/AIDS risk reduction among LDTs, albeit needing regular updates in the future, as the evidence is expected to grow and evolve further.
Introduction
The adoption of risk reduction approaches such as anti-retroviral therapy (ART) and pre-exposure prophylaxis (PrEP) in the course of the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) pandemic has markedly enabled a dramatic reduction of HIV incidence in many sub-Saharan African (SSA) countries. 1 For the first time in the history of the HIV/AIDS pandemic, more new infections are occurring outside SSA. 1 These outcomes signal an array of hope that the region is on the right track toward meeting the ambitious Joint United Nations Programme on HIV/AIDS (UNAIDS) goal of ending new HIV infections and AIDS by 2030.1,2 Nonetheless, the most recent UNAIDS report highlights that the current decline in new HIV infections may not be sufficient enough to end AIDS as a public health threat by 2030.3,4 This is partly due to the recent disruptions witnessed in HIV/AIDS donor funding for developing nations.3,4 Also, the continued disproportionate burden of HIV among certain key population groups, such as long-distance truckers (LDTs) in Kenya and other SSA countries, poses a potential challenge to the progress made so far in curbing new infections. 5 For instance, recent evidence indicates that the HIV prevalence among LDTs is 14.34% in SSA, multiplefold compared to that of the general population. 5
Briefly, LDTs in Kenya face a myriad of factors that uniquely predispose them to higher risk levels of HIV/AIDS compared to other migrant populations.6–8 Firstly, LDTs’ trucking career is often marred by high-risk sexual networks. Notably, the sexual networks are characterised by an abundance of female sex workers (FSWs) and high-risk sexual behaviours like inconsistent use of condoms.9–11 Besides, LDTs face chronic neglect from mainstream healthcare facilities, with most transit routes lacking targeted HIV/AIDS risk reduction services for them.12,13 Also, tight work schedules and strict deadlines often leave LDTs with little or no time to attend to their healthcare needs. 13 As such, LDTs are very difficult to reach with consistent risk reduction messages. 14 Understandably, they may often miss the much-needed regular updates of the current HIV/AIDS risk reduction strategies, such as PrEP. 13 Altogether, this multitude of factors has continuously fuelled new HIV infections among LDTs and their sexual partners. Therefore, it is increasingly important to better understand how the LDTs’ risk of HIV/AIDS can be alleviated with a specific emphasis on risk reduction interventions.
In Kenya, HIV/AIDS risk reduction interventions targeting LDTs are predominantly donor-funded and implemented through Non-Governmental Organisations (NGOs) such as the North Star Alliance. 8 However, the recent freeze on US foreign aid programmes, such as PEPFAR and USAID, has brought many of the NGO-driven initiatives to the brink of collapse. 3 Without urgent intervention, the significant gains made so far in control of HIV/AIDS in key populations such as LDTs may be reversed. 3 Therefore, alternative approaches to HIV/AIDS risk reduction that are cost-effective and user-friendly have increasingly become indispensable. One such approach is the short message service (SMS)-based mobile health (mHealth) interventions. 15
mHealth interventions refer to health-related initiatives that utilise mobile phones, smartphones, and other digital devices, such as tablets, to support medical and public health services remotely.15,16 Such interventions encompass a wide range of activities. These initiatives may include sending SMS-based health education and reminders for clinic appointments, conducting remote consultations, and supporting medication adherence, among others.16–18 Some mHealth intervention approaches, such as those based on video graphics, may require internet connectivity or additional charges for the end user to benefit from the shared information. On the other hand, SMS-based mHealth interventions relying on basic mobile phone networks may not require a smartphone or an internet connection. Therefore, SMS-based mHealth interventions provide a scalable platform for remotely delivering various HIV/AIDS risk reduction messages to LDTs. Mostly, it is possible to reach LDTs with the messages at any location, provided a cellular network is available and regardless of device type.15,17,19
Over the last decade, there has been a significant increase in mobile phone penetration in most parts of Kenya. It is almost unheard of for an LDT not to own a mobile phone device. Since LDTs rely on mobile phones as their primary means of communication with employers, these devices have become a natural necessity. Through their mobile phones, they can access critical information such as weather updates, security alerts, and documentation for cross-border purposes. Notably, the widespread use of mobile phones among LDTs presents a valuable opportunity for implementing mHealth interventions. 16 Therefore, healthcare professionals can leverage mobile phone platforms to remotely deliver timely and targeted HIV/AIDS risk reduction messages at moments when LDTs are most receptive. 16
The mHealth interventions on HIV/AIDS risk reduction can promote behaviour change while at the same time creating demand for existing services such as PrEP and ART treatment adherence.15,17,18,20 Moreover, mHealth interventions consume less time, are less intrusive, and offer a confidential environment for HIV/AIDS risk reduction among mobile populations such as LDTs.21,22 Indeed, mobile phone platforms have previously enhanced HIV testing among LDTs in Kenya, Zimbabwe, and South Africa.8,19 More recently, mobile phone-based text messaging education has been recommended to correct existing misconceptions and negative attitudes toward HIV/AIDS risk reduction among LDTs in Kenya. 14
Despite the growing discourse on the need to adopt digital-based approaches in HIV/AIDS risk reduction for key populations such as LDTs, critical gaps remain. Previous studies have focused on SMS alerts on free HIV self-test kits, somewhat neglecting other equally important HIV/AIDS risk reduction areas such as PrEP availability, condom use promotion, ART adherence reminders, and linkage to treatment and care for sexually transmitted infections (STIs). 8 Therefore, the present study leveraged an SMS-based mHealth intervention with a broader focus on the HIV/AIDS risk reduction areas mentioned above. As such, the study will inform how a multi-component SMS-based mHealth intervention can be adopted to enhance HIV/AIDS outcomes in vulnerable populations, especially in resource-limited settings. Eventually, the study not only extends the evidence base on digital health interventions but also aligns with the UNAIDS global goal to end new HIV infections and AIDS by 2030. 1
Theoretical framework
The theoretical framework was based on the Information, Motivation, Behavioural Skills (IMB) model, as recommended for HIV/AIDS risk reduction interventions. 23 This is because the theory has information sharing as its pre-requisite construct, which is an element of communication. 23 Information sharing triggers motivation to change risky HIV/AIDS behaviours.24,25 Individuals who are well informed and motivated to change their risky behaviours will eventually gain the behavioural skills to practice and sustain HIV/AIDS risk reduction.24,25 Thus, the IMB model provides a comprehensive guide to understanding behaviour change and is deemed generalisable in formulating interventions for HIV/AIDS risk reduction.24,25 Thus, the IMB model was deemed suitable for guiding this study, as shown in Figure 1.
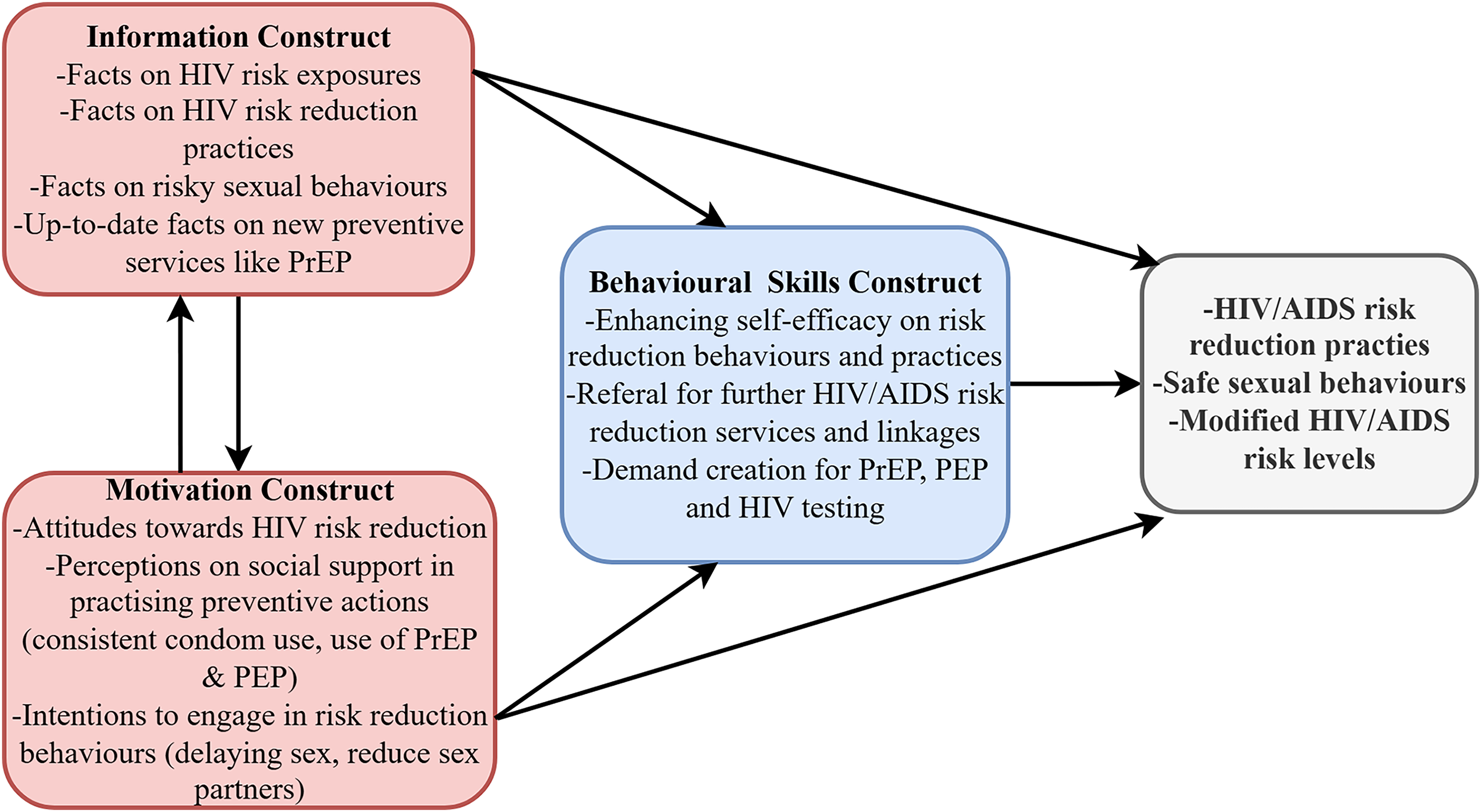
Information, motivation, behavioural skills model.
Objectives
The study sought to establish the effect of a short message service (SMS)-based mHealth intervention in enhancing HIV/AIDS risk reduction among LDTs in Kenya. Initially, it was hypothesised that an SMS-based mHealth intervention had no significant effect on HIV/AIDS risk reduction among LDTs in Kenya.
Methods and methodology
Study design
This study employed a pre-posttest, nonequivalent quasi-experimental design, comprising a control group (Namanga site) and an intervention group (Busia site). Specifically, this was the quantitative arm of a larger concurrent triangulation mixed-methods study, with the qualitative arm's findings published elsewhere.13,26 Moreover, the guidelines for the Transparent Reporting of Evaluations with Non-Randomised Designs (TREND) statement informed the study design. 27 A TREND statement checklist is given in Supplemental Material 1.
Study setting and duration
The study was conducted in both Busia and Namanga border towns in Kenya between March 2024 and January 2025. The two towns serve as key terminal entry and exit points for the interior of Kenya, connecting to the Kenya-Uganda and Kenya-Tanzania international borders, respectively. Given their strategic location at the international border points, the towns serve as key sexual network hotspots for LDTs; hence, they were purposively sampled as the study sites.
Sample
The study population consisted of LDTs who exit or enter Kenya through Busia and Namanga towns at the Kenya-Uganda and Kenya-Tanzania international border points. The study targeted the LDTs who operate along the Northern Corridor Highway in Kenya. The eligibility criteria are outlined below.
Eligibility criteria
The inclusion of the LDTs in the study was based on their ability to read SMSs in either English or Swahili through their mobile phones and their possession of a mobile phone that allowed them to access the SMSs. The study excluded individuals under the age of 18 years and truckers not involved in long-distance trucking. The drivers of vehicles covering short distances were also excluded because they may not have been experiencing the diverse vulnerabilities to HIV/AIDS that come with covering long distances across diverse geographical highway stopovers.
Sample size determination and sampling
The formula for calculating the sample size for two proportions was used as tabulated below
28
:


Initially, a sample size of 135 LDTs per study site was calculated. Furthermore, due to the anticipated high loss to follow-up, the sample size was adjusted by 40%, which translates to 54. Ultimately, the sample size for each site consisted of 189 participants (378 participants in total for both sites). The LDTs were assessed for eligibility as they approached the Busia and Namanga international border points. Precisely, a systematic sampling technique was used based on a predetermined kth value (sampling interval) of 21 for Busia and 11 for the Namanga site. Those who were eligible were briefed on the study details and then asked to sign an informed consent form voluntarily.
Recruitment and allocation of participants
Before the commencement of phase two of the study, the research team set the LDTs’ baseline HIV/AIDS risk levels as the criteria to determine the control and intervention sites. Understandably, the site where LDTs would demonstrate higher risk levels would be selected as the intervention site. Moreover, during the first phase of the study, LDTs were informed that they would be followed up with the mHealth intervention and subsequently undergo a risk assessment after the intervention. Thus, for recruitment, LDTs had to possess a mobile phone through which they could be followed up with the intervention and demonstrate the ability to comprehend text messages in either English or Swahili. Details of how LDTs were allocated across the different study sites are provided below.
Intervention group
The intervention group was allocated to 189 LDTs from the Busia site. The Busia site was purposively sampled based on baseline findings indicating that LDTs from the site experienced a slightly higher risk of HIV/AIDS (though not statistically significant) compared to those from the Namanga site. Therefore, LDTs from the Busia site received the mHealth intervention during the study period.
Control group
The control site consisted of 189 LDTs from the Namanga site. Based on baseline findings, LDTs from this site experienced lower HIV/AIDS risk levels, which is why the site was allocated the control group. Thus, LDTs from this site did not receive the targeted mHealth intervention, but the routine risk reduction services available from healthcare facilities along their transit routes.
Data collection tool and process
A structured, interviewer-administered questionnaire, formulated in accordance with existing guidelines, was used.29–31 More specifically, the questionnaire employed an HIV/AIDS risk assessment tool adapted from the Risk Reduction Assessment, Planning, and Support (RRAPS) manual toolkit and the Denver HIV Risk Score (DHRS) tool.32,33 Briefly, the final questionnaire consisted of three sections: knowledge of HIV/AIDS risk reduction (35 items), sexual behaviour and substance use (11 items), and HIV/AIDS risk reduction practices (15 items). Therefore, the questionnaire comprised a total of 61 items, out of which a composite risk score was computed for each participant at both baseline and post-intervention. The data collection tool is provided in Supplemental Material 2.
Although the original tools (DHRS and RRAPS) from which the current questionnaire was adapted had already been validated, further validation was necessary to ensure relevance to the context of LDTs in Kenya.32–34 Accordingly, the risk assessment tool underwent a validation exercise conducted by a panel of eight experts. Subsequently, the tool was pre-tested among 30 LDTs in Mlolongo town, Machakos, Kenya.
The data collection exercise was carried out by the researcher (principal investigator) and two research assistants. The research assistants had background training in nursing or public health. Before the data collection exercise, the research assistants underwent a two-day training on the data collection tools and the necessary study protocols.
Due to the hard-to-reach nature of the LDTs, the questionnaires were administered by interviewers to facilitate a high response rate. Understandably, self-administered questionnaires may have been difficult to trace, given that the LDTs are on constant mobility over far distances.
Study procedures
The study entailed three distinct phases. The first phase of the study was a baseline study to elicit the barriers to HIV/AIDS risk reduction, 13 existing behaviour change communication strategies, the effectiveness of HIV/AIDS risk reduction interventions (systematic review of global evidence), 35 and LDTs’ HIV/AIDS risk levels from both Namanga and Busia sites. The findings in phase one would later inform the development of a targeted SMS-based mHealth intervention in phase two to promote HIV/AIDS risk reduction among LDTs. 36 The second phase involved the development and validation of an SMS-based mobile health (mHealth) intervention, the details of which are published elsewhere. 36 Briefly, the mHealth intervention entailed 57 SMS items distributed across various HIV/AIDS risk reduction themes such as consistency in condom use, reduced number of sexual partners, the type of sexual partners, uptake of PrEP and PEP, enhanced uptake of HIV testing, STI screening and treatment, and initiation and adherence to ART care. Subsequently, the participants were followed up for 6 months with the SMS-based mHealth intervention. In the last phase, the participants were subjected to a post-test to determine the effect of the mHealth intervention on HIV/AIDS risk reduction.
Digital design and implementation of the SMS-based mHealth intervention
The development of the SMS-based mHealth intervention was guided by the World Health Organisation's (WHO) classification of digital interventions. 37 The WHO guideline provides a structured framework for designing digital interventions, services, and applications to address specific health needs. 37 The SMS-based mHealth intervention falls under the category ‘targeted communication to persons’ (1.1), which involves sharing targeted health education messages to specific groups of people based on their preferences and health needs. 37
Initially, the researcher registered a digital text messaging platform called TD_Educator (meaning “truck driver educator”) with a cloud-based bulk SMS company called Text.SMS. 38 The TD_Educator platform was also formally registered with the Government of Kenya and given an authorisation certificate to share the SMSs with the LDTs. 36 The digital platform enabled the archiving and scheduling of the SMSs for sending at a later time. It was set in such a way that scheduled messages were sent on Mondays, Wednesdays, and Fridays of every week. Considering the varying length of the SMSs and the total number (57 unique SMSs), the SMSs were shared for at least 24 weeks. One SMS (English Version) was sent at 7 a.m. and the other (Swahili version) at 5 p.m. on the three select days of the week. The weekly SMSs were sent only once, without being repeated at a later date. This timing was based on the qualitative feedback gathered from LDTs at baseline, indicating that this was the optimal time for them to read and comprehend the BCC SMSs uninterrupted, given their busy schedules.
The TD_Educator digital platform enabled the sharing of SMSs across multiple mobile phone networks, ensuring a broad reach regardless of the service provider. Additionally, the platform provided a user-controlled opt-out option, allowing LDTs to discontinue messaging and respect their autonomy. Moreover, the platform generated delivery reports, allowing the researcher to track the status of each message and verify if the end user had successfully received it. The mHealth intervention SMS items are provided in Supplemental Material 3.
Data management and analysis
The researcher reviewed the baseline and post-intervention questionnaires to verify completeness and ensure that they were assigned unique serial numbers to prevent duplicate entries. This was followed by creating datasets in MS Excel® for data entry, cleaning, and coding. Subsequently, the datasets were exported to the R statistical software version 4.4.1 for analysis. 39
Initially, individual sample data for all variables in the main dataset were checked for normality using the Shapiro-Wilk test for normal distribution. 40 For continuous numeric variables whose data were normally distributed, means and standard deviations were computed as the corresponding descriptive statistics. On the other hand, for the continuous numeric variables whose data were not normally distributed, medians and interquartile ranges (IQRs) were computed. For categorical variables, summaries were made, and corresponding percentages were computed.
Subsequently, the researcher performed a comparative analysis of all socio-demographic and socio-economic factors for both Intervention (Busia) and Control (Namanga) sites. The goal was to establish whether there were any significant differences between the two sites at baseline. To compare the normally distributed continuous numeric variables at baseline, the independent t-test (a parametric test) was performed. Using the independent t-test function in R statistical software, the test returned a t-value, degree of freedom (df), and a p-value. For continuous numeric variables that were not normally distributed, the Wilcoxon test (a non-parametric test) was used to compare the existence of any difference between the two study groups at baseline. Using the Wilcoxon test function in R, the test returned a Wilcoxon rank value (W) and a p-value. For the categorical variables, the Pearson's chi-square test was used to assess differences between the two study groups. Using Pearson's chi-square test function in R statistical software, a χ2-value, degrees of freedom (df), and a p-value were returned. Where a p-value was < 0.05, a statistically significant difference between the two sets of variables in the two study groups was deemed present in all of the above tests. Additionally, where categorical variables had > 25% of the cell counts with fewer than 5, a Fisher's exact test in R statistical software was used. The test returned a p-value, with an outcome of < 0.05, indicating a statistically significant difference in the observed counts.
Overall risk scores of HIV/AIDS were generated from the domains of knowledge, HIV/AIDS risk reduction practices, and sexual behaviour characteristics. This was done in accordance with the guidelines of the RRAPS HIV risk assessment manual toolkit and the Denver HIV risk assessment tool.32,33 For the knowledge domain, the scores were reverse-coded. This is because the absence of HIV/AIDS risk reduction knowledge enhances vulnerability to HIV infection, whereas its presence has a protective effect. Thus, incorrect scores were assigned a value of one (1) to indicate the presence of some risk, whereas the correct scores were assigned a value of zero (0) as an indication of reduced risk. Knowledge of HIV/AIDS risk reduction was tested on questions framed around the following items, namely condom use, number of sexual partners, alcohol and substance use, HIV testing, PrEP use, PEP use, history of STI, screening and treatment of STIs, linkage and adherence to ART care. A participant responded with a “True” or “False” and scored (incorrect = 1) or (correct = 0).
Similar to the knowledge domain, the HIV/AIDS risk reduction practices were reverse-coded. A participant was asked a yes-or-no question about whether they had performed selected HIV/AIDS risk reduction practices. Where a participant did not perform the respective risk reduction practice, a score of one (1) was given to indicate the presence of some risk. Conversely, a score of zero (0) was given when the participant performed the respective HIV/AIDS risk reduction practice, indicating a reduced risk. The HIV/AIDS risk reduction practices were based on the following items: condom use (consistent condom use = 0 and inconsistent condom use = 1), HIV testing within three months (tested for HIV = 0 and not tested for HIV = 1), PrEP use when on an ongoing risk of HIV infection (uses PrEP = 0 and does not use PrEP = 1), PEP use after a potential exposure to HIV within three days (used PEP = 0, never used PEP = 1), history of STI while on trucking career (no history of STI = 0 and history of STI = 1), screened and treated for STI within 7 days after onset of symptoms (screened and treated for STI = 0, not screened neither treated for STI = 1), linkage to care and adherent to ART care for those who are HIV positive (linked and adherent to ART = 0, not linked or not adherent to ART care = 1).
Unlike the knowledge and HIV/AIDS risk reduction domains, the sexual behaviour characteristics domain was not reverse-coded. This is because the presence of a risky sexual behaviour is an indication of some risk of HIV/AIDS. In contrast, the absence of risky sexual behaviour is an indication of reduced risk. Thus guided by the RRAPS and DHRS risk assessment tools, sexual behaviour characteristics were measured as follows: number of sexual partners (one or no sexual partner = 0 and more than one sexual partner = 1), alcohol and substance use during or before sexual interaction (no alcohol and substance use = 0, uses alcohol and other substances = 1), and frequency of sexual interactions (delays sexual interactions while on transit = 0, engages in multiple sexual interactions while on transit = 1).
Eventually, a composite score was generated from the above three domains to give an overall risk level of HIV/AIDS among the LDTs. The risk levels of HIV/AIDs were categorised into low, moderate, and high risk based on the overall scores from a particular participant, guided by the Denver HIV risk assessment scoring.30–32 These scores have been tested and validated elsewhere and have been shown to categorise patients into the correct risk groups.34,41 According to the DHRS tool, risk scores of below 30% indicate a low risk of HIV, risk scores of 30–39 indicate a moderate risk of HIV, and risk scores of 40 and above indicate a high risk of HIV infection.33,34,41 The risk scores were dummy coded as follows: low risk = 0, moderate risk = 1, and high risk = 2 for analysis.
A comparative analysis was conducted to determine the existence of differences between the risk scores at baseline and post-intervention in both study sites using the two-proportion Z-test function in R. Subsequently, the researcher compared whether there were any statistically significant differences across all risk levels (low, moderate, and high) in both study groups. This analysis was conducted using Pearson's chi-square test function in R. Additionally, a clearer perspective on the risk level differences across the two study sites was visualised using grouped bar plots with error bars in the R statistical software. 39 The error bars were created using 95% confidence intervals (CIs) of the specific risk level proportions. The upper tail of the error bar was based on the upper CI, and vice versa.
To gauge the effectiveness of the intervention on HIV/AIDS risk reduction among LDTs, several tests were conducted. First, the researcher used a two-proportion Z-test to compare the proportion of HIV/AIDS risk scores in the control and intervention groups at baseline and post-intervention. Additionally, a chi-square test of independence was used to determine whether there were statistically significant differences in the overall risk scores (combined) between the control and intervention groups.
Further, the researcher performed the Cochran-Armitage test for trend in proportions to examine the trend in the HIV/AIDS risk levels (low, moderate, and high) across the intervention and control groups post-intervention. 42 The purpose of this test was to detect any shift or linear trend in proportions of HIV/AIDS risk from low-risk to high-risk levels and vice versa. Ideally, the Cochran-Armitage trend test would enable a better understanding of the effect of the mHealth intervention on HIV/AIDS risk reduction among LDTs post-intervention. The test returned a Z-value and a p-value. A positive Z-value would indicate a positive association between exposure to the intervention and HIV/AIDS risk reduction, and vice versa. A p-value of <0.05 would indicate statistical significance in the outcome. The Cochran-Armitage results were visualised using a Mosaic plot from the (ggplot2) and (dplyr) packages in the R statistical software. 39
Ethical considerations
Ethical approval for the study was obtained and approved by the Ethics Review Committee of Jomo Kenyatta University of Agriculture and Technology (JKUAT) (Ref: JKU/ISERC/02317/1256). Written informed consent was obtained from the study participants prior to the commencement of each interview. More precisely, the informed consent detailed the risks and benefits of the study, the voluntary nature of participation, and the participants’ right to withdraw from the study at their discretion. Confidentiality was maintained by observing the anonymity of all study participants during data collection, archiving, and analysis.
Results
Socio-demographic and socio-economic characteristics of study participants at baseline
A total of 378 LDTs from both study sites (189 for each) were recruited. The mean age and standard deviation (SD) of LDTs from the Namanga site were 33.58 (± 8.48) years, and for the Busia site, 41.13 (± 9.00) years. At the Namanga site, slightly more than half of the participants were Tanzanians (99, 52.38%). A vast majority of participants at the Busia site were LDTs of Kenyan origin (161, 85.19%). The median time spent on transit by LDTs was relatively uniform across both study sites: Namanga, 12 (12–15) hours; Busia, 12 (9–15) hours; and both study sites combined, 12 (10–15) hours. A detailed summary of the participant characteristics is given in Table 1.
Baseline characteristics and their comparative analysis outcomes among LDTs.

M ± SD: mean ± standard deviation; Mdn (IQR): median (interquartile range); LDTs: long-distance truckers; USD: US Dollars.
Comparative analysis for baseline characteristics
It emerged that there was no statistically significant difference in most of the independent variables between the two study sites. Nonetheless, statistically significant differences were found for age, citizenship, years of experience, hours spent on transit, hours spent on rest, and days spent away from family/spouse across the two study sites. For age, there was a statistically significant difference between the Namanga and Busia sites, as indicated by the independent t-test (t = −8.40; df = 376; p < 0.0001). A p-value of < 0.0001 suggested that the distribution of citizenship significantly varied between the two study sites. Based on a Wilcoxon rank test, there was a statistically significant difference among LDTs from both sites regarding their duration of experience in years (W = 10,314; p < 0.0001), hours spent on transit (W = 21,807; p = 0.001), and hours spent on rest (W = 12,428; p < 0.0001). An independent t-test also revealed a statistically significant difference in the number of days spent off duty in a week (t = −2.07; df = 376; p = 0.038). A summary of the comparative analysis of baseline characteristics from both study sites is presented in Table 1.
Risk levels of HIV/AIDS among long-distance truckers at baseline
The proportion of LDTs at low-risk levels (< 30%) of HIV/AIDS in the Namanga site was 49 (25.93%), almost twice that of LDTs in the same risk category from the Busia site, 21 (11.11%). At both sites, approximately half of the LDTs had moderate risk levels (30%–39%), with a slightly higher proportion in Busia 106 (56.09%) compared to Namanga 96 (50.79%). The LDTs at high-risk levels (≥ 40%) in Busia were higher at 62 (32.80%) compared to those of the same risk category in Namanga, at 44 (23.28%). Generally, on combining both study sites, slightly above half of the LDTs were at moderate HIV/AIDS risk levels 202 (53.44%), followed by those at high-risk levels 106 (28.04%), and lastly, those at low-risk levels 70 (18.52%).
Upon performing a two-proportion z-test, it was found that there was only a statistically significant difference in the proportion of LDTs at low-risk levels between the two sites. At the Namanga site, the proportion of LDTs at low-risk levels was significantly lower compared to those in the same category from the Busia site (χ² = 12.78; df = 1; p = 0.0004). There was no statistically significant difference in the proportion of LDTs at high-risk levels in both study sites (χ2 = 3.78; df = 1; p = 0.051), same to moderate risk level (χ2 = 0.86, df = 1; p = 0.353). Overall, there was no statistically significant difference in the proportion of LDTs in all risk levels (χ2 = 1.68; df = 4; p = 0.793), Table 2.
Risk levels of HIV/AIDS among LDTs in both study sites at baseline.

HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome; LDTs: long-distance truckers.
Outputs of the mobile phone-based text messaging (TD_Educator) platform
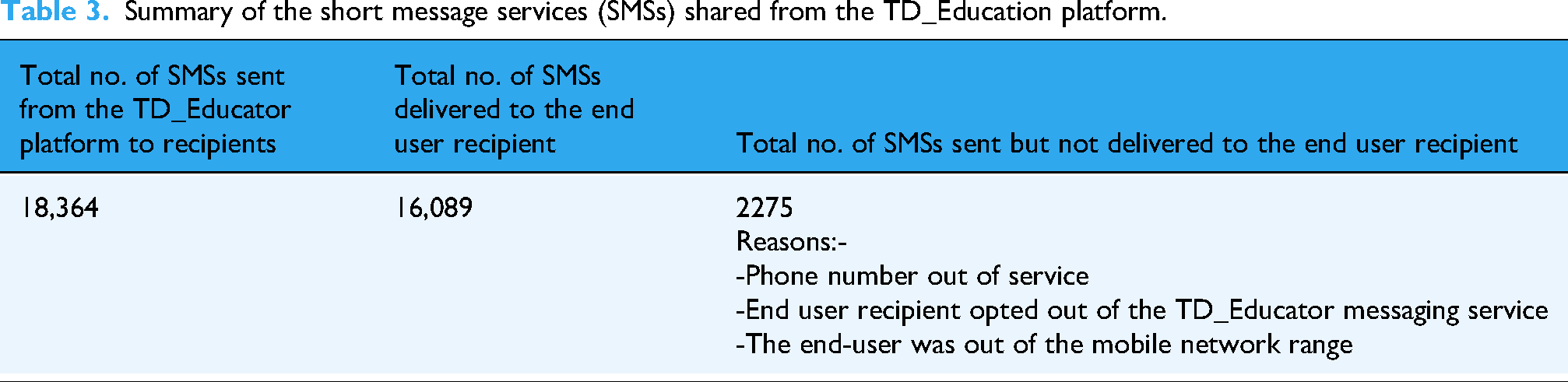
Overall, 18,364 SMSs were shared from the TD_Educator platform to the 189 LDTs in the intervention group for 24 weeks (6 months) between June and December 2024. Half (9182) of the SMSs were in the English language, while the rest were in Swahili. Out of the total SMSs shared from the TD_Educator platform, 2275 SMSs were not successfully delivered to the end user recipient. Several factors may have contributed to the undelivered SMSs. First, some of the recipients’ phone numbers may no longer have been in service. Additionally, the limited network range at the end user's location at the time of sending the SMSs may have hindered their delivery. Lastly, the end users may have opted out of the TD_Educator platform (given that the platform allowed for opting out). A summary of the number of SMSs from the TD_Educator platform is given in Table 3.
Summary of the short message services (SMSs) shared from the TD_Education platform.
Loss to follow-up and response rate post-intervention
Overall, 65 (17.2%) LDTs were lost to follow-up in both study arms. The loss-to-loss rate was highest in the control group at 38 (20.1%) and lowest in the intervention arm at 27 (14.3%). Therefore, post-intervention, the response rate was 82.8% for both study arms combined, 79.9% for the control group, and 85.7% for the intervention group. A study flow diagram is given in Figure 2.

Study flow diagram.
A comparison of the HIV/AIDS risk levels at baseline and post-intervention
There were no statistically significant (χ2 = 0.84, df = 2, p = 0.657) differences in the risk levels of HIV/AIDS among LDTs in the control group (Namanga) at baseline and post-intervention. In contrast, on comparing the HIV/AIDS risk levels for the intervention group (Busia), statistically significant (χ2 = 67.07, df = 2, p < 0.001) differences were observed between baseline and post-intervention. Specifically, statistically significant (χ² = 72.25, df = 1, p < 0.001) higher proportions (50.62%) of low HIV/AIDS risk levels were observed post-intervention compared to baseline, where the low-risk levels were at 11.11%. Conversely, the proportions of moderate and high-risk levels were significantly lower at the post-intervention stage compared to the baseline. The outcome is an indication of a shift from high to lower HIV/AIDS risk levels following the mHealth intervention. Similarly, when comparing the overall risk levels for both study sites, statistically significant differences were observed (χ² = 29.50, df = 2, p < 0.001), with a statistically significant shift from high to lower risk levels. A summary of the risk levels in both study arms is presented in Figures 3 and 4, as well as in Table 4.

Bar plots and error bars showing the risk levels of HIV/AIDS among LDTs in the intervention group (Busia) at baseline and after 6 months follow-up.

Bar plots and error bars showing the risk levels of HIV/AIDS among LDTs in the control group (Namanga) at baseline and post-intervention.
A comparison of the risk levels of HIV/AIDS among LDTs in control and intervention groups at baseline and post-intervention.

HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome; LDTs: long-distance truckers.
Two-proportion Z test examined within-arm risk category differences.
Pearson's chi-square test examined overall risk category differences in each study arm.
Effect of the SMS-based mHealth intervention on HIV/AIDS risk reduction among LDTs
Cochran-Armitage (CA) trend test for proportions in HIV/AIDS risk levels
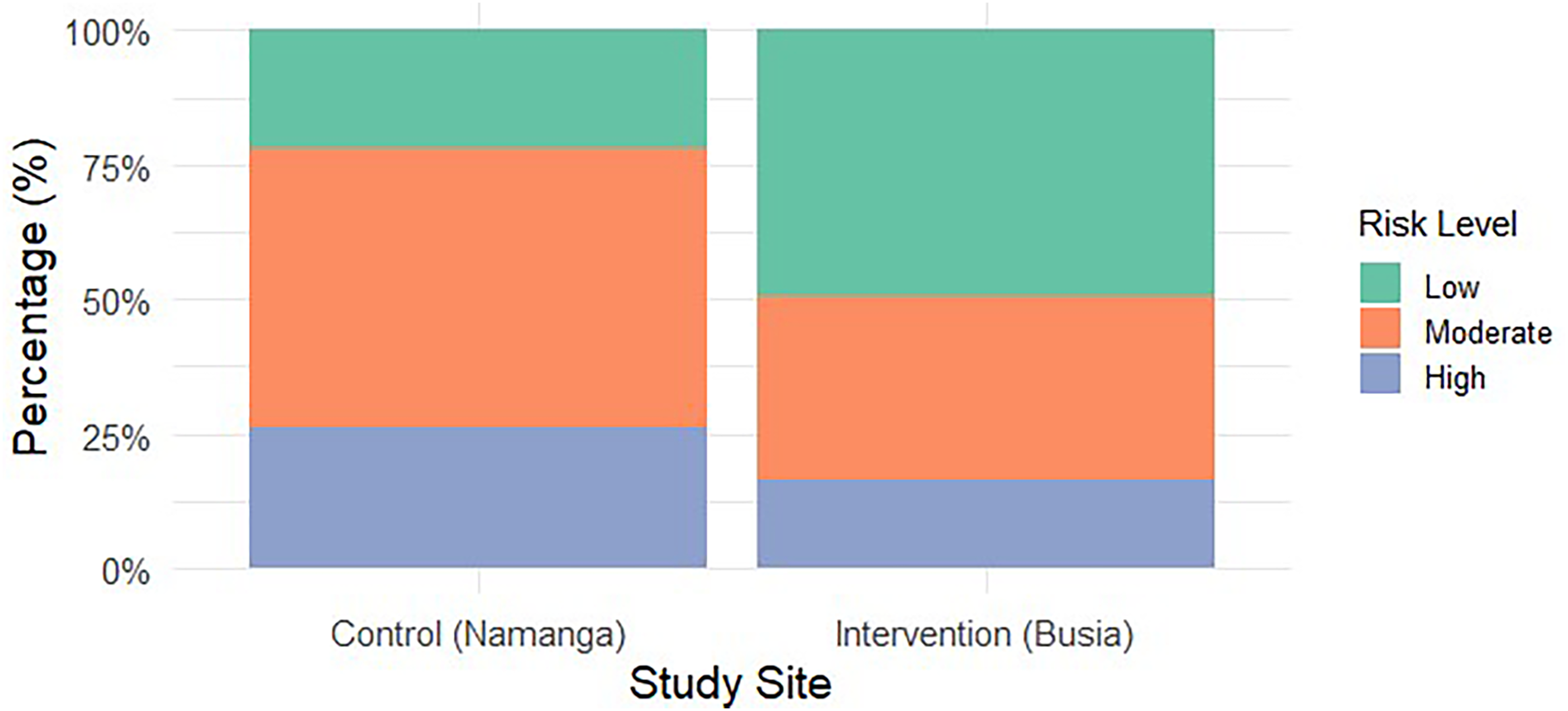
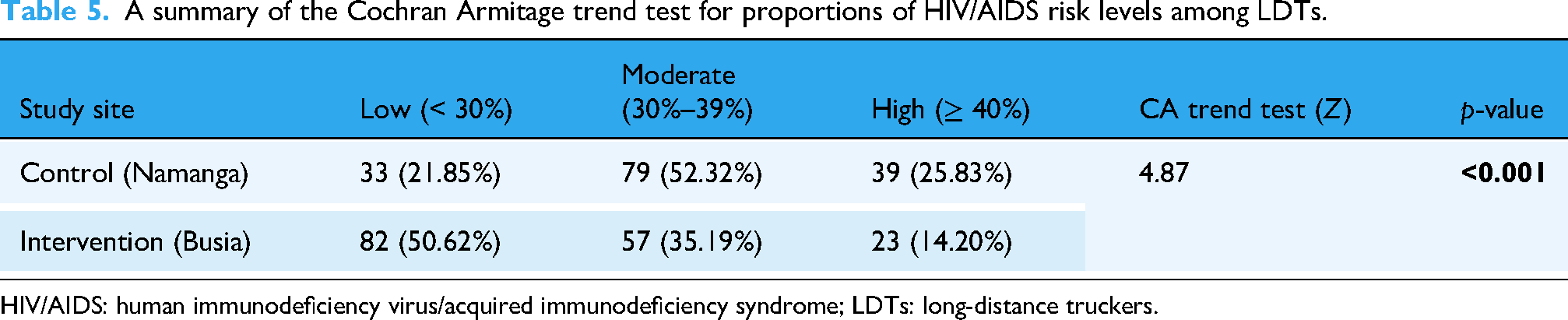
The CA trend test revealed a statistically significant decreasing trend in HIV/AIDS risk levels in the intervention group compared to the control group (Z = 4.87, p < 0.001). Specifically, in the control group, 33 (21.85%) participants were at low risk, 79 (52.32%) at moderate risk, and 39 (25.83%) at high risk. In contrast, in the intervention group, a greater proportion of participants were classified as low risk 82 (50.62%), with 57 (35.19%) at moderate risk and 23 (14.20%) at high risk. These findings suggest that the intervention was effective in reducing HIV/AIDS risk levels. A summary of the CA trend test in proportions is provided in Table 5 and illustrated in Figure 5.
A mosaic plot visualising the effect of the mHealth intervention based on the Cochran Armitage test of proportions in HIV/AIDS risk levels among LDTs.
A summary of the Cochran Armitage trend test for proportions of HIV/AIDS risk levels among LDTs.
HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome; LDTs: long-distance truckers.
Effect size of the mHealth intervention on HIV/AIDS risk reduction among LDTs
The Cramér's V results showed a moderate effect of the mHealth intervention on HIV/AIDS risk reduction. A Cramér's V of 0.3 indicated a meaningful change in risk levels post-intervention. Moreover, the chi-square test results showed a highly significant association between the intervention and changes in risk levels (χ² = 28.214, df = 2, p < 0.001), supporting the effectiveness of the intervention as given in Table 6.
A summary of the mHealth intervention Cramér's V effect size on HIV/AIDS risk reduction among LDTs.

mHealth: mobile health; HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome; LDTs: long-distance truckers.
Discussion
A novel SMS-based mHealth intervention anchored on the IMB model was implemented to enhance HIV/AIDS risk reduction among LDTs in Kenya. Overall, the findings reveal that the intervention significantly lowered HIV/AIDS risk levels in the intervention group (χ2 = 67.07, df = 2, p < 0.001) over the 24 weeks (6 months) follow-up, compared to the control group (χ2 = 0.84, df = 2, p = 0.657), albeit with a moderate effect (Cramér's V = 0.3, χ² = 28.214, df = 2, p < 0.001). As such, the findings reaffirm SMS-based mHealth interventions as a promising platform for HIV/AIDS risk reduction among the hard-to-reach LDTs.8,19
The significant reduction in HIV/AIDS risk levels in the intervention group is a suggestion that the intervention influenced behaviour change over time. Arguably, it is likely that the regular exposure to the risk reduction messages prompted the LDTs in the intervention group to practice safer sexual behaviour, such as sexual partner reduction and enhanced condom use. Furthermore, regular exposure to the messages may have played a role in removing stigma barriers associated with the uptake of HIV risk reduction services like HIV testing, thus creating an enabling environment for LDTs to go for such services, consistent with a similar study done in South Africa. 19 Thus, the findings add weight to the recent UNAIDS call for enhanced technology-based interventions to reach more hard-to-reach populations such as LDTs. 1
More precisely, the success of the intervention can be partly attributed to its foundation on the IMB model. Briefly, the model emphasises the interplay between information, motivation, and behavioural skills. By delivering up-to-date, targeted, and structured SMSs, the intervention addressed information gaps, reinforced motivation for safer practices, such as consistent condom use, and enhanced behavioural skills necessary for risk reduction, including PrEP use. Thus, the model improved HIV/AIDS risk reduction post-intervention. The findings align with another study that demonstrated the effectiveness of an IMB-anchored intervention in promoting HIV/AIDS risk reduction outcomes like enhanced condom use among LDTs in India. 43 However, another study based on the same IMB model found no effect on the intervention outcomes due to high rates of loss to follow-up. 44 Understandably, high loss to follow-up may affect the internal validity of interventional studies and render them ineffective.45,46 However, while the current study was expected to have a considerable loss to follow-up, it was still within (17.2%) the allowable minimum of 20%.45,46 Therefore, it is believed that the loss to follow-up reported here didn’t adversely affect the study's internal validity.
The moderate effect size (Cramér's V = 0.3) identified in this study highlights a meaningful, albeit not large, effect of the mHealth intervention on HIV/AIDS risk reduction among LDTs. This outcome is expected in a real-world scenario where multiple other contextual factors may affect mHealth interventions. Several factors are likely to explain the moderate effect of the intervention in this study. First, given their extremely busy schedule, LDTs may have received the SMSs at varying times. This may be due to network issues, exhaustion, or a lack of time. Second, the TD_Educator digital platform, like other text-messaging platforms, had character limits. This made it challenging to have the SMSs comprehensive enough, especially in certain areas that were fairly new to LDTs, such as PrEP. Consistently, a study by Kelvin et al. (2019), which utilised text reminders to enhance HIV testing, faced similar challenges, thereby affecting its overall effectiveness. 8 Approaches that integrate text-messaging and elaborative video-supported animations on HIV/AIDS risk reduction have been recommended. 8 Moreover, other interventions targeting LDTs have failed to register a significant effect on reducing sexual behaviours. 19 Briefly, while the intervention by Governder et al. (2019) improved HIV testing, it didn't have any effect on risky sexual behaviour reduction among the LDTs, mainly due to inconsistencies in sampling and failure to aggregate outcomes from those of other populations involved, such as FSWs. 19
Additionally, barriers unique to LDTs’ trucking career, such as tight work schedules, high-risk sexual networks, and limited access to HIV/AIDS risk reduction services, may have moderated the overall effect of the intervention.10,12,47 Consistently, the study by Kelvin et al. (2019) achieved a proximally moderate effect size of 2.7 in one of the HIV/AIDS risk reduction domains (HIV testing). 8 However, the study by Governder et al. (2019) had a small effect size of 1.71 on the same HIV/AIDS risk reduction domain of HIV testing. 19
Notably, message delivery was successfully tracked through the TD_Educator platform during the intervention's implementation phase. However, engagement and comprehension during the intervention were not assessed. This is a key shortcoming of the mHealth intervention, as it is unclear whether the end users merely received the messages or were able to apply them practically. Not surprisingly, similar limitations have been encountered in other mHealth interventions. 17 Therefore, future studies should apply strategies such as periodic comprehension checks, follow-up calls, or interactive messaging systems to mitigate this shortcoming.
Lastly, when interpreting the current study's findings, it's essential to note that some baseline characteristics differed significantly between the control and intervention groups. These include age, time spent resting, hours spent in transit, and years of experience. Nevertheless, while the current analysis did not adjust for these differences, a separate ordinal logistic regression analysis for the predictors of HIV/AIDS risk levels at baseline identified age and duration spent on transit among LDTs as significant factors. This suggests that these variables may have influenced the outcomes reported here in one way or another. Thus, future studies should adjust for such predictors to strengthen the internal validity of the intervention effects.
Strengths and limitations
Given the geographical diversity of the two study sites (Namanga and Busia), it was anticipated that the likelihood of interaction between LDTs in the two study arms, leading to contamination of the SMS-based mHealth, would be minimal, which is a strength. Nevertheless, various limitations should be considered while interpreting the findings of this study. First, the reliance on self-reporting of behavioural measures may have introduced social desirability bias, thereby affecting the risk scores reported here. Nonetheless, this was mitigated by creating risk scores based on an interplay of behavioural skills and knowledge outcomes. Additionally, given the longitudinal study design, recall bias may have also affected the risk scores. Moreover, the current study lacked a comprehensive linkage mechanism for the LDTs to a broader range of targeted facilities offering HIV/AIDS risk reduction services, due to the limited nature of such facilities along the Northern Corridor highway in Kenya. However, LDTs were strongly encouraged to seek such services from the available facilities, such as the Busia International Border Point Health Unit. More importantly, the few differences in baseline characteristics such as age, hours spent in transit, and experience in years may have introduced selection bias, limiting comparability of the HIV/AIDS risk outcomes in the two study groups. Thus, the observed changes in the risk levels may partly reflect pre-existing differences rather than the true effect of the mHealth intervention. Lastly, given the constantly evolving evidence on specific aspects of HIV prevention, such as PrEP, the validity of the mHealth intervention may weaken over time, needing extensive revisions in the future.
Conclusion
The current study underscores the potential of SMS-based mHealth interventions in enhancing HIV/AIDS risk reduction among LDTs. By leveraging the IMB model, such interventions can enhance knowledge, motivation, and behavioural skills, ultimately improving HIV/AIDS risk reduction outcomes like PrEP use, safe sexual behaviours, and HIV testing among the hard-to-reach and vulnerable LDTs. Nevertheless, considering the differences in some of the baseline characteristics observed in this study, caution should be exercised when generalising the present study's findings to broader populations of LDTs, as contextual differences may lead to varied outcomes. Nurses, clinicians, peer educators, and other relevant stakeholders directly involved in the provision of HIV/AIDS risk reduction services to LDTs should implement a multi-modal SMS-based mHealth intervention that incorporates the current TD_Educator digital platform and elaborative short video animations to overcome the character limitations and enhance comprehensiveness in relatively new topics such as PrEP.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251390322 - Supplemental material for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study
Supplemental material, sj-doc-1-dhj-10.1177_20552076251390322 for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study by Cyrus Mutie, John Gachohi, Kawira Rosemary Kithuci and Grace Mbuthia in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251390322 - Supplemental material for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251390322 for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study by Cyrus Mutie, John Gachohi, Kawira Rosemary Kithuci and Grace Mbuthia in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251390322 - Supplemental material for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study
Supplemental material, sj-docx-3-dhj-10.1177_20552076251390322 for Effectiveness of an mHealth intervention in HIV/AIDS risk reduction among long-distance truckers in Kenya: A quasi-experimental study by Cyrus Mutie, John Gachohi, Kawira Rosemary Kithuci and Grace Mbuthia in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the long-distance truckers at Busia and Namanga points in Kenya for finding time to participate in this study amidst their busy transit schedule. We also acknowledge the tremendous support and cooperation offered by the trucker peer educators, community mobilizers, healthcare professionals and data enumerators at Busia and Namanga border points in Kenya.
Ethical considerations
Ethical approval was granted by the ethical review committee of Jomo Kenyatta University of Agriculture and Technology (JKUAT), JKU/ISERC/02317/1256. The study was also licensed by the National Commission for Science, Technology, and Innovation, Kenya (NACOSTI), NACOSTI/P/24/33837. More approvals were obtained from Busia (ADM 15/27 Vol. 1/151) and Kajiado (KJD/CC/ADM/45 VOL.V (4) Counties in Kenya.
Consent for publication
All information used in the development of the manuscript is fully anonymized and does not contain any identifying details of study participants. Therefore, a publication consent was not applicable.
Authors’ contributions
CM conceived the study and methodology, performed administration, data collection, software and analysis and wrote the original draft. KK, JG and GM conceived the study and methodology, supervised the study, and writing and reviewing.
Funding
The authors did not receive any financial support in the development, data collection, analysis, authorship and publication of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets and other relevant material used in the development of the current study findings are available upon request from the corresponding author.
Guarantor
CM is responsible for the overall content as guarantor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.