
Abstract
Background
Hypertension and diabetes are typically managed in primary care settings, where continuous and tailored care based on continuity in daily life is essential to improve health outcomes.
Objective
To address the shortage of human and material resources in primary care and to enhance health outcomes, we developed and implemented a comprehensive digital medicine platform in a real-world setting.
Methods
A patient application (app) and a web app for healthcare providers were developed to enable bidirectional communication between patients and healthcare providers. Primary physicians and care coordinators utilized this platform to deliver personalized care management. To manage multiple patients with limited staff, automated message generation logic was used.
Results
Using the app, patients could self-measure blood pressure and blood glucose level, receive feedback from healthcare providers, and obtain personalized medication management, disease education, and lifestyle guidance regarding smoking, alcohol consumption, and exercise. Healthcare providers can view the data generated by the patient app, in real time, on the web app, and immediately send messages when an action is required. An evaluation of effectiveness was conducted with 502 patients in the intervention group and 502 patients in the control group over a 24-week intervention. In the intervention group, systolic blood pressure decreased by 3.8% (P < 0.001), diastolic blood pressure by 3.4% (P < 0.001), body mass index by 1.6% (P < 0.001), and waist circumference by 1.5% (P < 0.001). HDL cholesterol increased by 2.4% (P < 0.05), and triglycerides decreased by 5.4% (P < 0.05).
Conclusion
This study demonstrated that the adoption of a digital medicine platform is effective and essential for continuous patient management in primary care. Information and communications technology-based tools and applications are becoming increasingly important in healthcare, and our study has provided valuable insights into the management of chronic diseases.
Introduction
Non-communicable diseases (NCDs) refer to chronic diseases such as hypertension and diabetes, which are major concerns worldwide. NCDs account for 74% of global deaths. They arise from a combination of factors, such as lifestyle habits, environment, and genetics.1–4 In South Korea, NCDs accounted for 79.6% of total deaths, as of 2021. 5 During the coronavirus disease 2019 (COVID-19) pandemic, obesity—a major risk factor for both hypertension and diabetes—has shown a continuous increase, with prevalence rising by 38.8% after the 2020 outbreak compared to a decade ago, representing a 7.4% increase. 5 Given that obesity is closely linked to insulin resistance, increased blood pressure, and systemic inflammation, its rising prevalence during the pandemic has contributed to the worsening burden of hypertension and diabetes, increasing the risk of cardiovascular complications. Additionally, the management of modifiable risk factors, including smoking, alcohol intake, and obesity, remains stagnant or at a disappointingly low level. 5 These trends highlight the urgent need for continuous and comprehensive management strategies to prevent complications such as cardiovascular diseases6–8 and cancers9–11 particularly through innovative, technology-driven approaches. Meanwhile, one of the commonly proposed solutions is strengthening primary healthcare with a focus on chronic disease management models.12–14 In south Korea, compared with the Organization for Economic Cooperation and Development (OECD) average, the proportion of NCD management in primary healthcare settings was only 37.8% in 2016, indicating a concentration of cases in higher-level hospitals. 5 To address this issue, led by the Ministry of Health and Welfare, South Korea has implemented chronic disease management pilot projects in primary healthcare since 2007, starting with registration and management initiatives for conditions such as hypertension and diabetes. 15 This effort continues with the Primary Healthcare Chronic Disease Management Pilot Project initiated in 2019. 15 Through this project, primary care physicians in local communities receive assistance from registered nurses or dietitians, who act as care coordinators. They collaborate to establish individualized care plans for patients with hypertension and diabetes, enabling effective patient care. Daily monitoring of medication, diet, exercise, and lifestyle habits is essential for disease management, but there are limitations in comprehensively managing a large number of patients due to restricted medical personnel and resources. 15 With the advancement of digital healthcare, efforts are being made to utilize mobile phone-based health management services to assist patients in monitoring their everyday health and improving health outcomes.16–20 Recent studies have demonstrated the effectiveness of mobile-based health interventions for managing diabetes and hypertension. Islam et al. highlighted the role of smartphone apps in improving diabetes medication adherence, 16 while Eberle et al. showed that telemedicine interventions lead to better glycemic control. 19 For hypertension, Kario et al. introduced digital therapeutics systems that successfully reduced blood pressure through AI-driven monitoring and guidance.17,18 Additionally, Yang et al. reported improved clinical outcomes using a mobile glucose-monitoring system in primary care settings. 20 Despite these advancements, challenges remain in integrating digital health solutions into routine care, especially for patients managing both conditions simultaneously. This study aims to address these gaps by developing and evaluating a mobile-based health management application tailored for diabetes and hypertension patients, with a particular focus on its feasibility and clinical impact in primary healthcare settings. Specifically, it seeks to enhance chronic disease management and treatment rates by overcoming the limitations of the South Korean government's Primary Care Chronic Disease Management Integrated Pilot Project initiated in 2019. While the project aimed to strengthen chronic disease care in primary healthcare settings, challenges such as the lack of integration with hospital information systems, manual data entry errors, and difficulties faced by elderly patients in using digital tools hindered its long-term implementation. To overcome these limitations, we designed an ICT-based platform that enables personalized patient management while ensuring accessibility and feasibility for both patients and medical professionals. This study focuses on validating the practicality and effectiveness of this digital health model through a feasibility test in real-world primary healthcare settings.
Methods
Mobile phone app for patients
The mobile phone application was designed to enhance patient convenience and motivation. The application features functionalities such as the creation of consent forms, self-reporting records, Bluetooth integration with wearable devices, provision of personalized content, alarm functionality, and a question-and-answer feature. Prior to the usability study, all functions, especially bluetooth integration with wearable devices, was tested separately to ensure proper functionality and data synchronization. The system was confirmed to operate smoothly, allowing seamless transmission of patient health data to the platform.
In addition, the app supports real-time monitoring of health metrics such as blood pressure, blood glucose, and weight through integration with wearable devices, while also allowing users to manually input lifestyle data, including meals, exercise, and medication adherence. This information is synchronized with a web app for medical staff, enabling tailored interventions and personalized care plans based on the patient's lifestyle and medical history. The app is designed for accessibility, featuring an intuitive interface, large text, and gamification elements such as progress tracking and rewards to maintain user engagement. Developed for both Android and iPhone Operating System (iOS) platforms, the app empowers to actively manage their health and adhere to clinical protocols.
Web app for medical staff
A web app was designed to enhance feasibility and safety for medical staff. A dashboard for patient management was developed and interfaces for individual patient health analyses were created. Integration with the HIS was performed to improve work efficiency. Moreover, a feature to provide personalized feedback to patients was designed and an additional review feature was implemented to minimize errors. The web app also incorporates automated care plan generations, classifying patients into intensive or general management groups based on health data from the patient app. Additionally, a rule-based model supports real-time monitoring and tailored interventions, while the dashboard enables efficient prioritization of patients requiring intensive management.
Moreover, the study incorporated an automated logic system to enhance the operational efficiency of physicians and care coordinators. During the care plan development stage, individual care plans were formulated considering the patient's current health status. Additionally, the study introduced a logic for delivering tailored educational content that has been integrated into mobile phone and web applications. Even among patients diagnosed with hypertension and diabetes, their medical conditions and risk factors vary significantly. To efficiently provide personalized interventions tailored to each patient's specific issues, we developed a rule-based management algorithm that incorporates key factors such as blood pressure, blood glucose levels, and problematic lifestyle habits. This algorithm is designed to assist healthcare professionals in formulating optimized treatment plans for individual patients.
Feasibility test: implementation of the system in primary care
A feasibility test was conducted to evaluate the feasibility and effectiveness of the platform. The primary task of the feasibility test was to evaluate whether the use of the developed platform resulted in significant improvements in clinical indicators such as glucose levels and blood pressure (BP). Additionally, assessing patient and healthcare provider satisfaction with the platform was included as a supplementary task.
Participants were recruited from primary care clinics through posters and brochures that provided information about the study. Patients who were interested in participating voluntarily contacted the research team for further details. Eligible participants were adults diagnosed with hypertension or diabetes who were taking medication for their condition. There were no gender restrictions, and any adults (age over 20) meeting these criteria were eligible to participate. Once patients expressed interest, the research team provided a detailed explanation of the study, including its purpose, procedures, and potential benefits and risks. Participants then provided written informed consent before enrollment. The study was conducted in eight primary clinics located in Seoul and Bucheon City, Gyeonggi-do, over a 24-week intervention. While both groups received care from their existing primary physicians, the intervention group also utilized the application developed in this study for health management. We explained the study and obtained informed consent from the individuals who agreed to participate. Upon completing the feasibility test, the effectiveness of the model was evaluated using clinical indicators, participation level, and satisfaction ratings. User surveys examined perceived usefulness, perceived ease of use, and satisfaction with the service. Participants rated their level of perceived importance on a 5-point Likert scale: (1) strongly disagree, (2) disagree, (3) undecided, (4) agree, and (5) strongly agree. 21 Cronbach's alpha was used to measure the internal consistency of the survey. 22 The survey was conducted anonymously to ensure participant privacy and reduce potential response bias.
For all participants, waist circumference, body mass index (BMI), blood pressure, fasting serum glucose, glycated hemoglobin A (HbA1c), total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides were measured before and after the 24-week intervention. The effectiveness of the intervention was evaluated based on these tests. Statistical significance was defined as a two-sided P-value of < 0.05. All analyses were conducted using R software (version 4.1.1).
Focus group interview
Focus group interview (FGI) was conducted to collect qualitative data exploring experiences from medical professionals. The interview process involved six primary clinics located in Seoul and Bucheon City, Gyeonggi-do. Three registered nurses (RNs) working as researchers and experienced in conducting research facilitated the FGI sessions. Participants included primary care physicians and care coordinators from each clinic who were directly involved in using the platform. Key questions focused on the following areas:
Opinions on the dashboard's usability for viewing patient data at a glance. Opinions on features for organizing and managing detailed patient records. Opinions on effectiveness of the manager page in supporting clinical tasks. Opinions on the ease of evaluating patient conditions after care plan implementation. Opinions on difficulties and suggestions for improving the management of intervention messages. General feedback and suggestions for improving the overall system.
This study was approved by the Institutional Review Board (IRB) of Kangbuk Samsung Hospital (IRB number: KBSMC 2020-07-026-012). All the participants received a sufficient explanation of the research and voluntarily agreed to participate.
Results
Three strategies have been established to alleviate the burden on medical professionals and enable effective personalized patient management: automation, development of a mobile phone application (app) for patients, and creation of a web app for medical professionals (Figure 1).
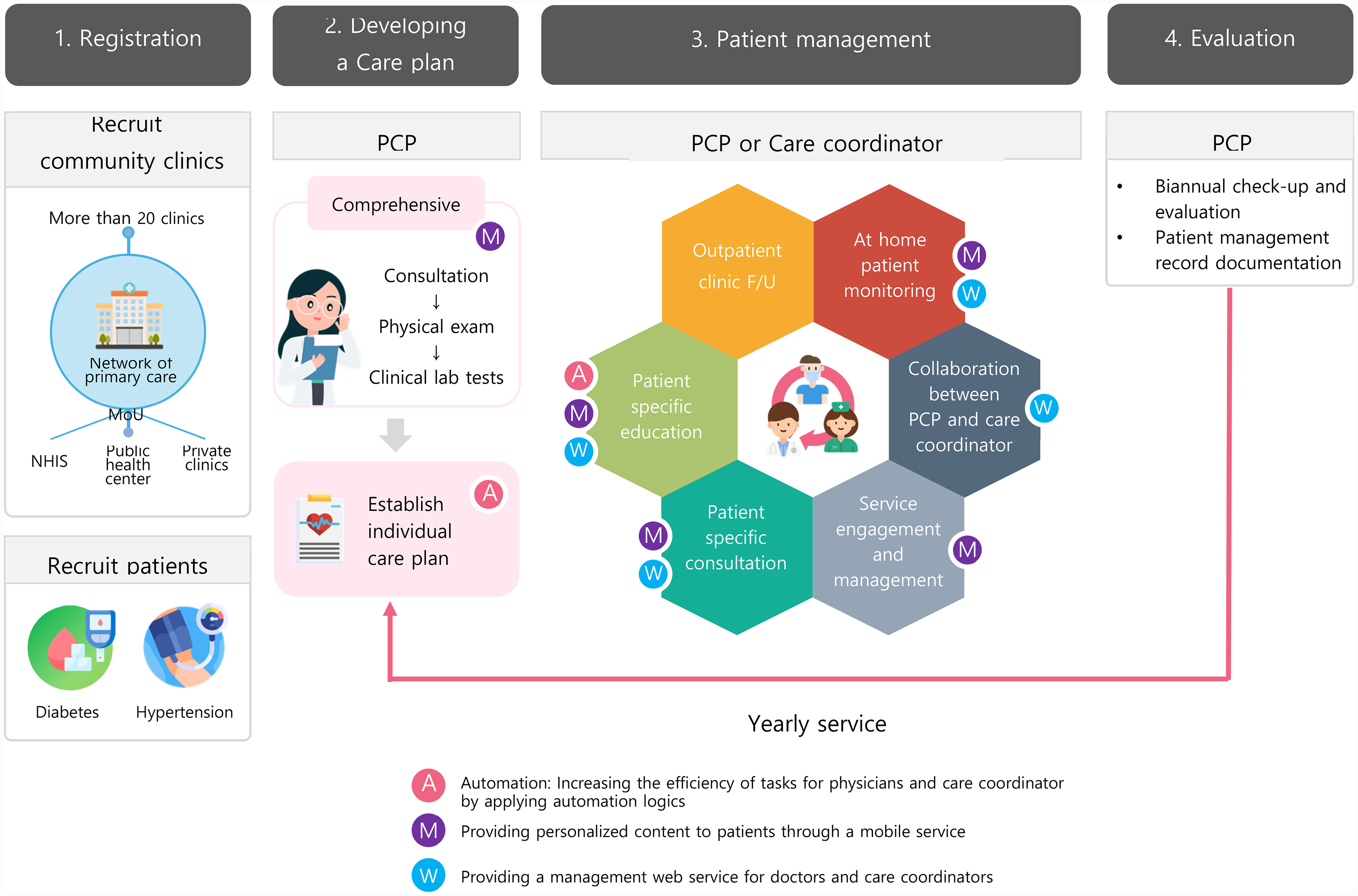
Implementation of additional features for chronic disease management program: automation, mobile phone service, and web service.
Mobile phone app for patients
In this study, a mobile phone app was developed with the aim of increasing patients’ self-care abilities to personally manage their chronic conditions and enhance communication with medical professionals. There are three main features: smart device connectivity and self-reporting, personalized health content provision, and integration with hospital information systems.
Smart device connection and self-reporting
We developed a function to integrate blood pressure monitors, glucose monitors, and body composition scales. Patients can measure their lifelogs, such as blood pressure, blood glucose, and weight, and check them at any time by using the app. Moreover, it is possible to check the trends over the previous 7 days to understand the patterns of change. In addition, the app allows users to manually enter information regarding their meals, weight, medication intake, exercise, smoking, alcohol consumption, and sleep, thereby enabling them to understand their health situation at a glance. Such patient-generated health data are accumulated in the app and then transmitted to a web app for medical professionals. Medical staff can then send customized intervention messages based on this information, and patients can receive these messages through the app to personally manage their health (Figure 2).

Mobile phone app: smart device connection and self-report.
Personalized health content provision
Based on the patient's lifestyle behaviors, such as smoking, alcohol consumption, physical activity, and medical history, a tailored care plan was provided. The care plan was established by the primary physicians, and patients were assigned to either an intensive management group or a general management group. Subsequently, personalized disease information, self-management methods, and educational materials for correcting poor lifestyle habits were provided through the app. Moreover, patients received lifestyle habit missions suited to their health behaviors; smokers receive a smoking cessation program, high-risk consumers of alcohol receive a moderation program, and patients requiring exercise receive a program designed to increase their physical activity in daily life (Figure 3).

Mobile phone app: personalized health content provision.
Integration of app to hospital information system
This feature enables users to check the results of blood tests conducted at the hospital or enter the results directly, enabling them to be informed about their current state at any time. Additionally, it enables users to view their prescription history and, if necessary, set alarms for convenient medication management, thereby enhancing medication adherence (Figure 4).

Mobile phone app: medication and test results inquiry through hospital information system integration.
Web app for medical professionals
A web app was developed to enable precise and rapid management based on the individual conditions of patients and for the convenience of medical professionals.
Establishment of patient specific care plan
Based on the data integrated from the patient app, this feature automatically establishes care plans according to the severity of the condition. The web app for medical professionals automatically classifies new patients diagnosed with chronic diseases such as unstable blood pressure/blood glucose control, complications, and undergoing insulin therapy, as requiring intensive management, into the “Intensive Management Group.” Patients diagnosed with hypertension or diabetes, excluding those in the intensive care group, were automatically classified into the “General Management Group.” In the intervention group, 418 participants were selected from the general management group and 84 from the intensive management group. Furthermore, the goals for each management group were automatically set based on patient-generated health data and comorbidities. Medical professionals can review and, if necessary, modify the plan that was set automatically and finalize the individual care plan for the patient by setting goals for areas that require additional education and counseling. The established care plan can be viewed by patients in the app.
Dashboard and patient management summary
On the dashboard, primary physicians and care coordinators are presented with reports that enable them to understand a patient's health status and health information on a single screen. Particularly, patients whose disease management was inadequate and who are priority targets for intensive management are categorized by type, enabling easy access for managers (Figure 5). Additionally, a summary of patient management is provided, which enables the assessment of the achievement level of each patient's care plan, disease control rate, and lifestyle improvement rate (Figure 6).

Web app for medical professionals: establishment of dashboard and care plan.
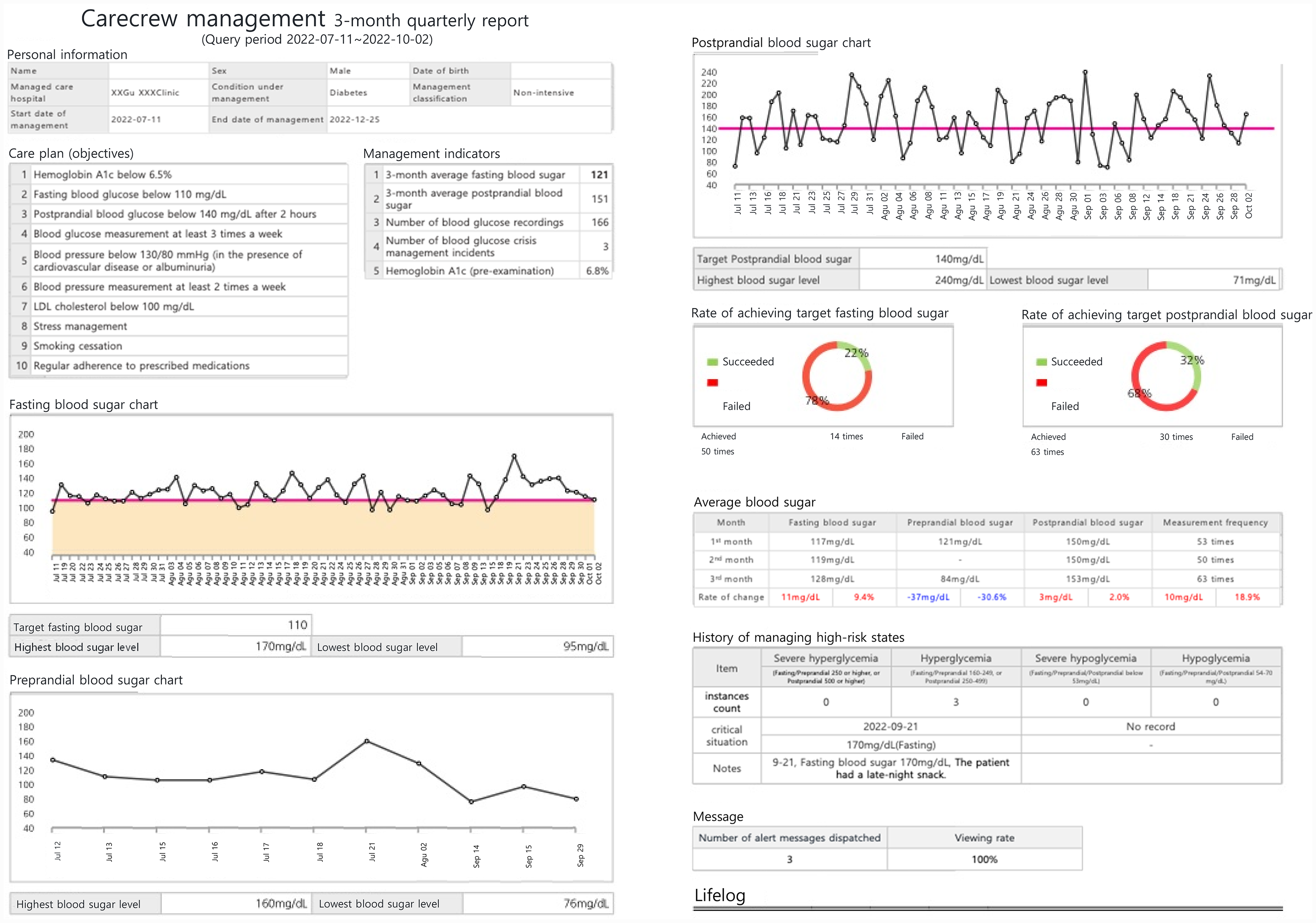
Web app for medical professionals: patient management summary.
Rule-based model for patient-specific care
A rule-based model was developed for patient-specific care. The analysis of real-time patient monitoring data has been utilized in patient management. It contains eight components that automatically monitor patient lifelogs, such as blood pressure, glucose level, physical activity (including step counts), body weight, pharmacotherapy adherence, smoking, alcohol consumption, and sleep hygiene. Based on the data produced by the patient app, a rule engine was developed to automatically provide intervention content based on the results (Supplemental figures). Medical professionals can confirm via a web app whether to provide the necessary content to the patient based on the automatically generated intervention messages, depending on the patient's current state.
Feasibility test
The feasibility test was conducted between May 2022 and February 2023 and involved 502 participants in the intervention group (279 with hypertension, 223 with diabetes) and 502 in the control group (290 with hypertension, 212 with diabetes). Table 1 presents the basic characteristics of the study population. The case and control groups consisted of 502 individuals each, with an identical sex distribution of 265 males and 237 females. The mean age of the intervention group was 60.06 years and the mean age of the control group was 64.64 years. In the intervention group, diastolic blood pressure, BMI, HDL cholesterol, and LDL cholesterol were significantly higher, whereas fasting serum glucose and triglycerides were lower.
Baseline characteristics.
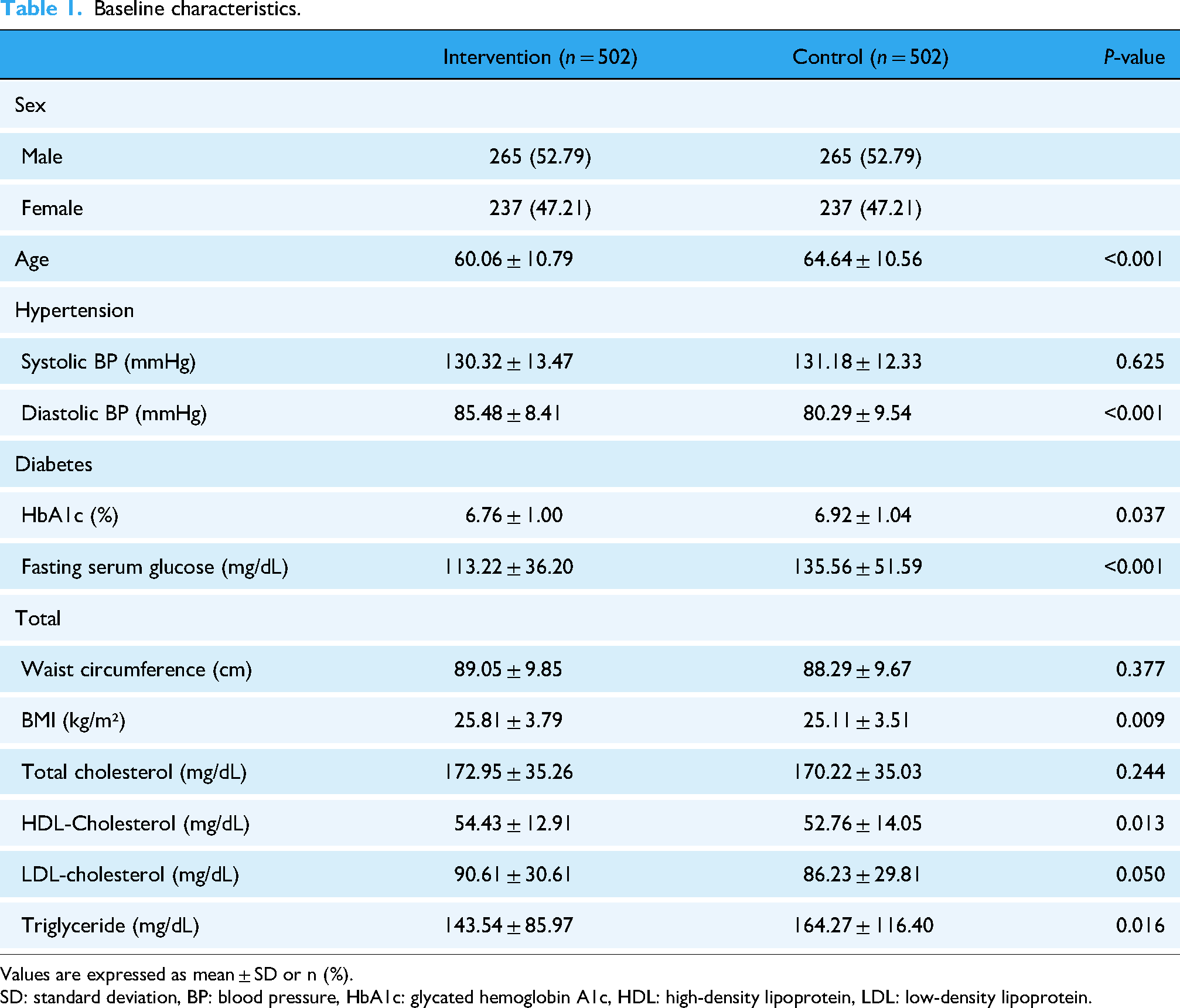
Values are expressed as mean ± SD or n (%).
SD: standard deviation, BP: blood pressure, HbA1c: glycated hemoglobin A1c, HDL: high-density lipoprotein, LDL: low-density lipoprotein.
Table 2 shows a comparison of the differences between the case and control groups before and after 6 months. Prior to analysis, the normality of the variables was assessed using the Shapiro–Wilk test, which revealed that all variables except systolic blood pressure in the intervention group did not follow a normal distribution. Accordingly, the Wilcoxon signed-rank test was applied for the analysis. Additionally, effect sizes were calculated using Cohen's r to complement the statistical significance results with values interpreted as very small (<0.1), small(<0.3), moderate(<0.5), or large(≥0.5) effects. In the intervention group, all indicators improved, and the Wilcoxon signed-rank test showed significant improvements in systolic blood pressure, diastolic blood pressure, waist circumference, BMI, HDL cholesterol, and triglycerides. The systolic blood pressure of hypertensive patients decreased by 3.8% from 130.32 in the pre-test to 125.37 in the post-test (P < 0.001, effect size = 0.352). Among 67 high-risk patients with systolic blood pressure greater than 140 in the pre-test, 40 patients improved to less than 140 in the post-test, reducing the mean systolic blood pressure of the high-risk group from 148.31 to 130.24, a 12.2% decrease. The diastolic blood pressure of the hypertensive patients significantly decreased by 3.4% from 85.48 to 82.56 (P < 0.001, effect size = 0.343). The HbA1c and fasting blood glucose levels of patients with diabetes decreased by 0.7% and 3.5%, respectively. The mean waist circumference and BMI of all patients significantly decreased by 1.5% and 1.6%, respectively (P < 0.001, effect size = 0.359, 0.513, respectively), total cholesterol and LDL cholesterol decreased by 1.4% and 2.3%, respectively, HDL cholesterol significantly increased by 2.4% (P < 0.05, effect size = 0.139), and the triglycerides significantly decreased by 5.4% (P < 0.05), showing an overall improvement compared to 6 months earlier. In contrast, the control group showed significant differences in three parameters: systolic blood pressure, diastolic blood pressure, and HDL cholesterol; however, systolic blood pressure and diastolic blood pressure increased compared to 6 months prior. The Wilcoxon rank-sum test revealed significant differences in the 6-month changes between the case and control groups for four parameters: systolic blood pressure, diastolic blood pressure, waist circumference, and BMI (P < 0.001, effect size = 0.285, 0.316, 0.262, 0.320, respectively). For systolic blood pressure, diastolic blood pressure, and waist circumference, the direction of change differed between the groups; the intervention group had a decrease (negative direction), and the control group had an increase (positive direction).
Changes of metabolic risk factors after intervention for 24 weeks.
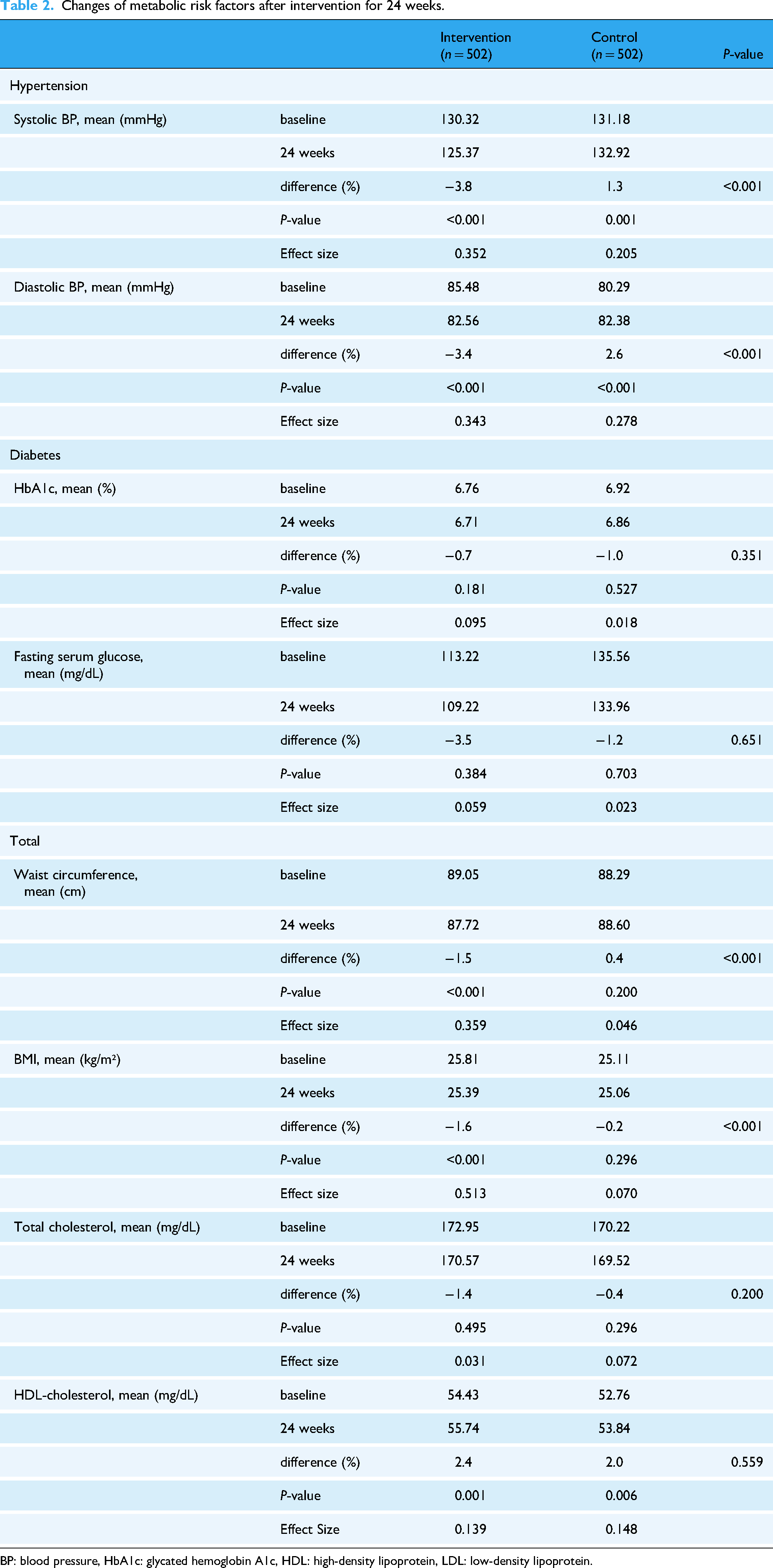
BP: blood pressure, HbA1c: glycated hemoglobin A1c, HDL: high-density lipoprotein, LDL: low-density lipoprotein.
Sensitivity analysis was conducted to assess the robustness of the intervention's effects among high-risk subgroups. For hypertensive patients with baseline systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, the mean systolic blood pressure decreased significantly by 8.7% (P < 0.001, effect size = 0.777) in the intervention group compared to 1.48% in the control group. Similarly, diastolic blood pressure in the intervention group decreased by 7.1% (P < 0.001, effect size = 0.688), while the control group showed a negligible reduction of 0.4%. For diabetic patients with baseline fasting glucose ≥ 126 mg/dL or HbA1c ≥ 6.5%, fasting glucose decreased by 8.9% in the intervention group to 4.4% in the control group (P = 0.004, effect size = 0.259) (Supplemental Table 1).
After the 24-week intervention, a satisfaction survey was conducted in the intervention group (Table 3). Satisfaction with the usefulness of the health information was the highest (3.93, standard deviation [SD] 0.62), followed by the likelihood of recommending the service to family or friends (3.88, SD 0.79). Satisfaction with personalized messages that increased patient understanding was rated at 3.82 (SD 0.70). The internal consistency among the survey items, indicated by the Cronbach's alpha coefficient, was 0.836, suggesting that the survey items were appropriate for analyzing user satisfaction with the service.
Satisfaction survey.

Survey items were rated on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Values are expressed as mean ± SD.
SD: standard deviation.
Focus group interview
To further assess the platform's impact on clinical decision-making and workflow integration, a focus group interview was conducted with participating medical providers. The interview findings (Table 4) highlight the platform's overall usability, benefits, and challenges in real-world clinical settings. Medical providers reported that the user dashboard allowed for quick and convenient access to patient data, enhancing the efficiency of consultations. The ability to compare current and past health metrics, such as blood pressure and blood glucose levels, was particularly valuable for identifying trends and adjusting treatment plans. Additionally, the transition from manual record-keeping to a digital platform improved patient monitoring, allowing for more precise medication adjustments based on real-time data.
Focus group interview of medical providers.

The Automated Logic System received positive feedback, with providers highlighting its role in assisting with patient-specific decision-making and optimizing treatment plans based on key clinical parameters. They noted that the system helped streamline intervention strategies by automatically prioritizing critical health indicators and guiding timely clinical actions. This feature was seen as particularly useful in reducing the cognitive workload for healthcare providers while maintaining high-quality, individualized care.
Physicians also noted that intervention messages were effective in engaging patients, but suggested refining their content to emphasize key points for improved clarity. Despite these benefits, certain challenges were identified, including the need for better integration with Electronic Medical Records (EMR), improvements in user interface design for easier navigation, and optimized intervention messaging strategies. These insights provide valuable qualitative evidence supporting the platform's feasibility while also guiding future refinements to enhance usability and scalability in diverse clinical settings.
Establishing strategies to enhance patient engagement
Face-to-face education was conducted for older adults with low levels of digital literacy. Correct methods for measuring blood pressure/blood glucose, understanding health information using ICT, how to use the app, and customized education for specific diseases were provided. In addition, a user-friendly and intuitive user interface/user experience (UI/UX) was developed to ensure that the app is easy to use, even for older people.
However, for ICT-based healthcare programs, app adherence is an important management indicator of program performance. To encourage continuous participation, care coordinators made weekly phone calls to those with insufficient self-recording to encourage their participation. Material and financial incentives were also introduced to enhance engagement. Participants in the intervention group were provided with disease-specific self-monitoring devices, such as blood pressure monitors and glucometers, and incentives were offered based on the level of improvement in their management and adherence. Upon completing the entire process, including post-test and survey, both groups received thank-you gifts as an additional motivation. Control group participants were also compensated for providing personal information and completing blood tests and surveys. Moreover, maintaining a high retention rate for mobile apps is crucial for enhancing patients’ self-care capabilities. The South Korean government is also discussing additional measures to reduce out-of-pocket medical expenses for patients with well-controlled hypertension and diabetes. Furthermore, in anticipation of a decrease in compliance after 12 weeks, which was the midpoint of the program, face-to-face education sessions were conducted to foster sustained engagement. The 24-week feasibility test showed that the average number of daily active users (DAU) was 77.5%, surpassing the average 90-day retention rate of 31-36% and the annual retention rate 18% among healthcare apps.23,24
Discussion
In this study, an ICT-based digital platform for patients with hypertension and diabetes was developed. Through the platform, medical professionals can receive help with patient-tailored management, and patients can enhance their self-care abilities. Furthermore, as a platform that enables bidirectional communication between patients and physicians, customized interventions can be performed based on the patient's condition, and patients can receive assistance in establishing positive lifestyle habits for the treatment and prevention of diseases. In particular, through a 24-week feasibility test, a significant improvement in the key clinical indicators of hypertension and diabetes was confirmed.
Digital health, which employs digital technology for health purposes, is increasingly utilized in the management of NCDs. 25 This signifies health support using ICT. 25 Digital management of diabetes or hypertension involves the utilization of technology to enhance care and self-management. This technology, particularly diabetes apps, offers healthcare practitioners the opportunity to monitor patients’ glycemic data more closely, thereby improving the quality of care and health outcomes. The HERB-DH1 pivotal trial investigated the impact of a digital therapeutic system on essential hypertension management and it demonstrated promising results. 17 Moreover, a randomized, open-label, multicenter pilot study utilizing a smartphone application for hypertension management underscored the potential of digital therapeutics in facilitating ambulatory and home blood pressure monitoring and encouraging lifestyle modifications among patients. 26
However, despite these advancements, sustaining patient engagement and achieving meaningful health improvements remain challenging without a human touch. Previous research, including a consensus report by the European Association for the Study of Diabetes and the American Diabetes Association, has emphasized the critical role of medical professionals in integrating digital health technologies into chronic disease management. 27 Furthermore, studies have shown that incorporating human coaching into digital health programs significantly enhances adherence and treatment effectiveness. Personalized counseling, ongoing support, and tailored interventions improve patient engagement and long-term disease management. Nonetheless, human interaction requires substantial financial and human resources, posing scalability challenges. Recognizing this, our study sought to optimize the balance between digital automation and human intervention by developing an automated logic system that supports personalized patient management while reducing the burden on healthcare providers. Specifically, our system provided automated alerts and interventions for patients with low app engagement or inadequate self-reported health data, thereby enhancing adherence with minimal direct human input. Additionally, at the 12-week mark of the 24-week intervention, face-to-face counseling was incorporated strategically to reinforce personalized care plans, ensuring that patients received necessary guidance without excessive resource consumption.
As a result, our study achieved a 77.5% retention rate, significantly exceeding global benchmarks for health-related apps (90-day retention: 31 to 36%, annual retention: lower than 18%).23,24 This suggests that a hybrid approach—combining digital automation with targeted human touchpoints—can enhance long-term engagement and improve health outcomes efficiently. By leveraging automation to streamline human interaction where possible, digital health interventions can become more sustainable and scalable in real-world healthcare settings.
This study focuses on digital health interventions in primary healthcare. We demonstrated that digital health interventions for diabetes and hypertension offer significant promise in improving primary healthcare outcomes. Recent studies have identified critical barriers and challenges in managing chronic diseases in primary care settings, emphasizing the lack of human and technical resources. 28 These interventions encompass a wide range of technologies, including mobile phone health apps, telehealth services, and sensor-enabled devices for continuous physiological monitoring. These tools aim to enhance the self-management of chronic conditions, enable real-time monitoring, and support clinical decision-making. The use of digital medicine for continuous home patient care has contributed to improved health outcomes. This is exemplified by the case of a patient with diabetes who participated in this study. An 82-year-old male with uncontrolled diabetes experienced severe fluctuations in his blood glucose level with repeated occurrences of postprandial hyperglycemia and hypoglycemia. Moreover, while living alone, there was concerned about his ability to manage emergencies arising from blood glucose crises. Despite fear of diminished literacy due to his age, the patient was able to learn correct insulin use and diabetes management through regular phone calls from a care coordinator and continuous education on app usage. The success of the 82-year-old patient aligns with findings from relative studies demonstrating the effectiveness of mobile health diabetes self-management programs for patients with uncontrolled diabetes, improving HbA1C levels and self-management behaviors through app-based education and personalized support.29–31 Additionally, through the developed platform, the physician could monitor the patient's medication and blood glucose history and send customized messages for medication adjustment. From the third week of participation, fluctuations in the patient's blood glucose improved to a target range of 80–130 mg/dl. Furthermore, by the end of the 24-week intervention, there were no additional hyperglycemia or hypoglycemia events. Additionally, there was an improvement in the HbA1c level from 7.1% at the start of participation to 6.5% at the end, indicating a 0.6% improvement.
The engagement strategies described in this study—including mobile-based monitoring, automated reminders, and digital education content—offer high scalability due to their technological adaptability, automation potential, and low marginal cost.32,33 These digital interventions can be readily integrated into existing healthcare infrastructures, particularly in primary care settings, via cloud-based platforms and interoperability with electronic health records (EHRs). 34 In addition, national public health initiatives, such as government-funded incentives for patients achieving chronic disease control, create a favorable policy environment that promotes widespread adoption. 35 These strategies require minimal additional training for healthcare providers, which supports their feasibility in resource-limited environments and ensures operational sustainability at scale. 36 Ultimately, leveraging such scalable engagement models is critical for achieving long-term patient adherence and improving chronic disease outcomes at a population level. 37
A significant strength of this study is the large scale, with 1004 participants in a case-control design, and the lengthy 24-week intervention during which digital medicine was integrated into primary care to examine improvements in health outcomes. Digital medicine was designed not only for the convenience of patients but also to enhance the clinical efficiency of medical professionals, facilitating two-way communication between patients and health professionals. This study has several limitations. First, the lack of randomization may introduce selection bias, potentially affecting the generalizability of the findings. Future research should incorporate randomized controlled trials (RCTs) to more rigorously assess the platform's effectiveness and reduce confounding factors. Second, while the study briefly acknowledges the challenges faced by older adults, it did not specifically evaluate the impact of digital literacy on platform engagement and clinical outcomes. As individual literacy data were not collected in a way that allows correlation with platform usage, direct analysis of this relationship was not feasible in the present study. However, given that digital literacy can significantly influence usability and adherence, future studies should explore how literacy barriers affect intervention effectiveness and assess strategies to improve accessibility and engagement among older populations. Third, as survey responses were collected anonymously, it was not possible to correlate satisfaction levels with adherence or clinical improvement at the individual level. Future research could utilize non-anonymous longitudinal tracking to explore this relationship in greater detail. Fourth, the study did not include an economic evaluation of platform implementation and human resource utilization. As the Korean government is planning to provide reimbursements for primary care clinics adopting digital platforms for chronic disease management, future studies should assess long-term cost-effectiveness and financial feasibility. Despite these limitations, the study provides valuable insights into the feasibility of digital health interventions in chronic disease management and lays the foundation for further research into optimizing digital health adoption in real-world healthcare settings. In conclusion, this study demonstrated that the adoption of digital medicine is both effective and essential for continuous patient management in primary care. ICT-based tools and applications are increasingly important in healthcare, and our findings provide valuable insights into chronic disease management. As the next step, a randomized controlled trial is needed to rigorously assess the platform's clinical effectiveness. Additionally, further research should focus on optimizing automation logic, integrating with hospital information systems (HIS), and evaluating its long-term utility in real-world settings. Ultimately, these efforts will lay the foundation for advancing this system into a validated digital therapeutics solution for chronic disease management.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251344375 - Supplemental material for A comprehensive digital medicine platform for hypertension and diabetes care in primary care: A real-world feasibility test
Supplemental material, sj-docx-1-dhj-10.1177_20552076251344375 for A comprehensive digital medicine platform for hypertension and diabetes care in primary care: A real-world feasibility test by Ye Seul Bae, Seoyeon Park, Changbo Noh, Boram Choi, Seung Ah Yi and So Eun Kim, Yoon Ji Kim, Jae-Heon Kang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251344375 - Supplemental material for A comprehensive digital medicine platform for hypertension and diabetes care in primary care: A real-world feasibility test
Supplemental material, sj-docx-2-dhj-10.1177_20552076251344375 for A comprehensive digital medicine platform for hypertension and diabetes care in primary care: A real-world feasibility test by Ye Seul Bae, Seoyeon Park, Changbo Noh, Boram Choi, Seung Ah Yi and So Eun Kim, Yoon Ji Kim, Jae-Heon Kang in DIGITAL HEALTH
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board (IRB) of Kangbuk Samsung Hospital (IRB number: KBSMC 2020-07-026-012).
Author contributions
JK had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: YSB, JK. Acquisition of data: YSB and SP, BC, CN. Analysis and interpretation of data: YSB, SEK, and SAY. Drafting of the manuscript: YSB, JK. Critical revision of the manuscript: YSB, YJK. Statistical analysis: YSB, SEK, SAY, YJK. Administrative, technical, or material support: YSB, SP, BC, JK.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Promotion R&D Project, funded by Ministry of Health & Welfare, Republic of Korea (grant number: HS20C0041) and the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: 1711196171IRIS, RS-2023-00255145).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The clinical data used in this study cannot be shared due to institutional policy.
Guarantor
YS Bae, J Kang
Informed Consent
We explained the research to and obtained informed consent from patients who agreed to participate in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.