
Abstract
Objective
The Spanish national health system (SNHS) faces significant barriers to psychological care, such as long waiting lists and a lack of human resources. In addition, with emotional disorders being the most prevalent disorders worldwide, and less than half of those affected receiving proper treatment, there is an urgent need for new treatment alternatives for this group of disorders. The Unified Protocol (UP) is presented as a possible solution that has amply demonstrated its efficacy in different formats and contexts. Another promising alternative involves the use of blended formats, combining face-to-face UP sessions with a UP-based application. This manuscript focuses on the description of RegulEm, a UP-based application developed following a participatory design approach. In addition, a case example of receiving UP in a blended format in a specialized mental health unit of the SNHS is presented.
Methods
The following components of RegulEm are described: content and exercises of the modules; aesthetics and multimedia-based content; intervention delivery; testimonials section; emotional and motivation assessment; exposure hierarchy for guided in vivo and imaginal exposure; emergency button and Gamification. A case example of a 26-year-old male patient with anxiety and depressive symptoms receiving UP in a blended format in a specialized mental health unit of the SNHS is presented.
Results
The user showed improvements in emotional regulation skills, anxiety, and depressive symptoms over time, though stressors remained. RegulEm allowed independent progress between face-to-face UP sessions, but low internalization of some content emphasized the importance of therapist guidance in face-to-face sessions. User feedback highlighted satisfaction with the intervention but improvement proposals for RegulEm were identified, such as simplifying emotional exposure exercises.
Conclusion
This manuscript describes in detail the first UP-based smartphone application's components and illustrates important implications, such as enabling users to progress at their own pace between sessions and advancing more quickly in the intervention.
Keywords
Introduction
The Spanish National Health System (SNHS), established in 1986, provides free, quality public health services, including mental health care. 1 Several limitations that hinder attention to mental health problems in the SNHS have been described: (1) lack of human resources, 5.58 psychologists per 100,000 inhabitants compared to the minimum of 12 that it is recommended 2 ; (2) long waiting lists of 4 months in specialized care 3 ; (3) care overload, with 330 users per professional per year compared to the 86 users per year that it is recommended 3 ; (4) short appointment times, of 35 minutes in specialized care 4 ; (5) saturation of services; and (6) difficulty in the application of evidence-based treatments. 1 A similar reality is also found in other countries. In this regard, it is known that barriers to access to psychological care are a major problem of health systems in low- and middle-income countries, 5 as well as in middle- and high-income countries. 6
In addition, anxiety, depressive, and related disorders, also known as emotional disorders (EDs), 7 are the most prevalent mental disorders worldwide, with prevalence data of 31% for anxiety disorders and 28.9% for depressive disorders. 8 In addition, the WHO estimates that by 2030 EDs will be the leading cause of disability 9 an estimated scenario that is even worse considering the high comorbidity rates between different EDs. 10 Focusing on data from Spain, we find prevalence data of 2.4 million people (5.42%) regarding anxiety disorders and 2.6 million people (6.04%) for mood disorders. 11 Despite the high prevalence and burden of EDs, it is known that only 23% of people with a depressive disorder diagnosis receive proper treatment 8 and approximately 28–36% in the case of anxiety disorders. 12 These data, added to the barriers faced by mental health care from the SNHS mentioned above, highlight the need to focus on new treatment alternatives for this group of disorders.
Psychological interventions based on a transdiagnostic approach may be considered as an option that could help to face the barriers to the treatment of EDs. These interventions focus on common mechanisms underlying a wide range of disorders, 13 which enables the design of treatments for a broader group of disorders rather than for specific ones, allowing the treatment of people with comorbidity. 14 Different interventions following this approach have been proposed, as is the case of the Unified Protocol for the Transdiagnostic Treatment of EDs (UP), a Cognitive Behavioral Therapy (CBT) based intervention. 15 The UP is a modular and protocolized intervention, which makes it more flexible and able to be adapted to different formats and problems.16,17
In terms of the efficacy of the UP, six systematic reviews have been published so far, five of them meta-analyses18–23. These studies have demonstrated its utility, with effects that are statistically superior to waiting list conditions and between equivalent or slightly superior to those obtained by disorder-specific CBT.21,22 In addition, these results have been reported to be comparable across different application formats (individual, group, and online). 22 In Spain, the UP has proven its efficacy in group format in the SNHS with larger effect sizes compared to treatment as usual at 15 months after onset of treatment, as well as showing fewer dropouts and higher satisfaction with treatment. 24
In addition to transdiagnostic-based interventions, smartphone applications for psychological care are also presented as a promising solution to address the barriers to the treatment of EDs. 25 These applications provide advantages such as being easily accessible, anonymous, more cost-effective, and easily customized and tailored to individual needs. 26 However, focusing on efficacy data for these applications, findings are still inconclusive. 27 Systematic reviews and meta-analyses that support their evidence for the improvement of EDs can be found.28,29 But, at the same time, it has been reported that their use as standalone interventions cannot be recommended at this stage and further study on the possibility of integrating them into clinical settings which is known as blended format is encouraged. 30 In a blended format, applications and face-to-face (f2f) sessions are combined. 31 In this way, the blended format offers different advantages such as saving time for clinicians, allowing users to review treatment content as many times on demand, 32 transferring the content of f2f sessions into daily life, 33 and reducing dropouts. 31 In addition, a recent systematic review on applications for the treatment of emotional dysregulation in blended format reported that the integration of these applications as an adjunct to treatment appeared to prolong the duration of improvement over time and can be highly beneficial in enhancing treatment engagement. 34 In terms of its efficacy, emerging evidence suggests that the blended format might be comparable to f2f treatments for anxiety symptoms 35 and major depression. 36 According to the previously cited systematic review conducted by Diano et al., studies analyzing applications that are used as part of psychological treatment in a blended format are still in their infancy. Regarding available applications of this type, 19 applications for the treatment of emotional dysregulation were identified in this review. Most were primarily aimed at the treatment of EDs, but some were also found focused on the treatment of borderline personality disorder. In turn, all of them were based on theoretical frameworks belonging to CBT or derived from it. 34 Finally, those applications available and designed for the treatment of EDs were Pacifica, 37 ACT Daily, 38 and MindClimb, 39 which include mood tracking, mindfulness exercises, and CBT-based skills practice. Finally, alongside these are also available Behavioral Apptivation, 40 MoodKit, 41 and Ascend, 42 which focus on behavioral activation and cognitive restructuring to improve emotional regulation.
In view of the aforementioned, a transdiagnostic intervention as the UP applied in a blended format could be a promising option to improve the status of ED treatment in the SNHS, in an integrated way combining f2f UP sessions with an UP-based application. Accordingly, our team is conducting a randomized controlled trial aiming to compare the efficacy and cost-effectiveness of the UP in blended format versus treatment as usual, unstructured CBT in f2f individual format, for the treatment of EDs in different mental health units of the SNHS. 43 For this purpose, an UP-based application named RegulEm, was developed.44,45 In this manuscript, the characteristics of RegulEm are described through a case example of receiving psychological treatment within the randomized controlled trial in a specialized mental health unit of the SNHS.
Method
Characteristics of the study
As aforementioned, a randomized controlled trial is being carried out with the aim of comparing the effectiveness and cost-effectiveness of UP in a blended format for the treatment of EDs versus treatment as usual. The study started in January 2023 and is carried out in eight different mental health units of the SNHS, with the approval of all the corresponding ethics committees. In addition, this study was registered with ClinicalTrials.gov (NCT04304911). The inclusion criteria for the study were as follows: (1) age 18 or older, (2) primary diagnosis of ED, (3) fluency in Spanish, (4) Android operating system 8 or higher smartphone ownership and proficiency in its use, (5) patients taking pharmacological treatment for their ED will be asked to maintain the same dosages and medications for at least 3 months prior to enrolling in the study and during the whole treatment, and (6) signature of the informed consent form. On the other hand, the exclusion criteria were the following: (1) to present a severe condition warranting prioritized treatment (e.g., bipolar disorder, personality disorder, schizophrenia, or organic mental disorder), suicide risk at the time of assessment or substance use in the last 3 months and (2) to have previously received eight or more sessions of psychological treatment with clear and identifiable CBT principles within the past 5 years. 43 Thus, in each of the eight specialized mental health units collaborating in the study, participants who meet the inclusion criteria are invited to sign an informed consent form and undergo baseline assessments and then randomly assigned to either the UP condition in a blended format (individual f2f UP sessions + RegulEm) or the treatment as usual condition (unstructured CBT in f2f individual format).
RegulEm design and development
RegulEm was designed and developed in a two-stage participatory process with the involvement of an Information Technology engineer team and a psychology research group specialized in the UP intervention. This methodology implies that end users take an active role in all phases of the application design process, 46 which could facilitate the application's adaptation to the needs of future users and thus improve application adherence. 47 The first stage of the participatory process resulted in a preliminary version of the application, through a qualitative study involving users and professionals familiar with the UP as they have previously collaborated in a multicenter randomized clinical trial developed across different specialized mental health units of the SNHS. The aim of this study was to identify the needs, opinions, expectations, and design aspects of these users and professionals regarding an UP-based application, to be considered in its development. In this study, two focus groups, lasting 2 hours each, were carried out. From the information gathered in both focus groups, a total of 61 proposals were collected, of which 89% were finally incorporated in a preliminary version of RegulEm. 44 As for the second stage, this consisted of analyzing the perceived usability and quality of the preliminary version of RegulEm, to ensure that it was adequately designed and oriented to the needs of end users before proceeding to assess its effectiveness. For this purpose, a parallel mixed methods study was conducted with the same users and professionals who were previously involved in the first stage of the participatory process. Thus, participants completed MARS,48,49 uMARS,50,51 and SUS52,53 scales, and two focus groups were carried out. Results form this second stage study show that users rated RegulEm's usability as good (75 points) and professionals rated it as excellent (84.64 points) based on SUS scale scores. Regarding quality, it was rated as good by both groups using the uMARS and MARS scales, scoring 4 and 4.14 out of 5, respectively. In addition, various aspects of RegulEm's usability and areas for improvement were identified from the information gathered in the focus groups, with 20% of the suggested changes incorporated into the updated version of the application. 45 To date, RegulEm has been developed for use on Android Operating System devices and its Intellectual property rights registration number is n.º 00765-02388060. The following components and characteristics of RegulEm are described in more detail below: content and exercises of the modules; aesthetics and multimedia-based content; intervention delivery; testimonials section; emotional and motivation assessment; exposure hierarchy for guided in vivo and imaginal exposure; emergency button; gamification.
Content and exercises of the modules
RegulEm is based on the UP-patient manual. 54 The UP is a transdiagnostic CBT based intervention aimed at training in adaptive emotional regulation skills. It is composed of eight modules, five of which are considered core (from 3 to 7), as they target a specific emotional regulation skill: (1) setting goals and maintaining motivation; (2) understanding your emotions; (3) mindful emotion awareness; (4) cognitive flexibility; (5) countering emotional behaviors; (6) understanding and confronting physical sensations; (7) emotion exposures, and (8) recognizing accomplishments and looking to your future. 54 Thus, the content of the intervention in RegulEm is also presented in a modular manner and each application module faithfully reproduces the content of the same module in the UP manual. An overview of the content and exercises in each RegulEm module can be found in Table 1.
RegulEm contents and exercises.

This technique is not included in the original UP manual for adults.
Each module comprises the following structure: content presentation, comprehension evaluation of the content, exercises, and conclusion. A screen view of these different application components can be found in Supplemental Material. The main concepts of the 8 modules are explained through video. Comprehension of the content is assessed by means of true/false questions, with feedback and explanations provided for each answer. As it is presented in Table 1, users have different exercises available in each module to put into practice the content and skills learned. These exercises are in an instant message format, requiring at least two completions each. Users must complete all main exercises in a module before proceeding to the next. After completing a module, users can review the content and access additional practice exercises. Finally, the conclusion section offers reinforcement and a summary of the module's content.
Aesthetics and multimedia-based content
RegulEm is composed of three main screens which can be seen in Figure 1: Treatment, Your progress, and Tutorials.
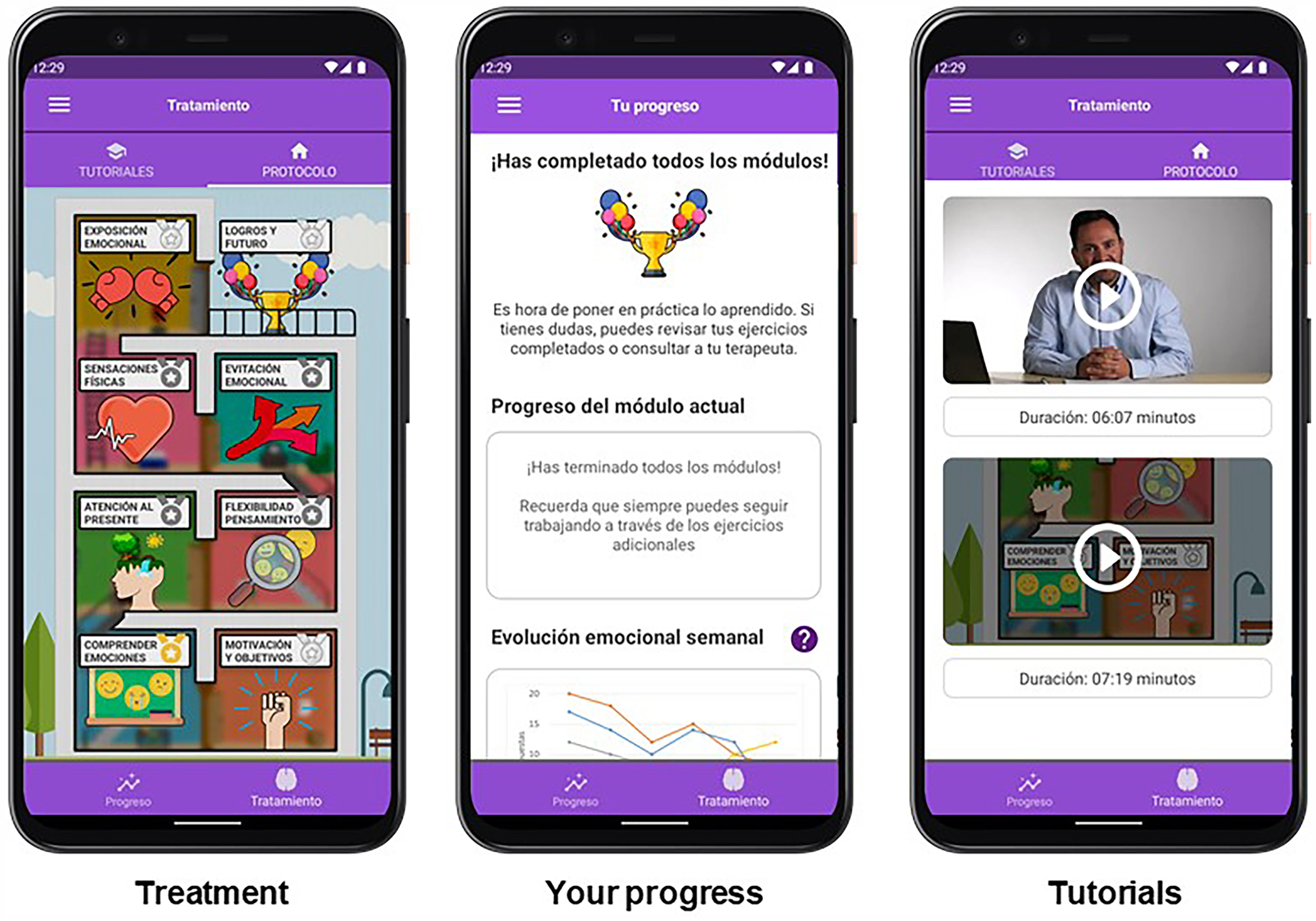
Regulem's main screens.
In the “Treatment” screen, following the design adopted in the UP-patient manual, 54 the content of the eight modules in RegulEm is depicted as a house, with each module representing a room in the UP-house. This design encourages users to think of building a healthier, more adaptive relationship with their emotions. Following the metaphor of the UP-house, with each module a new emotional regulation skill is acquired and practiced, which contributes to build the entire UP-house of emotional regulation. Therefore, each module or room remains unlocked until the previous one is completed. As can be seen in Figure 1, each room in the UP-house is assigned an image that illustrates the content of the represented module.
The other RegulEm main screen is called “Your progress,” and it provides information to users about the module they are currently in, as well as where they are in the module. In addition, on this screen, users have available a graphic of the evolution of their emotional state week by week (for more information, see the Emotional and motivation assessment section). Finally, users can access the third screen called “Tutorials,” where two videos are always available for viewing: one introducing RegulEm (welcome and intervention rationale) and the other showing how to use the application throughout the intervention.
In relation to the video-based content, different types of videos are included in the application. First, the content videos that appear in the presentation of the content section of each module. These videos introduce the main concepts of each module. On the other hand, the videos that appear in the tutorial section are starring members of the research group that developed RegulEm. One of the videos introduces the intervention, while the other shows different screens of the Application while explaining how it works and how to use it throughout the intervention. The module 6 exercise of confronting physical sensations uses also videos, which show how to carry out different interoceptive exposure exercises. Finally, the meditation exercise of module 3 is worked through guided meditation audios.
Intervention delivery
RegulEm was designed to be used in combination with f2f UP sessions, i.e., as part of a blended format intervention. In f2f sessions, the clinicians follow the second edition of the UP-therapist manual. 15 The first intervention session takes place f2f and, prior to its end, users are instructed by their therapist to download RegulEm on their smartphones. F2f sessions take place with the frequency established by the mental health unit. Therefore, RegulEm allows users to advance in the intervention on their own during the interval between f2f sessions. In this way, in the f2f sessions, the therapist continues applying the intervention from the module where the users are in the application, as well as reviewing what has been worked on the user's own in the previous weeks. Except for modules 1 and 7, which therapists are instructed to introduce in a f2f session before users start working on them through the application, users can start the rest of the modules on their own. Once patients complete all RegulEm modules for the first time, they can continue to carry out emotional exposures and work on the emotional regulation skills presented in each module using the application through the additional exercises available between f2f sessions.
Finally, as a measure to try to engage users in treatment, notifications are sent as a reminder to log into the application after 5 days without logging into. Moreover, a RegulEm web platform was also developed and connected to the application. Through the web platform, therapists have access to the information recorded by their users in the different modules as well as to the application usage data and emotional and motivational weekly progress. Thus, therapists can use this information to adapt the f2f sessions according to the information that the users have registered on the application.
Testimonials section
The testimonials section includes the cases of six different individuals presenting an ED (Depressive disorder, Illness anxiety disorder and Panic disorder, Social anxiety disorder, Obsessive-compulsive disorder, Posttraumatic Stress Disorder, and Bipolar disorder). In this way, for each of the application's exercises, users can visualize how each of these six people has completed the exercises. This section has been included to help users be identified with one or more testimonials and to help them when completing the exercises. A view of the testimonials section can be found in Supplemental material.
Emotional and motivation assessment
Users assess their emotional state (frequency and intensity of symptoms) each week through five items with a 5-point Likert-type response scale (0 = I did not feel “assessed emotion” during the last week / Nothing / None - 4= Constant / Extreme / All the time). Overall anxiety (OASIS) 55 and depression (ODSIS) 56 severity and impairment scales in its Spanish versions 57 were adapted, simplifying the response options to each item (e.g., “Constant anxiety. I felt anxious all the time and never got to relax” was reduced to “Constant anxiety”). In the first login to the application, users choose the emotion(s) they want to be assessed for frequency and intensity (anxiety, depression, positive emotions, other emotions [guilt, anger, shame]). Users can modify throughout the intervention the emotions they wish to be recorded, allowing them to add new emotions and to stop recording others. A graphic showing the weekly fluctuation of emotional symptomatology is available to users so that they can visualize progress throughout the intervention.
In turn, the application assesses weekly at the user's choice, the motivation with the intervention through the question “During the last week, how motivated have you been to continue working on your emotional improvement?.” Users respond through a 10-point Likert-type scale (0 = Very low to 10 = Very high). On the one hand, a response between 0 and 5 is considered as low motivation, opening a box in the application in which users can read information about the naturalness of the ambivalence of the motivation to change and recommending them to review the goals established and the decisional balance elaborated in module 1. On the other hand, a response between 6 and 10 is considered as high motivation, and the box that opens automatically in the application contains reinforcement information to the users for their high motivation with the intervention. It also warns that fluctuation in motivation is a natural part of the change process and can occur throughout the intervention. In such cases, it is recommended to review the goals and decisional balance.
Exposure hierarchy for guided in vivo and imaginal exposure
Module 7 of RegulEm involves guided exposure to intense emotions, both in imagination and in real-life scenarios. For this purpose, users create a personalized exposure hierarchy through two initial exercises. In the first exercise, users select an intense emotion and identify triggering situations, people, objects, places, thoughts, memories, images, and physical sensations. They rate discomfort and avoidance levels for each item on a scale from 0 to 10, organizing the hierarchy from least to most distressing. The second exercise prompts users to consider additional elements (e.g., time of day, location type, number of people) that could affect discomfort and avoidance levels in their hierarchy. This exercise allows for adjustments and additions to the exposure plan. Once completed, users finalize their hierarchy and proceed to the third exercise, which initiates emotional exposure. In the third exercise, the exposure hierarchy is divided into three sections: available exposures, future exposures, and completed exposures. Therefore, users can start exposing gradually to the recorded situations, beginning with the available exposure, which are those evaluated with a lower level of avoidance and discomfort.
Prior to each exposure, RegulEm prepares users by assessing discomfort and avoidance levels for the upcoming situation. It anticipates negative automatic thoughts and emotional behaviors that may arise and prompts users to generate alternative thoughts and behaviors. After each exposure, the application guides users through a post-exposure record. The application asks users about the emotions felt and their components (thoughts, physical sensations, behaviors), and the users evaluate how effectively the emotional regulation skills learned in previous modules were applied during the exposure. Users also rate their level of avoidance and tolerance towards the experienced emotion. A situation in the hierarchy is considered complete when the user has engaged in two consecutive occasions where discomfort and avoidance levels were rated at 3 or lower. A view of the Exposure hierarchy and the preparation before the exposure can be seen in Supplemental material.
Emergency button
Users have access to an “Emergency Button” in case of crisis. In this section, suicidal ideation and suicidal risk are assessed. The frequency of thoughts about suicide in the last week is assessed with a 6-choice response scale ranging from “Not at all. I have not had thoughts of suicide” to “All the time. Almost most of the time I have had thoughts of suicide.” Depending on the severity, the emergency button redirects the user to one of two options: On the one hand, in case of severe suicidal behavior (the user answers that thoughts about suicide were frequent or all the time), the user is redirected automatically to call the Suicide Hotline in Spain. On the other hand, if the risk is not high (the user answers that he/she has not had any thoughts about suicide or that these were frequent or occasional), the user is advised to contact his or her referral therapist and to immediately call the Suicide Hotline in Spain if his/her status worsens. A view of the Emergency button section can be seen in Supplemental material.
Gamification
RegulEm includes a gamification element, within the comprehension evaluation of the content section of each module. This gamification element consists of assigning a different medal depending on the number of correct and incorrect answers to the true/false questions. Thus, users can receive a gold, silver, or bronze medal in each module, which is reflected in the image of the UP house.
Results
The RegulEm version resulting from the two stages that made up its participatory design and development process is being used in combination with individual sessions of the UP, i.e., in a blended format. The following results will present the case of a user who is receiving UP in a blended format in a specialized mental health unit of the SNHS within the ongoing randomized controlled trial mentioned in the method section. The study is being conducted with the approval of Euskadi's Medicine Research Ethics Committee (PI2021101) and adhered to the principles described in the Declaration of Helsinki.
History
A man of 26 years old, came to specialized care referred by his primary care doctor, reporting anxious and depressive symptomatology. As a result of an accident at work for which the company assumed no responsibility, he was currently on medical leave and was taking legal action against the company. This situation, in addition to the physical and psychological sequelae of the work accident, fear, and uncertainty about his future employment and family conflicts, explained the anxious and depressive symptomatology.
The user reported the following symptoms: baseline anxiety, ruminations and intolerance to uncertainty, apathy and anhedonia with mood fluctuation, fragmented sleep, and loss of appetite. Obsessive personality traits were noted, but not reaching the threshold required for a personality disorder. He stated having occasional intrusive memories or images of the work accident, but that they do not interfere with his daily life. The user denied having any thoughts of suicide or suicidal ideation. No alterations of course, form or content of thought, nor sensory-perceptual alterations were observed. Consciousness and orientation were preserved. He mentioned that he tried to remain active, but he did not manage to do so daily. At the same time, he avoided spaces where he could run into colleagues from the company. The user mentioned that all these symptoms greatly limited his life, since they accentuated avoidance behaviors, made it difficult for him to concentrate on occupational and relaxing activities and he did not feel capable of seeking a new job. At the time of his visit, he was already taking pharmacological treatment prescribed by his primary care doctor: Duloxetine 60 MG, Pregabalin, Sedotime 45 MG, and Lorazepam 1MG. After a first information gathering and evaluation session, he received a diagnosis of mild single depressive episode with moderate anxious distress (296.21; F32.0) and it was determined that he met the criteria to be included and benefit from the study. Therefore, he was included in the study after signing the informed consent and randomly assigned to the experimental condition UP in a blended format.
Course of treatment
The first intervention session took place f2f. In this session, the intervention was introduced and the first UP module, on motivation to change and goal setting, was worked on. Two of the goals that he established, along with smaller ones for its achievement, were: “Be more self-confident- (1) To trust the people who advise me, (2) Not to be thinking all day long” and “Improve the emotional atmosphere of the family: (1) Do not mistrust a family member that I consider key to my support; (2) Do not be so resentful; (3) Know how to forgive”. At the end of the session, the user downloaded RegulEm with the guidance of his therapist. The therapist gave the user instructions to start working with RegulEm until the next f2f session. In this sense, users can progress through RegulEm at their own pace. However, the therapist recommended him to complete one module per week.
Following the therapist's indications, the user logged into the application for the first time and began to work on module 1. Thus, the user was able to review what had been seen in the f2f session and record the treatment goals and the decisional balance through the exercises in the application. Figure 2 shows the temporal evolution of the user throughout the intervention, and the combination of the use and work through the application together with the f2f sessions. As can be seen in Figure 2, the user progressed faster and soon reached module 4.

Descriptive data of the UP blended treatment progress by the user.
The second f2f session, held one month after the initial one, focused on reviewing modules the user had recently engaged with through the application. Therefore, the psychoeducational content of module 2 and the ARC analysis were reviewed, as well as the training in attention focused on the present. Although the user demonstrated engagement with the intervention and use of the application, there was little internalization of the content of modules 2 and 3. This was possibly attributed to inconsistent practice and difficulty in applying the content in daily life, coupled with a desire for rapid improvement.
As a result, the f2f session was dedicated only to the review of the contents of modules 2 and 3, and module 4 was not introduced. The therapist indicated to the user to continue working on module 4 through the application and to complete its exercises. Additionally, the session identified that the prolonged involvement in the legal process was contributing to obsessive rumination.
As can be observed in Figure 2, between the third and fourth f2f sessions, the user completed modules 4 and 5 and reached module 6 in the application. In the third f2f session, despite the user having already completed modules 4 and 5 in the application, it was observed that he had not yet internalized the practice of the skills of cognitive flexibility (module 4) and attention focused on the present (module 3). Thus, his difficulty in distancing himself from internal worries and ruminations and generating alternative thoughts was more evident. Therefore, the therapist recommended him to repeat the exercises in these modules during the following weeks to put into practice the emotion regulation skills worked so far and to be constant in practice. He was in module 6 in the application but had not yet worked through the content of the module and carried out any exposure to physical sensations. Therefore, he also was instructed to work on the content of module 6 in the application in the following weeks. On the other hand, the user remained very motivated with the intervention and the work through RegulEm and he was satisfied with this type of blended format, although seemed in a rush to reach his treatment goals.
In the fourth f2f session, the user reported a slight improvement in mood, mentioning efforts to enhance relationships with family members and explore new activities for entertainment. The user found cognitive flexibility and increased acceptance of his circumstances helpful in better managing his situation. Regarding RegulEm, the user had completed module 6 and was currently in module 7, which he perceived as challenging and demotivating, especially concerning exposure situations, which he felt that he would not be able to cope with. For this reason, the session focused on reviewing treatment goals, exploring reasons for change through decisional balance exercises, and reinforcing emotional regulation skills learned in previous modules. The session also involved working on module 7's content and creating an emotional exposure hierarchy. Exposure scenarios included looking at or approaching the work area, visiting bar areas, walking in home spaces without avoiding coinciding with family members, and going to the boardwalk.
During the month between the fourth and fifth f2f sessions, the user recorded the situations in the exposure hierarchy from module 7 exercises and began to carry out the first exposures. In the fifth f2f session, greater emotional tolerance and improved acceptance and attitude toward his emotions were observed. However, the user expressed demotivation and found the functioning of module 7's exposure hierarchy complex. Although some exposures were initiated, the user found the application exercises challenging and repetitive. The therapist encouraged him to continue to be exposed to recorded situations and reviewed content from previous modules. By the following week, the user had completed one situation in his exposure hierarchy, allowing progression to module 8 in RegulEm. Module 8 focuses on relapse prevention exercises, including anticipating future challenges and setting new goals.
In the application, he was instructed to keep accessing module 7 to continue exposing himself to the rest of the situations recorded in his exposure hierarchy. At this point, the second part of the intervention is reached in which, once the user has completed all the modules of the application and, therefore, worked on all the emotional regulation skills included in the UP, he can continue to access all the RegulEm modules, carry out the additional exercises available and continue with the emotional exposures through the application between f2f sessions with his therapist.
Assessment of progress and satisfaction with RegulEm and the blended format after completing all RegulEm modules
Regarding the treatment goals that the user established in module 1, it is important to mention that the increased awareness of the factors that influence his emotional state led the user to reformulate some of these goals throughout the weeks of intervention. Four months after starting the intervention, and after having completed the eight RegulEm modules, he had already achieved some of the treatment goals. In this sense, the patient succeeded in achieving the goals of “Trusting the people who advise me,” “Not being so resentful,” and “Taking distance from some relatives,” while the following are still in progress: “Managing rumination,” “Accessing a job,” and “Adapting to the functional limitation that hinders my work.” On the other hand, regarding the situations included in the exposure hierarchy created in the application, the patient has managed to complete two of them, while he continues to be exposed to the other remaining two situations in the hierarchy. Those he has completed are going to the boardwalk and looking at or approaching the work area. Concerning these situations, although he continues to experience some anxiety, tolerance to the emotion and non-avoidance have improved.
In turn, at that time point, the user did not meet the criteria for the established baseline diagnosis of a mild single depressive episode. Apathy and degree of enjoyment improved, although his functionality and activation continued to be conditioned by anxiety. Regarding the anxious symptomatology, this persists and continues to fluctuate due to the interaction of two factors: On the one hand, the persistence of stressors, since the legal process has not yet been resolved, he cannot access another job until the legal process is over and he has not received the desired support from some family members with whom he must continue cohabiting. On the other hand, the user presents high trait anxiety, and despite not reaching the threshold for a personality disorder, presents obsessive personality traits that explain the persistence of rumination and high reactivity to stressors. Nevertheless, the user presents a greater awareness of these traits which allows him to activate emotional regulation skills earlier and better tolerate anxiety symptoms and to avoid emotions and situations less.
In addition, the user completed the Multidimensional Emotional Disorders Inventory (MEDI)58,59 at baseline before the start of the intervention and four months later, after completing all RegulEm modules. Figure 3 shows the scores obtained in each of the transdiagnostic dimensions assessed by the MEDI at the two evaluation moments.
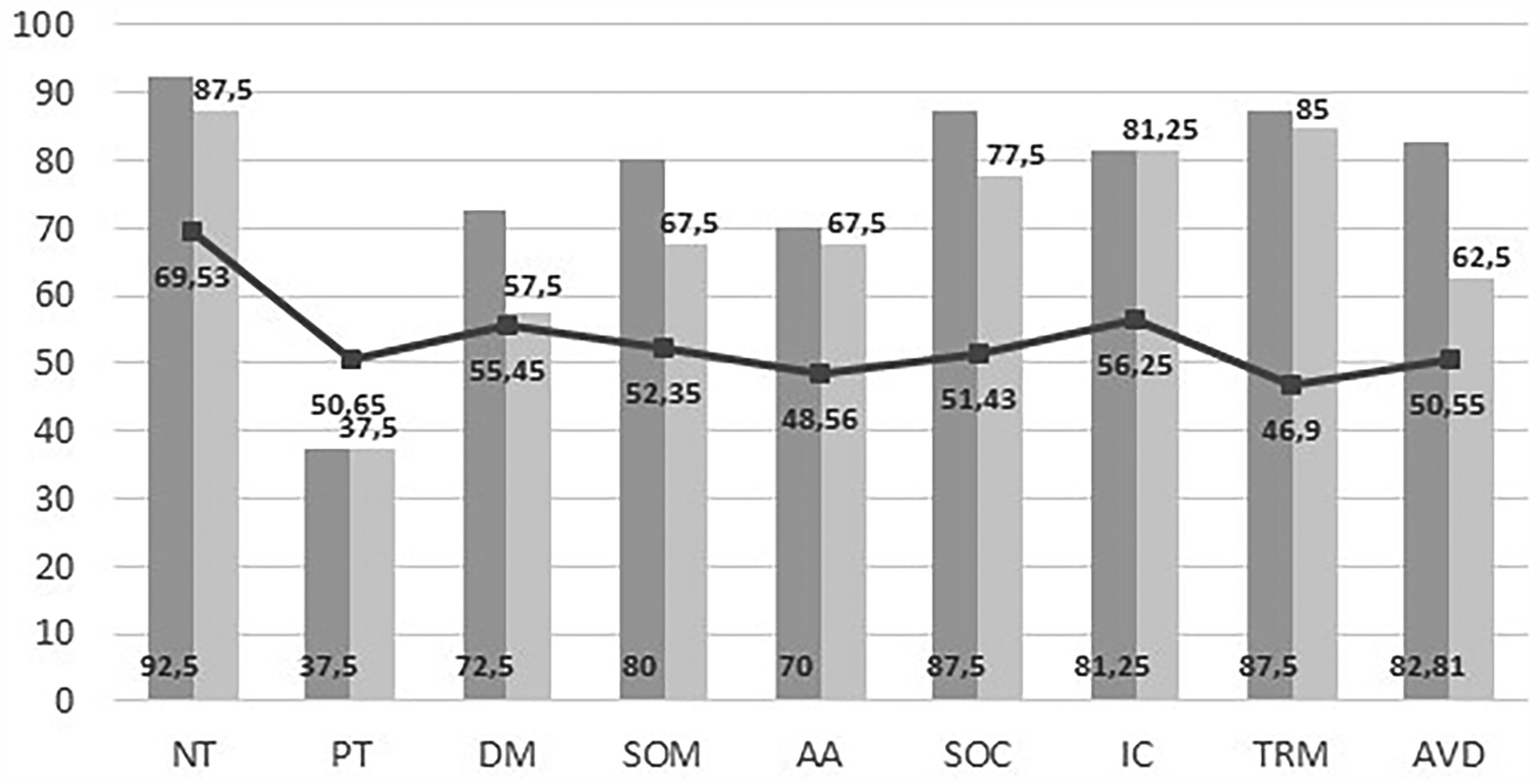
Profile obtained through the MEDI for the user and cut-off points in clinical population. 45
As can be seen in Figure 3, the scores in PT and IC remained constant at 4 months, while for the rest of the dimensions, there was a decrease in the scores, which was more pronounced in the AVD, DM, and SOC dimensions.
On the other hand, regarding the weekly emotional assessment through the application, the user initially chose to record the emotions of anxiety and shame. While, from the fifth week onwards, the user also chose to record sadness. As can be seen in Figure 4, anxiety and depression scores decreased from baseline to assessment time 4 months later. Although fluctuating and interspersed with peaks of higher scores, there was a trend toward improvement in both scores over the weeks. However, both scores have not decreased below the clinical cutoff point of 10 in ODSIS and OASIS, 57 being higher than it for anxiety, and right at the clinical cutoff point for depression. Regarding shame, a tendency to decrease the frequency and intensity with which the user experienced this emotion over the weeks can also be observed in Figure 4. In addition, regarding the motivation assessment, the user recorded several times his motivation with the treatment with a score of 8 out of 10.

Emotional assessment through the app and OASIS and ODSIS scores at baseline and 4 months after treatment onset.
Furthermore, the user was asked about his satisfaction with the intervention, through an adaptation of the Client Satisfaction Questionnaire (CSQ-8). 60 In this adaptation, 6 of the 8 items of the CSQ-8 (perceived quality, adequacy to previous expectations, recommendation of the treatment, usefulness of the skills learned, overall satisfaction with the intervention, and probability that they would choose this type of intervention again) and one item related to the distress generated by the intervention were included, with an 11-point Likert scale ranging from 0 (nothing or bad) to 10 (very much or excellent). The user valued positively the intervention based on the UP applied in a blended format, with an arithmetic mean of scores of 6.86. For more information, Table 2 shows the direct scores for each of the items in the satisfaction questionnaire.
Direct scores to each of the CSQ-8 items by the user.

Regarding satisfaction with the UP more specifically, the user answered an ad hoc questionnaire composed of seven questions; one that assesses the utility of the intervention to improve emotional regulation and six specific questions that evaluate the usefulness of each of the emotion regulation skills that are included in the modules of the UP. In this regard, the user rated with 7 points out of 10 the extent to which he believes the program has helped him to adequately regulate his emotions. In addition, the emotional regulation skill that he valued as the most useful was cognitive flexibility, with 7 points out of 10, followed by the rest of the emotional regulation skills (Analysis of the emotional experience [ARC], focus on the present, countering emotional behaviors, tolerance to physical sensations and tolerance to intense emotions) which he rated with 6 points out of 10.
Finally, after completing all the RegulEm modules, the user was also asked about his satisfaction and opinion of the application and the blended format through an ad hoc questionnaire, including questions with a Likert response scale and open-ended questions. In this sense, the user evaluated RegulEm as a moderately entertaining application (6/10 points) and as having provided somewhat valuable information (6/10 points). At the same time, the application's components (videos, audios, true/false questions, testimonials section, emergency button, and weekly emotional and motivation record) were rated as moderately useful (6/10 points), highlighting the videos and the weekly emotional and motivation record above the rest (7/10 points). On the other hand, in relation to the blended format, despite expressing satisfaction with the UP in blended format and indicating that he would recommend it, he indicated that he would choose a fully f2f format, with individual sessions with his therapist, if he had to receive the same intervention again.
In relation to the open-ended questions, the user mentioned that he was satisfied with the application and highlighted that the videos and their content are very well explained. However, he also emphasized that the exercises were repetitive and monotonous, causing him discomfort at having to complete each one at least twice to move on to the next one, given that they involve working on painful aspects and events. At the same time, he highlights as a barrier the complexity of the exercises in module 7, making it difficult for him to understand how the hierarchy of emotional exposure works. Therefore, he suggests as proposals for improvement that there should be greater variability in the exercises and that the exercises in module 7 should be simpler and easier to understand.
Discussion
The purpose of this manuscript was to introduce RegulEm and describe its characteristics and components, as well as to illustrate its use as part of the UP applied in blended format through the case of a user who attended a specialized mental health unit of the SNHS. Some strengths of the application can be highlighted from the information presented in this manuscript about its characteristics and the treatment course of the case example reported. RegulEm is the first smartphone application developed based on the UP and has been designed and developed following a participatory design approach, which could help to prevent future problems associated with its use that may emerge in clinical practice. 61 In turn, the content of RegulEm reproduces the content outlined in the UP patient manual, 54 therefore, the different CBT-based techniques gathered in the UP can be worked through the application. In addition, the problem-solving technique, also CBT-based and which is not included in the original version of the UP manual for adults, has been added to be worked on through the application's exercises. In this regard, it is noteworthy that RegulEm contemplates this technique, as well as that of exposure to physical sensations and intense emotions, as the literature considers these CBT techniques as the most difficult to implement in mental health applications as opposed to other CBT techniques such as cognitive restructuring or behavioral activation. 62 Especially the exposure technique, which according to the review by Denecke et al. 62 whose aim was to identify the CBT techniques that have been implemented in existing mental health applications, had not been represented in any application of these characteristics so far.
In relation to the case of the user reported, it is observed that receiving the intervention in this blended format allows the user to advance in the treatment between sessions, as well as to continue practicing and reviewing throughout the treatment of those modules completed previously. However, a low internalization by the user of the contents worked on through RegulEm was observed as the intervention progressed, which underlines the importance of the f2f sessions with the therapist, which can detect this low internalization and review the skills worked on in the application. This is important since evidence supports that change over the course of the intervention in improving the skills targeted by the UP is a predictor of improvement in anxiety symptoms. 63 In addition, improvements or maintenance are observed in all MEDI dimensions after completing all the UP modules included in RegulEm, especially in AVD, DM, and SOC. However, no improvements in scores below the clinical cut-off point are observed. In turn, although a trend towards improvement is observed, there is also no improvement in scores below the clinical cut-off point in anxious and depressive symptomatology over the weeks and up to the assessment 4 months after starting treatment, as well as for the emotion of shame. This may be due to the fact that, although a greater emotional tolerance and a better acceptance and attitude towards emotions were observed in the user, the stressors have not changed or disappeared over the weeks. In this sense, the legal process in which the user is immersed is still active and he also does not have the support from his family that he would desire. Therefore, the presence of these stress factors could lead to the maintenance of anxious and depressive symptomatology above the clinical cut-off point. Furthermore, even if the user has completed all the RegulEm modules, this does not mean that the intervention is finished, but rather that he must continue to put into practice the emotional regulation skills that have been worked on. In this sense, from this point on, the therapist can space out the sessions while the patient continues to practice with the application in order to see if the practice of the skills helps him to improve his tolerance to intense emotions and to achieve his goals. In relation to this, at the moment after completion of all RegulEm modules, the user has achieved three of the treatment objectives set, while three others are still in progress. The same applies to the exposure situations, of which he has completed two and still has two remaining situations to which he must continue exposing himself.
Moreover, in relation to user satisfaction with the intervention, in the direct responses to each item of the CSQ-8, it is observed that the user positively valued the quality and usefulness of the UP in a blended format and would recommend the intervention to others. At the same time, it is observed that the discomfort experienced by the user in the intervention was considerable, which could be explained by the fact that throughout the UP the users must invest effort and confront their intense emotions by responding differently to them 54 and also because the user reported complexity of the exposure exercises in module 7 in the application. In this regard, future updates of RegulEm could include a new functionality of monitoring the degree of discomfort that the user experiences while performing the exercises of the different application modules, in order to be able to, in case of discomfort, immediately intervene by suggesting the practice of one or more of the emotional regulation skills previously practiced in a face-to-face session with the therapist or through the application. This update corresponds to what is known in the mhealth field as Ecological momentary interventions (EMIs) and Ecological momentary assessment (EMA). In this manner, we would incorporate an EMA and, depending on the degree of discomfort experienced by the users, an EMI that would prompt them to engage in a specific skill, offering a range of skills to choose from. 64
On the other hand, although the user indicated that the UP in blended format had helped him to regulate his emotions in a more adequate way and valued the application and its components well, he indicated that he would choose a completely f2f and individual format if he had to receive the intervention again. This is supported by previous data indicating that the format of preference for users with an ED attended in public mental health units in the SNHS is individual format (85.4%), compared to group (14.2%) or online (0.4%). 65 In addition, this information stands with the idea that blended formats using applications could be better accepted and lead to greater engagement if the main format of the intervention is the f2f sessions and the application is a complement. 34
Finally, some obstacles related to RegulEm were identified, which affected the motivation and the progression of the intervention by the user, mainly related to module 7 in the application. Thus, from this information are derived the improvement proposals to increase the variability of the exercises and to simplify the exercises of module 7, to improve and simplify the way in which the hierarchy of exposures is presented, and the exposures are carried out. All these improvement proposals will be considered in future updates of RegulEm. This is in line with previous studies suggesting that before such an application can be considered satisfactory it may require several moments of evaluation and refinement in collaboration with end users. 66
In addition to these proposals for improvement, other proposals for future studies on the update of RegulEm could include the option for users to choose the UP module to work on, instead of a set sequence, or adding a support call by the therapist between f2f sessions, which has been suggested as a way to help maintain application usage. 67 Furthermore, another future proposal that has proven to be potentially beneficial could be to include a community support option through which to share with other users of the application recent circumstances and concerns and receive peer support and advice. 68 In addition, future research should analyze the utility of RegulEm as part of the UP in a blended format in other countries, since barriers similar to those present in the SNHS that hinder access to treatment of EDs are also common in a wide variety of countries. 5
Finally, it is necessary to mention some limitations of RegulEm, as well as of the present study. Regarding the limitations of the application, RegulEm is currently only available for Android systems. This decision was made because Android is the most widely used mobile operating system worldwide, 72.15% market share compared to 27.19% for iOS. 69 In turn, the problems detected and suggestions for improvement of the application are not being continuously fixed and updated, this is mainly due to the lack of budget. However, the suggestions for improvement identified will be considered in future updates of RegulEm. In this regard, in addition to the randomized controlled trial in specialized mental health units of the SNHS referred to in the present manuscript, RegulEm is being and will be used in other studies carried out with different populations and contexts such as, for example, university students attended by the university's psychological assistance services. In this manner, the application will continue to be tested and, in addition, thanks to the funding of future studies, will be updated and thus incorporate the suggestions for improvement that have already been identified as well as those that may arise in the future. Regarding the limitations of the study, since it describes the application, as well as its implementation as part of the UP in BF, the results cannot be generalized. On the other hand, another limitation to mention is that no information was collected about the participant's previous experience with the use of technology and/or applications of this type, considering that previous experience could have affected the results and comfort when using the application.
Conclusions
Despite the obstacles encountered during the intervention of the reported user case from which proposals for improvement are derived, the present study presents important implications. RegulEm is the first UP-based application to be developed and this study describes in detail its components and characteristics. In addition, as illustrated in the case example described the combination of f2f UP sessions with an application such as RegulEm allows the user the possibility to advance at his own pace between sessions and progress more quickly in the intervention.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251334442 - Supplemental material for RegulEm, a smartphone app based on the unified protocol for the transdiagnostic treatment of emotional disorders: description of its application in blended format in a clinical case
Supplemental material, sj-docx-1-dhj-10.1177_20552076251334442 for RegulEm, a smartphone app based on the unified protocol for the transdiagnostic treatment of emotional disorders: description of its application in blended format in a clinical case by Laura Martínez-García, Jon Belaunzaran Mendizabal, María Asunción Santos Goñi, Ignacio Miralles and Jorge Osma in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251334442 - Supplemental material for RegulEm, a smartphone app based on the unified protocol for the transdiagnostic treatment of emotional disorders: description of its application in blended format in a clinical case
Supplemental material, sj-docx-2-dhj-10.1177_20552076251334442 for RegulEm, a smartphone app based on the unified protocol for the transdiagnostic treatment of emotional disorders: description of its application in blended format in a clinical case by Laura Martínez-García, Jon Belaunzaran Mendizabal, María Asunción Santos Goñi, Ignacio Miralles and Jorge Osma in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to acknowledge the user whose case is reported for agreeing to participate in this study and for sharing his story to help other people who seek psychological help in public services. We would also like to thank the therapist who carried out the intervention for his collaboration in the study and the psychologists and patients who participated in the RegulEm development process for making its development possible.
ORCID iDs
Ethical Considerations
This study was approved by the ethics committee of Euskadi's Medicine Research Ethics Committee on January 25, 2023, and adhered to the principles outlined in the Declaration of Helsinki.
Consent to participate and for publication
Written informed consent was obtained from the participant whose case is described in this study to participate and for anonymized patient information to be published in this article.
Author Contributions/CRediT
LMG and JO were responsible for conceptualization and methodology; JO was involved in funding acquisition and project administration; LMG and JBM did formal data analysis; LMG, JBM, MASG, and JO were involved in investigation; JO, JBM, MASG, and IM provided the necessary resources to carry out the study; LMG was responsible for writing and original draft preparation; LMG, JBM, MASG, IM, and JO carried out critical review. All authors have read and agreed to the final version of the manuscript.
Funding
This study was financed by the Ministerio de Industria, Economía y Competitividad ISCIII (PI20/00697), and the Gobierno de Aragón (Grant Number Research team S31_23R). Additionally, the Spanish Ministry of Universities supported this work through the “Formación de Profesorado Universitario” Program (FPU20/03796). The funders had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.