
Abstract
Background
Social capital refers to the valuable resources that individuals can access through their social networks, which are often established within family ties, professional affiliations, community organizations, and neighborhoods. Evidence suggests that there is a positive association between social capital and well-being, health status, and sociability. Research has found a positive association between digital technology use and social capital, though limited attention has been paid to older adults. This systematic review aims to evaluate the association between digital technology use and social capital among older adults.
Methods
Five scientific electronic databases were searched for eligible studies in October 2024. The search strategies were developed by combining the keywords of the three main axes of the research (“older adults,” “digital technology,” and “social capital”) and respective synonyms using Boolean operators. The review protocol was developed in advance and registered in PROSPERO (CRD42024614622).
Results
The research strategy returned a total of 1229 citations from electronic databases, 20 of which met the exclusion and inclusion criteria. All the included studies had a cross-sectional design, and the samples of the included studies ranged from 118 to 9642 individuals. All the included studies found a positive association between digital technology and social capital among older adults.
Conclusions
Digital technology can offer opportunities to maintain or increase social capital, that typically tends to reduce with age. Since social capital positively impacts health and well-being, the importance of enabling older adults to use digital technologies must be considered when designing and implementing health behavior intervention programs.
Introduction
Social capital is defined as a general public resource that usually exists within connections formed through family ties, work environments, community organizations, and local neighborhoods.1–3 This concept refers to the various concrete (i.e., money, food, and running errands) and abstract resources (i.e., offering emotional support, giving advice, sharing nuanced information, and making recommendations) that can be accessed through interpersonal relationships. 4 According to Bourdieu and Coleman, social capital is not an active form of resource; instead, it exists in a dormant state that can be activated in response to particular needs.2,3 Thus, social capital is regarded as the collection of resources found in one's social ties, their accessibility, and the capability to make use of those resources. 5
Two distinct frameworks for categorizing social capital have been recognized. The first model makes a distinction between bonding social capital, which gives emotional support through deep connections, and bridging social capital, which relies on weaker ties that assist in gaining knowledge and new perspectives.6,7 The second approach categorizes social capital into two main components: cognitive and structural. The cognitive component pertains to individuals’ emotional experiences, including trust, reciprocity, a sense of belonging, and personal motivations such as attitudes, sharing, and values, which can be understood as how people view their social relationships. Conversely, the structural component relates to the precedents, regulations, and behavioral norms that emerge from social engagement, along with the roles and networks created through social interactions.6–8
Essentially, social capital encompasses the resources that individuals gain through their social connections, which can be interpreted as the degree of their social integration and the support they obtain from their community. 9 A person's social capital is fundamentally rooted in the connections and relationships that form their social networks. Individuals who possess robust and interconnected social networks find it simpler to obtain information and enjoy greater resources, as their network members offer both bridging and bonding support, enhancing their confidence and trust levels.10,11
Research indicates that social capital is linked to enhanced quality of life and well-being, as well as beneficial factors such as positive emotions, optimism, life satisfaction, trust, and hope, while showing a negative correlation with feelings of loneliness.12–20
Previous research has tried to assess whether the increasingly massive use of Information and Communication Technologies (ICTs) could have an impact on individuals’ social capital. Initial investigations suggested that online connections were insufficient,21,22 but with the increasing use of ICTs, particularly through social media platforms, there is now substantial evidence demonstrating how these technologies can aid in acquiring bridging and bonding social capital.4,23–26
Although previous research has found a positive association between digital technology use and social capital, limited attention has been paid to older adults. 27 With the rise of digital technology as a key means of accessing information, engaging in communication, and participating in society within developed nations, it is essential to examine its impact on social resources through an age-related lens. While the adoption of digital technology among older individuals is on the rise, they remain less inclined to utilize it compared to younger. 27 With the global rise in the number of older individuals projected to continue in the coming decades, promoting healthy aging has become crucial. 28 The growing concerns of social exclusion, isolation, and loneliness are increasingly impacting the health, well-being, and social engagement of older individuals. 27 Evidence suggests that senior citizens with elevated social capital levels are likely to be in better health, practice healthier habits, and experience superior physical and social wellness, even if they live alone or have a low income.29,30 Due to various factors, social capital is crucial for promoting healthy aging, however, its presence tends to diminish as individuals grow older. 27 This decline is often linked to life events that frequently involve loss, such as reduced work opportunities, declining physical abilities, and the death of loved ones, all of which can adversely affect one's social capital.31,32
If digital technology use proves to be positively associated with social capital also in older age, the improvement of digital literacy and a greater use of digital technologies among older individuals might help them maintain high levels of social capital also in the later stages of life. This systematic review aims to evaluate the association between digital technology use and social capital among older adults.
Methods
A systematic review was conducted. The review methods were defined in advance in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines 33 and PRISMA checklist (Appendix A). The review protocol was registered with International Prospective Register of Systematic Reviews (PROSPERO – CRD42024614622).
Search strategy
For the present study, PubMed, PsycINFO, CINAHL, Scopus, and Web of Science databases were systematically searched in October 2024. Search strategies were developed by combining the keywords of the three main axes of the research (“older adults,” “digital technology,” “social capital”) and respective synonyms using Boolean operators. For the PubMed database, a combination of Medical Subject Headings (MeSH) terms and text-words was used. The Medical Subject Headings (MeSH) thesaurus is a controlled and hierarchically organized vocabulary produced by the National Library of Medicine and used for indexing, cataloging, and searching biomedical and health-related information. 34 The combination of text-word and MeSH strategies is recommended to achieve the most comprehensive results. 35 The search strategies are provided in Appendix B.
Retrieved studies were independently reviewed for eligibility by two authors (GG and AB) in a two-step process: an initial screening was performed based on titles and abstracts, and then full texts were screened. Disagreements between the two reviewers were resolved by consensus. The reference lists of the included studies were also searched to identify additional relevant studies.
Inclusion and exclusion criteria
The review questions were predefined in advance using the PICO (Population, Intervention, Comparison, Outcome) framework. 36 The population group was identified in (a) older adults defined as individuals aged 60 years or more or (b) study's samples with the participants’ mean age of 65 years or above; the exposure was related to the use of digital technology including social network sites, apps, smartphones, and the Internet; the comparison was identified in older adults not using digital technology; and the main outcome was the assessment of the measure of the association between the exposure to digital technology and social capital.
Studies were considered for inclusion in the systematic review if they:
assessed the measure of the association between digital technology use and social capital among older adults; included individuals who were 60 years old and older or samples with a mean age of the participant over 65; were published from 2000 onwards; were written in English.
Studies were excluded from the systematic review if they:
targeted exclusively older adults affected by a specific disease or clinical condition; incorporated theoretical studies or published opinions as their primary source of evidence.
Data extraction and data analysis
A data extraction form based on the research question was developed in Microsoft Excel. The following data were extracted from the included studies: (a) main author, (b) year, (c) objectives, (d) study design, (e) country, (f) characteristics of the population, (g) variables of interest, (h) data sources, (i) methods and statistical analyses, (j) controls and confounders, (k) outcomes, and (l) conclusions. A descriptive analysis was performed to report the characteristics of the included reviews (Table 1) and their outcomes (Table 2).
Association between digital technology use and social capital.

Characteristics and findings of the primary level studies.
Association between digital technology use and others health outcomes: social capital as a mediating variable. Characteristics and findings of the primary level studies.

Quality assessment of the included studies
The RoBANS 2 tool 37 was used for a critical assessment of the methodological quality of the included studies (Appendix C).
Result
Identified studies
The initial search yielded a total of 1229 citations from electronic databases. After removal of duplicates, 932 titles and abstracts were screened, and 49 full texts were assessed for eligibility. Among them, 29 papers were excluded for the following reasons: 13 studies were not conducted in older adults as defined in the inclusion criteria; nine studies did not evaluate the social capital of the older adults; six studies did not assess the association between digital technology use and social capital; one study was written in a language other than English. Ultimately, 20 studies met the inclusion criteria and were included in the systematic review. No additional studies were included based on the manual search of the reference lists. The literature search is shown in detail in Figure 1.
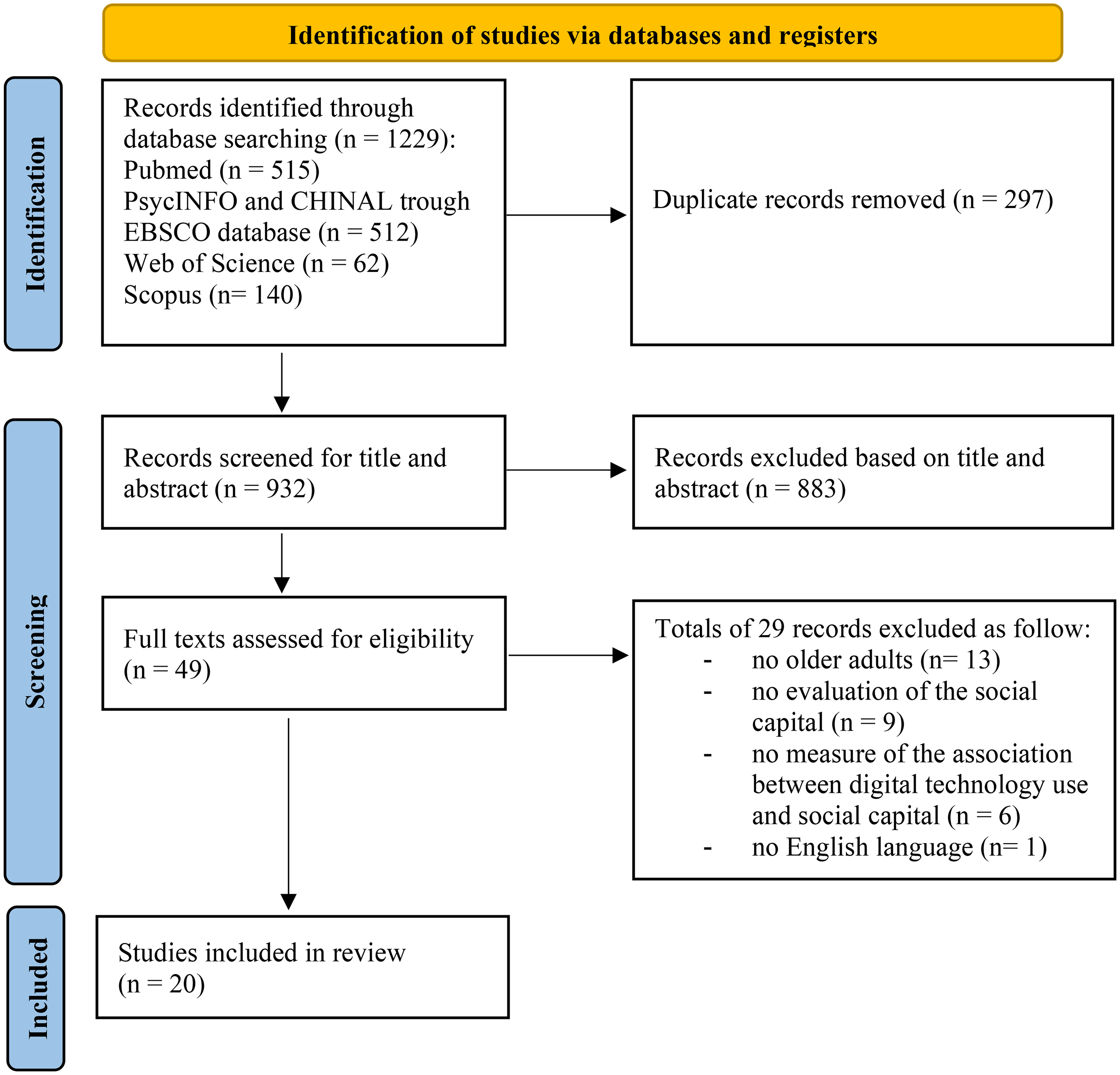
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram of the article search.
Characteristics of and findings of the included studies
All the included studies had a cross-sectional design. The studies’ samples ranged from 118 to 9642 individuals. Most of the studies (n = 12) were conducted in China,8,38–48 three were based in the United States,9,49,50 three in Europe,27,32,51 one in Canada, 52 and one in Taiwan. 53
The included studies were divided into two main categories according to the way that the two main variables considered in this systematic review, digital technology use and social capital, were treated in the analyses: 12 studies evaluated the association between digital technology use and social capital,8,9,27,32,38–40,49–53 and 8 studies evaluated the association between digital technology use and various health outcomes analyzing the mediating role that social capital played in this association (social capital as a mediator).41–48
The included studies utilized different variables as a measure of exposure to digital technology: most of them (n = 11) evaluated Internet use of the older adults;9,27,38,42,43,45–50 three assessed older adults’ eHealth literacy,8,40,44 two studies evaluated the participants Social Network Sites use,32,52 one studied the cell phone exposure, 39 one study considered the level of digitalization of the living area, 41 one evaluated the digital lifestyle, 51 and one the participants’ perceptions regarding the use of a telehealth system. 53 Regarding the second variable of interest, 10 studies assessed social capital globally,8,9,40–42,44,45,47,51,53 five studies evaluated bonding and bridging social capital separately,27,43,49,50,52 two studies focused on structural and cognitive social capital,39,46 one bonding social capital, 32 one structural social capital, 48 and one digital social capital. 38
All the included studies found a positive association between digital technology use and social capital among older adults, regardless of the type of digital technology used or subcategory of social capital considered.
Methodological quality of the included studies
The results of the methodological quality assessment are reported in Appendix C. The majority of the studies were evaluated at low risk of bias in the following domains of the RoBANS 2 tool: 37 “comparability of the target group,” “target group selection,” “confounders,” “blinding of assessors,” “incomplete outcome data,” and “selective outcome reporting.”
On the other hand, the included studies met one or more of the following RoBANS 2's criteria for “high” risk of bias for inappropriate “measurement of intervention/exposure”: 1) exposures were measured by simply self-response; 2) exposures were measured by unstructured interviews, and 3) measurements were not objectified or standardized properly by utilizing multiple measurements (two times or more), independent measurements by multiple investigators, or using a standardized measurement of exposure, even with no effort to do so. 37 This could lead to performance bias due to inappropriate exposure measurement. Also, most of the included studies were judged at high risk of bias for outcome assessment because they met the following criteria for “high” risk of bias: patient-reported outcome that was assessed using only simple self-response: 37 this could lead to detection bias due to inappropriate outcome assessment methods.
Discussion
The included studies consistently showed that the use of digital technologies was associated with higher levels of different types of social capital among older adults.
This result suggests that digital technology use, and Internet use in particular, among older adults can contribute to a greater social capital.8,54 Engaging socially online could actually enhance bonding social capital, as it provides greater chances to interact with loved ones, 55 while also fostering bridging social capital through the wealth of information and services accessible on the Internet.9,56
An earlier investigation involving a digital sample of older Australians found that engaging in online communication enhanced their satisfaction with family interactions, facilitated the expansion of their close social circles, and resulted in more face-to-face meetings. 57 Similarly, interviews conducted with senior users of a social media site showed that they primarily utilized it to keep track of their loved ones’ activities instead of for deep interactions. 27 This insight would, however, stimulate direct communication or phone calls, indicating that the social media platform might be facilitating the maintenance and activation of social capital through this awareness. 27 Also, studies show that digital media can enhance social engagement for those with limited mobility,58–60 a common issue for older adults, and can assist in accessing or preserving social relationships.61,62
O’Brien and colleagues 52 examined how various features of social networking sites influence interpersonal connections, discovering that the nature of exchanged message, whether they are personal or informational, varies in their effects on social ties. The research indicated that personal messages foster stronger ties in intimate relationships, whereas informational exchanges bolster more tenuous social links. 52 In this sense, social network sites can help to strengthen the bonding and bridging of social capital of their participants. Moreover, utilizing social media actively, along with the variety and number of connections, contributes positively to social ties, yet a higher level of engagement with these platforms does not appear to affect social relationships, implying that the frequency and length of use do not enhance the social capital of older adults. 52
Considering that all the included studies had a cross-sectional design, a bidirectional association might also be at play, implying that older adults with high levels of social capital might be more likely to use digital technologies. In this context, since a person's social connections form the essential foundation of their social capital, individuals with robust and interconnected social circles (such as family, friends, and volunteer companions) are more inclined to receive support in learning to navigate digital technologies, along with both emotional and practical help from their network members. 9 Engaging in activities with relatives, companions, and other connections is expected to enhance the demand for and perceived value of digital tools as a way to sustain social bonds and integration. 9 Supporting this hypothesis, previous research revealed that the primary ways individuals engage with digital technology include observing and discussing computer and Internet usage with their children and grandchildren, as well as receiving informal assistance from relatives and friends on navigating these technologies. 57
In addition, since digital literacy frequently correlates with socioeconomic factors such as educational attainment and income levels,49,63 implications for studies on digital inequality emerged.9,27,49 The research conducted by Barbosa-Neves and colleagues supported earlier findings that indicated a positive association between social capital and Internet use, while also showing an inverse association with age. 27 At the same time, the Internet appears to mitigate the adverse effects of age on social capital, as older individuals who frequently use the Internet are more likely to possess high social capital compared to their non-using or infrequent-using counterparts. 27 Therefore, the Internet appears to have a buffering effect that mitigates the negative association between age and social capital; however, older individuals are still less inclined to embrace the Internet compared to younger demographics, with education being a primary factor influencing Internet usage among seniors. 64 Consequently, it is primarily individuals with advanced education who would gain from that protective element. Likewise, the research by Choi and DiNitto supports these conclusions, indicating that older adults who are both older and from lower socioeconomic backgrounds are much less prone to use the Internet, including for health-related inquiries. 9
The findings suggest that although digital technology appears to support the preservation, accumulation, and activation of social capital via its social features, it simultaneously exacerbates certain social disparities, especially related to age and educational background.9,27 Specifically, engaging in social activities on the Internet can intensify the disparities between those with greater privilege and those with less, particularly in terms of the social capital they can acquire. Studies on digital disparity indicated that individuals are more likely to experience beneficial results from Internet usage when they have the necessary skills to effectively utilize it. 65 To fully harness the advantages of online social interactions for building social capital, individuals must have enough digital literacy to effectively utilize the Internet for fostering and sustaining social connections. 66 Supporting older individuals, particularly the most disadvantaged ones, in their use of digital technology to satisfy social demands might mitigate this disparity. 49 Knowledgeable family members and friends can offer support for older adults in using the Internet for social interactions, complemented by organized initiatives such as computer workshops that have yielded encouraging results.67–69
Finally, the landscape of security and privacy risks has evolved as fast as digital technologies, creating an urgent need to protect digital devices from key threats through a layered security approach. 70 Privacy and security concerns can adversely affect the adoption and use of digital technology, and older adults are particularly vulnerable compared to the rest of the population, mainly due to lower digital literacy or cognitive impairment. Strict regulation together with consistent social support for older adults should improve the use of and trust in digital technology while ensuring privacy and security.
Strengths and limitations
This systematic review has some limitations. First, all the included studies had a cross-sectional design; thus, only associations, not causal relationships could be deduced. Secondly, the variables of interest were measured with different scales and instruments across the studies; although, the consistency of the results through all the twenty publications supports the results and the conclusions of this review. Thirdly, limiting the language of publications to English only may have led to a linguistic bias and lack of data on specific cultural contexts that might have different results. Lastly, due to the great heterogeneity of the studies and the lack of standardized measurements, it was not possible to carry out a subgroup analysis concerning the characteristics of the population (age class of the participants, living environment), the type of digital media used and the characteristics of the use (duration, intensity, type of information shared, extent of contacts), as was planned in the study protocol.
Conclusions
Overall, this systematic review indicates that digital technology could play a crucial role in enhancing social connections for older adults, facilitating the renewal, maintenance, and creation of relationships while fostering social capital.
The results highlight some implications for future research and for the development of digital technology training for older adults. Specifically, when providing computer and Internet education for seniors, it is essential to acknowledge the important influence that social support systems have on the learning experiences of older individuals as they engage with digital technology. Children, relatives, and companions can serve as valuable sources of guidance and inspiration when navigating the digital landscape.
Furthermore, training in digital technology for seniors should prioritize specific groups, including older individuals, racial and ethnic minorities, those with limited education and financial resources, individuals who are unmarried and live alone, as well as those experiencing low social integration and support, to effectively bridge the digital gap. Seniors possessing these traits may gain the greatest advantages from the resources available through Internet technology.
Footnotes
Acknowledgements
The authors acknowledge funding from Next Generation EU, in the context of the National Recovery and Resilience Plan, Investment PE8 – Project Age-It: “Ageing Well in an Ageing Society” [DM 1557 11.10.2022]. The views and opinions expressed are only those of the authors and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
Author contributions
Alessandra Buja: Conceptualization, Validation, Writing – Review & Editing, Visualization, Supervision, Project Administration, Funding Acquisition; Giulia Grotto: Methodology, Software, Formal Analysis, Investigation, Resources, Data curation, Writing – Original Draft; Visualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was developed within the project funded by Next Generation EU - “Age-It - Ageing well in an ageing society” project (PE0000015), National Recovery and Resilience Plan (NRRP) - PE8 - Mission 4, C2, Intervention 1.3.” The views and opinions expressed are only those of the authors and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them. Next Generation EU - “Age-It - Ageing well in an ageing society” project (PE0000015), National Recovery and Resilience Plan (NRRP) - PE8 - Mission 4, C2, Intervention 1.3.”
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Appendix A. PRISMA 2020 Checklist.

| Section and Topic | Item # | Checklist item | Location where item is reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 5, 6 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 6 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 7, 8 |
| Information sources | 6 | Specify all databases, registers, websites, organizations, reference lists, and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 7 |
| Search strategy | 7 | Present the full search strategies for all databases, registers, and websites, including any filters and limits used. | Page 27–29 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 7, 8 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Page 8 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Page 8 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 8 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Page 8, 10, 30 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | Not applicable |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Page 8 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | Not applicable | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Page 8 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Page 8 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | Not applicable | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | Not applicable | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 8, 30 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Not applicable |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 9, 16 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Page 16 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Pages 9, 10 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Pages 10 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Not applicable |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Pages 10, 30 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Pages 10 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Not applicable | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Not applicable | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Not applicable |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Not applicable |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Pages 11–13 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 12, 13 | |
| 23c | Discuss any limitations of the review processes used. | Page 12, 13 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 13, 14 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Page 7 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Page 7 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Not applicable | |
| Support | 25 | Describe sources of financial or nonfinancial support for the review, and the role of the funders or sponsors in the review. | Page 15 |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 15 |
| Availability Of Data, Code And Other Materials | 27 | Report Which Of The Following Are Publicly Available And Where They Can Be Found: Template Data Collection Forms; Data Extracted From Included Studies; Data Used For All Analyses; Analytic Code; Any Other Materials Used In The Review. | Page 15 |
Appendix B. Research search strings
Appendix C. Quality assessment of the included studies according to the RoBANS 2 tool. 37

| Main author, year | RoBANS 2 domanis | |||||||
|---|---|---|---|---|---|---|---|---|
| Comparability of the target group | Target group selection | Confounders | Measurement of intervention/ exposure | Blinding of assessors | Outcome assessment | Incomplete outcome data | Selective outcome reporting | |
| Barbosa Neves, 2018 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Cai, 2024 | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk | Low risk |
| Cao, 2023 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Choi, 2013 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Cui, 2021 | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk | Low risk |
| Cui, 2024 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Duan, 2024 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Geithner, 2022 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Guan, 2024 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Jiang, 2022 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Jing, 2023 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Li, 2021 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Lyu, 2020 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Nguyen, 2022 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| O'Brien, 2021 | Low risk | Low risk | High risk | High risk | Low risk | High risk | Low risk | Low risk |
| Rios, 2019 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Simons, 2023 | Low risk | Low risk | Low risk | High risk | Low risk | Low risk | Low risk | Low risk |
| Tsai, 2014 | Low risk | Low risk | High risk | High risk | Low risk | High risk | Low risk | Low risk |
| Yang, 2022 | Low risk | Low risk | Low risk | High risk | Low risk | High risk | Low risk | Low risk |
| Zhu, 2021 | Low Risk | Low Risk | Low Risk | High Risk | Low Risk | High Risk | Low Risk | Low Risk |