
Abstract
Background
Word-of-mouth learning (WOML) plays a substantial role in patients’ physician choice behavior. However, there is still a research gap in analyzing the mechanism of WOML on chronic disease patients’ physician choice in online health communities (OHCs) considering individual differences.
Objective
This study aims to develop a physician choice mechanism research model to reveal the influence of WOML on chronic disease patients’ physician choice decision process from external interaction to internal cognition and emotion in OHCs based on social learning theory (SLT). The moderating effects of reasons for consultation and patients’ demographic characteristics on the model's relationships were also explored.
Methods
Guided by SLT, this study identified the external interaction factors and internal cognitive and emotional factors by analyzing 72,123 patients’ online reviews based on a Latent Dirichlet Allocation model and developed the physician choice mechanism research model. The model was validated using structural equation modeling based on an online questionnaire survey of 526 valid Chinese patients with chronic disease. The moderating effect of reasons for medical consultation and demographic characteristics was examined using multi-group analysis.
Results
Status capital (SC), decisional capital (DC), and price value (PV)) were the main external interaction factors to initiating chronic disease patients’ internal cognition and emotion (perceived convenience (PC), perceived health benefits (PH), and patients’ physician choice intention (CI)). PH and PC significantly mediated the relationship between SC, DC, PV, and CI. Reasons for medical consultation, district, and sex significantly moderated the relationships in the model.
Conclusions
Considering individual differences, the results of this study advance a comprehensive understanding of how chronic disease patients interact with the environment through WOML to make physician choice decisions. OHCs can recommend suitable physician information to chronic disease patients considering individual differences to match patients’ demands and improve service quality.
Keywords
Introduction
Background
Online health communities (OHCs) connect patients, physicians, hospitals, and other entities involved in the medical ecosystem through the Internet. 1 Online consultations through OHCs are not only cost-effective and time-saving, but also provide better patient care. 2 Patients with chronic disease require frequent diagnosis and treatment communication due to the long disease duration, high mortality rate, long treatment time, and high service demand. 3 As a result, both patients and society bear heavy economic burdens. 4
Chronic diseases cause more than 70% of China's overall disease burden.5,6 As of 2019, nearly 180 million Chinese citizens suffered from chronic diseases, many of whom with multimorbidity.7,8 Patients with chronic diseases must regularly consult with their physicians during treatment. China's medical resources are unevenly distributed.9,10 While medical resources are relatively abundant in Eastern China, they remain scarce in Midwestern China. Consequently, this makes it difficult for Midwestern China to meet the growing demand for medical services. 11
Through OHCs, patients with chronic diseases can consult with qualified physicians across the country for medical advice, examinations, and prescription refills, contributing to the optimization of medical resource allocation.12,13 In 2021, 73.8% of Chinese patients underwent online medical consultations for chronic diseases. 3 Recently, a clear upward trend was observed. Chronic disease management has become an important engine for the future development of OHCs. 3 Unlike traditional medical settings, physicians and patients cannot communicate face-to-face in OHCs.
Scholars have extensively examined patients’ physician-choice behavior from the perspectives of physicians’ prosocial behavior, activity levels, free knowledge sharing, personal image and reputation on social platforms in OHCs14–18 based on physicians’ personal information (e.g., physician's academic background, number of patients, consultation price, and online image)19–23 and patients’ evaluation information (e.g., service evaluation and emotional expression reflected in online reviews).14–17 There are two main approaches to studying the factors influencing patients’ physician choice in OHCs. The first is regression analysis which examines the influence factors on physician choice in OHCs.16,19 The second is natural language processing, which is used to analyze patient-generated online reviews14,15 to identify the key factors influencing patient attitudes regarding physician consultation and patients’ adoption of OHCs. Word-of-mouth (WOM) quantity and quality can significantly induce or reduce patients’ physician choice behavior in OHCs. 24 WOML is the primary form of social learning that has proven can enhance motivation and significantly influence consumers’ online behavior in the field of marketing and e-commerce.25,26
Despite considerable research on the influence of WOM on patients’ physician choices in OHCs, there is still an analytical gap in developing the physician choice mechanism to examine the influence of WOML on chronic disease patients’ physician choice process. Studies have shown that differences in patient satisfaction with physician services are impacted primarily by reasons for medical consultation and patient characteristics. 27 However, a research gap exists on patients’ physician choice behavior considering individual differences. Therefore, identifying the mechanism of WOML on chronic disease patients’ physician choice in OHCs and analyzing the influence of individual differences of chronic disease patients’ reasons for medical consultation and demographic characteristics on physician choice behavior is imperative. By doing so, OHCs can improve their services and enhance their ability to prevent, control, and treat chronic diseases by meeting patient needs.
The objectives of this study were to generate a mechanisms model by which WOML influences chronic disease patients’ physician choice and analyze the moderating effects of reasons for the consultation and patients’ demographic characteristics on the model relationships.
Theoretical background
According to social learning theory (SLT), individuals can learn new behaviors through observation, which involves perceiving, interacting, and reproducing observed behaviors during the interaction.28,29 In the Internet era, SLT plays a significant role in influencing online behavior. 30 Individuals prefer to make online purchase decisions through the social learning process, which can be described as a two-interaction process (external and internal interaction). 31 In the external interaction process, individuals interact with the external environment through the social dimension. In the internal interaction process, individuals form internal cognition and emotion. Internal cognition is based on individuals’ knowledge and beliefs. Emotion determines whether to imitate others’ actions. 31 Therefore, SLT is highly suitable for our research and provides the basis for our analysis.
WOML is the main social learning method that conveys opinions on products or sellers which help individuals form cognitive frameworks and make purchase decisions. 25 Individuals communicate with the external environment through WOM. They can be influenced by the opinions of others by reading online reviews that transmit information about brands, sellers or products to individuals. 25 In the context of online shopping, individuals decide whether to imitate the behavior of others by observing consumer evaluations of a product, such as its description and service quality, which are important factors when making purchasing decisions.32,33 Previous studies have confirmed that positive WOM can promote consumer purchase decision-making, whereas negative WOM has a greater impact on consumer adoption decisions. 26
Scholars have applied social learning theory (SLT) to explain individuals’ decision-making behavior in various economic and social phenomena.25,34–36 However, there is a gap in the analysis of patients’ physician choice behavior in OHCs utilizing SLT. Accordingly, this research analyzed chronic disease patients’ physician choice behavior from external interaction to internal cognition and emotion in OHCs during the WOML process based on the SLT framework.
Study overview
To present theoretical and empirical support, drawing upon SLT, a latent Dirichlet allocation (LDA) model was used to analyze chronic disease patients’ online reviews to identify the external interaction, internal cognitive and emotional factors during the process of WOML and develop the physician choice mechanism research model.
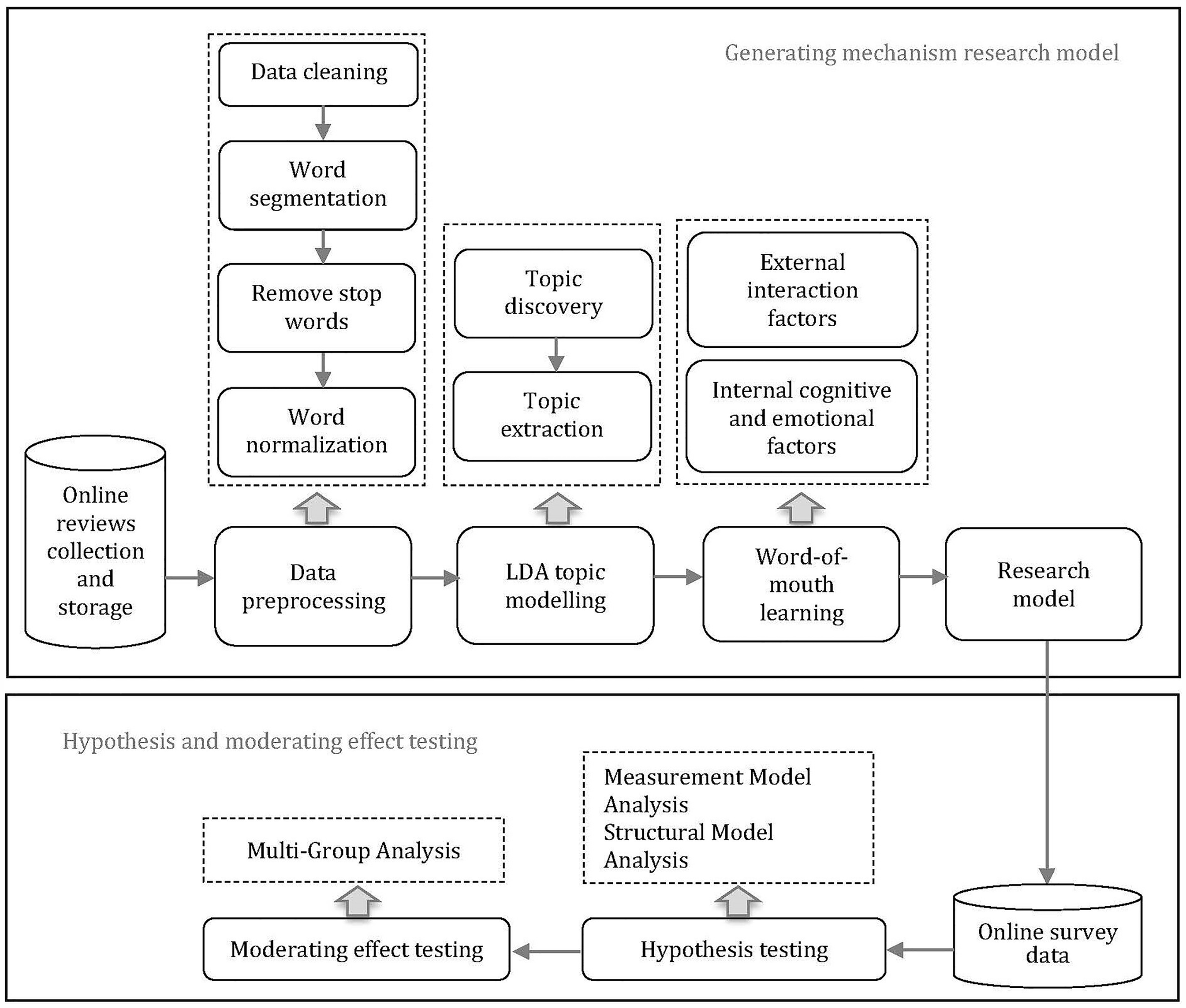
To estimate how these factors affect chronic disease patients’ physician choice behavior, and investigate the moderating effects of reasons for the consultation and patients’ demographic characteristics on the relationships in the research model, we conducted a cross-sectional online survey to examine the research model based on structural equation modeling (SEM) and tested the moderating effect of reasons for medical consultations and demographic characteristics based on a multi-group analysis (MGA). Figure 1 illustrates the research framework.
Research framework.
Research model and hypotheses
External and internal interaction in WOML
WOML helps individuals form cognitive frameworks and make purchase decisions by discovering their peers’ attitudes toward products or sellers in online reviews. 25 Patient reviews include the evaluations of physicians’ medical consultation, such as physicians’ communication skills, medical knowledge, bedside manners, personal ethical practices, internal cognitive and internal emotion. These factors are important to patients when selecting a physician.14,37 Scholars have employed natural language processing to analyze online reviews in OHCs and identify patient attitudes and experiences regarding physician consultation.14,15 Online reviews are an important subjective information resource for patients when choosing physicians.38,39 This study used the LDA model to identify external interaction, internal cognitive and internal emotional factors influencing patients’ physician choices.
Data collection and preprocessing
The online review data was obtained from WeDoctor, a leading OHCs platform in China, which provides patients’ comments on physicians according to disease type. We wrote a crawler program to gather online reviews in WeDoctor from chronic disease patients in six disease categories: heart disease, diabetes, chronic obstructive pulmonary disease, chronic kidney disease, asthma, and arthritis. Online review data included patient identifiers, physician names, review content, and review dates. As the number of online reviews for some physicians was small, 379 physicians treating chronic diseases were selected. The following steps were executed for preprocessing procedures (Figure 1). Firstly, we filter patients’ online reviews. Duplicate reviews for the same physician and reviews that did not involve specific subjective information were removed. Emoticons were replaced with their corresponding Chinese expressions. Since Wedoctor only allows patients who have made consultations to leave online reviews. There were no fake online reviews that influenced patients’ physician choice decisions. We also delete shorter online reviews of no more than five words which rarely include evaluations of the medical consultation experience. Finally, we obtained 72,123 online reviews involving 379 physicians from June 2015 to June 2024. Secondly, 'Jieba' package was employed to carry out tokenisation. Thirdly, stop words, punctuation and numbers were removed. Lastly, we removed the low-frequency words.
Topic modeling
LDA is a generative probabilistic model commonly used for uncovering topics from a corpus of documents.40,41 The process begins with assigning topics at random, followed by the computation of word distributions for each topic, as well as topic distribution within a document. Through the process of document allocation, it became possible to determine the leading topic for each online review included in the dataset. Figure 2 illustrates the process of document generation of LDA. Where

Graphical model representation of LDA.
In this research, the corpus is a collection of all patients’ online reviews. For every online review i in the corpus, an estimate
We determined the number of topics based on coherence score cross-validation which conducts an iterative process of running the LDA topic model by incrementally raising the number of topics.42,43 For every analysis conducted, a coherence score is generated. The coherence score measures how interpretable the topics are to humans and is suggested as an indicator for identifying the optimal number of topics. 42 We compared the coherence score of the LDA topic number k from 1 to 30. According to the coherence score and manual examination, the best model with 6 topics was selected and the coherence score was 0.441 (Figure 3).
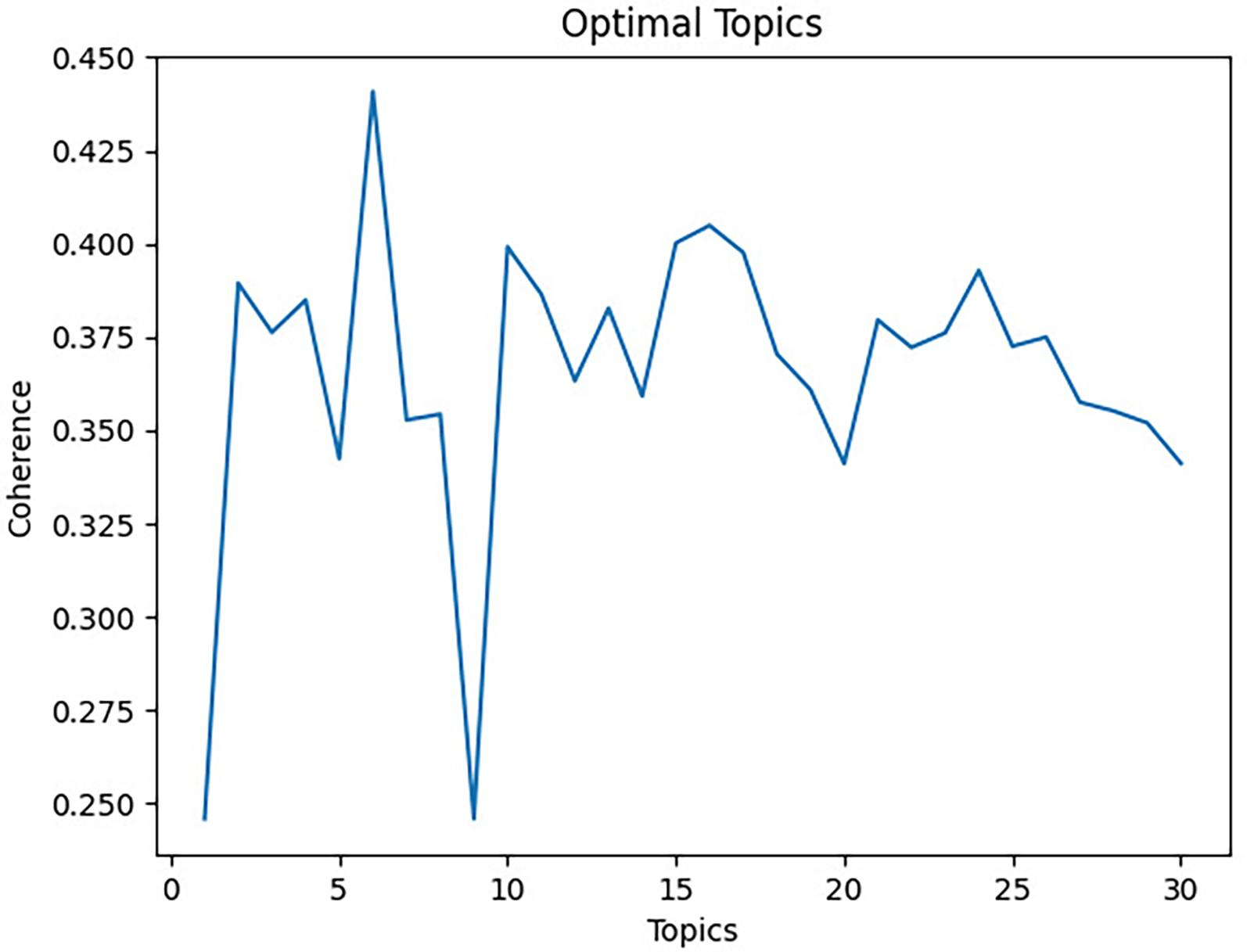
Coherence score plot for LDA model.
Topic labeling
We can define the meaning of various topics through the assignment of appropriate descriptive words or phrases. 44 In this research, topic labeling was manually done by evaluating the top words of each topic. 45 According to studies on physician choice in OHCs,14,15 three expert opinions of OHCs, and high-frequency feature words in each topic, final definitions were determined for the six topics. Ten words were chosen as high-frequency feature words. Table 1 shows each topic's names, high-probability words, and examples.
Topics in LDA model.
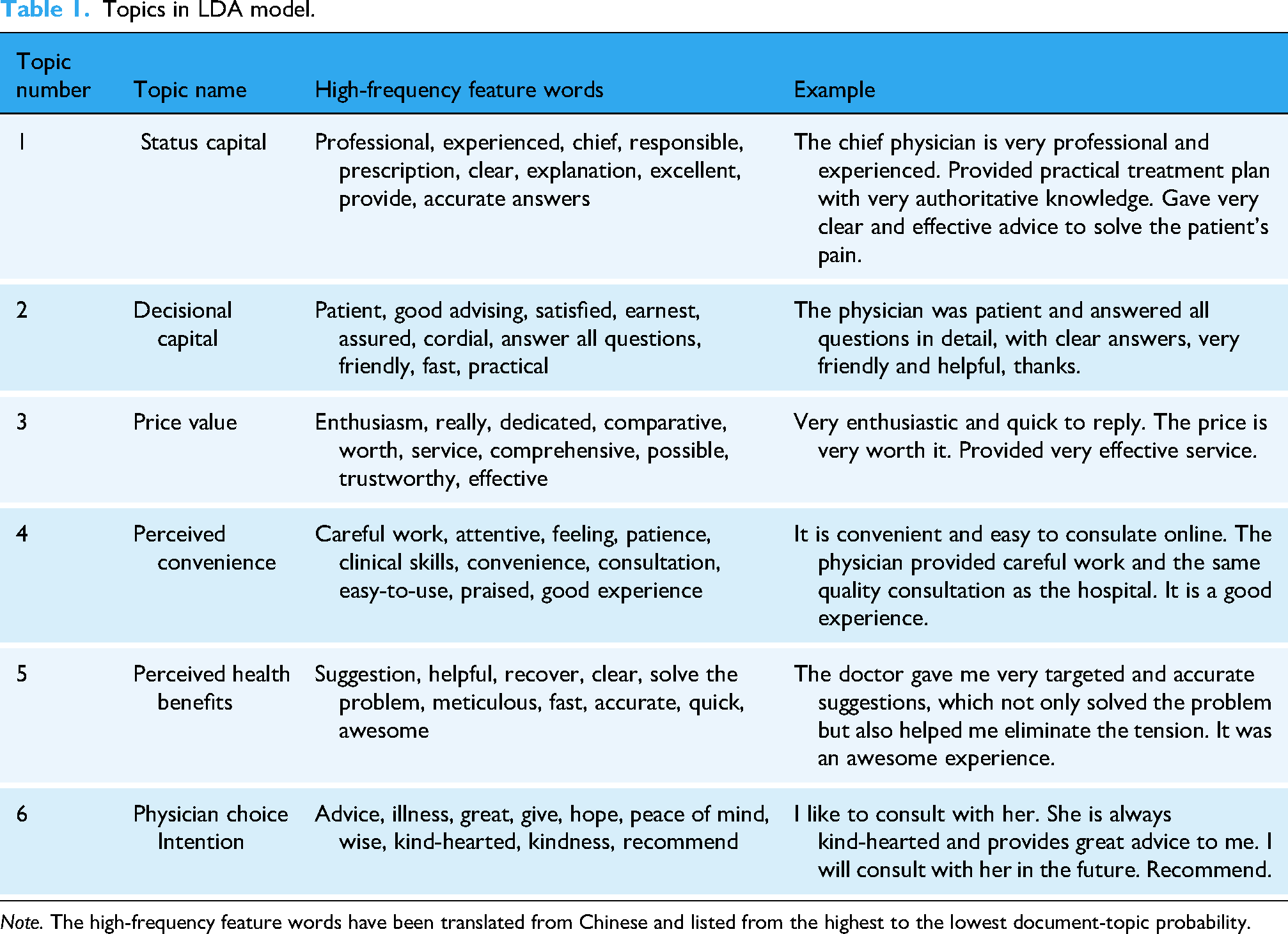
Note. The high-frequency feature words have been translated from Chinese and listed from the highest to the lowest document-topic probability.
The results of the WOML analysis suggest that physician status capital (SC), decisional capital (DC), and price value (PV) are external interaction factors patients learned through environmental interaction during the WOML process. Perceived convenience (PC), perceived health benefits (PH), and patients’ physician choice intention (CI) are internal cognition and emotional factors patients learned through the psychological acquisition process through WOML.
Hypotheses and modeling
Status capital and perceived convenience
In online consultations, patients evaluate physicians’ SC through their academic titles, clinical titles, hospital level to which the physician belonged, and hospital location.
45
Typically, high SC reflects physicians can provide high-quality medical treatment.46,47 Although SC does not reflect a physician's online behavior, patients with chronic diseases especially patients who are not in the same geographic area as the physicians will perceive the convenience of choosing a physician with high SC in OHCs, given the scarcity of physicians with high SC and the difficulty of consultation with physicians with high SC offline. Thus, the following hypothesis is: H1a: SC positively affects chronic disease patients’ PC in OHCs.
Decisional capital and perceived convenience
DC refers to physicians’ quality of interaction with patients and their ability to provide effective diagnosis and treatment.37,47,48 Physicians must show their DC to earn more trust from patients.
49
Physician's DC has been proven a key factor influencing patients’ physician choices in OHCs.50–52 In online consultations, patients cannot communicate with physicians in person. This absence of direct interaction elevates the importance of physicians’ DC. Physicians with high DC can develop adequate communication with their patients, enabling patients with chronic diseases to receive a consultation experience akin to that of face-to-face interactions,
47
and then perceive the convenience of online consultation. Thus, the following hypothesis is: H2a: DC positively affects chronic disease patients’ PC in OHCs.
Price value and perceived convenience
PV is the subjective judgment of a customer concerning the value of a company's product or service. Customers prefer to assess the utility of a product after weighing its perceived benefits to cost.
53
They like to acquire products or services when they can obtain more value for their money.54,55 In the context of OHCs, studies show that PV can positively affect patients’ physician choices.
50
Compared to traditional hospital consultation, the most distinguishing advantage of online consultation is convenience.
2
When the PV of online consultation is greater than or equal to the PV of traditional hospital consultation, chronic disease patients will perceive the convenience of online consultation. Thus, the following hypothesis is: H3a: PV positively affects chronic disease patients’ PC in OHCs.
Status capital and perceived health benefits
SC refers to physicians’ social status (e.g., job title, affiliations, etc.). Physicians with high SC means they have a high title and come from a hospital with a high level, which stands for their advantages in academic research and clinical experience, and their ability to dispatch and use more advanced medical resources during diagnosis.46,52,56 The purpose of online consultation for patients with chronic diseases is to address health issues, particularly for those living in regions where medical resources are scarce. Consulting with a physician with a high SC in OHCs will allow patients to perceive health benefits. Thus, the following hypothesis is: H1b: SC positively affects chronic disease patients’ PH in OHCs.
Decisional capital and perceived health benefits
DC reflects physicians’ ability to accurately express, insight and diagnose patients’ conditions, and willingness to communicate with patients online, which is the foundation for patients’ physician choices.46,57 Physicians with high DC can provide accurate diagnoses and adequate treatment services, enabling patients with chronic diseases to perceive health benefits. Thus, the following hypothesis is: H2b: DC positively affects chronic disease patients’ PH in OHCs.
Price value and perceived health benefits
The core function of OHCs is to be able to address the diagnostic and treatment needs of chronic disease patients, thereby enhancing their physical health.
12
Chronic disease patients need to regularly consult with physicians for medical advice, examinations, and prescription refills. In particular, given the geospatial and time constraints of offline consultations,
49
chronic disease patients will perceive the health benefits of online consultations when the PV of online consultations are greater than offline. Thus, the following hypothesis is: H3b: PV positively affects chronic disease patients’ PH in OHCs.
Perceived convenience and physician choice intention
PC refers to the time and effort consumers save during the purchasing process, which includes allowing them to contact sellers quickly, find the products they need, and conveniently complete their purchases. 58 In this study, PC indicates patients can conveniently obtain medical consultations through OHCs. Chronic disease patients require frequent medical consultation. 3 Once chronic disease patients assess that the physician they wish to consult matches the services they expect and achieve the same results as offline consultations, they perceive the convenience of online consultation. Moreover, their intention to consult the physician increases.
Thus, the following hypothesis is: H4. PC positively affects chronic disease patients’ CI in OHCs.
Perceived health benefits and physician choice intention
Generally, chronic disease patients seek medical advice when they believe the physician can benefit their health.
50
Through WOML, patients can assess whether the physician can provide them with the desired perceived health benefits. When chronic disease patients require physicians to treat high-risk diseases, they prefer to select physicians with high SC and DC even though the consultation cost is higher.
59
However, when such patients seek online consultation for prescription refills, they may choose a physician with a lower consultation cost. Once the physician matches chronic disease patients’ desires, they perceive health benefits, and their intention to choose the physician increases. Thus, the following hypothesis is: H5. PH positively affects chronic disease patients’ CI in OHCs.
Based on these eight hypotheses, we summarize our conceptual model (Figure 4).

Conceptual model.
Methods
Participants and data collection
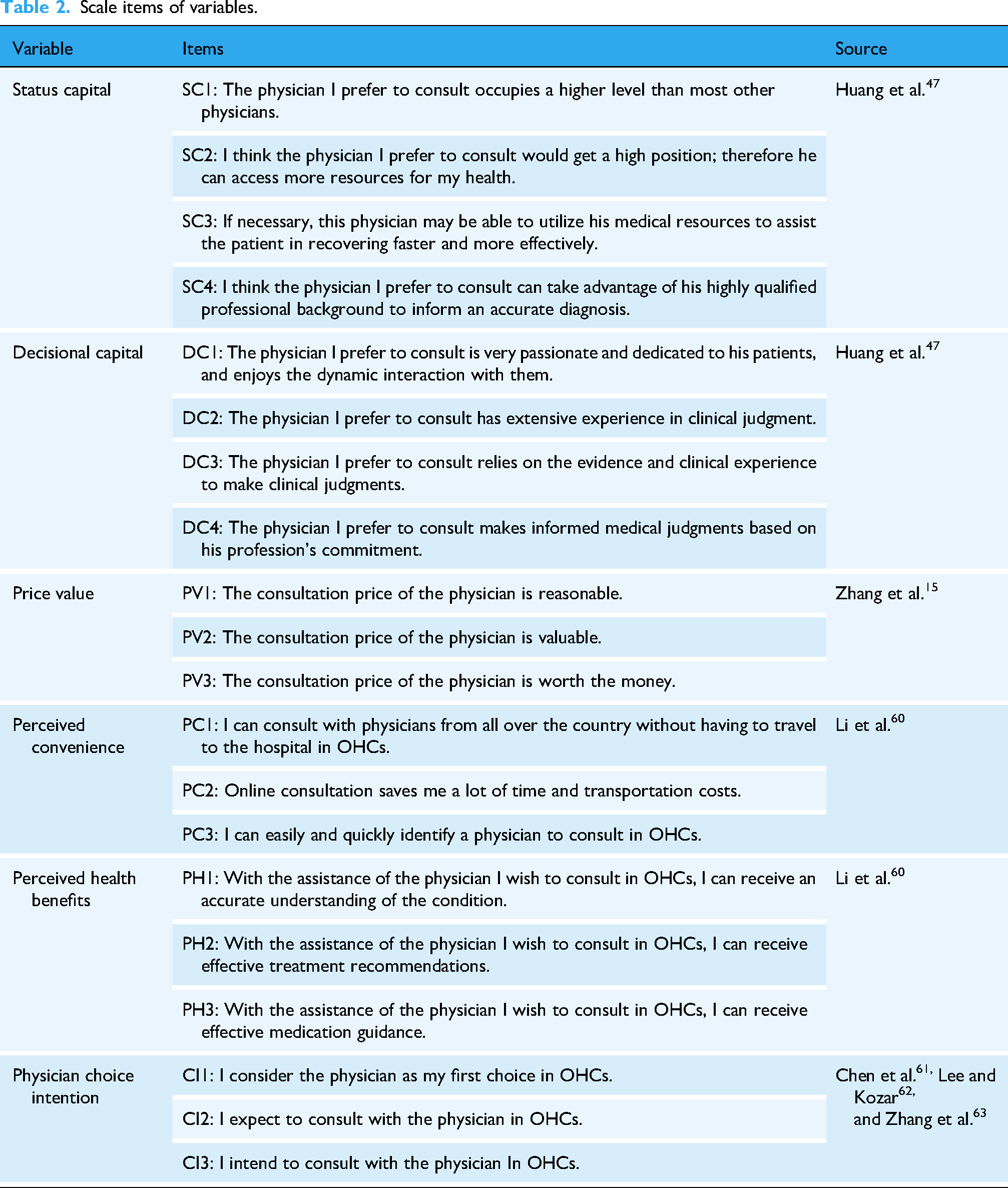
An anonymous online survey was conducted in 31 provinces of China between January and June 2024 using Credamo, a leading survey company that provides one-stop data collection solutions. The platform has a database of over three million respondents and can deliver surveys to targeted respondents based on demographic characteristics. Based on previous studies, A survey scale was developed to measure 20 items related to 6 variables associated with chronic disease patients’ physician choice in OHCs. SC and DC measurements were adapted from Huang et al.; 47 PC and PH were evaluated based on Li et al.; 60 PV was adapted from Zhang et al.; 15 CI was measured based on Chen et al., 61 Lee and Kozar, 62 and Zhang et al. 63 (Table 2). A 7-point Likert scale ranging from strongly disagree to strongly agree was used to measure the items.
Scale items of variables.
Since all our participants were from China, we employed a forward-backward translation method to translate our questionnaire in accordance with previous studies.64,65 First, two independent translators and one translator proficient in both English and Chinese translated the questionnaire into Chinese. Next, two professionals with medical translation capabilities compiled the two Chinese versions of the questionnaire and translated them into English. As a result, we selected 65 chronic disease patients who had consultation experiences in OHCs for a preliminary survey and refined the questionnaire to determine the final version. Chronic disease patients’ reasons for medical consultation and demographic items were collected for moderating effect analysis. To ensure that all respondents had online consultation experience, we asked two initial questions: "Do you have online consultation experience in OHCs?" and "What was your reason for the previous online consultation? The final sample consisted only of respondents who had experience with online consultations. We estimated that a reasonable time to complete the questionnaire should not be less than 60 s; thus, questionnaires with a response time shorter than 60 s were considered invalid. Finally, 526 valid questionnaires were obtained.
Demographic characteristics
Regarding demographic data, among the 526 participants (184 males and 342 females), the participant pool consisted of approximately 65% females, and the sex distribution is close to the data of China's online medical and health services consumption white paper report by iResearch 2022, a leading Chinese consulting firm which proved that the sex ratio for the overall actual and potential population is approximately 66.67 males to 100 females. Undergraduate and higher education participants accounted for 94.6%. A total of 34.8% of the participants came from East China, and 65.2% from Midwest of China. Of these participants, 57.6% had no more than 8000 monthly income. Moreover, 84.8% of the participants were aged < 41 years (Table 3).
Demographic statistics of respondents (N = 526).

Ethical considerations
All participants submitted written informed consent online before attending the survey. This research was approved by the Scientific Research Ethics Committee of Alibaba Business School at Hangzhou Normal University (approval number: 20240001). All participants were anonymous. Participants who completed the survey were awarded a cash reward.
Results
Measurement model analysis
This study investigates the reliability, convergent validity, and discriminate validity of the measurement model. SPSS 27.0 was used to test data reliability. Table 4 illustrates that all of the variables had Cronbach's alpha coefficients and CR values greater than 0.8, exceeding the recommended threshold of 0.7, which indicates a high level of reliability.66–68 Table 4 shows that the standardized factor loadings and AVE values exceeded the threshold of 0.5, which indicates sufficient convergent validity.69,70 AMOS 24.0 was used to conduct the CFA to examine the validity of the model. Based on the fitness indices (
Results of reliability and validity analysis.

Note. CR: composite reliability; AVE: average variance extracted; SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Discriminate validity.

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention; The square root AVE of each construct is bolded on a diagonal.
Structural model analysis
We employed AMOS 24.0 to evaluate the structural model. The fit indices (

Results of the structural model.
Results of hypotheses test.

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Results of mediation effects analysis (standardized coefficients).

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Multi-group analysis
Using pairwise comparisons of each relationship between the unconstrained and constrained models, differences between reasons for medical consultation, districts, and sex groups were identified. We impose an equal constraint on each path in the constrained model. A moderating effect exists if the change of chi-square values in the two models is significant. 66 We employed AMOS 24.0 to conduct MGA.
Regarding the comparison of reasons for medical consultation (Table 8), the path coefficients between PV and PC (
Results of MGA by reasons for medical consultation.

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Based on a comparison of the districts (Table 9), there are two significant path differences between the Eastern and Midwestern China groups. The effect of PV on PH (
Results of MGA by district.

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Table 10 shows that sex had a significant moderating effect on the relationship between PH and CI (
Results of MGA by sex.

Note. SC: status capital; DC: decisional capital; PV: price value; PC: perceived convenience; PH: perceived health benefits; CI: physician choice intention.
Discussion
Principal findings
This study developed a physician choice mechanism model to examine the influence of WOML on chronic disease patients’ physician choice process in OHCs. The three principal findings are as follows:
First, according to the LDA topic analysis of online reviews, SC, DC, and PV were identified as the main antecedents affecting physician choice during the external interaction process. This was consistent with previous research on the factors influencing patients’ physician choice.22,35,52 Furthermore, PC and PH were the main internal cognitions that patients with chronic disease learned from their internal cognition, which is rarely discussed in existing research. Since chronic disease patients require frequent diagnosis and treatment communication, patients will balance PH and PC according to physicians’ SC, DC, and PV, and finally make physician choice decisions based on their needs.
Second, based on the results of the LDA topic analysis, we developed a physician choice mechanism model to examine the influence of WOML on chronic disease patients’ physician choices. SC, DC, and PV were confirmed as all having positive correlations with PH and PC, and both PH and PC were positively correlated with CI. The mediating role of PC and PH in the relationships among SC, DC, PV, and CI were verified. This suggests that physicians’ SC, DC, and PV play a vital role in chronic disease patients’ physician choices. This is consistent with existing studies highlighting the importance of SC, DC, and PV on physician choice.15,47
Third, it was proven that reasons for medical consultation, district, and sex significantly moderated the relationships in the model. In existing research, it is rarely discussed. Based on these results, we found that the impact of PH on CI was stronger for patients seeking medical advice consultations (male patients) than for those seeking prescription refills (female patients). A possible explanation is that the purpose of patients seeking medical advice consultations (male patients) pays more attention to PH than those seeking prescription refills (female patients) in online medical consultations. We also identified that PV (DC) has a significant positive effect on PC (PH) for patients seeking prescription refills (patients from Midwest China). However, the influence of PV (DC) on PC (PH) is not significant for patients seeking medical advice (patients from East China). This could be explained that online consultations for prescription refills are more convenient than offline, so PV makes it easier for them to perceive the convenience of online consultations. The main purpose of patients from Midwest China is to seek better medical resources through online medical consultations. Physicians with high DC enable patients from Midwest China to perceive health benefits. Additionally, this study also identified the impact of PV on PH was smaller in patients with chronic disease from the Midwest than in those from the East. There is a possible explanation that qualified physicians are scarce in Midwestern China which led to the consultation price having less impact on perceived health benefits for patients from the Midwest than for patients from East China.
Theoretical contributions
The study contributes three theoretical insights to the literature. First, we applied SLT to analyze the mechanisms of chronic disease patients’ physician choice in OHCs during the process of WOML which revealed the physician choice process from external interaction (SC, DC, and PV) to internal cognitions (PC and PH) and, finally to internal emotion (CI), expanding the application of SLT theory to the OHCs field. Although previous studies have verified the factors influencing patients’ physician choices,22,35,52 there is still a research gap regarding patients’ psychological processes that stimulate chronic disease patients’ physician choices. This study opens the black box of the physician choice mechanism for patients with chronic diseases and contributes new insights to the existing literature on patients’ physician choice in OHCs.
Second, according to the WOML based on the SLT, by introducing PC and PH as mediating variables, the resulting findings provide insight into patients’ cognition of physician choices in OHCs. Although previous studies have verified that WOM is a key factor influencing patients’ physician choice behavior in OHCs,19,21 there is still a research gap regarding how WOML affects patients’ psychological processes that stimulate chronic disease patients’ physician choices. We demonstrated that both PC and PH can positively impact chronic disease patients’ CI. Guided by SLT, experience and guidance about chronic disease patients’ cognition and behavioral responses in physician choice are provided to help inform future research on this subject.
Finally, by examining the moderating effects of reasons for medical consultation and demographic characteristics, we developed a better understanding of the individual differences among patients’ physician choice mechanisms. Despite previous studies examining the mediating role of disease risk in service choices in OHCs, 50 little is known about the moderating effects of reasons for the consultation and patients’ demographic characteristics on patients’ physician choice behavior. The results provide valuable supplementation concerning the moderation effect of reasons for medical consultation, district, and sex on the chronic disease patients’ physician choice behavior.
Practical contributions
Specifically, our research has practical implications for physicians and OHCs to improve consultation quality for patients with chronic diseases.
First, results show that SC, DC, and PV are key antecedents of chronic disease patients’ physician choices, which initiate the internal cognitive process. PC and PH are internal cognitive factors which determine chronic diseases patients’ physician choice in OHCs. For physicians, in addition to clinical titles, emphasizing their skills and abilities in personal information in OHCs, setting reasonable consultation prices, 15 and improving their DC can increase the possibility of patients’ choices.12,49 For OHCs service providers, optimizing platform functions, improving the convenience of consultation, and strengthening the qualification review of physicians can stimulate patients’ behavioral intentions based on analyzing chronic disease patients’ needs for medical consultation in OHCs. For example, the introduction of artificial intelligence-assisted diagnosis and treatment provides patients with an initial diagnosis based on their own conditions and treatment needs and matches them automatically with the appropriate physician.
In addition, the results showed that reasons for medical consultation had a significant moderating effect on the relationship between PV and PC as well as PH and CI. District had a significant moderating effect on the relationship between DC and PH as well as PV and PH. The relationship between PH and CI is significantly moderated by sex. Therefore, for physicians, suitable consultation prices should be formulated for patients from different districts and increase the PV of patient consultations. Physicians should improve their diagnosis and treatment services quality to enhance male patients and patients requiring medical advice’ PH. For online health consultation service providers, artificial intelligence technology could be applied to recommend suitable physicians to patients based on their reasons for medical consultation and demographic characteristics. For example, for patients requiring medical advice (prescription refills), OHCs should recommend physicians with high SC and high DC (high PV) to improve patients’ PH (PC), which is more likely to help patients’ decision-making. For patients from Midwest China (East China), OHCs should recommend physicians with high DC (high PV) to improve their PH. For male patients, OHCs should recommend physicians with high SC, DC, and PV to improve their PH, which helps patients’ decision-making.
Limitations
This study has some limitations. First, the data used were derived only from China. The physician's choice behavior for patients with chronic diseases can be influenced by the degree of OHCs development and cultural differences in different countries. Future research could be expanded to other countries to enhance the applicability of our research model. Second, this study did not consider differences in physician choice behavior in OHCs among patients with different types of chronic diseases. In OHCs, different chronic diseases have different treatment options, which influence the patients’ physician choice behavior. The behavior of patients with severe chronic diseases differs from that of patients with common chronic diseases. Therefore, further research is needed to examine the differences in physician choice behaviors among chronic patients with different diseases. Third, the distribution of patients’ demographic characteristics varies in diverse online health communities. The moderating effect of patients’ demographic characteristics on the mechanism research model relationships may be different. Online health communities should develop operational strategies based on the distribution of patients’ demographic characteristics of their platform. Finally, owing to the privacy policy of OHCs, we were unable to obtain patients’ personal information. In the future, it may be possible to obtain patients’ personal information and combine it with their consultation behavior data from OHCs to conduct more accurate research.
Conclusions
Based on SLT, this study identified external interaction factors, internal cognitive factors, and internal emotional factors influencing chronic disease patients’ physician choices during the WOML process and developed a physician choice mechanism model. Our findings indicate that SC, DC, and PV are key antecedents to initiating internal cognition in patients with chronic diseases. Internal cognitive, such as PC and PH, determine physician choices behavior for chronic disease patients. Furthermore, reasons for medical consultation, district, and sex significantly moderated the relationships in the model. This study extends SLT to the study of OHCs, reveals chronic disease patients’ physician choice mechanisms, provides new insights about patients’ physician choice in OHCs, and offers empirical evidence for physicians and OHCs to improve diagnosis and treatment services for chronic disease patients considering individual differences.
Footnotes
Acknowledgements
We are grateful to acknowledge and thank all participants for their invaluable support, which made the completion of this study achievable.
Ethics approval
This study was approved by the Scientific Research Ethics Committee of Alibaba Business School at Hangzhou Normal University (approval number: 20240001). Informed consent was obtained from all participants. Consent can be obtained from the corresponding author. To protect participants’ privacy, these consents are not accessible to the public.
Contributorship
Linlin Han and Narongsak (Tek) Thongpapanl were key contributors to formulating the conceptual framework of this study, data collection, data analysis, and manuscript writing. Ou Li performed data collection, data analysis, and manuscript preparation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hangzhou Key Research Base of Philosophy and Social Sciences “Research Center for Innovation and Development of Platform Economy”, Humanities and Social Science Research Project of the Ministry of Education of China, (grant number 24JD024, 23YJC630086).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Linlin Han