
Abstract
Background
Personality traits influence behavioral changes and may impact engagement and outcomes in obesity management programs. However, their role in mobile app-based interventions for obesity remains underexplored. Understanding the relationship between personality traits and health behaviors can inform the design of personalized programs, potentially enhancing adherence and long-term success. Mobile health technologies offer scalable solutions for lifestyle modification, making this investigation particularly relevant.
Methods
This study analyzed 2716 participants with a body mass index of 25.0 or higher enrolled in a six-month mobile app-based lifestyle modification program. Personality traits were assessed using the five-factor model, and participants were categorized into resilient, overcontrolled, and undercontrolled prototypes through cluster analysis. App engagement metrics, such as session frequency, usage duration, and weight input rates, were recorded. Weight loss outcomes were measured as the percentage reduction in body weight, calculated by comparing the first and last 14 days of the program. Additional variables, including daily steps, blood pressure, and cholesterol levels, were evaluated to assess overall health changes.
Results
The undercontrolled group exhibited the lowest engagement metrics, including fewer app sessions (2.63 times/day) and a lower weight input rate (63.06%). In contrast, the overcontrolled group achieved the highest weight loss, with a mean reduction of −3.08% compared to −2.55% in the undercontrolled group (p = 0.015). The resilient group demonstrated the highest daily app usage duration (9.09 min/day). Across all groups, no significant differences were observed in blood pressure, daily steps, or cholesterol levels. Cluster analysis confirmed that three prototypes effectively captured behavioral and programmatic differences among participants.
Conclusion
Personality prototypes significantly influence engagement and weight loss in a mobile app-based lifestyle modification support program. These findings highlight the importance of considering personality traits to enhance program design and effectiveness. Further research is required to validate these outcomes across diverse populations and examine the long-term sustainability of behavioral changes.
Introduction
Obesity is a significant global issue, and its prevalence continues to increase. 1 Because obesity is a major risk factor for various non-communicable diseases (NCDs), such as hypertension, diabetes, ischemic heart disease, and chronic kidney disease, it must be urgently addressed. Lifestyle modification is a cornerstone of obesity management, with established evidence on weight reduction and controlling cardiovascular risk factors in adults with obesity.2,3 In recent years, mobile applications (apps) and digital technologies have been increasingly adopted to reach large numbers of people simultaneously and provide support at a low cost. Previous studies have reported the effectiveness of digital health and mobile apps in promoting weight loss through self-monitoring among individuals with obesity, facilitating behavioral changes such as improvements in diet and exercise, and reducing risk factors, including hypertension and diabetes.4–7
Individual personality traits influence the achievement of lifestyle modifications and the acquisition of disease management skills. Previous studies have reported that prominent personality types, types A (characterized by impatience and competitiveness) and D (marked by negative affectivity and social inhibition) personality patterns were associated with adherence to treatment for conditions such as cardiovascular disease and diabetes.8–12 In the five-factor model, which describes personality through five dimensions—neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness—previous studies have reported associations among neuroticism, conscientiousness, and disease management skills.13–16 Incorporating individual personality traits into lifestyle modification support programs could aid in the development of more personalized interventions, potentially leading to greater program effectiveness.
Clustering analysis of the five-factor model identified three distinct personality prototypes, categorized based on individuals’ adaptability to change, conflict, and self-control in a previous study. 17 These prototypes include the resilient type, characterized by high adaptability and flexibility in managing stress and unexpected events; overcontrolled type, defined by perfectionism, rigidity, and introversion, with a strong drive for goal achievement but difficulty coping with failure and unforeseen challenges; and undercontrolled type, marked by impulsivity, poor planning, and low tolerance to stress and adversity. The resilient type is distinguished by low levels of neuroticism and high conscientiousness. Conversely, the overcontrolled type was associated with high neuroticism and low extraversion, whereas the undercontrolled type exhibited both high neuroticism and high extraversion, along with low conscientiousness. These personality prototypes have been observed in various populations, including young individuals with eating disorders, 18 those with psychiatric symptoms, 19 and patients recovering from spinal cord injuries. 20 Another study reported the existence of these three personality prototypes in patients with type 1 diabetes, and differences in disease management status and behaviors were observed across different personality types. 21
These traits are also likely to influence engagement using a mobile app-based lifestyle modification support programs and their outcomes. However, no studies have investigated this aspect in people with obesity. Therefore, this study aimed to identify personality prototypes in individuals with obesity, evaluate their influence on app engagement and weight loss outcomes, and hypothesize that these traits affect program effectiveness.
Methods
Study design and setting
This retrospective observational study used data from PREVENT, Inc. (Nagoya, Japan). This company provides medical data analysis and mobile app-based lifestyle modification support programs for individuals with NCDs and predicts the risk of cerebrovascular and cardiovascular diseases using health insurance claims and health checkup data. Moreover, healthcare professionals could offer individualized support programs to employees or their dependents at a high risk of these diseases. All participants provided written informed consent before their inclusion in the program. This study was conducted with the approval of the Institute of Transdisciplinary Sciences Ethics Committee, Kanazawa University (Approval no. R6-003), and conducted in accordance with the principles of the Declaration of Helsinki. This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The completed STROBE checklist is available in Appendix 1 as the Supplemental Material.
Study population and procedure
PREVENT, Inc., offers the “Mystar” program through health insurance companies, targeting people who have NCDs such as hypertension, dyslipidemia, and diabetes and are at high risk of cerebrovascular and ischemic heart disease. Those who participated in the program between December 2018 and November 2023 and had obesity at the start of the program were included. Participants who did not complete the six-month program or had missing body weight measurements at the final evaluation were excluded from the analysis using listwise deletion. Obesity was defined as a body mass index (BMI) of 25.0 kg/m2 or higher.
Disease management program
The program was approved by the attending physicians of the participants. The lifestyle modification support program was provided over 6 months through a total of 12 phone call sessions with healthcare professionals, held every 2 weeks, along with chat messaging between sessions. Each participant was issued an account for a mobile app, through which they logged lifestyle data such as body weight, blood pressure, physical activity, salt intake, and food photos. Healthcare professionals analyzed these data to identify key areas for lifestyle modification based on each participant's situation, fostering communication that drives behavior change. Within the app, participants could log their lifestyle data, monitor changes in their habits, review corrective goals and behavior to-do lists, chat with their healthcare providers, and access disease management information provided by their coach. The program targets improvements in exercise, diet, sleep, alcohol consumption, smoking, stress management, and so on, with personalized health plans developed for each participant. Further details are described in a previous study.22,23
Personality traits
Personality traits were assessed using the 10-item personality inventory Japanese version (TIPI-J). 24 The original questionnaire was developed to provide a quick and easy assessment of personality traits, allowing evaluation using only 10 items. 25 The TIPI questionnaire is based on the five-factor model that assesses neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. The questionnaire consists of 10 items, with two items related to each of the five factors, and each item is rated on a seven-point Likert scale, ranging from 1 (strongly agree) to 7 (strongly disagree). The TIPI-J, a validated and widely used 10-item instrument grounded in the five-factor model, has demonstrated reliability and construct validity in Japanese populations.24,26,27 The full questionnaire used in this study is provided in Appendix 2 as the Supplemental Material.
Mobile app engagement
App engament during the six-month program—including session count, app usage time, chat message count, weight input rate, and number of meal photos uploaded—was measured to indicate participant engagement. The session count was defined as the average number of app launches per day. Other engagement metrics included app usage time, measured by the daily duration of app use; number of chat messages, counted for participants and healthcare professionals weekly; weight input rate, calculated by dividing the number of weight inputs by the total program days; and the total number of meal photos uploaded throughout the program.
Primary outcome
The primary outcome of the six-month lifestyle modification support program was the percentage of weight changes. The participants were instructed to achieve a weight reduction of ≥3% of the baseline body weight over 6 months according to the Japan Atherosclerosis Society Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases. 28 The weight change rate was calculated by comparing the average weight during the first 14 days of the program with the average weight during the period from 14 days before the program's end to the final day.
Other variables
Participant characteristics, including age, sex, height, weight, and blood pressure, were collected. Medical information such as medications; history of hypertension, dyslipidemia, diabetes, cerebrovascular disease, and ischemic heart disease, and health checkup results including serum lipid levels and hemoglobin A1c (HbA1c) from blood tests, were recorded. These demographic and medical data were collected at the start of the program.
Statistical analysis
Cluster analysis was performed using the k-means method based on the five personality traits. To determine the optimal number of clusters, both the elbow method and silhouette method were employed. In the elbow method, the within-cluster variance was plotted against the number of clusters to identify the point where additional clusters no longer substantially reduced variance. The silhouette method was used to assess the average silhouette width for each solution, with higher values indicating better-defined clusters.
Demographic characteristics, app usage engagement, and average program effectiveness across the extracted clusters were compared using the one-way analysis of variance (ANOVA) and chi-squared test. Post hoc analysis for the one-way ANOVA was performed using Tukey's method, and Bonferroni correction was applied for multiple comparisons. Subsequently, ANCOVA was performed to examine the associations between personality prototypes and outcomes, adjusting for age, sex, and baseline BMI. A p-value of 5% was considered significant, and all analyses were conducted using R (Version 4.4.1).
Results
Identification of personality prototypes
Data from 2716 participants with obesity who completed the program were analyzed. Of the initial participants, 145 (2.5%) were excluded due to missing outcome data at the final evaluation. The final analytical sample consisted of participants who completed the six-month program and had complete data for the main outcomes. The completion rate was 97.5%. The average age of the participants included in the analysis was 54.3 years, and 88.0% were male. The elbow method was applied to validate the number of clusters, suggesting that a three-cluster solution was relatively appropriate (Figure 1). Based on the silhouette analysis, the average silhouette scores for the two-, three-, and four-cluster solutions were 0.224, 0.185, and 0.173, respectively. Three groups were identified, namely, the resilient, overcontrolled, and undercontrolled types (Figure 2). Table 1 summarizes the characteristics of the participants by personality prototypes. The resilient type tended to be older and had a lower BMI than the other two types. The personality prototypes were distributed as the resilient (31.5%), overcontrolled (34.4%), and undercontrolled (34.1%) types.

Result of the examination of cluster numbers using the elbow method.

Cluster analysis using personality traits assessed by the five-factor model.
Characteristics of the participants by personality prototype.

aValues are presented as mean (standard deviation).
bValues are presented as number (percentage).
App engagement across personality prototypes
App engagement metrics were analyzed across the personality prototypes (Table 2). The resilient type had a significantly higher average number of sessions per day than the undercontrolled type (resilient type, 2.89 times/day; undercontrolled type, 2.63 times/day, mean difference = 0.26 times/day, 95% CI: 0.12–0.40, t = −3.406, p < 0.001). The daily app usage time was also longer for the resilient type (9.09 min/day) than for the undercontrolled type (7.76 min/day), with a mean difference of 1.33 min/day (95% CI: 0.30–2.36, t = 2.510, p = 0.012). The weight input rate throughout the program was higher in the resilient and overcontrolled types than in the undercontrolled type (resilient type, 67.17% vs. undercontrolled type, 63.06%, mean difference = 4.11%, 95% CI: 0.79%–7.43%, t = −2.635, p = 0.008; overcontrolled type, 68.82% vs. undercontrolled type, mean difference = 5.76%, 95% CI: 2.53%–8.99%, t = −3.690, p < 0.001). Overall, app engagement was lower in the undercontrolled type. After adjusting for age, sex, and baseline BMI using ANCOVA, only app usage time remained significantly associated with personality prototypes (p = 0.038).
App engagement by personality prototype.

aValues are presented as mean (standard deviation).
* < 0.05 versus undercontrolled group.
Comparison of program effectiveness by personality prototypes
The effectiveness of the program was assessed across the personality prototypes. The overcontrolled type exhibited the greatest weight loss, which was significantly higher than that of the undercontrolled type (overcontrolled type, −3.08%; undercontrolled type, −2.55%; mean difference = −0.53%, 95% CI: −0.84% to −0.22%, t = 2.958, p = 0.003). The difference in weight loss across clusters remained statistically significant after adjusting for age, sex, and baseline BMI (p < 0.05). However, among the personality prototypes, no significant differences were identified in other outcome measures, such as changes in blood pressure, low-density lipoprotein-cholesterol levels, or HbA1c (Table 3).
Program effectiveness by personality prototype.
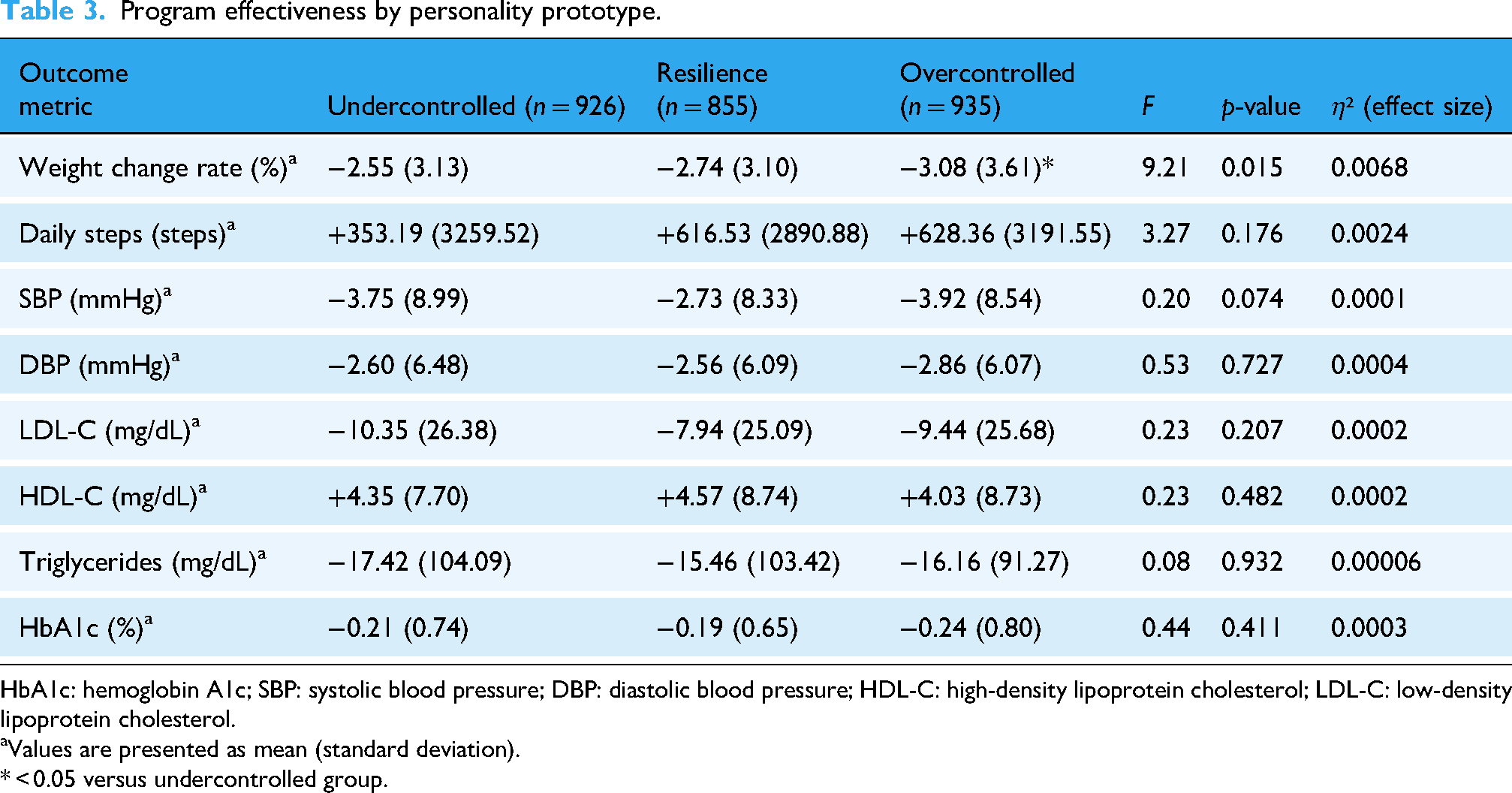
HbA1c: hemoglobin A1c; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol.
aValues are presented as mean (standard deviation).
* < 0.05 versus undercontrolled group.
Discussion
This study identified personality prototypes among individuals with obesity who participated in a mobile app-based lifestyle modification support programand examined their associations with app engagement and program outcomes.
Personality prototypes based on the five-factor model—resilient, undercontrolled, and overcontrolled—were identified using cluster analysis, reflecting differences in adaptability and stress management. 17 The silhouette analysis showed low Silhouette scores for all cluster solutions, suggesting ambiguous boundaries between clusters. While the two-cluster solution had the highest silhouette score, the four-cluster solution suggested the possibility of overfitting. Considering the changes in the graph for the two- and three-cluster solutions based on the elbow method, the differences in characteristics between groups in the three-cluster solution, and the fact that three clusters were identified in previous studies using similar personality traits metrics, it was determined that selecting three clusters for this study was reasonable. In this study, the rates for the resilient, undercontrolled, and overcontrolled types were 31.5%, 34.1%, and 34.4%, respectively. Asendorpf et al. 17 reported that in four studies of children and adults, the average prevalence rates of the three prototypes were 49%, 28%, and 23% for the resilient, undercontrolled, and overcontrolled, respectively. They also noted that the high prevalence of the resilient type was a consistent finding across all target populations. In the present study, the prevalence of the resilient type was low and similar to those of the other two groups. In a meta-analysis examining personality traits and the incidence of obesity, high conscientiousness exerted a suppressive effect on obesity development. 29 This study focused on obesity and hypothesized that the low conscientiousness characteristic of obesity might contribute to the low prevalence of resilient types characterized by high conscientiousness.
By app engagement, significant differences were identified based on the personality prototypes. The undercontrolled type had the lowest level of app engagement, whereas the overcontrolled type demonstrated significantly greater weight loss than the undercontrolled type. The undercontrolled type showed low app usage frequency, usage duration, and weight input rates. The undercontrolled type is characterized by high levels of neuroticism and extraversion, low conscientiousness, and a tendency to engage in impulsive and mood-dependent behaviors. In previous studies examining the relationship between disease management behaviors and personality traits in patients with diabetes and those undergoing peritoneal dialysis, high neuroticism, and low conscientiousness were found to be associated with lower adherence to exercise and dietary behaviors, high complication risk in patients undergoing dialysis, and lower medication adherence.15,30–32 In this study, the resilient type, characterized by low neuroticism and high conscientiousness, showed the highest engagement level in app usage. For the undercontrolled type, individualized strategies that include setting realistic and achievable behavioral goals that enhance self-efficacy rather than focus on high goal-setting may be essential. Utilizing social support to motivate the participants and promote behavior changes is another potentially effective measure for this population.
Conversely, the overcontrolled type demonstrated the highest weight loss effect. This type is characterized by high neuroticism, introversion, and a strong commitment to goal achievement and adherence to plans, often manifesting as perfectionism. These inherent tendencies may influence the weight loss outcomes. Previous studies examining the relationship between glycemic control and personality prototypes in patients with type 1 diabetes revealed that those with an overcontrolled type achieved the most favorable glycemic control than those with the resilient and undercontrolled types. 21 Neuroticism demonstrates both inhibitory and facilitative effects on disease management behaviors. In the study examining the relationship between glycemic control and personality traits in patients with type 2 diabetes, individuals with higher neuroticism levels demonstrated better glycemic control 33 because they perceive a greater risk of diabetes complications and subsequent severe diseases, which might promote disease management behaviors. Another study reported that high neuroticism levels were associated with high HbA1c levels in patients with type 2 diabetes. 32 The differences in disease management tendencies between the undercontrolled and overcontrolled types with high neuroticism propose that other personality factors may influence the opposing effects of neuroticism on disease management. In addition, the overcontrolled type tends to have difficulty with flexible responses to unexpected changes. The results of this study showed that although the weight loss difference between the overcontrolled and undercontrolled types was statistically significant, the absolute difference was small and may not be clinically meaningful. Based on these findings, personality prototypes may not serve as strong determinants of clinically meaningful weight loss, but they could still be valuable in guiding personalized behavioral support strategies. Considering their influence on engagement patterns, personality traits might help tailor intervention approaches to enhance adherence and effectiveness in digital health programs. However, as this was a retrospective observational study, we were unable to assess causal relationships, including whether engagement mediates the link between personality and outcomes, or whether individualized guidance had differential effects across personality types. Future studies using longitudinal or time-series data are needed to clarify these temporal and associative dynamics.
Also, the role of personality prototypes in behavior change over the medium to long term, particularly the continuation of behaviors after program completion and adjustments after failures in health behaviors, must be investigated.
This study has several limitations. Its findings should be interpreted with caution owing to potential selection bias. This study researched the data from participants in programs provided by corporate health insurance associations. Consequently, it is likely that most participants are male, being employed full-time, voluntarily participating in the programs, and inherently possess digital literacy. This sample bias may limit how broadly the findings can be applied, especially to populations with different backgrounds or work settings. Second, this study did not assess the effect of the content of healthcare professional guidance on outcomes. Participants received support through 12 telephone consultations and chat interactions over 6 months. Although no guidance policies were tailored to personality traits, healthcare professionals may have adjusted their support strategies to suit individual participant characteristics Third, while the TIPI-J is a validated and practical instrument for personality assessment based on the five-factor model, it relies on only two items per dimension. This brevity reduces respondent burden but may also limit its reliability and ability to reflect complex personality structures. These limitations should be acknowledged when interpreting the study's findings. Nevertheless, the TIPI-J has demonstrated acceptable validity and reliability in Japanese populations and is widely used in research, making it a practical choice for large-scale studies such as the current study.
Fourth, this study had several unmeasured confounders. The study did not examine the influence of IT literacy on app engagement, job characteristics or occupational demands that might affect the duration and manner of app usage, as well as familiarity with IT, and information regarding educational background that might be associated with disease management skills. While education was not directly measured, limited variation in Japan may have reduced its influence. Future studies should test this in more diverse groups.
Conclusions
This study identified resilient, overcontrolled, and undercontrolled personality prototypes among participants in a mobile app-based lifestyle modification support program. These prototypes influenced app engagement and weight loss outcomes. The findings might be useful for constructing personalized programs that consider personality prototypes, enhancing engagement and effectiveness. More studies are warranted to validate these results across diverse populations and explore long-term sustainability.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251347891 - Supplemental material for Impact of personality prototypes on app engagement and weight loss in a mobile app-based lifestyle modification support program for individuals with obesity and non-communicable diseases
Supplemental material, sj-doc-1-dhj-10.1177_20552076251347891 for Impact of personality prototypes on app engagement and weight loss in a mobile app-based lifestyle modification support program for individuals with obesity and non-communicable diseases by Yuta Hagiwara, Kotoe Shimizu, Takuji Adachi, Masashi Kanai and Takahiro Miki in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251347891 - Supplemental material for Impact of personality prototypes on app engagement and weight loss in a mobile app-based lifestyle modification support program for individuals with obesity and non-communicable diseases
Supplemental material, sj-docx-2-dhj-10.1177_20552076251347891 for Impact of personality prototypes on app engagement and weight loss in a mobile app-based lifestyle modification support program for individuals with obesity and non-communicable diseases by Yuta Hagiwara, Kotoe Shimizu, Takuji Adachi, Masashi Kanai and Takahiro Miki in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to express our gratitude to all participants who contributed to the program evaluation and the research team members at PREVENT, Inc., for their support in data collection and analysis. The authors thank the participants of the mobile app-based lifestyle modification support program for their contributions. Special thanks to the research team at PREVENT Inc. for their support in data collection and management.
Ethical Considerations
The project received ethical approval from the Institute of Transdisciplinary Sciences Ethics Committee, Kanazawa University (approval no. R6-003). The study adhered to ethical standards as outlined by the Declaration of Helsinki.
Consent to participate
All participants provided informed consent prior to their inclusion in the lifestyle modification program. The data used in this study were anonymized and aggregated to ensure participant confidentiality.
Author Contributions
Yuta Hagiwara: conceptualized the study, supervised data analysis, and drafted the article. Kotoe Shimizu: performed statistical analysis and contributed to article preparation. Takuji Adachi: provided expertise on study design and critically revised the article. Masashi Kanai: assisted in data collection and interpretation. Takahiro Miki: provided oversight on methodology and reviewed the final article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yuta Hagiwara, Kotoe Shimizu, Masashi Kanai, and Takahiro Miki are employees of PREVENT Inc., which provides the mobile app-based lifestyle modification program evaluated in this study.
Guarantor
Takahiro Miki accepts full responsibility for the integrity and accuracy of the study's data analysis and results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.