
Abstract
Introduction
Evidence-based practice is a problem-based solving approach to clinical practice that encourages nurses providing personalized patient care while utilizing the necessary scientific evidence for a better understanding of risks and benefits of diagnostic tests and treatments. Digital transformation of an organization begins with attaining an acceptable digital readiness level. One approach entails specifying and modeling their processes and the respective data models.
Objectives
In Jordan, at King Hussein Cancer Center—an international and regional accredited cancer care hospital—their nursing practice requires obtaining a standardized specification of evidence-based practice processes and their respective conceptual data model that is currently not specified for digital readiness.
Methods
The design science research methodology was adopted to deliver two increments. The first was concerned with the design, development, and demonstration of eight evidence-based practice processes specified using BPMN. The second was related to the design and development, demonstration, and evaluation of a respective derived data model of the case study. Both increments involved interviews with domain experts for elicitation and validation.
Results
Eight evidence-based practice process models were identified and specified using BPMN along with their associated data models, where one representative process model was utilized in this research to demonstrate the effectiveness of process and data modeling towards digital readiness of evidence-based practice in regional cancer center.
Conclusions
Both deliverables enabled the evidence-based practice management to attain common understanding to identify inefficiencies, redundancies, and areas for improvement that can be addressed through digital solutions. Evidence -based practice BPMN process models were considered as a road map to follow up a project implementation and a rich visualization to perform data analytics to identify evidence-based practice trends, patterns, and insights that can inform strategic data-driven decisions. Both deliverables were concluded necessary for developing respective information systems in the journey towards digital transformation.
Keywords
Introduction
Evidence-Based Practice (EBP) in nursing integrates research evidence, clinical expertise, and patient preferences. This problem-solving approach to clinical practice has encouraged nurses to provide personalized patient care. 1 Incorporating EBP into nursing offered nurses the scientific evidence necessary to make sound judgments. Nurses may keep current on new medical guidelines for patient care by using EBP. By identifying recorded therapies that match their patients’ characteristics, nurses may improve their patients’ chances of recovery. EBP has helped nurses to analyze studies in order to have a better understanding of the risks and benefits of diagnostic tests and treatments. EBP helped nurses to include patients into their care plans. This has empowered patients to take an active role in their own healthcare by allowing them to express concerns, share their values and preferences, and make recommendations about how to proceed. When EBP was used effectively, it resulted in improved patient outcomes, resulting in a reduction in the demand for healthcare resources. As a result, healthcare organization may save costs to reinvest elsewhere in healthcare. For instance, obsolete processes may have involved equipment, materials, or items that are no longer required for certain operations or approaches.2,3,4
The Covid-19 pandemic has led many countries to implement a variety of approaches for preventing its spread and empowered in dealing with patients’ cases through digital technology tools that focus on agility and patient centricity. The journey towards digital transformation of an organization begins with attaining an acceptable digital readiness level that necessitates, as one aspect, the availability of standardized validated business processes that guide how activities run and data manipulation to ensure safe and effective patient-centered care. 5 In this context, the questions arise of whether current healthcare organizations are digitally ready to involve digital technology solution tools in carrying out their EBP activities. Among recommendations in this regard is that organizations should specify and model their processes showing the flow of data and information aligned with their strategies and goals, as an approach for informing the extent to which digital technology solutions and tools can lead and enhance digital readiness in the future. 5 In Jordan, at King Hussein Cancer Center (KHCC), 6 the EBP processes have run manually with no existing agreed standardized process workflow models, and thus have been distant from digital readiness and automation in order to deliver its services efficiently and effectively, saving more time for patient care. This paper critically reports on the outcomes of investigating whether role-based business process modeling informs the derivation of respective data entities of EBP processes for digital readiness and transformation in a cancer center.
Background
Evidence-based practice (EBP)
EBP has few definitions, one of the influential definitions is of Sackett, D. (2000) “process of integrating the best available research evidence with clinical expertise and the patient's unique values and circumstances.” 7 Newhouse et al. (2007) defined EBP as a “problem solving approach to clinical decision making within a health-care organization that integrates the best available scientific evidence with the best available experiential (patient and practitioner) evidence.” 8 In addition, EBP is considered a fundamental element of today's nursing profession that requires specialized skills and knowledge, and as an enabler to promote patients higher care outcomes and nurses’ autonomy. The EBP concept has been expanded to include the most novel research findings combined with clinical expertise, patient values, and the current environmental factors to determine a plan for patient care. 9
Cassidy et al. (2021) discussed the need to create nursing contexts that are more adaptable to ongoing change due to the dynamic nature of EBPs and the ever-changing healthcare environment. They indicated that nursing environments must be better equipped and organized to be more adaptable and favorable to continue EBP implementation in general. One way to start enabling change in nursing environments is to observe related processes and associated involved data to identify the place and type of change. The study concluded that preparing an organization as a supporting environment for the adoption of research programs and maintenance of evidence in nursing practice is critical for closing the evidence-to-practice gap and enhancing outcomes for the health care systems, patients, and healthcare professionals. 10 Wilson, M. et al. (2015) discussed a prediction model where Registered Nurses (RNs) who participated in research, with specialized certificates, and were enrolled in a clinical career development program had achieved better EBP preparedness ratings. 11
In China, Gifford, W. et al. (2018) revealed that a lack of data accessibility is one of the implementation barriers of EBP. 12 They reported that the availability of web-based social networking technologies enabling simple access to information, as well as leadership support, were among the factors that contributed to the success of the EBP implementation initiative. 12 Johnston et al. (2016) explored the barriers to and facilitators of implementing research into practice. Their analysis identified four main issues that were keeping up to date with evidence, using clinical and technology tools, training and implementation, and barriers at organizational, professional, and personal levels. 13
Evidence-based practice in Jordan
According to descriptive, correlational, and cross-sectional investigations conducted in different hospitals, Jordanian RNs that have worked in critical care units concluded that they had a good degree of knowledge and practice in evidence-based therapies. 14 In addition, greater levels of knowledge of EBP, a favorable attitude towards EBP, higher educational credentials, and training in EBP collectively have contributed to a rise in the adoption of EBP in practice. This study also suggested that nurses should participate in continuing EBP education programs, while nursing educators in clinical settings should examine a variety of methods to increase EBP, such as qualitative research designs and/or open-ended questions. 14
The nursing department at KHCC has adopted strategies to leverage evidence-based research and practice within nursing units. Some activities that support these strategies are structured courses and workshops and peer-reviewed scientific publications. Also, the KHCC's nursing department manages shared governance councils to improve patients’ quality of life and nursing practices. One of the councils is the nursing research and evidence-based practice council that aims at encouraging scientific research culture, supporting evidence-based nursing practices, implementing them into clinical processes, and promoting excellence in nursing care through research, technology, knowledge, and creativity. 6
The EBP in KHCC is described through eight interrelated processes that are: (1) ideating and approving an EBP topic, (2) eliciting relevant literature, (3) critiquing and synthesizing EBP topic related studies, (4) piloting practice change, (5) integrating the practice change into a pilot unit, (6) monitoring and evaluating EBP outcomes, (7) disseminating EBP, and finally (8) obtaining IRB approval as needed. At present, these eight processes run manually with no existing agreed standardized process workflow models. Thus, they have been distant from digital readiness and automation. One of the main concerns in KHCC's research and evidence-based nursing unit management is readiness for digital transformation given the absence of agreed representation or models of EBP processes, let alone resolving bottlenecks, weaknesses and improving such processes through process modeling. 6
Business process modeling and healthcare
The research community has adopted business process modeling methods, languages, and notations in modeling healthcare processes for better understanding, standardizing, sharing, and managing practice or procedural changes with a central focus to improve the quality of health care processes and services. 15 Hammer and Champy defined a business process as “a collection of activities whose final aim is the production of a specific output that is of value to the customer.” 16 A business process has a goal that is affected by events occurring in the external world or in other interrelated processes. According to Bandara et al. (2007), “process modeling occurs before the background of an organizationally and information technology-supported setting in which process models are created to fulfil multiple purposes.” 17 Business process modeling has contributed to standardizing high-level abstract representation of guidelines and clinical pathways of evidence-based medical practice. 18 Role-based business process modeling has been widely adopted in understanding, visualizing, communicating, and improving healthcare processes.15,19–22 Also, the conceptual elements of role-based processing modeling have been well-aligned with the healthcare comprehensive practicing definition of the Australian Health Practitioner Regulation Agency. 23 Analyzing electronic health records’ data entities through role-based business process modeling has been observed to enhance user experience, minimizing cognitive load errors, and improving patient safety. 24 Ahamed et al. (2016) proposed a method to build a domain specific process-based meta model to assist nurses in informing decision making to improve healthcare outcomes, with adaptive guidelines compatible with evidence-based practices. 25
Among the core languages for visual role-based business process modeling is the industry standard Business Process Modeling Notation (BPMN) developed by the Object Management Group, an international non-profit technology standard consortium. 26 Recently, BPMN process models have been utilized in modeling homecare processes in a step towards delivering more effective and efficient palliative care services. 27 Also, BPMN process models have been enacted to compare managing test outcomes in ER and ICT acute departments through understanding similarities and differences in their processes and identifying factors that can improve quality of their respective systems’ design. 28 Moreover, BPMN process models guided the design of clinical pathway workflows for the automation of clinical guidelines, generating alerts in the respective decision support systems, and associating data of electronic healthcare record while diagnosing chronic obstructive pulmonary disease. 29
Digital readiness and healthcare
Weiner, B. J. (2009) has considered organizational readiness for digital transformation as a “multi-level construct” that should involve all individuals, grouped or linked stakeholders, processes, departments, individuals, or linked network of units. 30 Weiner explained that organizations with similar resources and structure can present different outcomes in digital readiness and transformation, as this can be attributed to effective means of managing the utilization of resources and assets. 30 Kaplan and Norton considered the concept of organizational readiness as the extent of preparedness of organization's processes, assets, and activities to transit from the “as-is” state to the “to-be” state. 31 Digital readiness has required articulating changed scenarios, that can be enacted using digital technology. This can be “context-specific operationalization of change readiness” and making “use of digital technologies such as artificial intelligence and data analytics.” 32 Therefore, digital transformation ought to consider comprehensive transformation of business processes where technology plays a central role in delivering business values to stakeholders while their organization is undergoing continual changes.
During and post Covid-19 pandemic, healthcare systems were no longer able to sustain themselves, given the huge volume of changes impacting the delivery of healthcare services under stringent constraints. For example, the situation when front-line services, including nursing, struggled to maintain and improve service quality while facing a shortage of resources. One of the foundational pillars for digital transformation in delivering healthcare services was related to the role of human resources involved in existing healthcare processes prior to enacting these processes in technological solutions. Therefore, two fundamental questions arise here before preparing for the state of digital readiness in healthcare context: (1) Is there a set of standardized agreed healthcare processes linked with organizational strategic goals?; (2) What is the state of readiness of each of these healthcare processes as a standardized means of communicating and sharing health care practices—where healthcare process workflows and associated data consumed, produced or both can be ascertained before they can be enacted using digital transformation technological solutions? Therefore, we claim that digital transformation is not just an end-product or service, but it necessitates continuous feedback to improve or redefine healthcare processes, patterns of care, quality of services, etc. Accordingly, and in the context of this research paper, we aim to investigate whether role-based business process modeling can infer respective data entities for better informing digital readiness of EBP in a cancer center.
Methods
The Design Science Research Methodology (DSRM) 33 has been adopted to orchestrate this research design. Many health informatics projects have adopted DSRM such as the iOntoBioethics research project and others.33,34 Design Science Research (DSR) has focused on designing, developing, and evaluating artifacts that can help solve real-world problems in a particular context. 33 In DSR, researchers have created innovative solutions or artifacts that addressed specific problems or improved existing systems. These artifacts could be tangible or intangible, such as software applications, algorithms, models, frameworks, or methodologies. A DSRM enacts a cyclical incremental and iterative process comprised of the following phases: (1) defining the research problem and motivation, (2) defining the solution objectives, (3) designing and developing the artifacts, (4) demonstrating artifacts’ application, (5) evaluating how efficient and effective are the artifacts, and (6) finally communicating the results. Figure 1 depicts the research design for this study following the DSRM approach as discussed below.
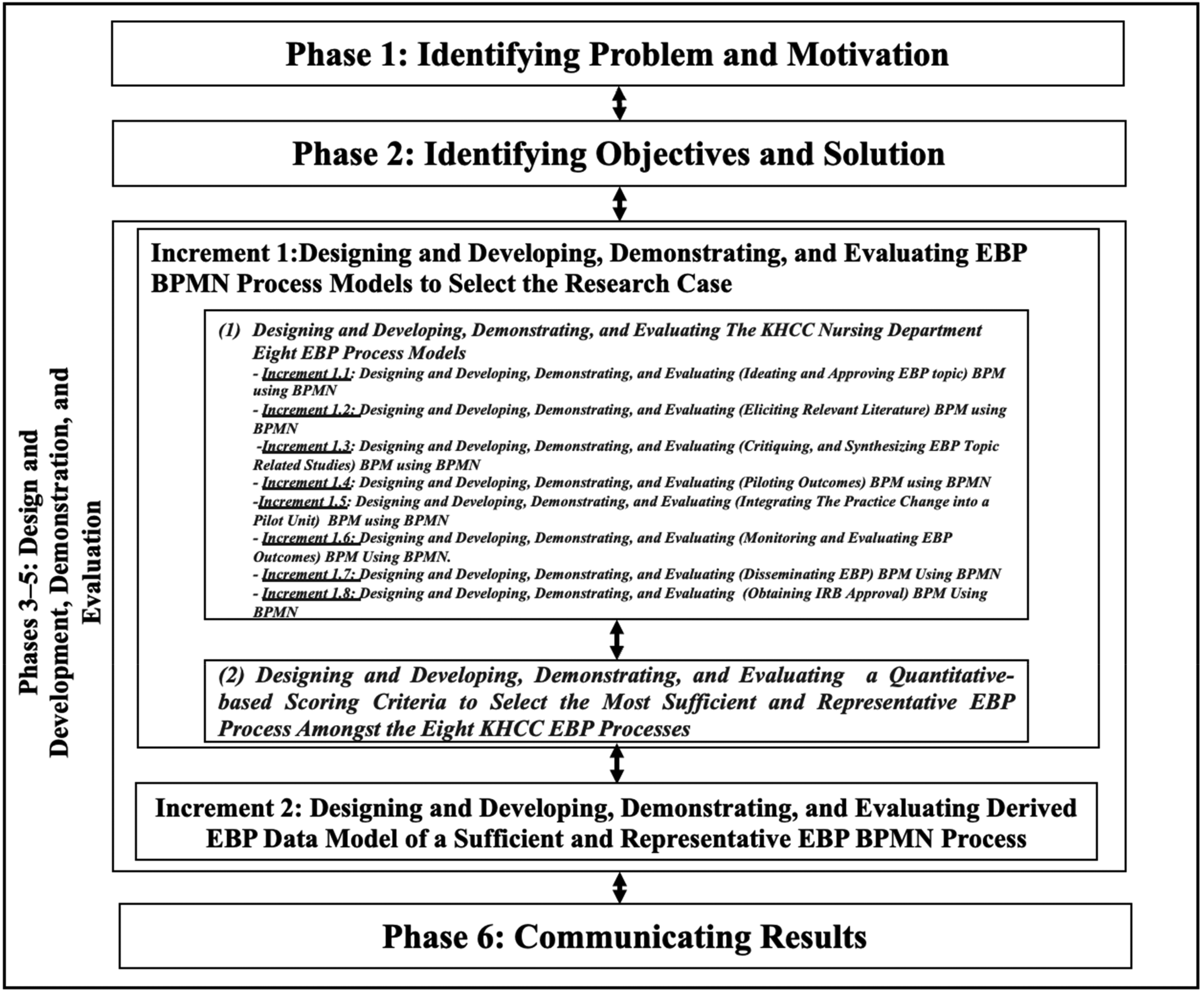
The research methodology.
Research design phase 1: defining the research problem
In this phase, the research gap analysis was synthesized as per the research problem and its motivation after the related literature review in relation to current EBP process practices in KHCC. The research problem states that the absence of standardized process models can create a significant gap in achieving digital readiness and in guiding the implementation of digital solutions and technologies within healthcare or cancer care organizations. Thus, this hinders optimizing the delivery of evidence-based care in healthcare settings. By addressing this problem, this motivates to improve the current situation by ensuring that nurses have access to the most up-to-date information in relation to agreed processes and needed data. Accordingly, the EBP team needs to be able to manage information using the respective EBP processes efficiently and effectively to improve patient care and to streamline their workflows, saving time and effort, with increased productivity and quality of patient care.
Research design phase 2: defining the research aim
Following the problem identification and motivation above in the first DRSM phase, this research was set to model KHCC EBP processes using BPMN and investigate whether such modeling yields a representative data model of EBP practices, as a base for the automatic capturing and management of data requirements for nursing evidence-based practices. Hence, addressing this aim may contribute to becoming closer to digital readiness and transformation. Accordingly, this research aims at “investigating whether using role-based business process modeling (with BPMN) reduces digital readiness gap of EBP processes in a cancer center.”
Research design phases 3–5: design and development, demonstration, and evaluation
This part is divided into two distinctive increments over the DSRM process three phases: (1) design and development, (2) demonstration, and (3) evaluation. Each of these increments yielded a significant artifact to achieve the aim of this research.
The 1st DSRM process increment: the design and development, demonstration and evaluation of EBP BPMN process models for the selection of the research case
This increment was concerned with designing and developing, demonstrating, and evaluating the final selected EBP process as the representative case study to address the aim of this research. This increment has two distinct sub-increments, where each of them implements one cycle of three phases of design and development, demonstration and evaluation as detailed below.
(1) Design and development, demonstration, and evaluation of the KHCC nursing department’s eight EBP process models Each of the eight KHCC EBP processes was designed and developed, demonstrated, and evaluated using the following research methods. Interview sessions were conducted (as needed with 60 min duration for each interview) and with one workshop. Both activities were led by a specialist in BPMN modeling with the presence of senior KHCC EBP domain experts. The interviews involved unstructured and structured styles and the workshop involved open-ended questions to gain a critical understanding of each of the eight KHCC EBP processes in terms of their process goals, roles, their interactions, flow of activities, data entities, and decision-making points. A 1-hour validation session was conducted through a semi-structured interview using the walkthrough approach with the KHCC Chief Nursing Officer and the Director of Nursing to confirm correctness, completeness, and consistency of the KHCC EBP processes and their BPMN process model elements such as roles, activities, data entities, and decision gates. This led to confirming the eight EBP BPMN process models, with one example in Figure 2 depicting the BPMN model of “Integrating a Practice Change into a Pilot Unit” EBP process. The delivered models paved the ground for establishing validated and agreed EBP process models, staff education, communication, collaboration, and future EBP process improvement. (2) Design and development, demonstration, and evaluation of quantitative-based scoring criteria to select the most sufficient and representative EBP process among the eight KHCC EBP processes, as the research case study.
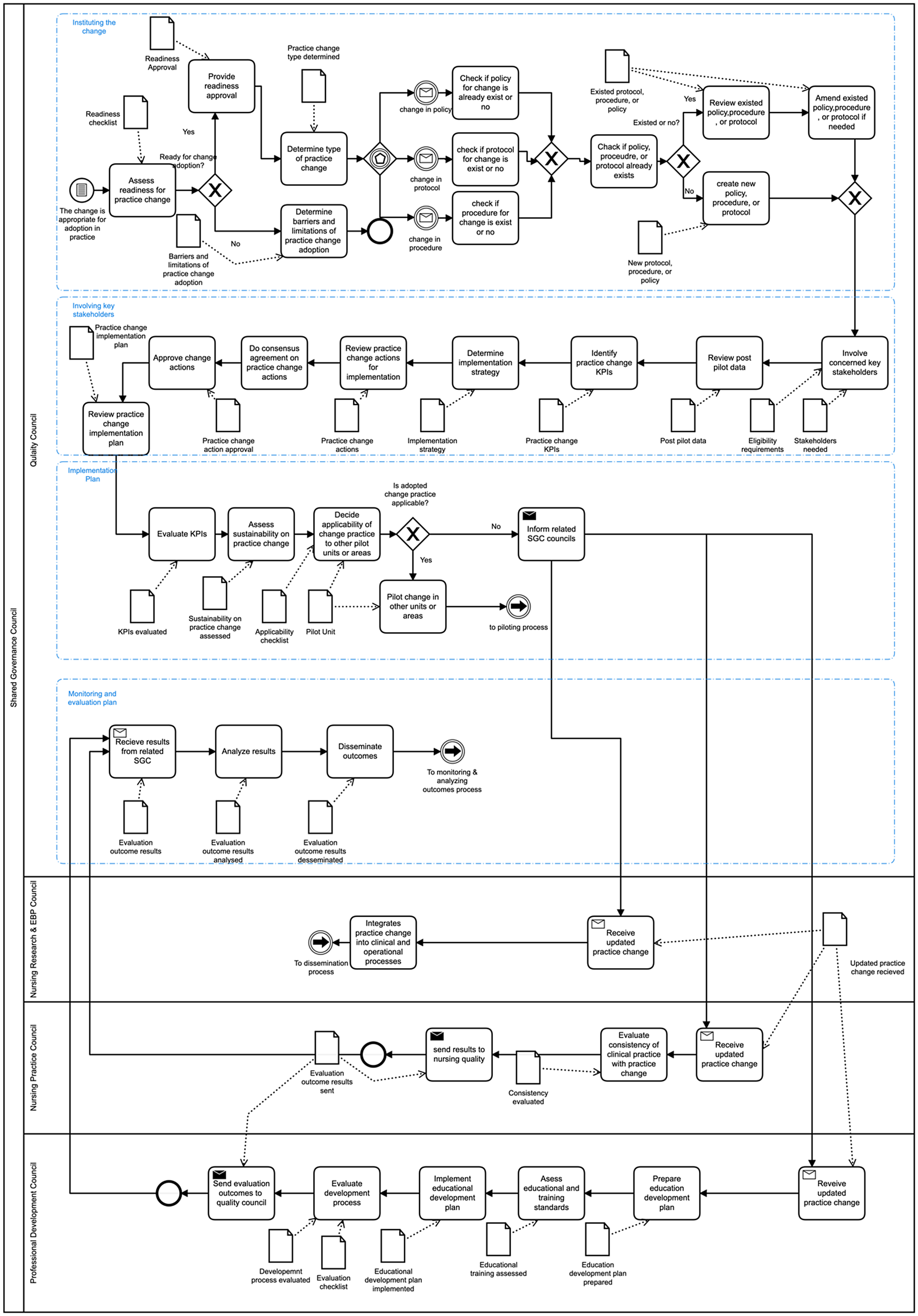
Integrating practice change into pilot unit process.
The authors have reviewed the KHCC nursing department eight EBP processes to select a sufficient and representative EBP process as a case study to inform whether role-based business process modeling can better reduce digital readiness gap in a cancer center. Accordingly, we have developed and followed quantitative-based scoring criteria to select the case study for this research, as the most sufficient and representative EBP process, among the eight KHCC EBP BPMN modeled processes. The rationale behind each scoring criterion is detailed below.
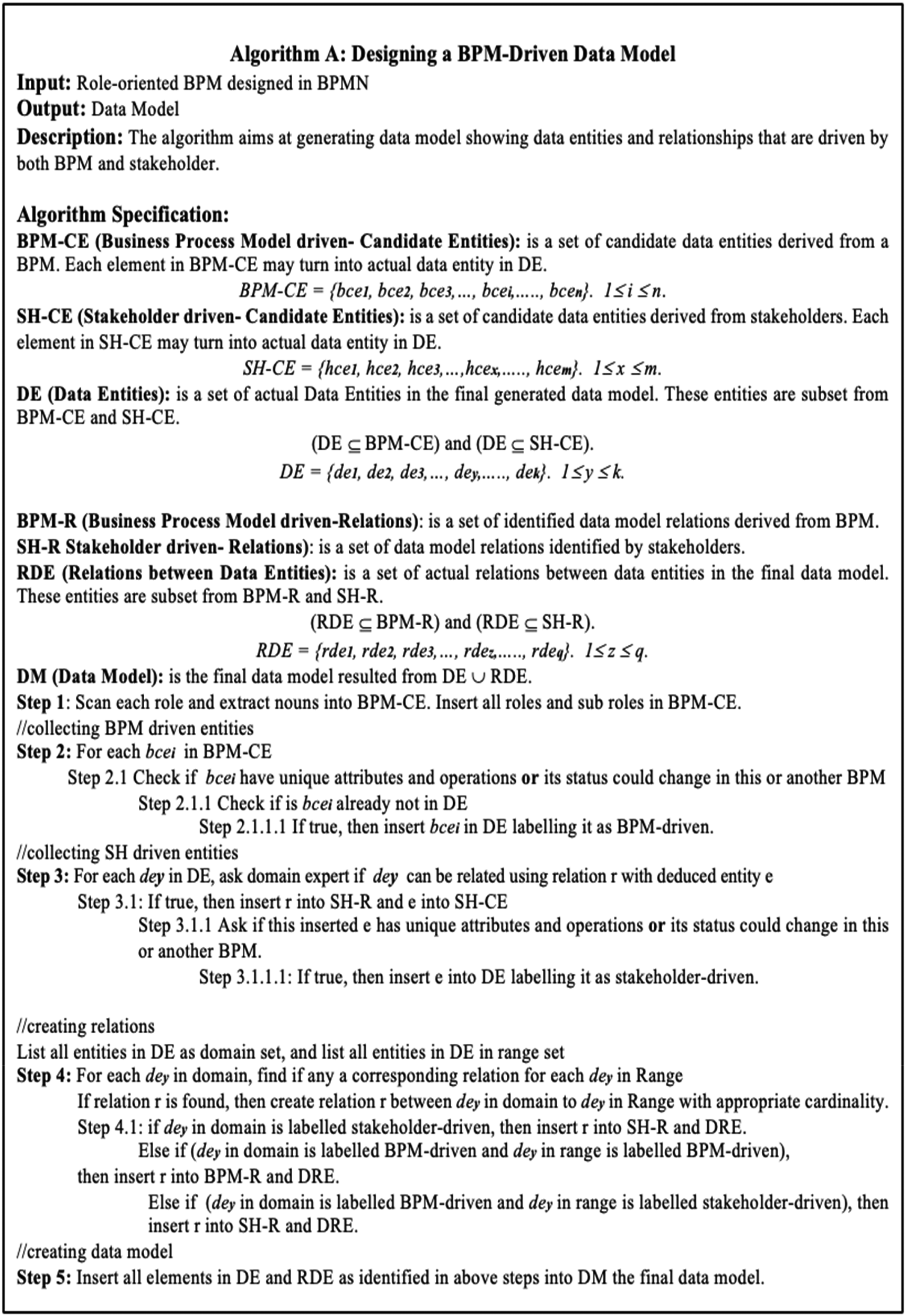
An algorithm for designing a BPM-driven data model.
The authors applied above criteria to each of the eight KHCC EBP processes, then “Integrating a Practice Change into a Pilot Unit” was observed to be the most sufficient and representative case study for this research as shown in Table 1. Senior members of the EBP team at KHCC have demonstrated and validated the results.
The quantitative-based scoring criteria to select the most sufficient and representative EBP process amongst the eight KHCC EBP processes.

Synopsis of the case study “Integrating A Practice Change into A Pilot Unit”
This process is aimed at handling the approval of practice change applicability in a designated pilot nursing unit. The process should proceed by determining the type of change, involvement of the concerned stakeholders in the change implementation, approving practice change applicability, informing shared governance council about approved practice change, and forwarding evaluation outcomes for monitoring and evaluation. This process should be executed after being called by the EBP project management process, namely piloting practice change. Also, three subsequent EBP project management processes depend on this process, and these are piloting practice change, monitoring and evaluating EBP outcomes or related measurement, and finally disseminating EBP as can be observed in Figure 2. This process has two main roles, and these are: Quality Council and Shared Governance Council (SGC). The latter role comprises three sub-roles, and these are: Nursing Research and EBP Council, Nursing Practice Council, and Professional Development Council.
In Figure 2, the reader can observe that the quality council appears as a central role in this process, responsible for driving the process forward and carrying out the necessary activities associated with a series of decision points (gateways) for its successful completion. Among areas that highlight implications for digital readiness are the requirements for the research council’s roles to minimize the risk of un-authorized process access. Therefore, this directs the EBP management and their IT specialists for the need to specify complex privileges in the respective EBP information systems to be enacted in support of such EBP process automation.
The 2nd DSRM process increment: the design and development, demonstration and evaluation of the derived EBP data model of a sufficient and representative EBP BPMN process
This increment was concerned with designing and developing, demonstrating, and evaluating an EBP data model derived from the sufficient and representative EBP BPMN process models (as an output from the 1st DSRM increment above). For the design and development phase, three interview sessions were conducted. Each consumed almost 60 min with the senior KHCC EBP domain specialists. The structured interviews involved close-ended questions with limited range of options in relation to an identification of data entities and their associated relationships using the research case study of the EBP BPMN process model in the section “The 1st DSRM process increment: the design and development, demonstration and evaluation of EBP BPMN process models for the selection of the research case.” A further 90 min validation session was conducted with the KHCC Chief Nursing Officer and the Director of Nursing to confirm the correctness, completeness, and consistency of all the EBP BPMN process data entities and associated relationships. Also, this validation involved determining whether each derived data entity is business process-driven or domain specialist-identified with further classification being quality-related data entity or not. In conclusion, this DSRM increment led to the construction of a UML-based EBP data model, 35 as shown in Figure 4, derived from the representative EBP BPMN process model shown in Figure 2. Figure 3 shows a special purpose algorithm, to systematically derive the EBP conceptual data model which comprised 44 conceptual data entities (36 EBP BPMN process-driven and 8 EBP domain specialist or stakeholder driven), as shown in Figure 4. Only five of these data entities were classified as quality-related.

The data model of integrating practice change into pilot unit.
Phase 6: communicating results
This phase was associated with disseminating the EBP BPMN process model and the EBP data model using internal workshops and journal publications such as the submission to this journal platform.
Results
In this research, results were presented in the two deliverables that are absent in the current EBP in KHCC. The first deliverable was the eight EBP BPMs specified and designed in BPMN. A representative example is shown in Figure 2 that was explained in section “The 1st DSRM process increment: the design and development, demonstration and evaluation of EBP BPMN process models for the selection of the research case.” The second deliverable was BPM-driven data model represented in the case study shown in Figure 4 and as explained in the section “The 2nd DSRM process increment: the design and development, demonstration and evaluation of the derived EBP data model of a sufficient and representative EBP BPMN process.” Further deliverable was the proposed algorithm for deriving the data model from respective role-oriented BPM as was shown in Figure 3. The designed BPM and associated data model contributed to reduce the identified gap for digital readiness and transformation according to Chief Nursing Officer and the Director of Nursing.
Discussion
Before this research was commenced, EBPs at KHCC were not modeled using industry standard process modeling languages such as the BPMN. KHCC EBP processes were manually attended to using paper-based forms and this was widening the gap to digital readiness excessively, let alone the absence of an EBP data model. In addition, changing management to these EBP processes was not based on process model implementation, and thus this was further digital readiness gap.
Digital readiness in an organization should be a “multi-level” preparedness construct upon all individuals, processes, departments, data assets, activities, and all linked units.30,31 Therefore, the KHCC EBP BPMN process models have represented a shared common visual construct that involved many actors in the nursing field of EBP. This increased visibility has promoted a shared understanding of current processes, which were essential for identifying areas for improvement and digital readiness for transformation. This has reflected on the potential generalization of research framework design in deriving EBP data models from a set of validated EBP BPMN process models in a cancer center. For example, in Figure 2, the Quality Council couldn’t execute the designated EBP process workflow without utilizing the EBP data and benefiting from SGC capabilities to attain the desired goal. 6 Also, the model in Figure 2 has provided a common language for EBP and IT teams. This has enabled them to collaborate more effectively to facilitate the enactment of EBP processes and development in the respective EBP information management systems. Moreover, the EBP BPMN process model in Figure 2, when aligned with the respective EBP information system's data model, in Figure 4, would promote higher level of digital readiness agility imposed by changes to EBP protocols, policies of the dynamic nursing environment in cancer care context.
Hospitals integrate EBP into clinical practice by adopting new practices or modifying the existing practices based on new research evidence or guidelines. EBP programs have ensured the availability of EBP education, time, and resources for the nurses to effectively implement the practice change. 36 Consequently, the newly developed EBP process data models, for example in Figure 4, contributes to attaining the aim of integrating evidence-based practice into clinical practice. This is because when EBP domain experts operationalize standardized representations of their processes along with the data consumed and produced by these EBP processes, this contributes to increase the stakeholder's accessibility involved in nursing and clinical practices. Using EBP BPMN models, KHCC EBP domain experts are now able to detect and trace EBP data processing activities that relate to respective entities in EBP data model as shown in Figure 4. The work in this research paves the ground for developing dashboard operated by the EBP team in a step towards the full enactment of all the eight interrelated EBP BPMN process models and in particular: (1) ideating and approving an EBP topic, (2) eliciting relevant literature, (3) critiquing and synthesizing EBP topic related studies, (4) piloting practice change, (5) integrating the practice change into a pilot unit, (6) monitoring & evaluating EBP outcomes or related measurement, and finally, (7) disseminating EBP, (8) obtaining IRB approval if needed. Before this research, these eight processes had no agreed EBP BPMN process model to automate their workflows that incorporate different nursing roles and committees’ communication, decision making, and around 200 EBP data entities with complex interrelationships. Therefore, this research has contributed to reducing the digital divide towards higher digital readiness, especially when data entity instances are managed by the respective EBP information systems.
Before the delivery of KHCC EBP data modeling, for example the data model in Figure 4, not only many EBP data entities were not identified or known, but also the relationships between them were not captured. Figure 4 depicts different kinds of EBP data entity relationships such as aggregation, composition, inheritance, and association. This has empowered the EBP team to take a data-driven and process-based approach for inspecting and informing evidence-based practices to attain higher levels of effective digital readiness. Furthermore, the data model derivation algorithm in Figure 3, though not yet fully automated, facilitated identifying and confirming EBP BPMN data entities. Using this algorithm, it is now possible to identify inefficient, redundant, ethically, or legally not compliant data entities. This clearly has reflected on a further requirement for digital readiness ahead of the digital transformation process in relation to the development of digital data governance models and framework.
According to nursing domain experts, incorporating EBPs (through BPMN process and respective data models) into the nursing practice empowers nurses to augment necessary scientific evidence while being involved in clinical decision-making and keeping up-to-date on advanced medical guidelines. Thus, this could result in promoting higher quality EBP-based care at reduced cost. Accordingly, this drives to developing and automating EBP processes into software systems that may contribute to organizational improvement of nursing practice, the working environment, and patient care outcomes. 1
Regarding conducting comparative analysis of the findings with other institutes, many cancer centers and healthcare organizations still rely on traditional, less structured methods for workflow documentation and process improvement. While BPMN has been recognized for its benefits in business process management, 37 its application in healthcare, particularly in EBP in cancer care, is not yet widespread or still in its early stages.38–40 The existing literature on BPMN and EBP in healthcare often lacks detailed case studies on the application of BPMN to complex, multidisciplinary workflows in cancer care. Much of the research has focused on general applications of BPMN in healthcare settings or on theoretical aspects of process modeling.20,22,38–41 Therefore, there is a current notable gap in comprehensive case studies that explore how BPMN has been employed in representing EBP in cancer care context, and this does not give enough space for comparison.
In this work, KHCC's advanced use of BPMN offers a model for how cancer centers can represent evidence-based practices into their operations along with their associated data model. This has included visualizing role-oriented multidisciplinary workflows along with the integration of respective data sources and objects. EBP BPMN models in KHCC has offered a clear and consistent way to document and visualize evidence-based workflows, which could aid in standardizing practices across different departments and multidisciplinary care teams. This consistency would help in benchmarking KHCC's EBP practices against industry standards and leads to identifying areas where KHCC excels or deviates from best practices. In future, and through the EBP BPMN deliverables, KHCC can track adherence to evidence-based guidelines, assess the impact of workflow changes, and iteratively refine processes based on continuous analysis and feedback. Deliverables in this work have provided a benchmark for other cancer centers and healthcare organizations looking to implement BPMN in their EBP workflows. Also, the deliverables have contributed to offering a reference point for best practices and demonstrated how BPMN can be employed to align with industry standards and enhance care quality.
The EBP BPMN-designed workflows developed at KHCC has offered a reference model that can be adapted and generalized to various healthcare settings, including public hospitals, smaller clinics, and international environments. Public hospitals often manage large volumes of patients and complex workflows like those at KHCC. EBP BPMN models at KHCC can be scaled to accommodate these larger operational scales by incorporating additional levels of details. This shall involve incorporating local protocols, resource availability, regulatory requirements, and other constraints. Smaller clinics may have fewer complex workflows compared to large cancer centers. EBP BPMN models can be simplified to focus on core processes and essential evidence-based practices relevant to the clinic's scope of healthcare services. Clinics can customize and reduce complex KHCC EBP BPMN models to reflect their unique patient populations, treatment modalities, and staff roles. International adaptation may also include translating BPMN models into local languages and adjusting them to align with regional healthcare infrastructure, resource availability, and other constrains. Collaborating with local healthcare experts ensures that models are relevant and feasible in diverse settings. And from here, we have proposed below generic guidelines as learned from literature to customize BPMN EBP models into other healthcare settings.
Review and incorporate local guidelines and standards: revisit KHCC EBP BPMN models and ensure they reflect local evidence-based guidelines, treatment protocols, and regulatory requirements. If not, customize workflows to align with national or regional healthcare standards and practices.20,42 Engage stakeholders in the customization process: collaborate with local healthcare professionals, multidisciplinary team, nurses, administrators, and patients to understand specific needs and challenges. Involve them in the design and validation of EBP BPMN models to ensure relevance and practicality.43,44 Stakeholders shall also identify potential risks and their respective risk management plan. Engaging stakeholders here would help in identifying some respective improvements in their EBP. Simplify and modularize EBP BPMN models: break down complex EBP BPMN models into modular components that can be customized for the purpose of scaling, that is either up or down, according to the size and scope of the healthcare setting to facilitate adaptation.
45
Ensure data integration into EBP BPMN models: revisit scoped EBP BPMN models and investigate that required data sources and/or objects are integrated in the workflows. This may require healthcare professional stakeholders to refer to the electronic health records in their information systems.
46
Also, they may identify some missing, but needed data sources. Provide training and support: offer training and support to healthcare staff on how to use and adapt BPMN models effectively in their healthcare settings. This shall also involve training on how to develop user-friendly documentation and resources to facilitate the design, development, implementation, ongoing use, and reference of their EBP BPMN models.47,48 Evaluate resulting EBP BPMN models: collect feedback from healthcare professional stakeholders to continuously refine and improve workflows based on practical experiences and desired outcomes.
48
The authors of this research have faced few practical challenges during the design of EBP BPMN models. The first challenge was clear in observing EBP experts’ lack of familiarity with BPMN and UML modeling tools and data analysis. This could have hindered implementation of this research. For example, it was required by the first author to conduct a tutorial session during elicitation and validation to EBP experts in KHCC to introduce the two languages’ purpose of use, their notations, and some examples. The lesson learned here was that it is recommended to employ standardized modeling languages to design EBP process workflows and data models, as the two languages approved their effectiveness in reducing familiarity and understandability gap between EBP experts and IT experts towards reducing the gap of digital readiness. Both languages have helped EBP professionals and IT people arriving at a common communication language via an industry standard business process modeling language such as BPMN and UML. In turn, this has helped in having a common agreement and understanding of the EBP processes and data models.
The second challenge was the decision to include and present the eight EBP business processes at KHCC in this article. Including complex representations in this research may be challenging for readers to comprehend, especially those unfamiliar with the specific modeling techniques or domain. This could have hindered the dissemination of knowledge and limited the accessibility of the research findings. Complex models might lead to misinterpretation, leading to misunderstandings or incorrect assumptions about the actual business processes being studied. This could have undermined the validity and reliability of the research findings. Therefore, the researchers have identified criteria as shown in Table 1 to select the most representative EBP process among the eight. This is one applied example to overcome this challenge. The lesson learned here was that it is recommended to identify criteria that cover core aspects or attributes given in the complex modeled processes to select a one representative example as a case study of the research work. This has enhanced the clarity of the research article and facilitated effective communication of the findings to a broader audience.
The third challenge was the complexity of EBP process model design due to the multidisciplinary workflows that have required careful attention by the analyst, who is not a domain expert, during the elicitation, design, analysis, and validation. Iterative designing and validation sessions were conducted to reduce possibility of chances of errors. The lesson learned here that it is recommended to iteratively revisit complex EBP BPMN process and data models and engage EBP multidisciplinary stakeholders in the elicitation and validation sessions, as complex EBP process models have required frequent updates to correct some errors and reflect changes in clinical practices or organizational workflows. This has helped in closely aligning the models to the current practice to towards preparing EBP for digital readiness.
Although the delivered work is novel and has contributed towards digitalizing EBP domain, it is necessary to point to some dark sides. The focus on standardized role-based business process modeling and data modeling may overlook the complexities and subtle differences of actual clinical practices. Cancer care has involved deeply personalized patient interactions and medical decision-making that cannot always be neatly standardized or reduced to data models. Another dark side was seen in the implementation challenges. Implementing standardized models across diverse clinical settings can be highly challenging. This research has not accurately addressed the practical obstacles such as resistance from healthcare professionals, interoperability issues with existing systems, and the substantial costs associated with system upgrades and training. Finally, neglecting human factors in EBP while emphasizing on digital readiness was a dark side that needs not to be overlooked. Effective evidence-based decision-making often has relied on the tacit knowledge and experience of healthcare professionals, which cannot always be codified into standardized models. The three dark sides have limited the delivered research in this article.
Finally, our future plan entails the representation of EBP quality requirements and their respective metrics in both the EBP BPMN and EBP data models as they do not exist in this research. This has been observed for example, when assessing the organization's readiness for adopting a change in evidence-based practice, identifying eligible stakeholders for implementation, assessing sustainability of evidence-based practice change, assessing applicability of evidence-based practice change, and evaluating consistency of clinical practice with respect to evidence-based practice change. These are examples where such alignment is needed between EBP BPMN process and data models, as can be inferred in Figures 2 and 4. Such alignment with digital readiness is of highest priority in the future work to ensure EBP data governance to satisfy requirements for scientific merit and strict compliance to related regulations and support in terms of new knowledge, innovations, and improvements requirement. One future work is to design and develop business process architecture for EBP that shows a blueprint of interrelated processes. 49 Process architecture is a daily tool for strategic and operational management in an organization that prioritizes service quality and continuous development.49–51 It is more than simply a model.
Incorporating a big data approach into EBP process can enhance digital readiness and transformation by leveraging data as a strategic asset to drive decision-making in identifying data quality measures through tracking sequence of events like the work conducted in targeted medicine. 52 Using the big data approach in EBP BPMN models, the workflow can be optimized using some algorithms where integrated data in EBP can help in intelligent predication and classification in EBP.53,54 Such predication can be obtained from EBP BPMN models to inform duration of patient hospital stay, treatment, or follow up meetings with help of machine learning. 55 The next step after having EBP processes visualized is to optimize them in terms of minimizing wastes and resources, as can be learned from the work applied using intelligent systems. 56
Conclusion
Undertaking a digital transformation process through achieving digital readiness has become increasingly prevalent attempts by healthcare organizations. This research has concluded that linking evidence-based practices with their respective BPMN modeled processes and derived data models is a pre-requisite to reduce significant gap for desired digital readiness, as demonstrated through the example of KHCC—an internationally accredited cancer center—in the study of integrating evidence-based practice into clinical practice in cancer care context. A further corollary of this research is that adopting new evidence-based practices or modifying existing ones based on new research evidence or guidelines can be visually traced through EBP BPMN process models. Thus, this alludes towards achieving higher digital readiness through enacting the designated EBP BPMN process models aligned with their data models within a comprehensive EBP information management system, accessible by all stakeholders involved in EBP-based nursing under strict and automated EBP data governance.
Furthermore, it has been observed that the EBP BPMN developed process models facilitate EBP projects’ follow-up, by identifying challenging project phase(s), and tracing communication of various involved personnel, councils, committees, and entities. Therefore, the EBP management can better monitor EBP projects through the responsible EBP councils and teams, more timely-bound. Also, EBP BPMN process models can be utilized by EBP programs to ensure higher availability of EBP education, time, and resources for nurses to effectively implement practice change. Therefore, once these EBP BPMN process models are aligned with the EBP process transformation for the respective hospital, the overall EBP data model directs harvesting EBP data in alignment that support new knowledge, innovations and improvements requirements. Consequently, EBP management in such hospitals can perform data analytics to identify EBP trends, patterns, and insights that can inform strategic decisions around evidence-based practices in hospital or cancer center. Therefore, this is anticipated to enable nursing departments, at KHCC for example, to stay ahead of emerging trends and technologies to make informed decisions around evidence-based practices in nursing and ultimately achieve sustainable automation of EBP.
Finally, achieving digital readiness to inform higher levels of digital transformation is a complex and challenging aim to attain, not just simply through enacting BPMN process models aligned with a holistic EBP data model for the respective EBP information management systems. Several key factors need to be considered such as organization's digital readiness cultural, competencies, skills, technical infrastructure, and maturity and complexity of its business processes. Further work has been planned in relation to developing EBP-based blueprint architecture of EBP-based processes linked with EBP governance framework, with notable examples adopted from other disciplines. Incorporating a big data approach into EBP process offers future contributions to KHCC. It is anticipated to enhance data-driven decision making, patient personalization, predictive analytics, and resources optimization.
Footnotes
Acknowledgements
The work would not be possible to finish without the very dedicated collaboration and support of the KHCC Nursing Department and their EBP team in all the stages of the research project development. The authors are grateful to the support provided by King Hussain Cancer Centre, Amman, Jordan, and Al-Zaytoonah University of Jordan, Amman, Jordan.
Contributorship
YO developed and led the research design of the paper, the method for developing digital readiness through process-model driven conceptual data modeling while re-modeling evidence-based practice process in KHCC, and also led completing the construction of the paper. MA led the writing and reflecting on evidence-based practice, co-participated in the identification and validation of conceptual data entities for the evidence-based practice process applied to, contributed to writing and reviewing the final draft of the paper. AA led the writing and reflecting on evidence-based practice, co-participated in the identification and validation of conceptual data entities for the evidence-based practice process applied to, contributed to writing and reviewing the final draft of the paper. HM provided an initial evidence-based practice process model which was revisited and remodeled by the research team: YO, MA, and AA. MO directed the overall research project in all its phases, contributed to writing in the paper, and its final critical contents review and structure.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
No human or animal participants were involved, and no patient data was collected. No human-identifiable data is reported in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Gurantor
YO.