
Abstract
Objective
This study aimed to explore the utility of a high-intensity interval training (HIIT) app as a remote exercise support strategy in children with obesity through assessing adherence, possible effects on obesity-related outcomes, and perceptions of its use to support counseling and improve the treatment of children with obesity.
Methods
Thirty-seven children (94.6% with obesity; 45.9% girls), with a mean age of 10.4 (±1.8) years and a mean body mass index (BMI) z-score of 3.31 (±1.09) were recruited to use the app during 6 weeks. Assessments were performed at baseline, 6 (end of intervention), and 12 weeks (follow up).
Results
Thirty-two (86.3%) participants completed both intervention and follow-up assessments and were analyzed. On average, children used the HIIT app 2.5 times per week (95% confidence interval (CI): 1.9 to 3.0), with the highest perceived exertion of 4.1 (95% CI: 3.6 to 4.5). No over-time differences were found in body composition, physical activity, screen time, sleep duration, or water intake after the intervention; however, an over-time decrease in sugary beverages intake (Δ−0.9, 95% CI: −1.6 to −0.1, p = .019). No differences in body composition were found at follow up. Although none of the children or parents perceived impairments in nutritional behavior, general wellbeing, or fitness as a consequence of intervention, most children (64.5%), but not parents, perceived improvements in nutritional behavior and general wellbeing.
Conclusion
Although feasible, the 6-week effect of HIIT app use is modest or absent regarding body composition, movement, and nutritional behavior change, probably due to its low volume. More studies are needed to explore the utility of HIIT apps as a remote exercise support strategy for children with obesity further.
Introduction
Insufficient physical activity (PA) is a growing public health problem with a significant social and economic impact. 1 Insufficient PA may contribute to increased incidence of noncommunicable diseases in childhood, which may track to adulthood,2,3 with obesity one of the most prevalent. 4
It is estimated that around 8% of Brazilian children and adolescents have obesity (body mass index (BMI) z-score ≥ 2). 5 Despite the low prevalence of pediatric obesity (compared to most European countries), the prevalence of physical inactivity is high in Brazil, with around 75% of children/adolescents not achieving the PA guidelines (i.e., 60 min/day of moderate-vigorous PA). 6 Even so, it has been estimated that a 10% decrease in the prevalence of physical inactivity would be associated with decreased chronic non-communicable diseases and related hospitalization costs in Brazil.7,8
In-person PA interventions targeting childhood obesity, including high-intensity interval training (HIIT), which has been identified as a suitable obesity-management strategy for adolescents, 9 have shown limitations, not only to the inconsistent results reported, in part due to low adherence 10 but also on its range, mainly due to its costs.
Technological advances and increased use of electronic devices have been suggested as one of the leading causes of high sedentary time and insufficient PA.11,12 Yet, recent studies suggest that electronic devices, appropriately used, may represent an opportunity to intervene among those with high exposure to technological advances (i.e. children), possibly becoming an efficient health promotion tool in the youngest generation. 13
Electronic devices such as active video games, wearables, smartphones, and mobile applications (apps) may be used to address diet, sedentary, and PA behavior, leading to improvements in those behaviors,14,15 thus suggesting a possible effect on obesity-related indicators, such as BMI. Specific apps targeting PA behavior allow activity monitoring, goal setting, progress tracking, and instant feedback, which are crucial components and facilitators of effective behavior change. 16 On the other hand, barriers to technology use also exist and may explain in part the modest effects reported. Barriers such as social and cultural aspects, family context, and parental acceptance may mediate the use of mHealth technology and its efficacy in turn.17,18
Multicomponent interventions (including in-person contact and mHealth support) seem more effective than stand-alone app interventions, especially when targeting behavioral change, including PA behavior,19,20 and may overcome parental reluctance regarding app use. 21 This evidence is, however, scarce among children. 16
This study aimed to explore the utility of the HIIT app as a remote exercise support strategy in children with obesity through assessing adherence, possible effects on obesity-related outcomes, and perceptions of its use to support counseling and improve the treatment in children followed at a pediatric obesity clinic.
Methods
Study design
This study used a mixed methods approach, including two phases: (i) an intervention phase, in which the participants were asked to install the HIIT app and to perform a structured exercise plan using the app at least 5 days a week for 6 consecutive weeks. During the intervention phase, parents were contacted daily by phone (weekdays) to reinforce adherence and to assess perceived exertion and (ii) a follow-up phase without any contact, also with 6 6-week duration (longitudinal design).
In addition, data on participants’ and parents’ perceptions regarding using the HIIT app was assessed using a semistructured interview at the end of the intervention, that is, week 6 (cross-sectional design).
Participants
Children aged 7 to 13 years, with overweight or obesity (BMI ≥ 85th percentile for gender and age 22 ), followed at the Obesity Outpatient Clinic, Hospital das Clínicas, State University of Campinas (Unicamp), with access to a smartphone, were eligible to be included. Exclusion criteria included the presence of psychiatric disorders, other concomitant diseases (e.g. endocrine, renal, pulmonary, or cardiovascular diseases), and menarche (girls).
Procedure
At baseline, the same nonblinded trained professional assessed anthropometric, movement, and nutritional data during routine clinical appointments. Additional data on body composition was assessed by a trained, blinded professional at an office used specifically for this purpose.
After baseline assessments, the HIIT app was set up, and an exercise plan was prescribed and provided to the participants by the research staff.
All the assessments performed at baseline were repeated at week 6 (end of intervention). A semistructured interview was conducted to assess children's and parents’ perceptions in week 6.
Anthropometric data were additionally assessed at week 12 (end of follow up). In week 12, children and parents were asked about the use of apps during the follow-up period.
Intervention
After the HIIT app setup (Tabata Timer®), facilitated by the research staff, aiming to support the short-duration exercise sessions prescribed, by setting the precise workout/recovery periods, participants were instructed to perform the prescribed exercise plan at least 5 days a week, for 6 consecutive weeks.
The exercise plan included a short mobilization/warm-up (10 seconds) and 4 sets (in 4 cycles) of jumping jacks, single-leg hop-to-foot (without horizontal displacement), dynamic squats, and isokinetic plank. Each exercise was set to be performed for 20 seconds, with 10 seconds of recovery between and 50 seconds of recovery between cycles, totaling 600 seconds (10 minutes).
Variables and instruments
Anthropometric and body composition
Height was assessed with a fixed stadiometer in the anthropometric position, without shoes, after an expiratory phase, and registered to the nearest 0.1 cm (height stadiometer, Sanny ES2020, American Medical do Brazil Ltd).
Body weight was measured with a mechanical anthropometric scale to the nearest 0.1 kg, with the participants wearing as little clothing as possible, without shoes, with the arms along the body (Welmy scales, Brazil).
BMI was calculated as body weight in kilograms divided by the square of height in meters (BMI = weight (kg)/height2 (m)). The BMI z-score was further calculated according to the World Health Organization reference 23 using the AnthroPlus calculator (version 1.0.4, WHO).
Body composition was assessed by a four-terminal single frequency (800 mA at 50 kHz) bioelectric impedance (Quantum II, RJL Systems, Clinton Twp., Detroit, USA) on a measuring table, with the participants in the supine position, wearing light clothing, without shoes or socks, with arms adjacent to the body (without touching), palms flat against the table, and legs adjacent to each other (without touching). Four surface self-adhesive spot electrodes were placed on the right foot (a distal electrode at the base of the middle finger and a proximal electrode just above the ankle joint line, between the medial and lateral malleoli) and on the right hand (a distal electrode at the base of the middle finger and a proximal one just above the wrist joint line, coinciding with the styloid process). Before electrode placement, the skin was wiped with alcohol at the four locations for electrode placement. Whole-body fat mass (BFM) and muscle mass (MM) were considered measures of interest.
Movement and nutritional behaviors
PA, specifically light physical activity (LPA) and moderate-vigorous physical activity (MVPA), screen time, sleep duration, as well as water and sugary beverages intake, were assessed by an interview. 24
Adherence and perceived exertion
Adherence (i.e. the number of times per week a participant used the app) and perceived exertion were daily proxy-reported by the parents during a phone call with the research staff. Perceived exertion was assessed with an adapted version of Borgs’ subjective effort scale (0–10).
Children and parents’ perceptions
The research team designed a semistructured interview guide, which experts subsequently evaluated until a consensus was reached. The semistructured interview guide can be found in Supplemental materials. Semi-structured interviews were conducted separately with children and parents. All the interviews were recorded and later transcribed for analysis purposes. The main topics included (i) changes in nutritional behavior, (ii) general well-being, and (iii) fitness as a consequence of apps’ use.
Both children's and parent's perceptions were assessed using a likert scale (0–5) 25 from “Much worse” (0) to “Much better” (5) regarding each topic, and transformed into a bivariate variable. The answers “Much worse now,” “A little worse now,” and “The same” were coded as impairment; and “A little better” and “Much better now” as improvement.
Parental education
Parental education was reported by parents and assessed at baseline (0, no school attendance; 1, uncompleted elementary school; 2, completed elementary school; 3, uncompleted middle school; 4, completed middle school; 5, uncompleted high school; 6, completed high school; 7, uncompleted bachelor's degree; 8, completed bachelor's degree; 9, uncompleted master's degree; 10, and completed master's degree or higher).
Ethical aspects
This study was approved by the Research Ethics Committee by following the norms established by Resolution 466/2012 of the National Health Council. All the participants (and respective parents) who agreed to participate signed informed consent/assent.
Statistical analysis
Data were analyzed using IBM SPSS statistics (version 28.0, IBM, New York, USA). Normal distribution was tested with the Shapiro-Wilk test and confirmed by histogram observation. Descriptive characteristics, that is, mean ± SD, were calculated for normally distributed outcomes. Baseline differences between girls and boys were analyzed with independent sample t-tests and Chi-squared for continuous and categorical variables, respectively.
Generalized estimating equations (adjusted for age and tanner stage) were used to analyze over-time changes, sex, and sex-by-time interaction in body composition, movement, and nutritional behaviors.
A p-value of ≤.05 was considered statistically significant.
Results
A total of 37 children (94.6% with obesity; 45.9% girls), with a mean age of 10.4 (±1.8) years and a mean BMI z-score of 3.31 (±1.09), and respective parents (all mothers, 73.0% with obesity) were included in the present study. No differences between girls and boys were found in body composition at baseline (Table 1).
Participants’ baseline characteristics.

*Parental education (0: no school attendance to 10: completed master's degree or higher) is presented as median (interquartile range).
Between-group differences analyzed with independent-Sample t-test and Chi-squared test, respectively.
BFM: body fat mass; BMI: body mass index; SMM: skeletal muscle mass.
Adherence and perceived exertion
Of the 37 children recruited, 5 (13.7%) did not attend 12-week assessments at the clinic, being excluded from the analysis. “Lack of time due to work obligations” and “family problems” were the main barriers reported by parents for not attending the assessments/appointments.
On average, children used the HIIT app 2.5 times per week (95% confidence interval (CI): 1.9 to 3.0), with no observed differences between girls and boys. In general, the highest app use was observed in week 2, with an average of 3.4 times per week (95% CI: 2.7 to 4.1), being observed a significant decrease in week 4 (Δ−1.2, 95% CI: −2.4 to 0.0, p = .038), 5 (Δ−1.2, 95% CI: −2.3 to 0.1, p = .024), and 6 (Δ−1.5, 95% CI: −2.8 to 0.3, p = .007) compared to week 2 (Figure 1). None of the children reported continuing their use of the HIIT app during the follow-up phase.
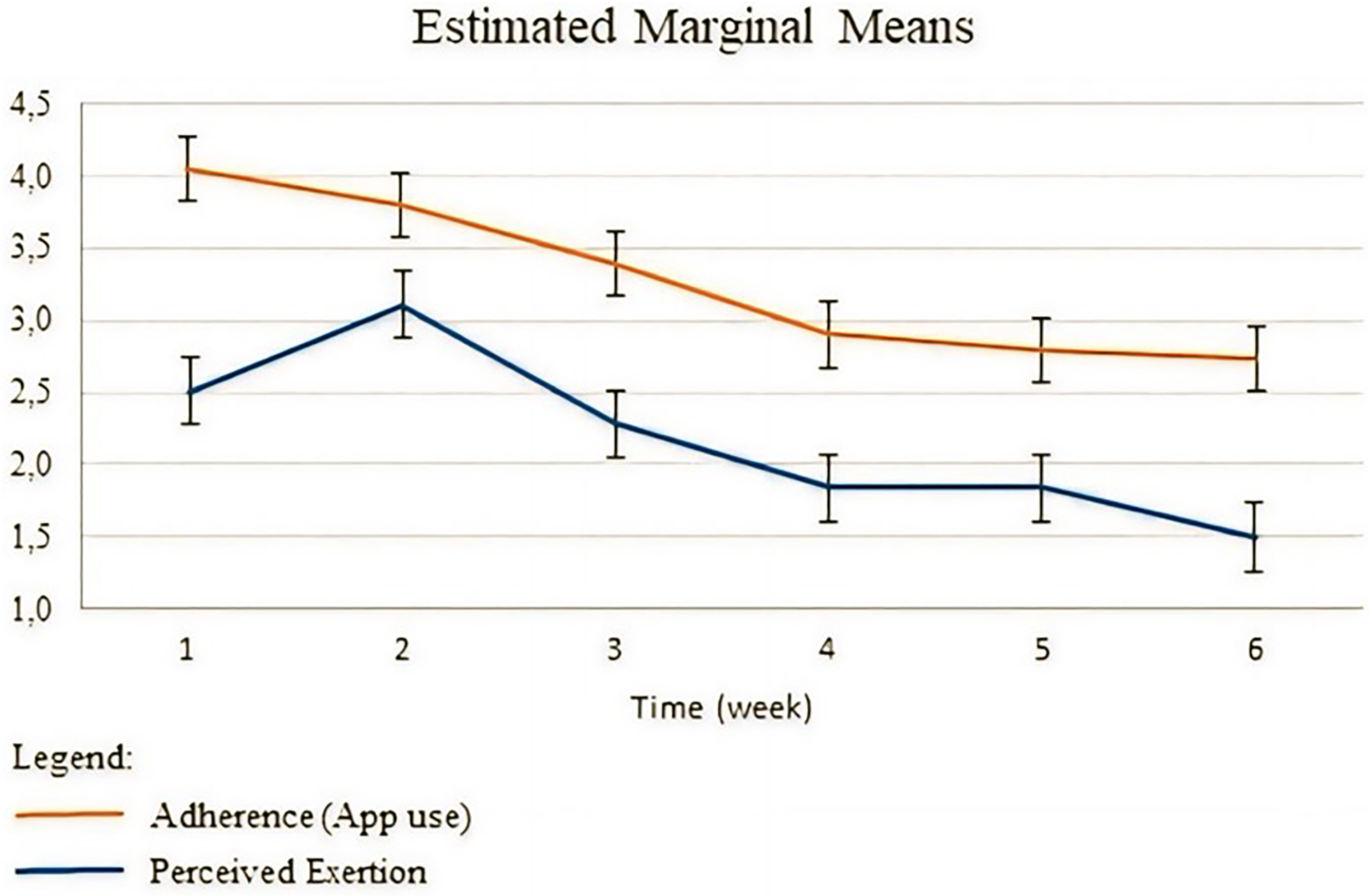
Over-time changes in adherence (i.e. apps’ use) and perceived exertion during the intervention.
No differences were found at baseline in perceived exertion between girls and boys. The highest value of perceived exertion was observed in week 1 (4.1, 95% CI: 3.6 to 4.5), with a significant over-time decrease found in week 4 (Δ−1.1, 95% CI: −1.9 to −0.4, p < .001), 5 (Δ−1.3, 95% CI: −2.1 to −0.4, p < .001), and 6 (Δ−1.3, 95% CI: −2.1 to −0.6, p < .001) compared to week 1 (Figure 1).
Effect on body composition
No significant over-time differences were found in BMI, BMI z-score, BFM, or MM, neither at week 6 (intervention) nor at week 12 (follow up).
A time-by-sex interaction was found in MM, with boys showing a higher MM increase at week 6 (intervention) compared to girls (β = 1.7, 95% CI: 0.0 to 3.3, p = .030) (Table 2).
Participants’ over-time changes in body composition, movement behaviors, and nutritional behaviors.
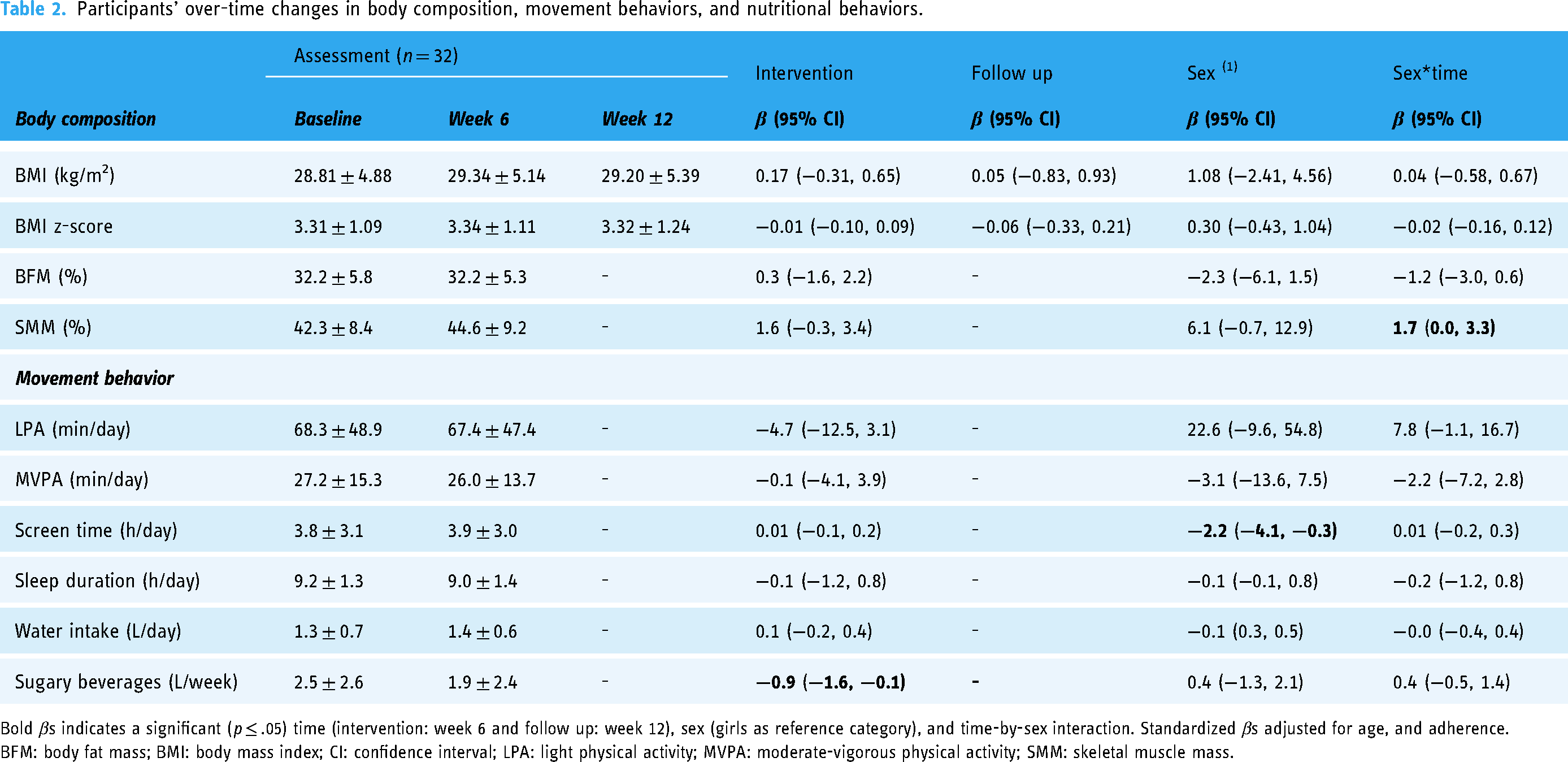
Bold βs indicates a significant (p ≤ .05) time (intervention: week 6 and follow up: week 12), sex (girls as reference category), and time-by-sex interaction. Standardized βs adjusted for age, and adherence.
BFM: body fat mass; BMI: body mass index; CI: confidence interval; LPA: light physical activity; MVPA: moderate-vigorous physical activity; SMM: skeletal muscle mass.
Effect on movement behaviors
At baseline, boys showed in average −2.2 hours/day of screen time compared to girls (95% CI: −4.1 to −0.3, p = .023). No other sex differences were found at baseline.
No significant over-time changes were found in LPA, MVPA, screen time, or sleep duration (Table 2).
Effect on nutritional behaviors
No significant differences were found at baseline in nutritional behaviors between girls and boys. In general, an over-time decrease in sugary beverage intake was observed (Δ−0.9, 95% CI: −1.6 to −0.1, p = .019), with no sex differences observed. No over-time differences were found in water intake.
Children and parents’ perceptions
None of the children or parents perceived impairments in nutritional behavior, general wellbeing, or fitness as a consequence of the intervention.
Overall, 64.5% of children perceived improvements in nutritional behavior (n = 20) and general wellbeing (n = 20), and 18.8% (n = 2) in fitness, with no significant sex differences observed in these perceptions.
Most parents perceived no improvements in nutritional behavior (90.9%, n = 30), general wellbeing (77.4%, n = 24), or fitness of their child (81.3%, n = 26).
Discussion
Multicomponent interventions, including in-person contact and mHealth support (e.g. through apps), seem to be more effective than stand-alone interventions when targeting PA/exercise behavior,19,20 yet evidence on the topic is scarce among children with obesity, 16 and parents may be reluctant regarding apps use. 21
This study aimed to add to the existent literature by exploring the utility of the HIIT app as a remote exercise support strategy in children with obesity through the assessment of adherence, possible effect on obesity-related outcomes, and perceptions of its use, to support counseling and improve the treatment of children with obesity.
Adherence to the HIIT app was low, with children engaging with the app 2.5 times per week, accounting for only half of the required use, and no children reporting continuing use of the app during the follow-up phase. Furthermore, an attrition of 13.7% was recorded during the study. Although this attrition seems to be below other studies, 26 it should be considered that this was a short-duration study (12 weeks, including follow up), which could contribute to the lower attrition rate observed.
According to study results, no significant over-time changes were found in BMI or BMI z-score after intervention or at follow up. One possible explanation for this may be the short duration of the intervention and associated low volume, with only 6 weeks long and exercise sessions of 10 min. Although it has been previously suggested that interventions of at least 4 weeks duration may be effective in improving BMI and BMI z-score, 27 the effect of exercise on BMI may not depend only on intervention duration but mostly on exercise volume (i.e. duration, frequency, and intensity). 28 Indeed, the higher app use was 3.4 times/week (equivalent to ≈34 min/week or ≈5 min/day), with study participants reporting engaging in approximately half of the physical activity recommended time (26 ± 13.7 min compared to the recommended 60 minutes of MVPA per day), even when factoring in the app using time; and the perceived intensity of the exercise sessions was low, with the highest value of perceived exertion of ≈4 (0–10).
Independently of the effect of exercise on BMI, exercise is known to have a selective effect on body composition, improving MM and decreasing BFM. 29 Even so, no over-time changes were found in MM or BFM after the intervention, which the low exercise volume may also explain.
Moreover, no changes were found in any movement or nutritional behaviors analyzed, except sugary-beverage intake, which decreased after the intervention. There is no consistent evidence that exercise interventions can increase overall PA among children with obesity, 23 a particular population probably with a more marked inactive behavior. 30 Regarding the decrease in sugary beverage intake, study results are not in line with the study of Bibiloni et al., 31 which reported a positive association between beverage intake and PA in adolescents. Yet, it should be noted that the study of Bibiloni et al. 31 used a sample of adolescents, not children, of all BMI categories (25% with overweight or obesity), limiting the comparison between the two studies. In line with the social cognitive theory, the decrease in sugary beverages intake may have been influenced by intervention, with the engagement in one healthy behavior, that is, exercise, leading to an increase in the awareness and motivation for other health-related behaviors, such as reducing sugary beverage consumption.32,33
Although none of the children or parents perceived impairments as a consequence of apps’ use, children and parents showed distinct perceptions regarding its effect on nutritional behavior, general wellbeing, and fitness. Most children, but not parents, perceived improvements in nutritional behavior and general wellbeing. Although it may not be considered a barrier to the apps’ use, as previous studies suggest, 21 parents’ perception can reflect their engagement in the study and supporting behavior among their children, influencing study results in turn.
Although other factors, such as the app's unattractiveness, may also have contributed to the low adherence observed, 34 parent unengagement seems to have played the most relevant role in adherence. In fact, parents perceived no app-related improvements in their child, possibly discrediting any eventual positive effect of the app. It has been suggested that parents act as role models for their children regarding the adoption/engagement with mHealth apps. 18
The small sample size and the absence of a control group are the two main study limitations. Indeed, without a control group, it is impossible to assume that any outcome change was a consequence of the intervention. Also, although the semistructured interview guide was developed according to expert judgment procedures, no data analysis from pilot testing or validation was performed, which may be considered a study limitation. Other limitations include the use of a single HIIT app, not allowing the generalization of the results for different apps; the subjective assessment of PA, and the lack of data regarding week 12 assessments, not allowing in-depth follow-up analysis.
Despite the acknowledged limitations, this study adds to the existing literature by exploring the utility of the HIIT app as a remote exercise support strategy in children with obesity. Nevertheless, more studies, with larger samples and with the inclusion of a control group and other apps, are needed to explore the utility of HIIT apps as a remote exercise support strategy for children with obesity further.
Conclusion
This study suggests that although feasible, the 6-week effect of HIIT app use is modest or absent regarding body composition, movement, and nutritional behavior change. Family involvement may be crucial to improve intervention adherence and behavior change.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241291386 - Supplemental material for Utility of a high-intensity interval training app as a remote exercise support strategy in children with obesity: An exploratory study of adherence, effect, and perceptions of its use
Supplemental material, sj-docx-1-dhj-10.1177_20552076241291386 for Utility of a high-intensity interval training app as a remote exercise support strategy in children with obesity: An exploratory study of adherence, effect, and perceptions of its use by Fábio de Freitas, Maria Ângela Antônio, Mariana R Zago, Mariana Zambon and António Videira-Silva in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank Mariana Zambon for her assistance and guidance in this research.
Contributorship
AV-S and FF researched the literature and designed the study. FF participated in developing the protocol, obtaining ethical approval, recruiting patients and AV-S in analyzing the data. FF wrote the first version of the manuscript. All authors contributed to the literature search, writing, reviewing, and editing of the manuscript.
Ethical approval
This study was approved by the Research Ethics Committee of the State University of Campinas, by following the norms established by Resolution 466/2012 of the National Health Council.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Guarantor
FF
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.