
Abstract

Introduction
Antimicrobial resistance (AMR) is a critical global challenge in managing infectious diseases that affect both humans and animals. The rise in AMR mechanisms has led to widespread treatment failures, posing severe public health and economic burdens. 1 Multidrug resistance (MDR) has been observed in numerous pathogens, including E. coli, Salmonella spp., Staphylococcus spp., and Pseudomonas spp., making infections like pneumonia, tuberculosis, urinary tract infections, gonorrhea, and foodborne diseases increasingly difficult to treat. AMR has significantly reduced the effectiveness of antimicrobial agents and exacerbated the global disease burden. Addressing antimicrobial-resistant pathogens requires the precise identification of susceptible or resistant strains to ensure effective treatment. 2 At the 79th United Nations General Assembly (UNGA) High-Level Meeting on AMR, global leaders emphasized the importance of adopting a One Health approach—integrating human, animal, plant, and environmental health. As part of their commitment, they pledged to reduce AMR-related deaths by 10% annually by 2030, as outlined in a political declaration. 3 AMR presents particularly acute challenges in geriatric healthcare, where multidrug-resistant organisms (MDROs) contribute significantly to increased morbidity, mortality, and healthcare costs. Overuse and misuse of antimicrobials has accelerated the selection and proliferation of resistant strains. 4 Furthermore, frequent hospitalizations and institutionalization expose geriatric patients to environments with a high MDRO prevalence. These settings, combined with invasive procedures, such as urinary catheterization and central line placement, create conditions conducive to colonization and severe infections caused by MDROs. 5
The global disparity in access to effective antibiotics, particularly in low- and middle-income countries (LMICs), exacerbates the AMR crisis by fostering the spread of resistance through suboptimal treatments. 6 In 2021, an estimated 4.71 million deaths were associated with AMR, with 1.14 million directly attributable to AMR. The Global Research on Antimicrobial Resistance (GRAM) Project forecasts that bacterial AMR will cause 39 million deaths between 2025 and 2050, equating to three deaths per minute. The study projects a 67.5% rise in AMR-attributable deaths, from 1.14 million in 2021 to 1.91 million in 2050, while AMR-associated deaths are expected to increase by 74.5%, from 4.71 million to 8.22 million.7,8 The complexity of the worldwide AMR epidemic is oversimplified when it is presented as a problem that can be solved by new technology and innovative approaches, such as artificial intelligence (AI) and machine learning (ML). AI techniques are highly effective in processing vast amounts of data, making them powerful tools for uncovering valuable insights from complex datasets. ML, a branch of AI, leverages statistical algorithms to detect intricate patterns within data and make predictions on new inputs. Deep learning (DL), a specialized subset of ML, utilizes neural networks with multiple interconnected layers to analyze and interpret data. These models are typically trained on task-specific datasets and then applied to new, unseen data for broader generalization. 9
As a result, the integration of AI into healthcare systems presents promising opportunities for addressing the challenges posed by AMR by facilitating tailored interventions, early threat detection, and real-time surveillance, all of which improve the efficacy and efficiency of responses to infectious diseases and antimicrobial stewardship (AMS). 10 In this article, we examine the unique issues surrounding AMR in geriatric patients and exploring the potential role of AI in combating this global health burden.
Applications of artificial intelligence in managing antimicrobial resistance for geriatrics
Artificial intelligence is a promising tool for the control of antimicrobial resistance, 11 especially in geriatric groups where various infectious diseases are prevalent (Table 1). In the following subsections, we discuss the models contribute to AMR control.
Applications of AI in managing AMR for geriatrics.
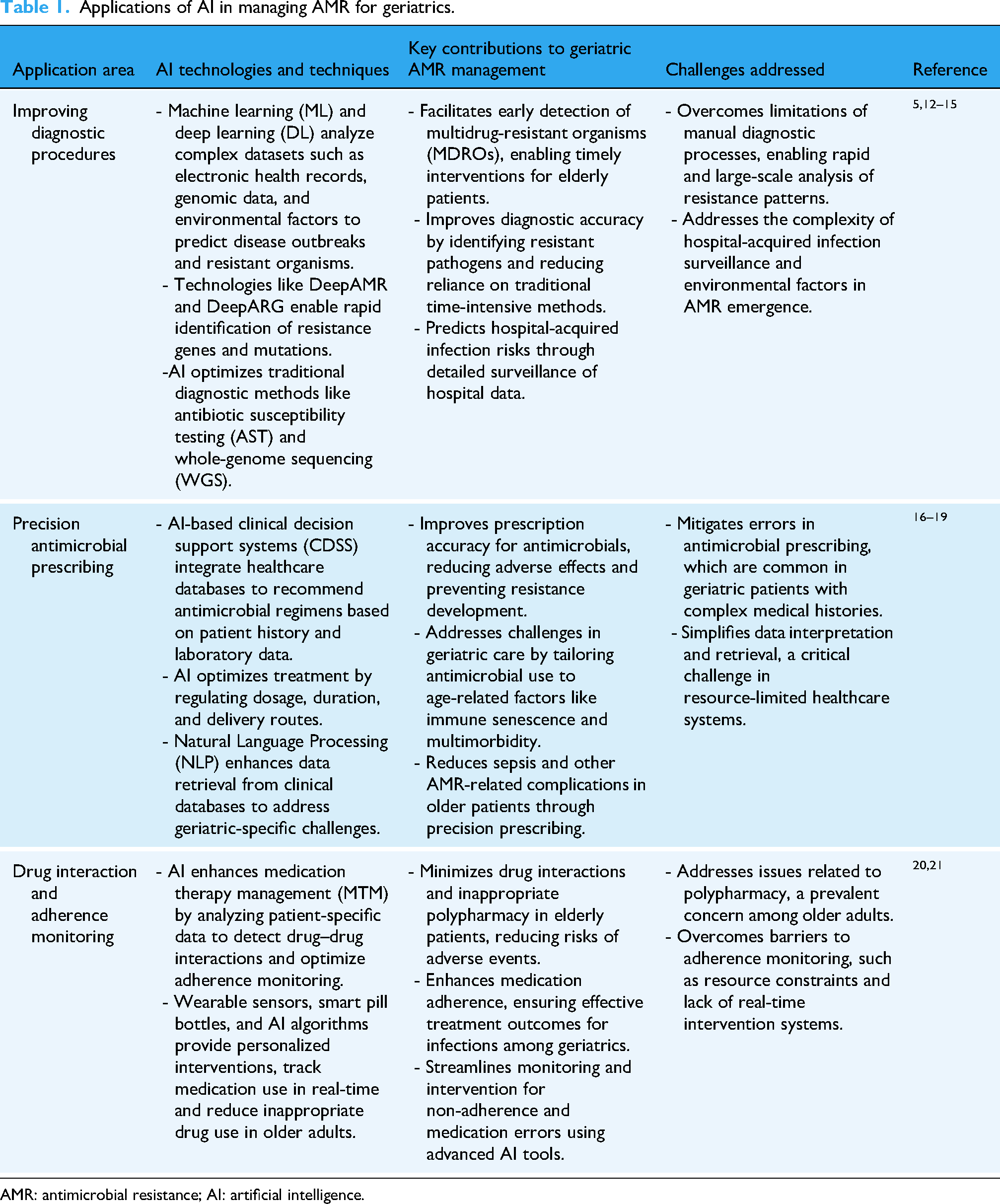
AMR: antimicrobial resistance; AI: artificial intelligence.
Improving diagnostic procedures for infectious diseases
MDROs lead to increased morbidity and mortality and excessive cost of care, especially in high-risk populations such as those suffering from comorbidities and experiencing immune function problems, which require effective and efficient means of predicting the occurrence and spread of these infections. 5 For example, ML has been used to estimate epidemic incidence in regions by studying the genetic material of pathogens and estimating the infection vulnerability of individuals based on their attributes. 12 Furthermore, AI has contributed to the optimization of traditional methods of detecting AMR, including antibiotic susceptibility testing and whole-genome sequencing, by identifying emerging AMR strains and improving overall health system management. 13
DeepAMR and DeepARG are AI technologies that employ DL and analyze DNA sequences to identify resistance genes and mutations, enabling accurate and rapid identification of resistant pathogens and AMR, which is crucial for treatment decisions and public health interventions. 13 DeepAMR is a multi-task DL model which minimizes both reconstruction error (ensuring meaningful feature extraction) and classification error (improving resistance prediction). 14
While, DeepARG can predict antibiotic resistance genes (ARGs) across 30 resistance categories. It consists of two variants: DeepARG-SS, which predicts resistance from short sequence reads (such as those in metagenomic data), and DeepARG-LS, which predicts from full-length ARG-like sequences. 15 Hence, early detection of resistant organisms is a significant step towards tackling AMR among elderly patients, and AI has demonstrated a potential role. 5
Precision antimicrobial prescribing
AI and ML techniques are indispensable for precise antimicrobial prescription, which is a complex process. Appropriately prescribing antimicrobial drugs requires the selection of a suitable treatment for the infectious organism, which includes the regulation of antimicrobial agent concentration, frequency of administration, dosage, duration, and the appropriate route to ensure optimal levels of drug reach the infection site. 16 Hence, the AI-clinical decision support system (CDSS) Markov decision system can review these types of prescriptions and provide feedback for healthcare professionals to identify incorrect antimicrobial prescriptions and prevent their adverse effects, which consequently reduces morbidity and mortality rates and the rate of sepsis.
Natural language processing, on the other hand, solves data retrieval problems from clinical databases, which are currently the biggest limitations of CDSS, enabling the more rational and effective use of antimicrobials. 17 Additionally, older patients face challenges with the effective implementation of antimicrobial stewardship programs (ASP), as antimicrobial exposure considerably increases with age due to multimorbidity and immune senescence. 18 AI-powered CDSS can further enhance ASP by optimizing prescribing practices, which is key for geriatric patients with complex medical needs. Moreover, by addressing issues such as gut microbiota disruption caused by antimicrobials, AI technologies can help minimize the risk of secondary infections among older adults. 19
Drug interaction and adherence monitoring
Medication therapy management (MTM) is a collaborative effort between pharmacists and other healthcare professionals that encompasses comprehensive review and monitoring to improve patient adherence to prescribed medication regimens to ensure safe and effective treatment outcomes for patients. Moreover, MTM seeks to recognize and prevent drug interactions, duplicate therapies, dosage errors, and inappropriate medication use. 20 Innovative AI solutions for adherence monitoring include smart pill bottles, wearable sensors, and smartphones contribute significantly to manage the condition. More than 93% of audio inhalers achieved audio analysis accuracy, and the timing of medications was tracked by wearables with a good level of accuracy. Therefore, AI applications can significantly enhance older patient outcomes by predicting drug interactions and adherence monitoring. 21
Challenges of integrating artificial intelligence in combating antimicrobial resistance in geriatric care
On average, patients above the age of 65 years are prescribed more antimicrobials than younger individuals, and these antimicrobials might not be appropriately prescribed and administered owing to age-related factors, such as weakened immunity and chronic conditions requiring polypharmacy. 22 Despite the potential advantages of AI in healthcare, particularly in combating AMR, it also raises important ethical concerns, including obtaining informed consent for data usage, ensuring safety and transparency, safeguarding data privacy, and addressing biases in algorithms. 23
A study analyzing 300 participants’ perceptions found that AI-generated medical responses were rated as more valid, trustworthy, and satisfactory than those from doctors, leading to a strong inclination to follow potentially misleading advice and seek unnecessary medical care. 24 However, medical experts remain skeptical due to AI's lack of explainability, making it difficult to interpret and trust its recommendations, a challenge known as the “black box” issue. Physicians also doubt AI's accuracy in specific tasks, fear negative patient outcomes, and worry about AI undermining their professional autonomy. Additionally, concerns persist that AI recommendations could introduce biases, compromising clinical decision-making and leading to harmful consequences. 25
Bias in AI models poses a significant ethical concern, particularly when training data lacks diversity, as the effectiveness of AI models is heavily dependent on the availability of high-quality and comprehensive datasets. However, the collection of such data can be hindered by privacy concerns, lack of standardization across data sources, and the underrepresentation of certain populations or conditions, leading to raise significant privacy and security concerns. Hence, this imbalance can reinforce healthcare disparities and compromise equitable treatment.10,26
For example, age-related biases in AI systems affect older adults at multiple stages of the ML pipeline, leading to discrimination, exclusion, and reinforcement of societal stereotypes. These biases arise due to several factors, including underrepresentation in datasets, algorithmic misclassification, and the failure to account for the diversity of aging populations. 27
Algorithmic design choices, such as feature selection and model weighting, can also reinforce these biases, exacerbating disparities in real-world applications. Missing data, fragmented health records, and differences in health literacy further contribute to biased AI outputs, potentially skewing CDSS. 28
While, integrating AI tools into healthcare infrastructures poses significant technical challenges, including compatibility with electronic health record (EHR) systems, ensuring reliable performance across diverse healthcare settings, and managing the computational resources required for AI applications. EHR systems play a crucial role in surveillance, research, and interventions aimed at preventing AMR, and AI integration in EHR systems faces multiple challenges, including data quality issues such as missing, heterogeneous, and biased datasets, which can affect model accuracy and lead to disparities in care.29,30
Among older populations, the increasing use of AI technologies raises further concerns about depersonalization, as standardized algorithms may overlook individual patient variations. This risk diminishing holistic, patient-centered care by prioritizing averages over unique experiences. 31
Furthermore, a thematic analysis demonstrated the ethical concerns surrounding equitable access to AI technologies. Participants worried that the high costs associated with AI implementation might create disparities in care quality especially in resource-constrained settings. Financial limitations could restrict access to AI tools, ultimately affecting the fairness of patient care. These concerns emphasize the ethical responsibility to develop inclusive and accessible AI advancements that ensure patients can benefit equally. 32
Lastly, there is currently a lack of well-defined, universally accepted guidelines for designing, developing, evaluating, and deploying healthcare AI tools in a manner that ensures trustworthiness, meaning they are technically robust, clinically safe, ethically sound, and legally compliant. 33
Recommendations
The implementation of AI-driven solutions for geriatric AMR management requires a comprehensive and strategic approach. A critical priority should be the establishment of integrated AI systems that can effectively monitor and predict infection patterns in older care facilities. 34
Healthcare providers should implement AI-driven clinical decision support tools that can assist in optimizing antimicrobial prescription practices and comply with regulatory agencies including the Food and Drug Administration (FDA) and the European medicines regulatory network's to produce information or data intended to support regulatory decision-making regarding safety, effectiveness, or quality for drugs and increased insights into data and strengthened decision support for the benefit of public health.35,36
From an ethical perspective, healthcare institutions must establish clear guidelines for responsible implementation of AI technologies. This includes the development of frameworks for data privacy and security, ensuring transparent decision-making processes, and maintaining appropriate human oversight of AI tools. 37 For example, the FUTURE-AI framework is structured around six guiding principles: fairness, universality, traceability, usability, robustness, and explainability to define international guidelines for trustworthy healthcare AI. 33
AMR surveillance is essential in LMICs due to the high prevalence of microbial infections. However, its implementation in resource-limited settings is hindered by weak healthcare systems, limited financial resources, and a shortage of trained professionals. In response, the United Nations World Health Assembly endorsed the WHO's Global Action Plan to combat AMR. Consequently, many countries are working to strengthen their AMR surveillance capabilities by making substantial investments and expanding surveillance networks. 38 AI further contributes to improved disease monitoring, early outbreak detection, and public health surveillance especially in LMICs.
Moreover, studies exploring the integration of AI-driven infection prevention tools in older care facilities are critical for reducing the burden of MDROs. As shown in Table 2, key research priorities include advancing predictive analytics for AMR trends, optimizing CDSS, and improving AI interfaces for elderly users.
Key research priorities and questions for AI in geriatric AMR management.
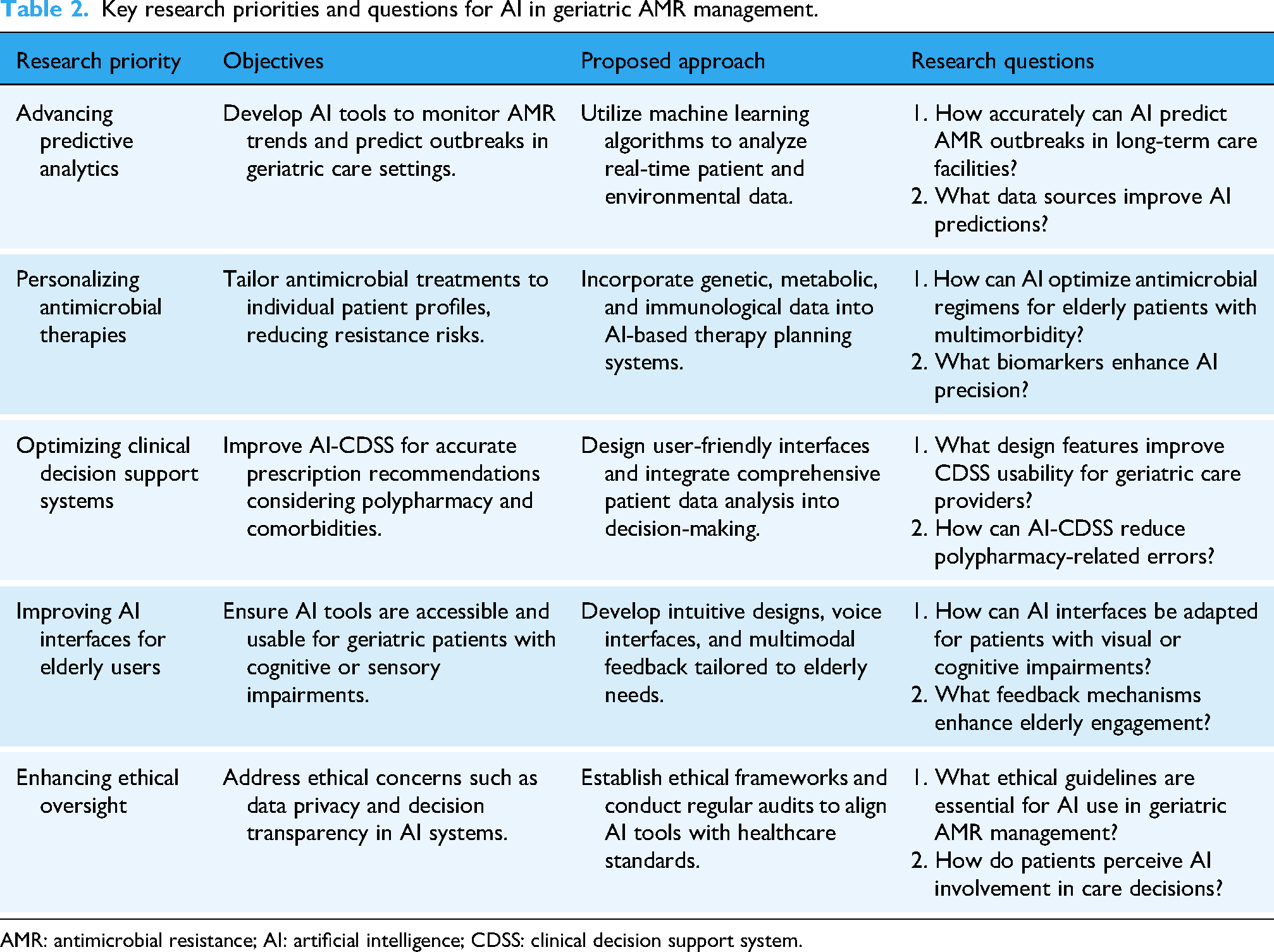
AMR: antimicrobial resistance; AI: artificial intelligence; CDSS: clinical decision support system.
Conclusion
AMR is a significant global health challenge, especially in geriatric populations, owing to increased vulnerability to infections, multimorbidity, and polypharmacy. The integration of AI can enhance diagnostic precision, predict resistance patterns, enhance the prescription accuracy for antimicrobials, and improve medication adherence. AI-powered models can analyze genomic, clinical, and epidemiological data; accelerate the development of novel antimicrobials; and optimize ASP. However, challenges remain in implementing AI-driven solutions, such as incorporating guidelines for fairness, age-related biases, and transparency in utilizing AI systems to mitigate AMR among geriatrics. Comprehensive strategies such as AI-driven clinical decision support and establishing clear frameworks can reduce the global burden of AMR among elderly individuals.
Footnotes
Ethics considerations
Approval from the Ethics Committee was not required.
Author contributions
ZKO and MMA conceptualized and designed the study. ZKO, OJO, and BAO conducted literature reviews and curated the data. ZKO, BAO, SGE, MMA, and OJO wrote the first draft of this manuscript. YAA and SSM critically revised the manuscript for intellectual content. DELP III supervised the study. All the authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.