
Abstract
Introduction
As the population increase and cancer becomes a leading cause of death, there is an increasing need for personalized, technologically aided, and cost-effective home care. Instead of adding more hospital beds, more patients may receive long-term, high-quality treatment at home by transitioning to digital home healthcare systems. The economic challenges in Jordan could significantly impact the availability of palliative healthcare services for cancer patients. Home care can be a useful and affordable solution to these problems. However, a critical analysis of the current process and its corresponding data structure is necessary to prepare for digital solutions.
Objectives
To comprehend the existing palliative home care process and its respective data for cancer patients in Jordan prior to its digital transformation.
Methods
The design science research methodology has been applied within two increments of deliverables. A role-oriented business process modeling technique was used in the first increment to present and get a critical understanding of the current palliative home care process and the accompanying data consumed to narrow the digital readiness gap. A data model from the first increment was algorithmically derived in the second increment. The King Hussein Cancer Center in Jordan's case study on the palliative home care process is used to demonstrate and evaluate the work.
Results
The work delivered 33 data entities and their relationships from role-oriented business process models that were not identified before this research.
Conclusion
The business process model and data model contribute to attaining a higher digital readiness before a digital transformation into a technology-supported palliative home care system. This has involved eliciting roles, associated responsibilities, interactions, and privileges regarding their activities and respective data for future development. However, still some limitations are identified.
Keywords
Introduction
The rise of advanced technologies such as machine learning and data analytics presents a great opportunity to enhance home-based healthcare. Business process models (BPMs) play a crucial role in bringing technology closer to the healthcare domain by providing a structured framework for understanding, analyzing, visualizing, and improving healthcare processes.1–4
In cancer care hospitals, palliative care aims to improve the quality of life for patients and their families, paying attention to their comfort, dignity, and overall well-being throughout the illness. 5 Palliative care is not limited to the terminal stages of a disease; it can be used at any point in the illness.6,7 It aims to prevent and alleviate suffering through comprehensive management of pain and other distressing symptoms, such as nausea, fatigue, shortness of breath, and depression. The care is provided by a multidisciplinary team of healthcare professionals, including general practitioners, oncologists, nurses, social workers, psychologists, and other specialists, who work together to create a personalized care plan. 8 In Jordan, King Hussein Cancer Center (KHCC) is the main palliative care service provider.9,10 Although home-based care is one of the crucial services offered during the palliative care process, there are barriers to providing home nurses with proper palliative care education and training.9–11 In the KHCC, BPMs have been utilized to communicate a critical understanding and analysis of palliative care for education and training. 1 The research community also emphasized the value of quality measurement and highlighted many areas where process-related aspects have been considered while designing home care. 12 This indicates the significance of considering the BPM approach in developing Palliative Home Care (PHC).
According to the head of the palliative care department in the KHCC, who is the second author of this article: While palliative care involves multidisciplinary teams engaging in complex communication, it remains a challenge for domain experts to accurately assess the importance and value of the current processes and data entities that are regularly handled. The extent of their necessity for digital transformation within the context of palliative home care is yet to be fully understood. This demonstrates the present shortcoming or gap in the KHCC PHC's digital transformation readiness.
Despite Jordan's reputation as a Middle Eastern healthcare provider, the country continues to confront economic obstacles that limit access and creation of highly accessible and equitable palliative care services. 13 Jordan is categorized as a middle-to-low-income country. 13 By the end of 2024, the population was estimated to be 11,734,000, 14 while the unemployment rate was 17.9%. 15 Official data from the World Bank indicates that Jordan's GDP was valued at US$50.97bn in 2023. 16 The GDP value of Jordan represents 0.05% of the world economy. 16 Approximately 8.9% of Jordan's GDP is expended on healthcare. 17 Nonetheless, Jordan's national debt has grown to a high level, reaching 89.20% of GDP in 2023. 18 Non-acute services like palliative care, which are seen as low priority in the healthcare system budget, have seen limited funding and narrow investment due to this financial burden. Units in specialized hospitals like KHCC and non-governmental organizations are the only places that provide palliative care services because of this low investment. This indicates that there are not many specialized units that are easily accessible, which results in a shortage of infrastructure and qualified providers. Jordan's healthcare system is facing further pressure because of the refugee crisis. According to the UNHCR, the country has hosted over 1.3 million refugees by 2024. 19 About 77,335 were foreigners, whereas the great majority were Syrian citizens. In addition to living in poverty, many refugees have little to no access to official medical treatment, much less specialized palliative care. All of these provide serious obstacles to funding and access to palliative care and treatment.
Lokuge et al. has defined organizational digital readiness “as an organization's assessment of its state of being prepared for effective production or adoption, assimilation and exploitation of digital technologies for innovation.” 20 Rising et al. defined digital health readiness as “people's ability and comfort in using digital tools for health care engagement, inclusive of the many factors that extend beyond digital health literacy.” 21 This becomes a gap when healthcare professionals and patients lose or record low ability and comfort in using these digital tools in healthcare management. For example, this gap becomes wider when BPM and data models are absent in palliative care. Weiner has articulated the obligatory involvement of individuals, processes, grouped stakeholders, departments, and networked units as a “multi-level construct.” 22 The term “digital” should not be narrowly considered from a technology perspective, as this limits its potential impacts. Digital is significant when it is used to improve present experiences and results for stakeholders by redefining work processes, patterns, data, quality of service, and business models. 23
As palliative care society develops, palliative healthcare providers intend to achieve a level of digital readiness for digital transformation to continually address changing health situations and use technology to gain a competitive advantage and enhance quality of life. 24 Use of digital solutions has contributed to reducing pandemic risks and spread, 25 enhanced patient experience, optimized systems, helped healthcare professionals and providers,26–30 and increased diagnosis preciseness and prediction robustness. 31 However, in-person interactions are still necessary for therapy and follow-up. 25
The research community highlighted the need to assess digital readiness for palliative care consumers and providers. 32 Digital health is not always the solution. This is due to several limitations including those related to interoperability, connection, design, usability, cybersecurity risks, and more.32,33 For example, telehealth in PHC, through mobile apps, seems widely adopted as a technology solution that improves patients’ access to healthcare professionals.26,28 However, no research has shown if telehealth has helped patients with their burdensome symptoms and quality of life. 33
In order to accomplish person-centered care goals, researchers must distinguish between customizing digital solutions to satisfy patient care needs and determining if telehealth adoption is acceptable for communication.32,33 Despite the fact that PHC technology might provide possible solutions in Jordan, 34 no digital solution can be implemented without first determining its level of readiness. 35 This entails developing a thorough understanding of the targeted population's processes, persons, culture, beliefs, setting, and general needs for a high quality of life. 34 BPMs have contributed to promoting an understanding of digital readiness and transformation in health.3,4 In addition, resource availability and PHC community willingness are key for assessing PHC care system readiness for digital transformation.34,36
The digital readiness gap in PHC is a widely acknowledged issue that is not exclusive to Jordan or low-middle-income countries. It also presents a problem for nations with aging populations and fragmented healthcare systems. PHC is lagging in the ongoing digital transformation of healthcare because of fragmented processes, a lack of standardized workflows or BPMs, and poorly resourced care locations. 37 According to recent studies, digitization in PHC improves communication, decision-making, education, information exchange, and costs. 38 The process-to-data proposed approach improves digital readiness by aligning workflows with the data model. This strategy is adaptable to other situations and might be used in other healthcare systems. In order to assist international initiatives like the World Health Organization (WHO) Global Strategy on Digital Health 2020–2025, this study aids in mapping current practices and identifying data gaps. Interoperability, adaptability, and scalability are essential for sustainable digital health programs worldwide. 39
The literature lacks work reporting how the BPM methodology helped PHC in Jordan reduce the digital readiness gap. The purpose of this study is to employ a role-oriented BPM method to narrow the digital readiness gap in the PHC process at the KHCC in light of the increased demand for home-based care, which necessitates high-quality, cost-effective personalized care.
Background
Palliative home care
Saunders developed the hospice care strategy in the middle of the 20th century as means to help people who are near death and manage the pain they are experiencing. 40 In 2002, the WHO defined palliative care as “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.” 41 It is “a holistic interdisciplinary approach that focuses on supporting the quality of the end of life to be included in the definition of a palliative care patient.” 42 This also entails patients’ readiness to participate in the palliative care process and communicate their goals to all healthcare professionals and caregivers. 42
Palliative or hospice home care is a designated service delivered to people with a life-limiting illness who want to be cared for and die. In the latter stages of an incurable disease, PHC provides compassionate and empathetic holistic care and support for patients and their families focusing on the quality of the patient's life rather than its length. A multidisciplinary team of healthcare professionals, caregivers, social workers, nurses, physicians, technicians, and volunteers work together to provide comprehensive care and support for patients and their families. 43 The delivery of PHC requires many interventions to address the complex needs of patients with advanced illnesses. 44
Expanding PHC's digital integration into the corresponding healthcare systems is one of the recommendations drawn from the body of current literature to improve the standard of end-of-life care. Palli-MONITOR was proposed to serve these recommendations. 45 It is an initiative aimed at developing and testing the feasibility of using electronic Patient-Reported Outcomes Measures (e-PROMs) in the electronic version of the Integrated Palliative Care Outcome Scale in specialized PHC settings in Germany. 45 It is designed to improve patient-centered care by enabling real-time, standardized collection of patient-reported outcome regarding symptoms and concerns. Results have indicated that patients’ poor general health and the inadequate equipment of web-enabled services have hindered their ability to participate in interviews. 45 As a result, fewer medical experts now embrace it. When family carers support the use of e-PROM, it facilitates patient-level reflecting processes. There have been concerns reported over the capability for e-PROMs in Palli-MNIOTOR to interfere with existing systems, such the emergency call system that operates 24/7. These identified limitations emerge due to the absence of a comprehensive patient-centered process that identifies and presents patients’ conditions and needs and PHC professional's needs before digital implementation. 45 Furthermore, healthcare workers’ limited awareness of the Palli-MNIOTOR service process and the absence of process and data standardization remain to be barriers to digital readiness and transformation. 46 These limitations highlight the need of carefully designing the PHC process from a patient-centered perspective prior to implementing PHC systems like the Palli-MONITOR. Therefore, the necessity of a patient-centered process that leads to the development of a patient-centered questionnaire to assist healthcare professionals is essential for acceptability. 45 Understanding carefully the PHC process before deriving data needs is a major part of this research to reduce the above difficulties and limitations.
In Jordan, researchers from KHCC developed Jordan's National Palliative and Home Care Strategic Framework for ensuring universal access to high-quality palliative care with agreement from the government and stakeholders reflecting on its 5-year impact and encompassing six domains. 47 They highlighted the importance of national strategies to improve palliative care access and the role digital tools can play in mitigating logistical and resource-related obstacles. Expanding digital solutions in Jordan necessitates a critical understanding of the PHC process and its consumed data before any targeted development and training for users. However, implementing digital solutions in Jordan faces many barriers that continue to hinder the development of PHC. Barriers include PHC workforce shortage, limited opioid access, limited public awareness and service availability, and limited governmental funding. 47 Moreover, the process for achieving this is still absent.
Telehealth apps may be a positive addition to PHC patients. It enhanced experiences with security and safety, improved access to healthcare experts at home, and increased satisfaction.33,48,49 Telehealth apps for PHC are reported as cost-effective because they lessen the financial burden related to hospital resource utilization, travel, and in-person visits.48,49 On the patient's side, the frequent travel burden to healthcare facilities is reduced, as patients access and receive care at their homes within flexible time schedules that suit them best.48,50 This has benefited in reducing waiting times in the queues and improving overall care satisfaction. 50 Telehealth apps enable continuous monitoring of symptoms, allowing for early intervention and better pain management. 50 An additional advantage is that the PHC team can tailor support and care by using real-time data to inform personalized interventions. This enables family members to participate in a personalized care environment.51,52
However, there are no reported findings indicating that these telehealth applications enhanced life quality or alleviated burdensome symptoms. 33 This remains a limitation. PHC telehealth apps may be inaccessible due to device and internet connectivity issues. 48 A lack of digital literacy can hinder the efficient use of technology and cause patients and professionals to become less involved. 48 According to one study, 70% of 251 families who received palliative care through telehealth stated that, if given the option, they would prefer to see a physician in person. 53 Additionally, because telehealth requires less empathy and face-to-face engagement in patient care, PHC providers can be hesitant to adopt it. 54 Patients’ concerns about privacy invasion act as another barrier to the adoption of PHC telehealth applications. 54 Understanding the PHC process is the first step in conducting further research to expand the body of knowledge on how well telehealth improves symptoms and quality of life. Researchers assert that in order to gain the full benefits of telehealth in PHC, it must be appropriately digitally prepared for deployment, taking into account technology, integration, and user-centered design.48,49 Researchers advocate following a hybrid model by combining telehealth and in-person visits to balance efficiency with human connection and needs. 55
Due to the current lack of access to PHC services, Jordan, like many developing countries, faces a shortage of qualified PHC professionals. 56 This shortage hinders the adoption and implementation of respective digital solutions. Also, there is still a shortage of competent staff to adequately administer and utilize these telehealth technologies for the benefit of PHC patients and professionals. For instance, nurses’ perceptions are impacted by their limited knowledge of telemedicine; according to experts, this may be improved by training nurses about modern technologies like as telehealth. 57 Lack of regulations and policies to support healthcare digital solutions remains a gap and a challenge.58,59 This highlights the necessity for organizations to put great effort in making the consent processes comprehensive and transparent to meet patient-centered needs.58,59 Implementing digital solutions requires large investments where lack of financial resources for this need is still a barrier in Jordan. However, the Ministry of Health's strategy emphasizes the need of enhancing digital transformation and current information technology (IT) infrastructure, which is crucial for supporting digital palliative care solutions. 60 Privacy is another reported challenge in implementing digital solutions. Patients frequently hesitate to participate in telemedicine therapy because they lack confidence in the way their data is maintained and shared. 59 In this context, educational initiatives are required to raise public awareness and acceptance of telehealth palliative care services. However, when there are several interventions in common living areas, privacy issues arise. 58 The absence of standardization in Jordan's healthcare system presents additional difficulties. 59 Setting an adequate health standardization approach is a priority before adopting and implementing electronic health records in Hakeem, which is a non-profit organization aiming to revolutionize the healthcare sector in Jordan. 61 Hakeem recognizes how important it is to work with hospital administrators, staff, and patients to establish clear standards and guidelines for healthcare providers. 59 However, this is not a simple task for Hakeem and requires big efforts due to the variety of involved environments, rigid policies, and different visions and agendas. 59
Business process modeling for palliative home care
BPM is a structured approach to analyzing, designing, and optimizing processes in healthcare, ensuring their alignment with patient needs. Hammer and Champy defined “a business process as a set of partially ordered activities intended to reach a goal.” 62 It is also considered “a collection of activities whose final aim is the production of a specific output that is of value to the customer.” 63
The business process management lifecycle phases are process identification, process analysis, process design, process implementation, process monitoring, and process optimization. 64 BPMs are visualized during process analysis and design using languages that enable organizations to model workflows and facilitate useful and rich communications between stakeholders. Standardization and interoperability in BPMs are other key features that permit organizations to use the agreed syntax and semantics for reusability and automation. BPM languages vary based on purpose. The selection of language depends on process complexity, targeted users, and intended outcomes. Business Process Modeling Notation (BPMN) is a role-oriented open-source standardized language developed by Object Management Group for automation purposes, 65 whereas Unified Modeling Language (UML) is for generic use for both business and software domain experts. 66 The Case Management Model and Notation is the appropriate language when steps are less structured within dynamic scenarios in a process. 67
Employing business process management in healthcare contributed to the continuous improvement of processes and their automation, development of decision support systems, improvement of patient privacy, identification of interactions and their complexity between different roles, redesigning processes to adapt to needed changes, and detection of weaknesses and failures. 68 Since 2009, there has been a significant evolution in the business process modeling of healthcare processes. 2 However, they have not been widely reported or evolving in the PHC context until recently in Odeh et al. 1
PHC involves complex, patient-centered processes, often requiring collaboration among healthcare providers and caregivers. One of the BPM approaches is the role-based, which enables stakeholders to visualize and restructure their workflows with respect to the roles, ensuring a clear and consistent representation of the responsibilities without redundancies. In Jordan, the role-oriented BPM was employed using the industry standard BPMN language to design PHC for KHCC. 1 These models have informed further required improvements and their associated implications for cancer patients. It has also assisted palliative care domain experts in attaining a critical understanding of the currently running operations that were the current gap for digital readiness at that time. Moreover, the PHC BPMN model contributed to developing goal-oriented models to visually trace the most critical and strategic actors in the PHC process and to bridge the gap between the world of PHC requirements and their computer-based information systems, future cloud services, and Internet of Things (IoT) smart devices.69,70 However, the delivered BPMs in Odeh et al. 1 have missed the integration of the data consumed over the workflow execution. Without integrating its data, a process cannot be complete, consistent, and accurate especially when a business process is continuously evolving to accommodate different organizational performance levels. This involves reflecting the change in both the workflow of the process and the data consumed.
Research methodology
The applied research methodology in this research is the design science research (DSR), which is a structured problem-solving approach to conducting research. DSR is a research paradigm that focuses on creating and evaluating artifacts to address specific problems or improve existing practices or situations while contributing to both theoretical and practical knowledge. 71 Artifacts could be in the form of models, algorithms, processes, methods, or implemented systems. During DSR, artifacts are evaluated to demonstrate utility, quality, and efficacy. DSR has been adopted in health informatics, information technology, project management, and related research fields.71–74 Its outcomes can lead to improved practices, technological advancements, and practical contributions to the field of study.71–74
Peffers et al. outlined the following six phases in the DSR process: (1) identifying a research problem, (2) identifying respective solution and objectives, (3) designing and developing the artifact, (4) demonstrating the developed artifact, (5) evaluating the artifact, and finally (6) communicating and disseminating knowledge. 71 Figure 1 shows the DSR methodology flowchart. The first phase involves identifying the research problem and its motivation. The second phase involves identifying research objectives based on the problem. Creating the artifact using the appropriate tools and methodologies happens in the third phase. The fourth phase shows how the artifact solves the problem through a case study, simulation, or experiment. The fifth phase presents an assessment of the artifact against criteria such as quality, cost, performance, and effectiveness. Finally, the results are presented to stakeholders through presentation or publication. The DSR of this research is shown in Figure 2, and it involves iterative cycles of building and evaluating artifacts to refine and tune the aimed solutions. In DSR, a major challenge is reported when researchers attempt to bridge the gap between theoretical contributions and practical relevance.
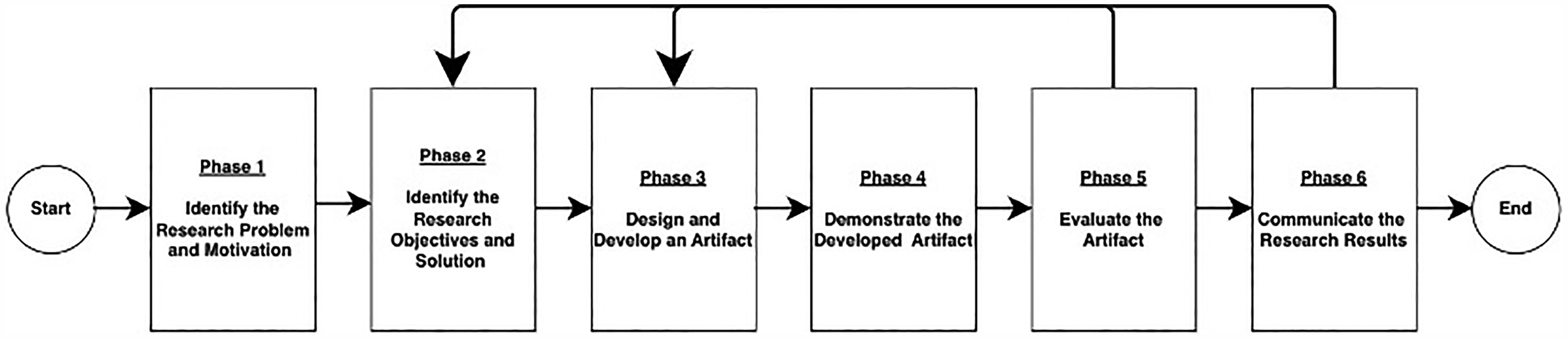
Design science research methodology.
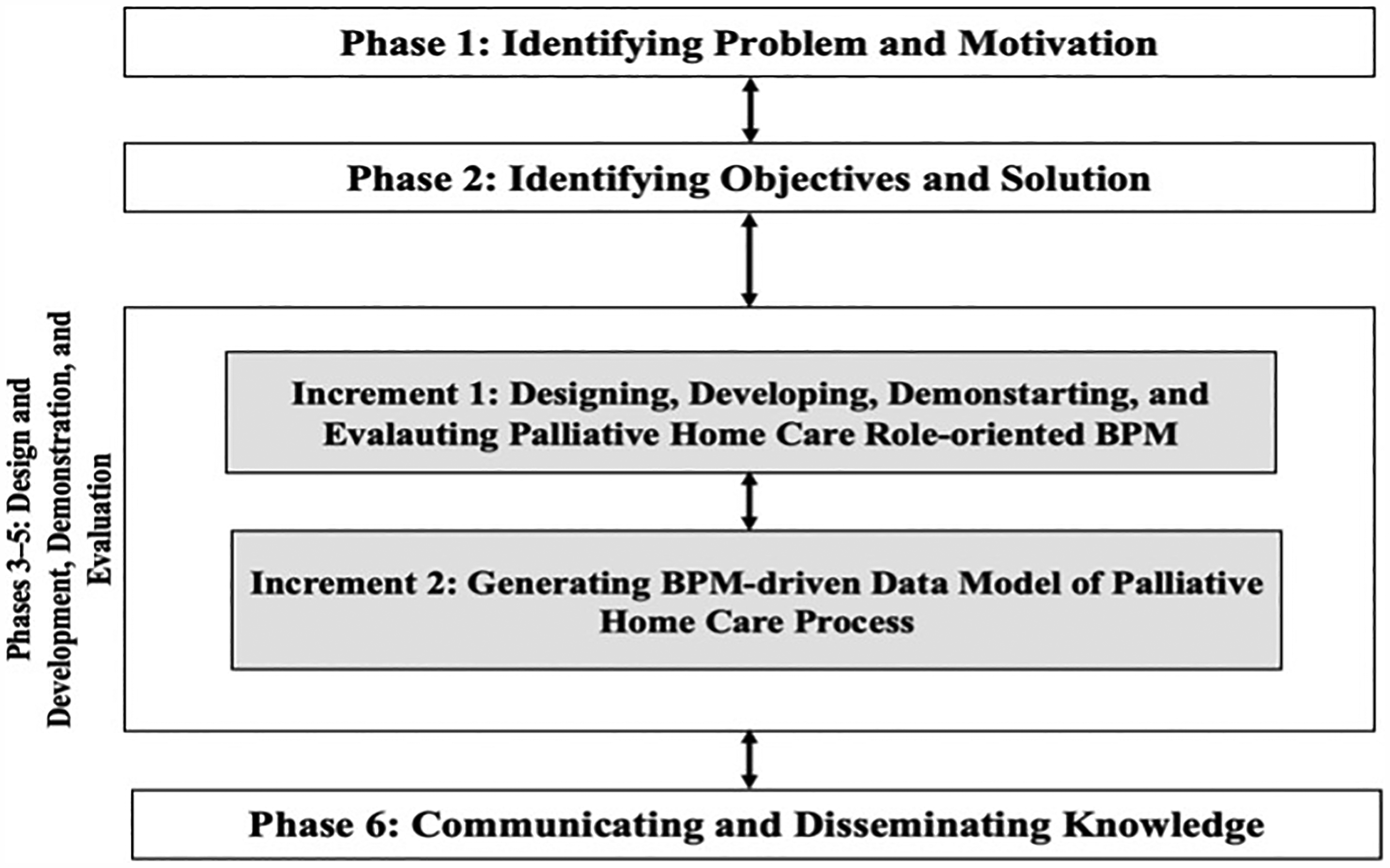
Applied research methodology.
Phase 1: Identifying the research problem
Understanding the current digital readiness situation of PHC in KHCC 9 has led to identifying the research problem: a notable absence of a data model is recognized for reducing the PHC process digital readiness gap in KHCC, using the BPM-driven approach. Having both BPM and the associated data model of PHC would contribute to the advancement of home care through data analysis to enhance the quality of care, promote patient autonomy, and improve the overall well-being of patients and their families.
Phase 2: Identifying the research objectives and solution
This research was set to employ the designed and evaluated PHC process modeled in BPMN,1,65 to investigate whether it derives a PHC data model to support an integrated coordination of information, decision-making, and quality improvement for getting closer to digital readiness. This aim will be achieved by first revisiting the developed PHC process in KHCC,1,9 and then employing an algorithm for deriving a data model from a role-oriented BPM.
75
Two research questions pave the way to addressing the aim. Q1: To what extent does the KHCC PHC process designed using BPMN reduce the digital readiness gap? (Answered in first increment deliverable) Q2: To what extent does the KHCC PHC BPM and stakeholder-driven data model reduce the digital readiness gap? (Answered in second increment deliverable)
Phases 3 to 5: Design and development, demonstration, and evaluation
This part is described as a block of the three phases, which are the design and development, demonstration, and evaluation as shown in Figure 2. This block delivers two distinctive increments. Each of the two increments contributes to answering a research question.
The first increment: The design, development, demonstration, and evaluation of the palliative home care role-oriented process model
This increment involves eliciting, designing, developing, and evaluating the current workflow of the PHC process in KHCC that has already been conducted in Odeh et al.
1
However, the reader can observe the newly added data entities linked to the activities in the workflow. The outcome of this increment is the PHC process specified using BPMN 2.0 shown in Figure 3. The second increment relies on this increment as a source to extract the data entities to generate the respective data model. For the design and development, facilitated elicitation sessions were conducted in the form of workshops led by representatives from the PHC multidisciplinary team, which are nurses, specialists, and social workers.
1
The researchers have adopted a role-oriented business process modeling methodology for understanding the roles, responsibilities, privileges, interactions, flow of activities, and associated consumed data in the existing PHC process at KHCC in Jordan. The selection of participants in the workshops and interviews is designed to ensure the inclusion of individuals with relevant roles and expertise. The inclusion criteria are identified below:
Participants who have direct involvement and expertise in PHC at KHCC. This included some specific roles such as oncologists, palliative care physicians, general practitioners, PHC pharmacists, PHC consultants, PHC specialists, PHC nurses, psychologists, social workers, caregivers, administrators, and health policymakers. Participants who have at least 3 years of experience in delivering, planning, or educating PHC for cancer patients and their families. Familiarity with challenges in delivering the PHC service.

PHC at KHCC business process model designed using BPMN showing data entities.
Exclusion criteria included individuals who were unwilling to participate or failed to meet the inclusion criteria. The workshops involved open-ended questions to gain a critical understanding of the current workflow that runs for handling PHC service at patients’ homes. In the session, the critical understanding involved specifying respective goals, flow of activities, decision-making points, roles, their interactions, and involved data entities. For execution, the researchers have mapped the “as-is” PHC process using BPMN language for visualizing the workflow for digital readiness in a standardized form. For evaluation, an hour-long session was conducted with the Head of the Palliative Care Department in KHCC to verify the clarity, completeness, and correctness of all activities, roles, decision points, transactions, and data entities as specified in the resulting BPMN model. The evaluation session involved walking through the BPMN model in Figure 3. This increment has set the stage for designing the “to-be” process aligning with the digital transformation goals.
In Figure 3, seven multidisciplinary roles collaborate to deliver PHC service to a designated patient. It shows complex interactions between the roles along with necessary data entities required to complete processing respective activities through the workflow. When a process is not clearly defined, it leaves room for error and can lead to inconsistent results and poor patient experience. Whether the palliative care team is transferring a patient for home care or not, handling patient queries, or resolving an issue, they are required to follow a process before digitalization.
The second increment: The design, development, demonstration, and evaluation of the palliative home care data model
This increment involves designing, developing, demonstrating, and evaluating the data model using the BPM delivered from the previous increment. The outcome of this increment is designed and specified using UML 66 as presented in Figure 4. It shows data entities that are used to maintain and manipulate critical information and their relationships for the PHC process.
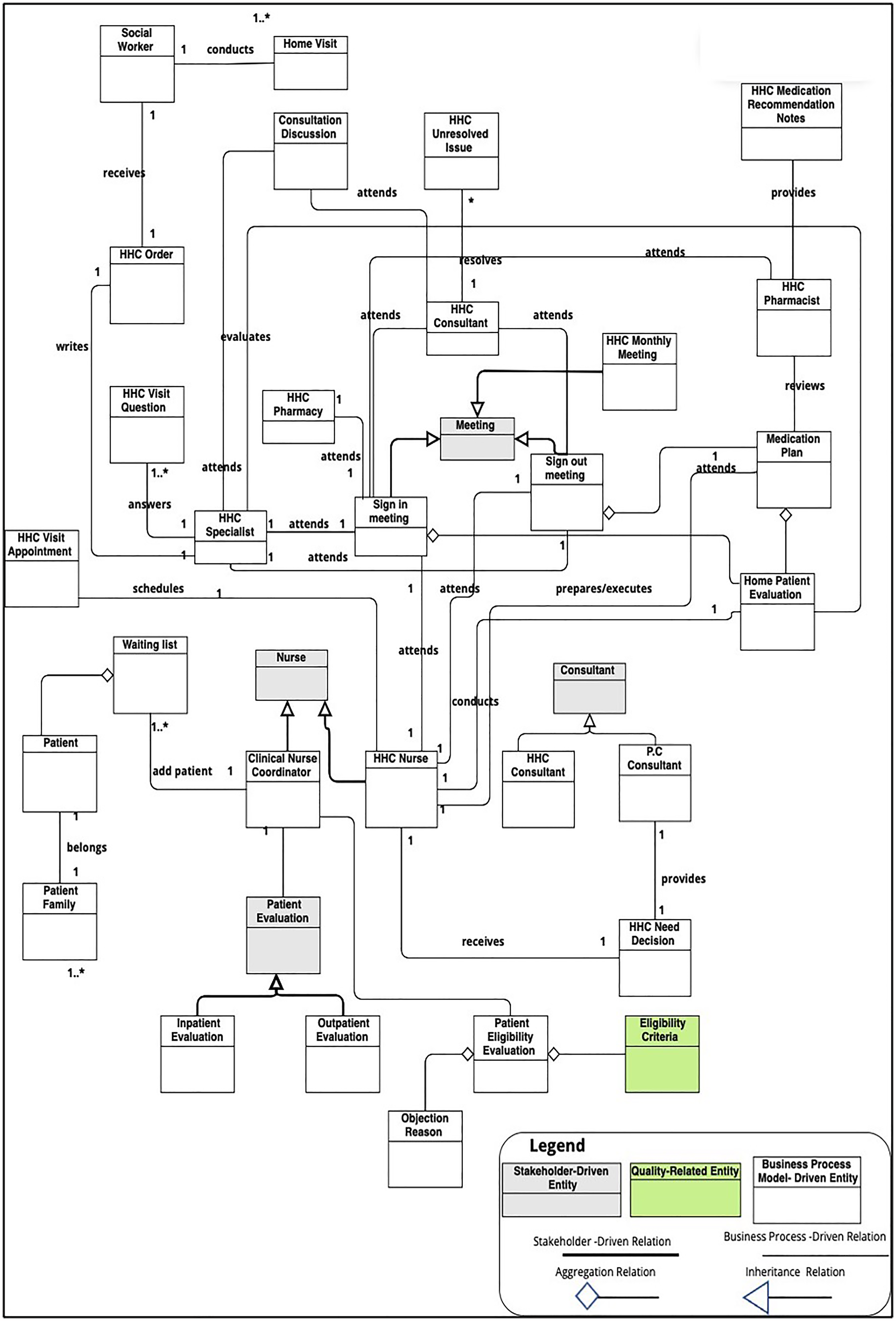
Resulted data model for palliative home care (PHC) process.
For the design, the first author has designed a structured algorithm for generating data entities and associated relations from a corresponding role-oriented BPM and concerned stakeholders. 75 The algorithm is visualized and shown in Figure 5.

Workflow-based algorithm for deriving data model from role-oriented business process modeling (BPM).
A 2-hour interview session was conducted with the presence of palliative care experts in KHCC to apply the algorithm to design and develop the data model for stakeholder-driven entities and relationships. For execution, the algorithm was applied to derive the 33 classified data entities and their relationships. Also, in execution, the UML was adopted for visualizing the algorithmically derived 33 data entities and their relationships in a standardized model. For this reason, the interview involved a limited range of options in the form of close-ended questions to identify stakeholder-driven data entities and their associated relationships that originate from the first increment. Most of the data entities and their relationships in Figure 4, were derived by applying the designed algorithm in Odeh et al. 75 A 60-minute validation session was conducted with the Head of the Palliative Care Department to confirm the completeness, consistency, correctness, and clarity of all data entities and associated relationships. The validation also entailed classifying each data entity into BPM-driven or stakeholder-driven and whether it is a quality-related entity, as per the algorithm. Table 1 is the output of the validation session and lists the 33 data entities, their classification, and relations.
Data entities, their classification, and relations sheet for the PHC process at KHCC.

PHC: palliative home care; KHCC: King Hussein Cancer Centre; PC: patient care.
Identifying attributes and operations is not in the scope of the current version of the algorithm. The resulting data model is constituted of 33 data entities (where 28 of them are labeled as BPM-driven and 4 of them are labeled as stakeholder-driven). Only one is classified as a quality-related entity. This highlights some limitations regarding the identification of quality requirements.
Phase 6: Communicating and disseminating knowledge
The outcomes are communicated to the research community through publishing this article. This dissemination of knowledge has contributed to the collective understanding of the field and reduced the digital readiness gap in PHC practice.
Results
This research has generated the following results:
A role-oriented and data-integrated BPM designed using the BPMN language for the PHC process at KHCC. It is the result of the first increment, as shown in Figure 3. A standardized data model designed using the UML for the PHC process at KHCC. It is the result of the second increment, as shown in Figure 4. The data model consists of 33 data entities that are source-classified into a business process, quality, or stakeholder. A flowchart visual representation of the structured algorithm, as shown in Figure 5. It is another result of the second increment. A table summarizing the 33 data entities and their relationships is shown in Table 1. This table is more accessible and easier to understand for stakeholders. It is another result of the second increment.
In Figure 4 and Table 1, although one quality-related entity is identified (i.e. Eligibility Criteria), it emphasizes the importance of maintaining high-quality PHC service delivery that directly impacts patient care outcomes and satisfaction. Having quality-related entities within the digital readiness context allows healthcare providers to identify performance metrics such as patient safety, satisfaction, and service responsiveness. This facilitates the integration into digital systems. Integrating and representing quality-related entities into BPM paths the way for standardizing PHC procedures increases compliance with protocols.
Identifying only one quality-related entity could be a limitation. As a result, this means more focus is needed to elaborate on more quality-related entities. One identified quality-related entity may reflect local priorities or specific challenges within the PHC system in KHCC. Examples of quality-related entity classification could be patient satisfaction, PHC service responsiveness, holistic care, and external requirements. The current limited availability of data might have restricted the identification of more quality-relate entities. This may highlight the need to run focused sessions to overcome this limitation in the future.
Discussion
The existing PHC process has reported low automation in its activities and some complex interactions of communications within roles. 1 Before communicating this research, the data model of the process was absent. 9 The two research questions are answered in this section.
Answering the first research question requires understanding how BPMN elements in Figure 3 contribute to reducing the digital readiness gap. The BPMN elements in the case study are roles, activities, interactions, and gateways. Each of them can contribute to the digital context as below:
Roles: The model is rich with seven roles due to the involvement of the multidisciplinary team. In Figure 3, stakeholders and the IT team can understand and analyze each role's responsibilities in the desired digital environment. This enables mapping roles to specific digital tools, systems, or interfaces. However, this mapping may not be fully digital, as face-to-face interactions are still required for quality of life and patient satisfaction.1,71 For example, face-to-face home visits by Home Health Care (HHC) nurses are compulsory for some situations even if HCC goes digital. Assigning roles to appropriate digital resources ensures that the right palliative care stakeholders have access to the necessary digital capabilities, facilitating seamless collaboration and execution. For example, one of the Patient Care Clinical Nurse Coordinator (PC CNC) role responsibilities is informing the team of objection reasons in case a patient is not eligible for home care, as in Figure 3. Activities: They are the tasks performed within a role. Some are classified as automatable tasks that can be performed by the to-be digital systems. By analyzing and optimizing the PHC activities through BPMN, palliative care management can identify opportunities for digitalization and automation or the use of data analytics tools, leading to increased quality of service. For instance, in Figure 3, evaluating patients and discussing plans with HHC specialists and HHC Nurses are non-automated. This may call for a digital solution. Gateways: they present different home care branching of scenarios based on specific conditions. Gateways can be defined to incorporate digital decision-making into the process, evaluate real-time data, or route activities based on predefined rules. By leveraging gateways, palliative care management can introduce digital intelligence and agility into their processes, enabling adaptive and responsive operations. This can contribute to increasing patient's quality of life and satisfaction for patients, their families, and the palliative care team. For instance, some decision-support digital tools may be introduced to assist in informing whether an HHC is needed or not for a patient based on the current dataset. This would support the efficiency of the HHC nurse role. Interactions: they are the information flow for communication between different process participants. In Figure 3, different home care roles interact and exchange data during the execution of the PHC process. This not only helps in visualizing, but also contributes to optimizing the digital interactions and integrations between various health systems, applications, and stakeholders enabling a digitally integrated home care system. This involves modeling interfaces, service invocations, event-based triggers, or data exchanges. For example, PC CNC may require an efficient way of informing all palliative care team members of objection reasons to manage resolving it within a minimum period. Interactions that may be delayed because of physical attendance such as discussions could be replaced with telehealth apps. This couldn’t be marked without having a BPM validated and agreed.
Apart from BPMN notations, BPM promotes sharing the current practice of PHC to develop and advance it through injecting and adopting other good palliative care practices found in research or similar organizations.
Regarding answering the second question, this requires understanding the data model generated by BPM and stakeholders. Before this research, not only the number of data entities was unknown, but also the relationships were not identified. Figure 4 shows different entity relations that are inheritance, aggregation, and association. This can help identify areas of strength and weakness, thus increasing data quality, and informing decisions around data management processes and investments in data-driven digital solutions. In Figure 4, the data model paves the way for designing a database, implementing a knowledge management system, and integrating it with other systems such as telehealth and m-health applications.
Having the PHC data model provides a view of the resource needs. This facilitates the estimation of staff, tools, equipment, and medication requirements for implementation. Implementing both PHC BPM and data model in a real setting can be done through training PHC professionals on using BPMN and data modeling tools to create new workflows and data entities. Then, execute the model in the pilot PHC unit. Then, collect feedback from patients, caregivers, PHC professionals, and family members to refine the models. Finally, they advocate for policies that support digital transformation in the PHC domain.
The practical implications of having the PHC BPM and data models are beyond just visualizing workflow or data entities. A PHC BPM designed in BPMN standardizes the workflow of activities and interactions for automation purposes making the PHC professionals more focused on patient care. Automation involves scheduling sign-in meetings, scheduling a home visit, and tracking a medication plan. Standardizing the workflow of the PHC model facilitates the derivation of functional and non-functional requirements for the design and development of the PHC software system. Moreover, the PHC BPM acts as a unified communication platform among multidisciplinary teams, including doctors, therapists, nurses, oncologists, and pharmacists. This ensures everyone has access to common information. By leveraging the data model, the PHC management and IT team can apply advanced analytics techniques, such as data mining, machine learning, and predictive modeling, to uncover valuable insights, identify patterns, and make strategic data-driven decisions. These insights would empower the palliative care department to optimize processes, improve patient experiences, and drive innovation in the digital era. For example, analyzing patient data can help identify high-risk patients who may benefit from targeted interventions or identify areas for quality improvement.
Addressing the ethical and legal considerations of digital transformation in palliative care is a requirement, but it remains early at this stage of this research, while data privacy and patient autonomy shall also be ensured. The PHC digital system shall consider compliance with data protection regulations, and the applied automation using a particular technology shall consider safety and privacy standards. Data sharing is possible when consent is informed in the digital system. Therefore, PHC digital systems shall facilitate informed consent specifying how data will be stored, shared, and used. The IT experts, digital team, and PHC professionals shall ensure that the implementing technology is enhancing the PHC process rather than replacing human interaction to maintain a higher quality of life and empathy.
In the future, following some strategies to leverage flexibility and scalability in the data model would enable the palliative care department to accommodate new data sources, adapt to changing data requirements, and incorporate new data elements or attributes due to continuously changing healthcare conditions.76,77 This would support the integration of emerging technologies, such as the IoT, cloud platforms, or artificial intelligence, by providing a foundation for data modeling and integration. 77 However, it is important to note that the specified PHC process using BPMN and its data model are just two tools in the larger PHC digital readiness toolkit. Their role in reducing the digital readiness gap is limited and does not guarantee it alone for the future development of virtual communities. 78 Digital readiness is a complex concept that involves many factors, including the availability of digital infrastructure, the skills of the PHC team, the KHCC organization's culture and leadership, the complexity of processes, strategic thinking, and project management. The future work plan involves investigating digital readiness from a strategic view69,70 considering process optimization, and investigating ethical and legal issues.79–81 Ontology development of the data model is necessary to promote consistency and interoperability between different palliative care systems. Identifying PHC agility principles is also a plan before digital transformation.82,83
Limitations
The work in this research presents the current state of the KHCC, where PHC workflows, associated data, and regulations are continuously evolving. Therefore, any future modification in PHC policies and regulations should be reflected in the KHCC PHC medical practice and proposed models. According to the role-oriented BPMs, limited stakeholders have been involved, although a deeper engagement of a broader range of stakeholders would enrich the current perspectives of the models. For example, engaging IT experts would enhance the selection of technology adoption, and engaging policymakers would improve the current workflow and reduce bottlenecks. The algorithm design is limited to the role-oriented BPM based on some assumptions that may limit its applicability to other BPMs. The study focuses on delivering process and data models without extending them to an actual implementation for the PHC software system. Thus, the effectiveness of the delivered models remains untested. Although the study identifies data entities and relationships, it still does not explicitly address data privacy, security, or compliance requirements. Also, the identification of other quality requirements in the form of quality-related entities is a limitation in this research. This means more focus is needed to elaborate on more quality-related entities.
The context-specific nature of this study affects generalizability, as the study focuses on the KHCC palliative care system. Since Jordan is considered a middle-low-income country with limited resources and workforce, this has constrained and shaped the design of the present BPM and data model. Also, the study did not test these models in different palliative care settings. However, in higher funding countries, these models will require adaptations to include process automation and optimization. Both the PHC BPM and data model were presented for a single case study that is particularly for the KHCC institution. Other institutions may require integration with other systems or have different role hierarchies. This makes the presented PHC models in this research less applicable. Finally, the study did not consider exploring the diversity of patients and their personalized care.
Conclusion
The research has concluded that the specified PHC process using the BPMN language promotes a higher digital readiness. This is demonstrated in the designed BPMN elements in the PHC process that are potential for a respective digital solution to be enacted into their information systems, telehealth systems, or m-health apps in terms of roles, activities, interactions, and gateways. Due to the applied standardized visualization, PHC professionals can rely on the BPMN PHC process in sharing their practice and analyzing the impact of change for digital transformation. By identifying critical decision points and information required to make those decisions, the PHC management can determine how digital tools can be integrated to enhance the process. The delivered PHC data model with 33 data entities contributes to the initial development of the PHC database management system.
While these models have offered a foundation for digital transformation, several limitations must be addressed through a clear future work roadmap. (1) Refine the as-is PHC process and data model concerning PHC quality requirements and automation points; (2) specify the functional, non-functional, external, and data requirements for the to-be PHC software system; (3) design and implement the to-be PHC software system; (4) apply the implemented to-be PHC system using a pilot case study; and (5) evaluate the implemented system and collect feedback to develop another business plan for refinement and improvement. Beyond this specific application, the work in this research is scalable in low-resource settings for digital PHC initiatives. This can be achieved by revisiting and optimizing current PHC BPM and data models under limited resources, budget, and infrastructure. This shall also involve multisite evaluation to validate and refine these models to maximize their impact on improving PHC system outcomes in resource-challenged settings.
Footnotes
Acknowledgements
The authors are grateful to Al-Zaytoonah University of Jordan, Amman, Jordan, Palliative Care Department and Home Care Services, King Hussein Cancer Center, Amman, Jordan, and the University of Jordan, Amman, Jordan for research support.
Ethical considerations
No human or animal participants were involved, and no patient data was collected. No human-identifiable data is reported in this study.
Consent statement
All authors of this manuscript have provided their consent for submission. Furthermore, patient consent is not required as this is a bibliometric study that does not involve any patients.
Author contributions
YO conceptualized and designed the research methodology. YO used software to visualize models. YO and OS validated the work. YO conducted the formal analysis and investigation. YO and OS collected and provided resources. YO and OS curated data. YO prepared and wrote the original draft of the manuscript. OS reviewed and edited the manuscript. All authors contributed to the manuscript and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All required data is available in this manuscript. No datasets were generated or analyzed during the current study.
Guarantor
YO.