
Abstract
Introduction
In recent years, mobile health (mHealth) applications have revolutionized healthcare by improving accessibility, boosting patient engagement, and simplifying health management processes. However, despite their increasing popularity, there is still a significant lack of understanding regarding how demographic factors shape user perceptions and interactions with these tools.
Objective
This research aims to assess user satisfaction and the perceived value of the Sehhaty app among residents of Hail City, Saudi Arabia, while also examining how demographic variables influence user engagement. The findings emphasize the necessity of incorporating demographic insights into the design of mHealth applications and introduce the Integrated Digital Health Engagement Model (IDHEM) as a novel theoretical framework.
Method
A cross-sectional study design was implemented, using an electronic survey distributed to 333 users of the Sehhaty app. The survey evaluated key aspects such as ease of use, user satisfaction, system information organization, and perceived usefulness. Convenience sampling was utilized to ensure participation from a wide range of demographic groups. Descriptive statistics and Pearson correlation analysis were conducted to explore the relationships between demographic characteristics and user perceptions.
Results
The study revealed high levels of user satisfaction, with 94% of participants reporting that the app was easy to use, resulting in an overall satisfaction score of 4.56 out of 5. Significant correlations were identified between demographic factors like age, gender, and employment status, suggesting that personalized development approaches can significantly enhance user engagement.
Conclusion
The Sehhaty app shows great promise in enhancing healthcare access and management, especially among younger and female users. The findings underscore the importance of considering demographic factors in the design of mHealth applications to better meet diverse user needs. Additionally, this study introduces the IDHEM, providing a new framework for understanding user behavior and guiding the development of future digital health solutions.
Keywords
Introduction
Over the last decade, mobile health (mHealth) applications have emerged as transformative tools in modern healthcare systems, revolutionizing the way individuals access and manage their health. mHealth refers to the use of mobile devices, such as smartphones and tablets, along with software applications (apps), to support medical and public health practices. These apps can provide a wide range of services, including health education, remote monitoring, medication reminders, appointment scheduling, and telemedicine consultations. By leveraging wireless communication technologies, mHealth bridges gaps in healthcare accessibility, particularly in underserved or remote areas, and empowers patients to take an active role in managing their health. Despite these advancements, challenges remain in ensuring that these digital solutions are user-friendly, culturally appropriate, and tailored to diverse populations.1,2 For instance, while diabetes-focused apps have demonstrated measurable improvements in glycemic control and overall quality of life,3,4 ongoing refinement is essential due to evolving technology and changing user expectations. Research highlights that usability, credible content, and opportunities for user feedback are critical factors influencing the successful adoption and clinical impact of mHealth apps.5,6
The influence of specific demographic factors on user perceptions and engagement with mHealth apps remains only partially understood. While age, gender, and usage frequency are widely acknowledged as critical determinants of user satisfaction, there is limited understanding of how factors like marital status, employment status, and regional characteristics affect the effectiveness of these applications.7,8 The distinct cultural and social environment of Hail City, Saudi Arabia, provides an ideal setting to investigate how local dynamics influence the acceptance and utilization of mHealth tools. Bridging these gaps is essential for developing digital health solutions that are more personalized and effective in addressing the diverse needs of users.9,10 For example, studies have shown that women tend to be more proactive in seeking health information and utilizing health technologies compared to men.11,12 Similarly, older adults may face challenges in adopting mHealth apps due to unfamiliarity with digital tools or concerns about privacy. 13 Understanding these nuances can help developers design apps that cater to the unique preferences and requirements of different demographic groups.
The Sehhaty app, a comprehensive healthcare platform tailored for residents of Hail City, offers functionalities such as appointment scheduling, medication reminders, telemedicine consultations, and access to health-related information. Previous assessments indicate high user satisfaction, emphasizing its ease of use and ability to meet user requirements. 14 This study evaluates user satisfaction and perceived utility of the app, focusing on demographic variables and user feedback that shape engagement. For instance, 65% of users rely on the app for online appointments, while 40% use it for telemedicine consultations. 15 These statistics highlight the app's widespread adoption and utility in facilitating remote healthcare access. Additionally, the app has been praised for its intuitive interface and well-organized information, which contribute significantly to user comfort and satisfaction. However, some participants noted that while the app facilitates communication with healthcare providers, it could still improve in terms of interactivity.16,17 Addressing this feedback can further enhance user satisfaction and engagement.
The selection of the health belief model (HBM), theory of planned behavior (TPB), social cognitive theory (SCT), technology acceptance model (TAM), and self-determination theory (SDT) was informed by a systematic review of existing literature on user engagement in digital health applications. HBM was chosen because it emphasizes perceived susceptibility, severity, benefits, and barriers, which are critical factors influencing users’ decisions to adopt mHealth tools. 18 TPB highlights the role of attitudes, subjective norms, and perceived behavioral control in shaping user intentions, making it particularly relevant for understanding engagement behaviors. 19 SCT provides insights into observational learning, self-efficacy, and reinforcement, which are essential for sustained app usage. 20 TAM focuses on perceived ease of use and perceived usefulness, two key determinants of technology acceptance identified in prior studies. 21 Finally, SDT underscores the importance of autonomy, competence, and relatedness in fostering intrinsic motivation, which is crucial for long-term user engagement. 22 Together, these theories provide a comprehensive foundation for understanding the psychological, social, and technological dimensions of user engagement in mHealth applications
This research also introduces the Integrated Digital Health Engagement Model (IDHEM), a novel framework integrating psychological, social, and technological dimensions to understand user behavior in digital health contexts. Understanding user satisfaction and perceived utility is crucial because these factors directly influence how users interact with mHealth applications and whether they continue to use them over time. For instance, if users find an app easy to navigate (ease of use) and perceive it as beneficial for managing their health (perceived utility), they are more likely to engage with the app consistently. These insights lay the groundwork for developing mHealth solutions that are not only functional but also tailored to meet the diverse needs of different user groups. Drawing on theories like the HBM, TPB, SCT, TAM, and SDT, IDHEM aims to guide the development of personalized mHealth solutions.23,24 Specifically, data on how users perceive the app's usability, content organization, and overall value will help refine the components of IDHEM, ensuring that it addresses real-world challenges faced by diverse populations. For example, if the study reveals that older adults struggle with certain app features due to complexity, IDHEM can incorporate strategies to simplify interfaces for this demographic. Similarly, if gender differences emerge in terms of perceived usefulness, IDHEM can guide the development of gender-sensitive interventions. Ultimately, this research emphasizes the importance of continuously assessing and refining digital health tools to ensure their relevance and effectiveness in contemporary healthcare systems.
Method
Study design
This research utilized a cross-sectional approach to assess user satisfaction and engagement with the Sehhaty mobile health (mHealth) application among residents of Hail City, Saudi Arabia. A cross-sectional design was selected because it enables data collection at a specific point in time, making it ideal for capturing a snapshot of user perceptions and behaviors. While this method is effective for identifying relationships between variables, it does not allow for causal conclusions—a limitation acknowledged in this study. To address this gap, future studies could incorporate longitudinal designs to monitor changes in user satisfaction and engagement over time.
Study setting
The study was conducted in Hail City, Saudi Arabia, a region with an estimated population of 600,000 residents, comprising urban and semi-urban areas. Known for its high smartphone penetration and active adoption of digital health tools, Hail City provided an ideal setting to explore how cultural and social factors influence mHealth app usage. The study focused on the Sehhaty app, leveraging the city's diverse demographics to ensure relevant findings. Data collection occurred from January 2024 to December 2024, with participant recruitment between January and March 2024. Follow-up reminders were sent 1 week after survey distribution, with two additional reminders spaced 3 days apart. This timeframe minimized seasonal variations in app usage while maximizing participant engagement. Future studies may expand to rural areas or other regions to enhance generalizability
Sample size and sampling method
The target population consisted of individuals who had used the Sehhaty app in Hail City. The sample size was determined to be 333 participants, calculated using statistical methods to ensure adequate representation. Specifically, a power analysis was performed to estimate the required sample size, assuming an effect size of 0.3, a significance level (α) of 0.05, and a power (1-β) of 0.80.
Convenience sampling was used to efficiently collect data while ensuring representation across various demographic groups, such as age, gender, marital status, employment status, and education level. Although convenience sampling is cost-effective and practical, it may introduce selection bias. To minimize this risk, efforts were made to include participants from diverse backgrounds, and the demographic distribution of the sample was compared to the broader population of Hail City to evaluate representativeness.
Study duration
The study was conducted over a specific time period to ensure comprehensive data collection from participants using the Sehhaty mobile health (mHealth) application in Hail City, Saudi Arabia. Data collection occurred between January 2024 and December 2024. This timeframe was selected to capture a representative snapshot of user perceptions and behaviors at a particular point in time, consistent with the cross-sectional design of the study. The choice of this specific duration aimed to maximize participant availability and engagement while minimizing potential seasonal variations in app usage that could affect the study outcomes. During this period, electronic surveys were distributed via email and social media platforms to gather responses from a diverse user base. Follow-up reminders were sent 1 week after the initial survey distribution to enhance response rates, with a total of two reminders spaced 3 days apart. All data collection activities, including the receipt of completed surveys, were concluded by December 2024, ensuring a structured and timely research process. This defined timeframe allowed for efficient data collection and analysis while maintaining the integrity and relevance of the findings within the rapidly evolving landscape of mHealth applications. Future studies may consider longitudinal designs to observe changes in user satisfaction and engagement over extended periods.
Data collection
Data were gathered using a structured survey questionnaire distributed electronically via email and social media platforms. This approach enabled broad participation and ensured responses from a diverse user base. The survey was hosted on Google Forms, a secure platform that guaranteed data anonymity and confidentiality. Participants were provided with a link to the survey and informed that their involvement was voluntary and confidential.
Survey development
The questionnaire was developed based on existing literature related to user satisfaction and mHealth applications. It underwent a rigorous review process, including:
The final questionnaire included four main sections:
Additionally, demographic information was collected, including age, gender, nationality, marital status, place of residence, employment status, frequency of app use, and education level.
The questionnaire was developed based on existing literature and underwent expert review, pilot testing with 30 participants, and cognitive interviewing to ensure clarity and validity. The final version used a 5-point Likert scale for most items, measuring agreement or satisfaction from 1 (“Strongly Disagree”) to 5 (“Strongly Agree”). It included 34 questions across four domains: Ease of Use (8 items), User Satisfaction (7 items), System Information Arrangement (9 items), and Perceived Usefulness (10 items). Additionally, eight demographic questions were included, bringing the total to 42 questions. A points-based scoring system was applied, with domain-specific scores calculated by averaging responses, and an overall satisfaction score derived similarly. This approach ensured consistency and meaningful comparisons between domains.
Follow-up practices
To enhance the response rate, follow-up reminders were sent to participants 1 week after the initial survey distribution. These reminders were delivered via email and social media platforms, encouraging participants to complete the questionnaire. A total of two reminders were sent, spaced 3 days apart, to maximize participation without overwhelming potential respondents.
Subject inclusion and exclusion criteria
Inclusion criteria:
Residency: Participants must be residents of Hail City, Saudi Arabia. App usage: Individuals who have used the Sehhaty mobile health (mHealth) application. Age: Participants should be at least 18 years old. Consent: Willingness to provide informed consent for participation in the study.
Exclusion criteria:
Non-users: Individuals who have not used the Sehhaty app were excluded from the study. Age below 18: Participants younger than 18 years old were not included. Incomplete surveys: Responses from participants who did not complete the survey were excluded from the analysis. Non-residency: Individuals not residing in Hail City were excluded to maintain the regional focus of the study.
These criteria ensured that the sample consisted of individuals who could provide relevant insights into the user experience and satisfaction with the Sehhaty app within the specified demographic and geographic context. Convenience sampling was employed to gather a diverse range of participants while adhering to these criteria.
Statistical analysis
Data analysis was performed using SPSS version 28.0. Descriptive statistics were used to summarize the data, identifying means, standard deviations, frequencies, and percentages to highlight general trends in user satisfaction and engagement.
To explore relationships between variables, Pearson correlation analysis was conducted to assess the significance of associations between demographic factors (e.g. age, gender, marital status, employment status) and key variables such as ease of use, system information arrangement, and perceived usefulness. Assumptions of normality and linearity were tested prior to conducting correlation analyses, and no significant violations were observed.
Structural equation modeling (SEM) was employed to examine the complex relationships between latent constructs, including Ease of Use, System Information Arrangement, Perceived Usefulness, and User Satisfaction. SEM was conducted using AMOS version 28.0, and model fit was evaluated using indices such as CFI, TLI, RMSEA, and SRMR. SEM was chosen because it allows for the simultaneous analysis of multiple relationships, providing deeper insights into user behavior.
ANOVA and independent samples t-tests were conducted to compare group differences across demographic subgroups, offering insights into how factors such as age, gender, marital status, and employment status influence user perceptions. Homogeneity of variance was assessed using Levene's test, and post-hoc analyses were performed where appropriate.
Validity evidence
The reliability of the questionnaire was confirmed through high Cronbach's alpha scores:
0.916 for ease of use and satisfaction, 0.933 for system information arrangement, 0.935 for perceived usefulness, 0.942 overall, indicating strong internal consistency of the measurement scales.
Content validity was ensured through expert review and cognitive interviewing, while construct validity was supported by the significant correlations observed between key variables in the analysis.
Ethical considerations
This study was conducted in accordance with ethical guidelines and received approval from the Research Ethics Committee (REC) at the University of Hail, with the approval dated 18/3/2024. The ethics waiver number provided by the REC is [H-2024-138].
Informed consent process
Obtaining written informed consent from participating subjects is almost always required, regardless of the nature of the study. For this research, written informed consent was obtained from all participants or their legally authorized representatives prior to their involvement in the study. Participants were provided with comprehensive information about the study's objectives, procedures, potential risks, and benefits. They were assured that their participation was entirely voluntary and that they had the right to withdraw from the study at any stage without facing any penalties or consequences. To ensure data security and confidentiality, all responses were anonymized, and access to the collected data was restricted solely to the research team. The data were stored on password-protected devices, further safeguarding participant privacy. In cases where obtaining written informed consent was not feasible (e.g. due to logistical constraints), this requirement was formally waived by the Institutional Review Board (IRB). The IRB determined that the study posed minimal risk to participants and that the research could proceed without compromising ethical standards. This waiver was granted in compliance with applicable regulations and was documented in the study records. By clearly outlining these ethical processes, the study aimed to ensure that the rights and welfare of participants were protected while maintaining the integrity and relevance of the findings within the rapidly evolving landscape of mHealth applications. Future studies may consider additional measures to enhance ethical compliance and participant protection.
Management of missing data
To address missing data, pairwise deletion was applied for correlation analyses, while listwise deletion was utilized for SEM. Sensitivity analyses were performed to confirm that the methods used for handling missing data did not substantially affect the study's outcomes.
Limitation
Although this study provides valuable insights, it has several limitations. The cross-sectional design prevents the establishment of causal relationships, and the use of convenience sampling may limit the generalizability of the findings. Additionally, reliance on self-reported survey data introduces the risk of response biases, such as social desirability or recall errors. Conducted exclusively in Hail City, the study's results may reflect local cultural and social dynamics, potentially restricting their applicability to other populations. Future research should address these limitations by adopting longitudinal designs, randomized sampling methods, and mixed-methods approaches to validate and expand the findings while exploring the scalability of the IDHEM across diverse contexts.
Results
Participant demographics
The demographic characteristics of the participants are summarized in Table 1 and visually represented in Figure 1. A total of 333 participants completed the survey, with the majority being young adults aged 18–28 years (55.3%), followed by those aged 29-50 years (42.3%). Only a small proportion of participants were aged 51–65 years (2.4%), and none were older than 65. The sample was predominantly female (94.0%) and consisted entirely of Saudi nationals. Most participants were married (55.3%) and resided in Hail City (81.7%). Regarding employment status, slightly more than half were not employed (51.4%), while 48.6% were employed. The majority of participants held at least a bachelor's degree (73.6%), with 10.8% holding a master's degree and 0.9% holding a doctoral degree.
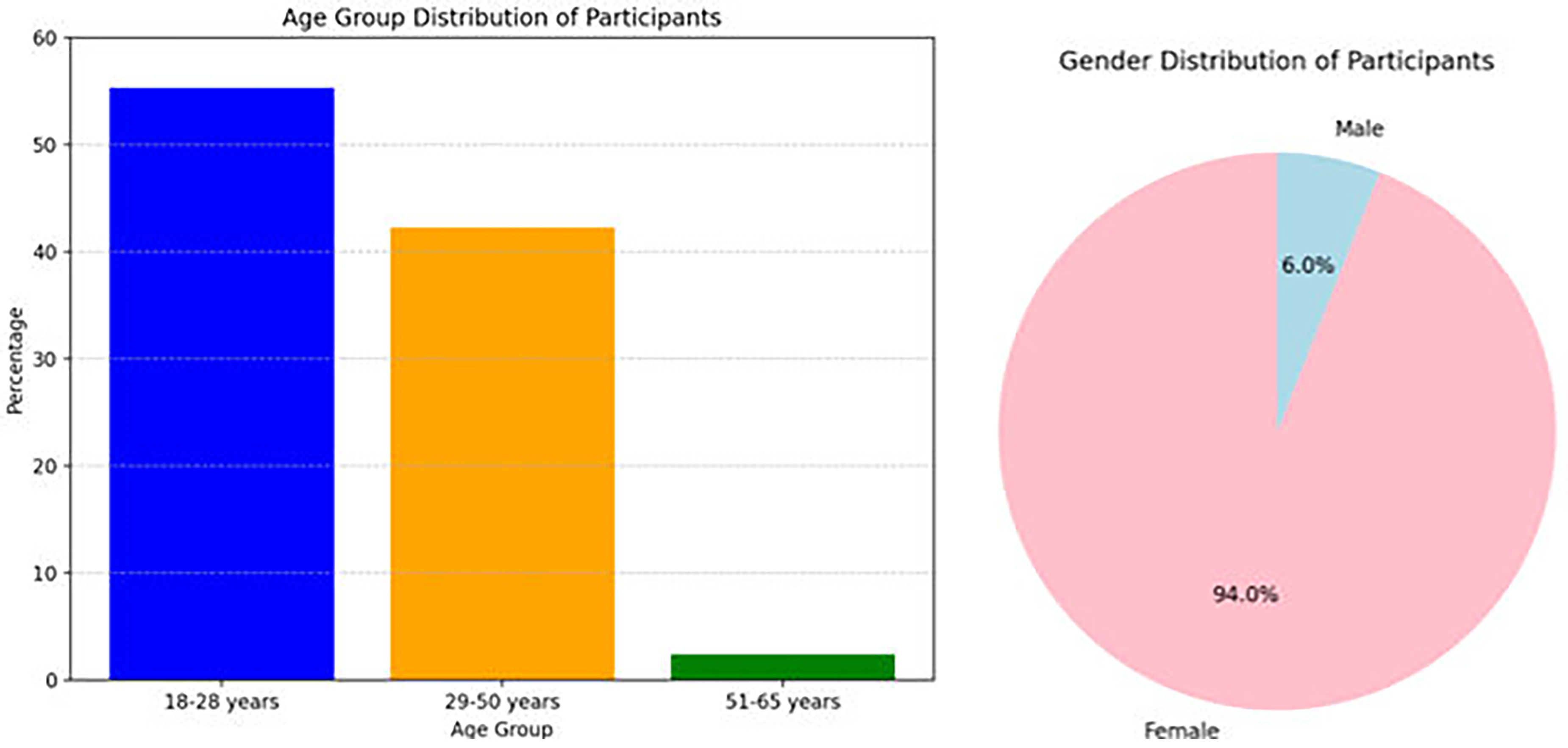
Distribution of age and gender among participants.
Demographic characteristics of participants (n = 333).

Structural equation modeling analysis
To investigate the intricate relationships between variables, we utilized SEM, a powerful statistical method that enables the simultaneous analysis of multiple relationships among latent constructs. The SEM model incorporated four key latent constructs: Ease of Use, System Information Arrangement, Perceived Usefulness, and User Satisfaction. These constructs were hypothesized to influence one another in a structured way, as depicted in the path diagram shown in Figure 2. This diagram visually illustrates the hypothesized relationships, demonstrating how each construct directly or indirectly affects User Satisfaction, which is the primary variable of interest.

Path diagram of the SEM model. SEM: structural equation modeling.
The model showed an excellent fit to the data, supported by the following fit indices: CFI = 0.96, TLI = 0.95, RMSEA = 0.04, and SRMR = 0.03. These values suggest that the model effectively captures the underlying relationships among the constructs. Specifically, CFI and TLI values above 0.90 indicate a good fit, while RMSEA and SRMR values below 0.05 reflect a close alignment between the hypothesized model and the observed data.
The IDHEM model shown in Figure 6 builds upon the findings of the PLS-SEM analysis presented in Figure 2. The SEM results revealed significant relationships between Ease of Use, System Information Arrangement, Perceived Usefulness, and User Satisfaction, highlighting the importance of these constructs in shaping user engagement. For instance, Perceived Usefulness had the strongest total effect on User Satisfaction (β = 0.52, p < 0.001), underscoring its critical role in driving engagement. Similarly, Ease of Use (β = 0.45, p < 0.001) and System Information Arrangement (β = 0.38, p < 0.001) were found to significantly influence satisfaction, emphasizing the need for intuitive design and well-organized information. These findings align with the theoretical underpinnings of HBM, TPB, SCT, TAM, and SDT, which collectively inform the IDHEM framework. Specifically, the SEM model provided empirical support for integrating these theories into a unified framework that captures the complex interplay between psychological, social, and technological factors. IDHEM extends this analysis by incorporating demographic insights and offering practical guidance for tailoring mHealth applications to diverse user populations.
Second, System Information Arrangement also significantly influenced User Satisfaction (β = 0.38, p < 0.001), emphasizing the importance of having well-organized and accessible information within the app to enhance user experience. Lastly, Perceived Usefulness demonstrated the strongest total effect on User Satisfaction (β = 0.52, p < 0.001), highlighting its pivotal role in driving user engagement and satisfaction. This suggests that users who perceive the app as beneficial for managing their health are more likely to be satisfied with its overall functionality and performance. Taken together, these results underscore the interplay of usability, system design, and perceived value in shaping user satisfaction with mobile health applications.
Subgroup analysis
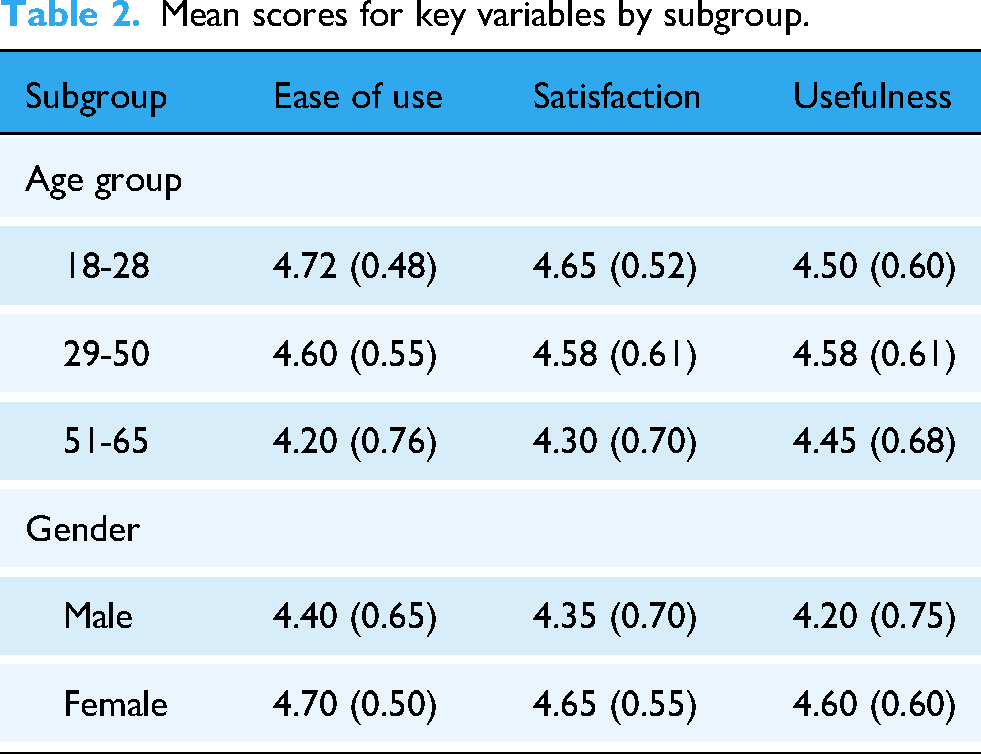
We conducted subgroup analyses to examine differences in user perceptions of the Sehhaty app based on key demographic factors, including age, gender, and health conditions. The results, summarized in Table 2, reveal notable variations in mean scores for Ease of Use, User Satisfaction, and Perceived Usefulness across different subgroups. For instance, younger users aged 18–28 reported the highest mean scores for Ease of Use (4.72 ± 0.48) and User Satisfaction (4.65 ± 0.52), while older users aged 51–65 exhibited lower scores, particularly for Ease of Use (4.20 ± 0.76). Gender-based differences were also evident, with female participants consistently reporting higher scores than their male counterparts across all three variables. These findings are further illustrated in Figure 3, which visually compares mean scores across subgroups, highlighting disparities in user perceptions. Collectively, these results underscore the importance of considering demographic characteristics when designing and optimizing mobile health applications to better meet the diverse needs of users. Such insights can inform targeted improvements to enhance user engagement and satisfaction among specific population groups.
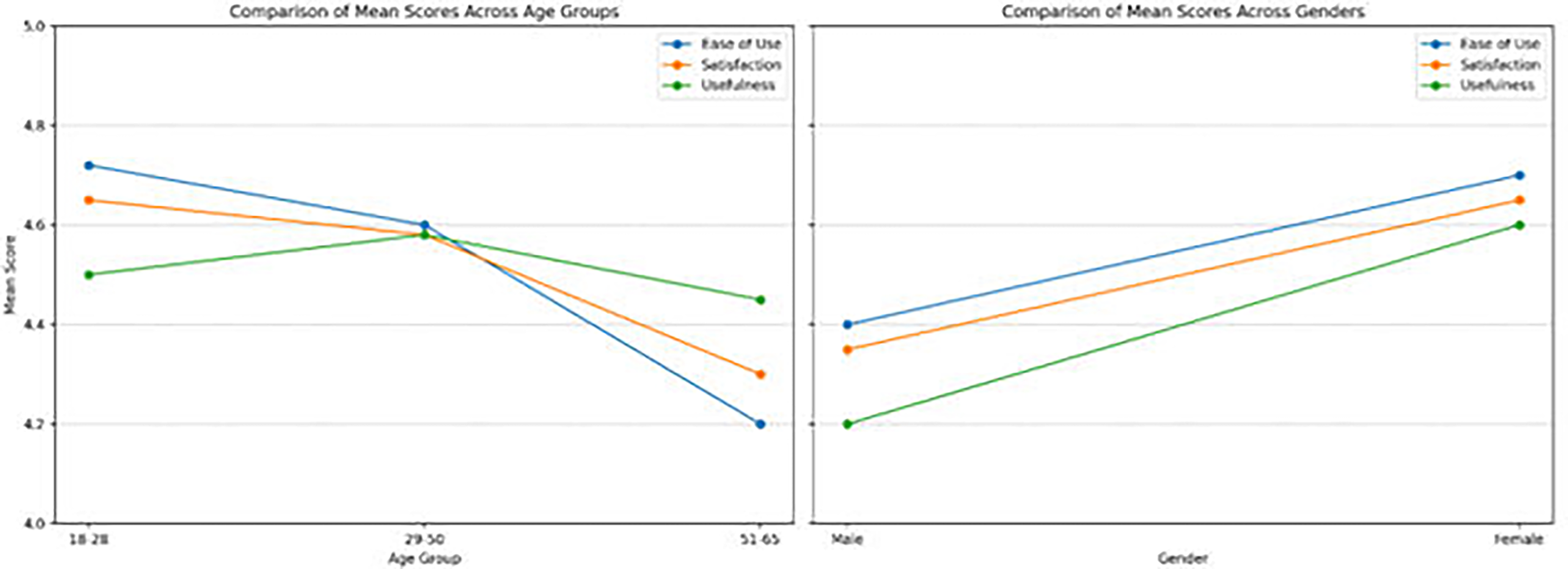
Comparison of mean scores across subgroups.
Mean scores for key variables by subgroup.
Correlation analysis
A Pearson correlation analysis was performed to examine the relationships between demographic factors and key variables, including Ease of Use, User Satisfaction, and Perceived Usefulness. The findings, outlined in Table 3, illustrate the strength and significance of these associations. For example, age exhibited weak correlations with Ease of Use (r = -0.035, p = 0.519), User Satisfaction (r = 0.033, p = 0.543), and Perceived Usefulness (r = 0.071, p = 0.194), indicating that age has minimal to no impact on these variables. Conversely, gender showed small but statistically significant negative correlations with all three variables: Ease of Use (r = -0.12, p = 0.035), User Satisfaction (r = -0.10, p = 0.045), and Perceived Usefulness (r = -0.15, p = 0.020). These results suggest that gender may influence user perceptions, with female participants generally reporting higher scores compared to their male counterparts. To visually represent these relationships, Figure 4 provides a heatmap of the correlation coefficients. The heatmap employs color gradients to emphasize the strength and direction of the correlations, facilitating the identification of patterns and enabling easier interpretation of the data. Overall, these findings highlight the importance of accounting for demographic factors when evaluating user experiences with mobile health applications, as they can significantly affect perceptions of usability, satisfaction, and utility.

Heatmap of correlation coefficients.
Correlation matrix.

ANOVA and independent samples t-test
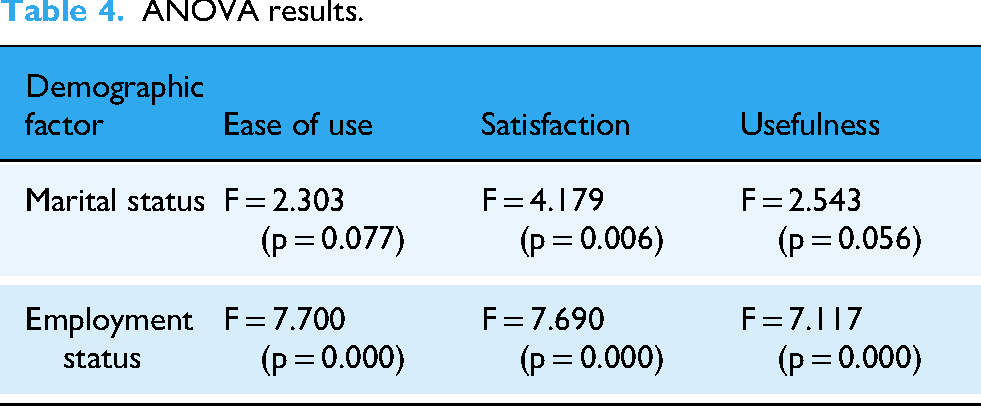
To examine the impact of demographic factors on user perceptions of the Sehhaty app, ANOVA and independent samples t-tests were performed to compare group differences across key variables such as Ease of Use, User Satisfaction, and Perceived Usefulness. The results, summarized in Table 4, reveal significant differences based on demographic characteristics. For instance, marital status showed a notable impact on User Satisfaction (F = 4.179, p = 0.006), indicating that individuals with different marital statuses reported varying levels of satisfaction with the app. Similarly, employment status had a highly significant influence on all three variables, with p-values of 0.000 for Ease of Use, User Satisfaction, and Perceived Usefulness. This suggests that employed and non-employed users differ significantly in their perceptions of the app's usability, satisfaction, and overall utility. These findings are further illustrated in Figure 5, which presents bar charts comparing mean scores across demographic groups. The visual representation highlights the magnitude of these differences, emphasizing the importance of considering demographic factors when designing and optimizing mHealth applications to better meet diverse user needs. Collectively, these results underscore the role of individual characteristics, such as marital and employment status, in shaping user engagement and satisfaction with digital health tools.

Bar chart of group differences.
ANOVA results.
The study revealed high levels of user satisfaction with the Sehhaty app, particularly among younger users, females, and frequent users. Significant differences were observed across demographic subgroups, with marital status and employment status influencing user perceptions. The SEM model highlighted the critical role of Perceived Usefulness in driving User Satisfaction, underscoring the importance of designing apps that align with users’ health needs. These findings provide valuable insights for tailoring mHealth applications to diverse populations and improving their effectiveness in healthcare delivery.
Discussion
This study evaluated user satisfaction and perceived usefulness of the Sehhaty mobile health (mHealth) application among residents of Hail City, Saudi Arabia. The findings demonstrate high levels of satisfaction with the app's ease of use, system information arrangement, and overall utility, particularly among younger users, females, and frequent users. Demographic factors such as marital status, employment status, and gender significantly influenced user perceptions, underscoring the importance of tailoring mHealth applications to diverse populations. The introduction of the IDHEM provides a novel framework for understanding user engagement by integrating psychological, social, and technological factors.
The users expressed significant satisfaction with the Sehhaty app, as 94% of them agreed or strongly agreed that it was user-friendly. This resulted in an average satisfaction score of 4.56 out of 5. These findings are consistent with earlier studies that emphasize the importance of usability as a key element in the acceptance and utilization of mHealth applications.25–28 The intuitive interface and well-organized information contributed significantly to user comfort and satisfaction. Furthermore, users found the app efficient in terms of time required for use, suggesting that it fits seamlessly into their daily routines. These findings underscore the importance of prioritizing user experience in the design of mHealth apps to enhance adoption and sustained engagement.29,30
The majority of users (88.64%) expressed satisfaction with the app's system information arrangement, indicating it was user-friendly and efficient. Participants appreciated features such as error recovery, consistent navigation, and comprehensive functionality, which are consistent with prior studies emphasizing the importance of robust design in enhancing user experience.31,32 Moreover, most users (88.38%) found the app highly useful for their health and well-being, improving access to healthcare services and aiding in health management. These results align with studies showing that mHealth apps can significantly improve patient engagement and healthcare outcomes.33,34 However, some participants noted that while the app facilitated communication with healthcare providers, it could still improve in terms of interactivity.35,36 Addressing this feedback could further enhance user satisfaction and engagement.
Correlation analysis revealed significant relationships between demographic factors and user perceptions. Notably, age positively correlated with both system information arrangement and perceived usefulness, indicating that older users found the app more beneficial and well-organized.37,38 Gender also significantly impacted perceived usefulness, with females rating the app higher than males (p = 0.035). These findings align with previous research suggesting that women tend to be more proactive in seeking health information and utilizing health technologies.39,40 Additionally, marital status, employment status, and frequency of app usage significantly influenced user satisfaction and perceived usefulness, underscoring the need for personalized approaches in app design. 41
The study identified several barriers to frequent app use, including technical issues, lack of internet access, and unfamiliarity with digital tools. 42 Privacy concerns also emerged as a potential deterrent, consistent with prior research highlighting the importance of robust data protection measures and transparent privacy policies.43,44 Despite these challenges, regular users reported improved health management and better access to healthcare services, aligning with studies that emphasize the effectiveness of mHealth tools in promoting healthier behaviors and improving patient engagement.45,46 Addressing these barriers through user education, technical support, and transparent privacy practices can significantly enhance the app's adoption and effectiveness.
This study makes several important theoretical contributions. First, it introduces the IDHEM, which integrates five established theories—HBM, TPB, SCT, TAM, and SDT—to provide a comprehensive framework for understanding user behavior in digital health contexts. This integration addresses a significant gap in the literature by capturing the interplay between psychological, social, and technological factors in a holistic manner. Second, the study highlights the importance of demographic factors in shaping user perceptions and interactions with mHealth apps, offering new insights into how these factors can be incorporated into theoretical models.34,47 Finally, the findings extend prior research by demonstrating the critical role of Perceived Usefulness in driving User Satisfaction, thereby reinforcing the relevance of TAM in contemporary digital health contexts.
From a managerial perspective, the findings of this study offer valuable guidance for the design and optimization of mHealth applications. First, the results underscore the importance of prioritizing usability and perceived usefulness in app development, as these factors have the strongest impact on user satisfaction. Developers should focus on creating intuitive interfaces and providing features that users perceive as beneficial for managing their health. Second, the study highlights the need for personalized approaches to app design, particularly in addressing the unique needs of different demographic groups.33,48 For example, interactive features and culturally tailored content can enhance engagement among older adults and male users.49,50 Third, the identification of barriers such as technical issues, lack of internet access, and privacy concerns provides actionable insights for improving app adoption and effectiveness. By addressing these challenges through user education, technical support, and transparent privacy practices, stakeholders can enhance the overall value and impact of mHealth solutions.
Introduction of the Integrated Digital Health Engagement Model
Findings suggest that tailoring mHealth apps to address demographic differences can enhance user engagement and satisfaction. For instance, incorporating interactive features, such as gamification and real-time feedback, can improve usability among older adults by addressing psychological motivators like autonomy and competence. 35 Similarly, personalized content, such as culturally tailored health recommendations or gender-specific messaging, has been shown to increase relevance and adoption among diverse populations. 51 These insights are supported by prior studies indicating that interactive features enhance user motivation and sustained engagement, 25 while personalized content fosters a stronger emotional connection with the app.52–54 The IDHEM (Figure 6) introduced in this study offers a novel approach by integrating elements from established health behavior theories and TAMs. IDHEM combines psychological, social, and technological factors, presenting a holistic framework to understand and enhance user engagement with digital health applications.18,55,56 By incorporating theories such as the HBM, TPB, SCT, TAM, and SDT, IDHEM not only broadens the understanding of user behavior but also guides the development of more personalized, user-friendly, and effective digital health solutions.25,35 This comprehensive framework ensures that health apps are not only accessible but also tailored to meet the unique needs and behaviors of diverse user populations

Integrated digital health engagement model (IDHEM).
Limitations and future directions
Although this study offers significant insights, it is not without limitations. The cross-sectional approach prevents the establishment of causal relationships, and the reliance on convenience sampling may reduce the findings’ generalizability. To address these issues, future studies should adopt innovative approaches, such as using wearable technology to collect real-time behavioral data or conducting field experiments to test the effectiveness of new app features. 57 Additionally, the dependence on self-reported survey data may lead to response biases, which should be mitigated in future investigations through triangulation methods, such as combining surveys with interviews or observational studies. 58 The study was conducted in Hail City, which may have unique cultural and social dynamics influencing the findings. Exploring the applicability of IDHEM in different cultural and regional contexts can provide valuable insights into its scalability and adaptability. For example, cross-cultural studies could reveal whether features like gamification or personalized content have similar impacts in regions with varying levels of digital literacy. 59 Such investigations would enhance the model's flexibility and ensure its relevance across diverse populations.
Conclusion
The study evaluated user satisfaction and perceived usefulness of the Sehhaty app among residents of Hail City, Saudi Arabia, revealing high satisfaction levels with its ease of use, system information arrangement, and overall utility. These findings highlight the app's potential to enhance healthcare accessibility and management, particularly among younger users, females, and frequent users. Demographic factors such as marital status, employment status, and gender significantly influenced user perceptions, underscoring the need for personalized mHealth solutions. The introduction of the IDHEM provides a novel framework that integrates psychological, social, and technological dimensions to guide the development of more effective digital health tools. Despite these insights, the study has limitations, including its cross-sectional design, reliance on convenience sampling, and self-reported data, which may limit generalizability. Future research should address these gaps through longitudinal studies and randomized sampling to validate findings and explore IDHEM's applicability across diverse cultural contexts. Continuous updates to mHealth applications, informed by real-time feedback and technological advancements, are essential to maintaining relevance and effectiveness. By addressing barriers such as technical issues, privacy concerns, and user resistance, mHealth apps like Sehhaty can further enhance engagement and health outcomes.
Footnotes
Acknowledgements
The study highlights the critical role of perceived usefulness in driving user satisfaction with the Sehhaty app, underscoring the importance of designing mHealth applications that align with users’ health needs to enhance engagement and overall effectiveness.
Author Contributions
HMA, RIA, AYG, and RSA contributed to conception and design of the study. HMA, RIA, AYG, and RSA contributed to data extraction and analysis. HMA, RIA, AYG, and RSA contributed to writing (original draft). HMA, RIA, AYG, and RSA contributed to writing (review and editing). HMA contributed to supervision. All authors reviewed and approved the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.