
Abstract
Background
Childhood obesity significantly impacts health, making the promotion of healthy behavior (HB) among children crucial to address this issue. Virtual reality (VR) has emerged as a promising tool for encouraging HB in children.
Objective
This systematic review aims to evaluate the literature on the application of VR in promoting healthy dietary habits and physical activity (PA) among children.
Method
A systematic search was conducted across Web of Science, PubMed, and Scopus databases in January 2024 according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, focusing on English-language studies published between 2013 and 2023. The quality of the studies was assessed using the Cochrane Risk of Bias 2 and Risk of Bias in Nonrandomized Studies of Interventions tools. This review is registered at PROSPERO, CRD4202347801.
Result
A total of 25 studies involving participants aged 4–15 years were assessed. Sixteen studies focused on increasing PA through VR interventions, and six studies focused on healthy eating. Most studies utilized nonimmersive (n = 11) or semi-immersive (n = 10) VR technologies. Six theories were employed across the studies, and five design strategies were categorized. While most studies reported improvements in PA (n = 9) and healthy eating (n = 6), the short durations and small sample sizes limited the assessment of long-term impacts.
Conclusion
This review reveals the promising potential of VR as an effective tool to enhance PA and promote healthier eating among children. However, it also highlights the need for further rigorous research to explore the long-term effects of VR interventions on child HB change. These findings provide valuable input into the development of more effective VR interventions that can be applied in child health strategies.
Highlights
Reviewed virtual reality interventions promoting physical activity and healthy eating in children.
Key theories applied include Self-determination and Social Cognitive Theories.
Revealed the effectiveness of VR intervention in promoting physical activity and healthy eating in children.
Design strategies include virtual avatar, narrative, and goal setting.
Research gaps highlight the need for long-term rigorous studies.
Introduction
Childhood obesity is a serious global health problem, with over 390 million children identified as overweight or obese in 2022. 1 Children living with obesity are at higher risk of diabetes and cardiovascular disease. While diseases and genetic factors can contribute to childhood obesity, the primary cause is an imbalance between calorie intake and expenditure. 2 Addressing this issue requires promoting healthy behaviors (HBs) including dietary habits and more physical activity (PA) among children. 1 Consequently, developing effective interventions that encourage these HBs is critical.
Interactive technology–based interventions have been widely used in the field of child health. Virtual reality (VR) technology, which provides a multisensory, interactive, and controllable environment, is a potentially valuable intervention for promoting healthier diets and lifestyles. 3 VR is a computer-generated simulation that creates immersive environments similar to real life. It enables functionalities that may be difficult to achieve in reality, with sensors recording user behavior and providing timely feedback, and the environment adapting to user movements. 4 For children, this sense of immersion and interactivity enhances their engagement and concentration on virtual scenes and narratives, which provides opportunities to guide and study children's health-related behavior. Previous studies demonstrate the effectiveness of VR in influencing children's behavior and education, such as improving dietary choices and increasing PA time.5,6 Hence, VR has great potential in promoting healthy eating habits in children, encouraging them to maintain PA, and thereby promoting HB. This systematic review aims to review and evaluate the effectiveness of VR interventions in promoting healthy eating and PA among children, contributing to the broader efforts to child health.
Background
Virtual reality systems and types
VR technology encompasses a range of systems from nonimmersive to fully immersive. While the traditional definition of VR emphasizes a fully immersive environment provided by an advanced head-mounted display (HMD), a broader definition includes any computer-generated simulation that allows the user to interact with a virtual environment (VE). 7 For the purposes of this review, an inclusive framework of three VR types will be adopted to cover nonimmersive, semi-immersive, and fully immersive VR systems. This categorization is consistent with previous research8,9 that aims to explore the full range of digital interventions that use VR to influence children's HB.
Nonimmersive VR refers to computer-created virtual simulations that allow users to interact with VE through traditional devices (such as computers, touch screens, and input devices such as mouse and keyboard) while retaining control of the physical environment. 10 These digital intervention systems do not provide full immersion, but still involve complete virtual situations and could achieve interactive feedback, allowing users to experience the health decision-making process through the designed simulation scenarios. 11 Semi-immersive VR provides a more immersive experience than nonimmersive VR by using high-resolution displays and projectors, allowing users to interact with the VE through screens or basic headsets while remaining aware of their physical environment. Examples include virtual tours or interactive 3D environments, which provide enhanced visual engagement without full sensory immersion. 12 Finally, fully immersive VR offers the most realistic experience by fully enveloping users in the VE through advanced HMDs, handheld controllers, and multisensory feedback (visual, auditory, and haptic), creating a sensation of being physically present in the virtual world. These systems create a sensation of being physically present in the virtual world, making them particularly effective for health interventions requiring high levels of engagement and interaction.13,14 Each VR type has unique benefits and can promote health habits. Besides, understanding the different types of VR systems is essential for evaluating their potential in interventions aimed at promoting children's healthy dietary behavior and PA.
Previous work
The application of VR in health-related interventions has attracted increasing attention. Many systematic reviews have focused on adult populations and specific health factors. For example, VR has been evaluated as a tool to help adults with weight management, finding that VR interventions incorporating cognitive behavioral concepts were effective in supporting weight loss, improving health self-efficacy and body image satisfaction. 15 In another review, the authors not only examined the effectiveness of VR in reducing the risk of obesity but also primarily addressed adult participants. 16
Emerging research demonstrated that VR's ability to create interactive environments is not limited to weight management but can address a wider range of HB. Tatnell et al. 16 reviewed the effectiveness of VR in influencing smoking, nutrition, alcohol consumption, PA, and obesity. This review found that VR-based interventions were generally superior to traditional methods (conventional nondigital intervention, such as treadmill running and nutrition lectures) in promoting PA and improving nutritional behaviors, but no firm conclusions were drawn about long-term outcomes such as body mass index (BMI) reduction. Importantly, this review highlights the potential of VR to engage people in active health-related behaviors, especially when traditional interventions cannot be carried out, such as during the Coronavirus disease of 2019 (COVID-19) lockdown.
In addition, VR has been explored in the context of gaming and its effects on cognitive and emotional states. A review explored the intersection of neurogaming and VR, highlighting VR's ability to engage participants and maintain attention through gaming experiences. 17 This suggests that VR may be a tool to promote sustained HB change in children, and by utilizing gamification and cognitive engagement, VR interventions may encourage children to develop healthy eating habits and PA.
Despite these encouraging developments, research on VR interventions in childhood HB is limited. Lu et al. 18 reviewed the effects of health-promoting video games on children, finding that approximately 40% of the studies reported positive impacts on weight loss. However, this review primarily focused on nonimmersive VR and did not comprehensively address other VR types. Similarly, Lamas also focused on the impact of serious games on children's PA and diet and emphasized that games should be diversified and a broader perspective should be sought. 19 To date, despite the promising potential of VR interventions for improving childhood HB, few systematic reviews have comprehensively evaluated the effectiveness. Systematic reviews of current research on VR interventions that promote healthy eating and PA in children are needed to fill this gap.
Review scope
This systematic review aims to provide a thorough evaluation of the literature on the application of VR in promoting healthy dietary habits and PA among children, key factors in promoting HB. Specifically, it focuses on: (1) reducing or restricting the intake of unhealthy foods such as high-calorie and high-sugar foods, increasing the intake of nutritious foods such as fruits and vegetables (F&V), and improving a balanced diet; and (2) reducing sedentary behavior and enhancing PA.20,21 Studies addressing indirect factors, such as the family dietary environment and school health education, are excluded from this review.
This systematic review seeks to answer the main research question (RQ): How effective are VR-based interventions in influencing children's dietary habits and PA levels to promote health? To answer this question, this review will be guided by the following research objectives (RO): RO1: To review the intervention approaches aimed at promoting healthy eating and increasing PA among children, and to identify the types of VR employed in the included studies. RO2: To identify the theoretical frameworks or models that guided the development of VR interventions. RO3: To investigate the specific design strategies utilized in VR and assess their potential benefits in influencing children's HB and attitudes. RO4: To assess the effectiveness of VR in promoting healthy dietary habits and PA by examining outcomes reported in the included studies. RO5: To identify current research gaps in the use of VR for promoting HB among children and to provide recommendations for future research and practical applications.
Methods and materials
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol of this systematic review was registered with PROSPERO (International Prospective Register of Systematic Review) (protocol ID: CRD4202347801).
Literature search
The literature search was conducted in January 2024 using three primary databases: Scopus, Web of Science, and PubMed. Additionally, reference lists and other databases like CINAHL Complete were examined to ensure the inclusion of as many relevant articles as possible.
The search strategy was developed based on the Population, Intervention, Comparison, and Outcome framework. The search terms included combinations of keywords related to: Population: “children” OR “pupil”; Intervention: “virtual reality” OR “VR” OR “virtual environment” OR “immersion”; Outcome: “obesity” OR “overweight” OR “health” OR “diet” OR "food” OR “nutrition” OR “activity” OR “exercise” OR “sedentary.” These terms were combined using Boolean operators to identify relevant English-language articles published between 2013 and 2023. The search was performed across the three databases, resulting in the identification of 2288 articles. In addition, manual searches of other sources led to the discovery of an additional three articles, resulting in a total of 2291 records during the initial stage of the systematic review process.
Eligibility criteria
Inclusion criteria:
Articles published in English between 2013 and 2023. Studies were included if they involved an interactive virtual simulation scenario designed to promote or change children's attitudes or behaviors toward healthy food, nutrition, or PA. Empirical research articles, including randomized controlled trials, quasi-experimental studies, observation studies, and qualitative studies. Studies focusing on children under 18 years old, regardless of weight status, country, race, or sex.
Exclusion criteria:
Reviews or meta-analyses. Books, book series, book chapters, conference papers, or dissertations. Studies focusing on subjects with health conditions, such as mental illness or disabilities. Studies focusing on the use of VR to promote children's healthy dietary habits and PA by improving indirect environmental factors.
Screening process
All studies were imported into the reference management software for further screening. Two independent reviewers conducted the process, with a third resolving disagreements. First, 598 duplicate records were excluded, and 1610 studies were excluded because they were review papers, books, or conference papers or because the subjects were children with disease; 83 studies were left for full-text screening, 2 studies were excluded because the full text was not available, 4 studies did not focus on children under 18 years old, 25 studies lacked empirical data, and 27 studies did not focus on the utilization of VR to promote healthy eating and PA from the perspective of the children themselves. Finally, a total of 25 studies met the criteria for further analysis in this systematic review. The selection process is illustrated in the PRISMA flow diagram (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Data collection process
Two independent reviewers systematically extracted data from each included study using a table. The following data were collected: study design, geography, sample size, sample age, study objectives, VR type, theoretical basis, design strategy, intervention method, measures, and outcomes. Outcome variables included PA and healthy eating, as well as secondary outcomes such as self-efficacy, immersion, preference, motivation, nutrition knowledge acquisition, and heart rate (HR). Other variables collected included sample characteristics and intervention characteristics (VR type, duration, device used). Missing information was recorded, and the available data were used for analysis.
Risk of bias tools
For the quality assessment of the included studies, the Cochrane Risk of Bias 2 Tool (RoB 2) was used for randomized studies, and the Risk of Bias in Nonrandomized Studies of Interventions Tool (ROBINS-I) was used for nonrandomized studies and one-group pretest‒posttest studies. 22
The quality assessment in RoB 2 comprised five characteristics: (1) randomization process; (2) deviations from the intended interventions; (3) outcome data; (4) measurement of the outcome; (5) selection of the reported result. Conversely, the ROBINS-I evaluated seven domains for nonrandomized studies: (1) confounding factors; (2) selection of participants into the study; (3) classification of interventions; (4) deviations from intended interventions; (5) handling of missing data; (6) measurement of outcomes; (7) selection of the reported result. Two reviewers independently assessed each study's risk of bias, with a third researcher resolving any disagreements.
Results
Risks of bias of included studies
Among the 25 articles reviewed, there were 9 randomized studies,11,23–30 9 nonrandomized studies,31–39 and 7 one-group pretest‒posttest studies.40–46 In the randomized studies, two articles included two studies each, we treat them as individual studies for the purposes of our analysis and risk of bias assessment.27,30 Therefore, although there are 25 articles included in the review, the total number of studies assessed is 27. This includes 11 randomized studies (from 9 articles), 9 nonrandomized studies, and 7 one-group pretest–posttest studies.
The risk of bias assessment using RoB 2 categorized the randomized studies into “low risk,” “some concerns,” and “high risk.” Among the assessment results of 11 randomized studies, four were rated as “low risk,” six as “some concerns,” and one as “high risk” due to significant regional differences between the groups 25 (Table 1). For the ROBINS-I assessment, studies were classified as having “low,” “moderate,” “serious,” “critical,” or “no information” risk of bias. None of the studies were rated as “critical,” and only one study was rated “no information” because of a lack of description of measurements and outcome data 31 (Table 2).
Risk of bias of randomized studies (RoB 2).

* Low risk, ** Some concerns, *** High risk.
Risk of bias of non-randomized studies (ROBINS-I).

* Low, ** Moderate, *** Serious, ***** No information.
General findings of the included studies
Characteristics of the included studies
All the included articles were published between 2013 and 2023. One to three studies on VR for promoting children's healthy eating and PA were published annually. These studies were distributed across the Americas,11,23,25,28,29,32,35,37,39,42,46 Europe,24,26,27,30,31,34,43,44 and Asia33,36,38,45; however, there was a higher concentration of studies from the Americas and Europe compared to Asia.
Participants in the included studies ranged from 4 to 15 years old. The majority of studies (n = 23) focused on children aged 7–15 years,11,23–32,34–41,43–46 while two studies included younger participants aged 4–10 years.33,42 With respect to sample size, ten studies had sample sizes greater than 100,23,27,30–32,35,36,39,40,43 with the largest sample size being 404 participants. 35 Thirteen studies analyzed sample sizes between 20 and 100.11,24–26,28,29,33,37,38,41,44–46 Only two studies had smaller sample sizes of 11 34 and 15. 42 Studies with larger sample sizes may have increased statistical power compared to those with smaller samples (Table 3).
Results of general characteristics of included studies.
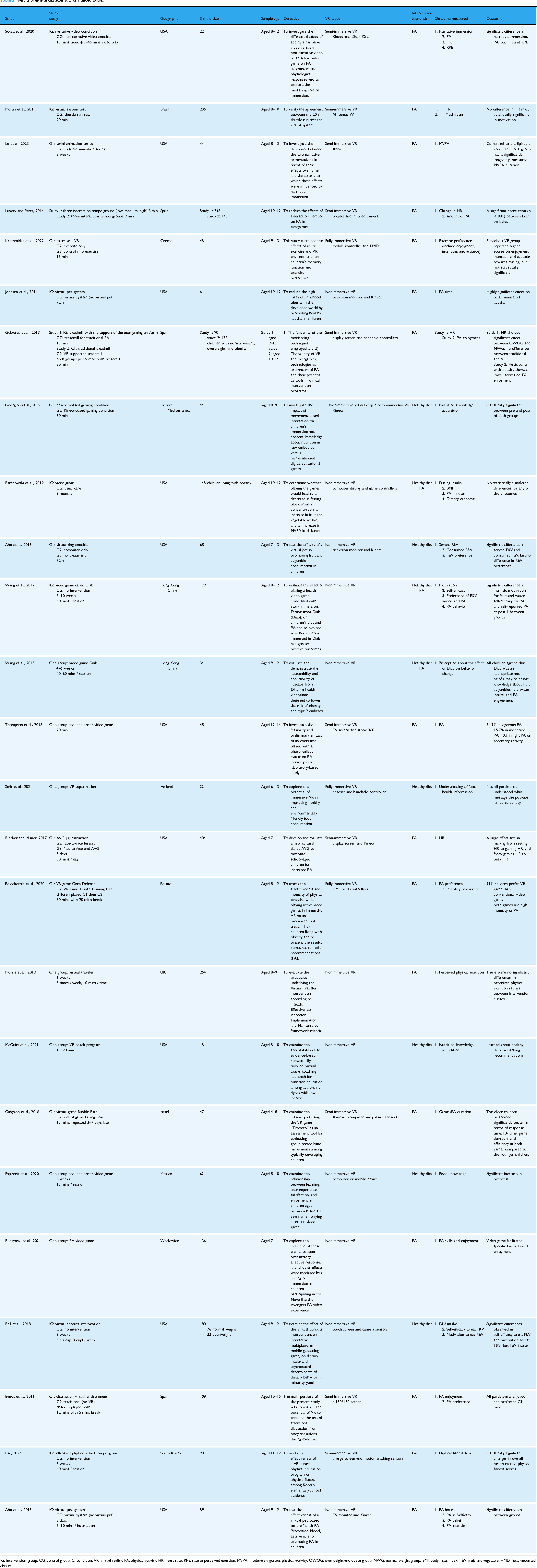
IG: intervention group; CG: control group; C: condition; VR: virtual reality; PA: physical activity; HR: heart rate; RPE: rate of perceived exertion; MVPA: moderate-vigorous physical activity; OWOG: overweight and obese group; NWG: normal weight group; BMI: body mass index; F&V: fruit and vegetable; HMD: head-mounted display.
Intervention approaches and VR types (RO1)
Consistent with our review scope, the two main ways to promote HBs are: (1) promoting a healthy diet by reducing the intake of unhealthy foods, while increasing the intake of healthy foods such as F&V; and (2) increasing PA while reducing sedentary behavior. Out of the 25 included studies, 16 focused on increasing children's PA.25–31,33–35,37–40,43,46 Six studies aimed to improve children's diets and increase their awareness of healthy eating.11,24,32,41,42,44 Three studies addressed both approaches.23,36,45
Regarding the types of VR used, the majority of studies utilized nonimmersive VR (n = 12)11,23–25,32,36,37,40–43,45 and semi-immersive VR (n = 11).24,27–31,33,35,38,39,46 One study compared both nonimmersive and semi-immersive VR. 24 Only three studies employed fully immersive VR,26,34,44 all of which were published after 2020 (Table 3).
Main findings of the included studies
Theories applied in using VR to promote childhood HB (RO2)
Among the included studies, 13 explicitly mentioned their theoretical frameworks, with some applying multiple theories.11,23–25,31,32,34,36,37,42,44–46 The most commonly used theories were Social Cognitive Theory (SCT) (n = 7)11,25,32,34,36,37,45 and Self-Determination Theory (SDT) (n = 6).23,32,36,42,45,46 Other theories included the Elaboration Likelihood Model (n = 2),23,44 Narrative Transportation Theory (n = 1), 23 Embedded Cognition Theory (n = 1), 24 and Attention Allocation Theory (n = 2)31,34 (Table 4).
Theoretical frameworks or models that guided the development of VR interventions.

VR: virtual reality.
VR design strategies for promoting HB and attitude change in children (RO3)
Design strategies are practical implementations of theoretical frameworks within the VR interventions to promote HB and attitude changes. Based on the descriptions in the included studies, design strategies can be categorized into five themes (Table 5). First, most of the studies included virtual participants, which could be customizable virtual avatars representing oneself35,36,41,46 or responders11,25,33,37 and guides who intervened in the participants’ HB.39,41 The next two most commonly used strategies are goal setting and progress tracking,11,23,25,32,35–37,41,42,45 and immersive storytelling.23,24,28,29,36,40,41,45,46 Five studies specifically mentioned the setting of immersive scenes in VEs.26,31,34,36,38 Finally, some individual design strategies have been combined and summarized as other interactive strategies, including pop-up design,30,44 peer feedback, time pressure, and game guidance. 24
Design strategies utilized in VR.

F&V: fruit and vegetable; VR: virtual reality.
Effectiveness of VR in promoting healthy dietary habits and PA
Among the studies focusing on VR to enhance children's PA, eight studies reported increases in PA time following VR intervention.25,27–29,34,37,38,46 For instance, one study indicated that children in the VR condition engaged in an average of 537 min of PA compared to 352 min in the control condition. 25 Another study noted age-related differences, with older children participating for longer durations. 33 Four studies measured children's HR as an indicator of exercise intensity,27,30,35,39 with one reporting a significant increase in HR under VR conditions. 35 In addition to objective measures, several studies have measured their affective responses using the Feeling Scale and found that children enjoy doing PA in VEs and perceived it as beneficial, suggesting that VR may foster positive attitudes and preferences, supporting longer-lasting engagement26,31,40 (Table 3).
Among the studies aiming to improve children's dietary habits, none measured BMI changes pre and post interventions, again highlighting the focus on more immediate behavioral outcomes rather than long-term anthropometric or behavior changes. Three studies reported an increase in children's motivation to consume F&V,11,32,45 but only one study observed an actual increase in F&V consumption. 11 Additionally, three studies found that VR intervention enhanced children's knowledge of healthy diets41,42,44 (Table 3). These findings suggest that VR interventions can have short-term effects on dietary behavior and knowledge acquisition, although the included interventions do not typically track long-term measures.
Discussion
Discussion of the RO2 and RO3 findings
First, the review focuses on the theories contributing to VR interventions. The basis for examining the effectiveness of VR interventions lies in the theoretical framework that guides them. SCT and SDT are widely used in research on children's HB.25,32,34,42,45 Children can access information to change attitudes and behavior from a variety of sources, which include themselves and their social environment.11,25 When the environment meets their intrinsic needs, behavior is likely to change.23,46 In this context, self-efficacy is crucial in both theories. Notably, these widely adopted frameworks are not unique to digital health interventions; rather, VR applications appear to build on traditional behavioral principles rather than introduce new theories specifically for immersive environments. This suggests that the novelty of VR technology in intervening in HB lies in the medium and the degree of experience, rather than redefining the theoretical basis for HB change.47,48 Based on the positive results of the above studies, it can be concluded that the two theories of SCT and SDT can be used as a guiding basis for research on VR interventions in children's behavior, providing a holistic perspective for planning the design of studies, implementation, and interpretation and analysis of research results.
Next, the design strategies used in VR interventions are analyzed, along with their potential benefits for promoting healthy dietary habits and PA. In general, design strategies are mostly implemented and adopted on the basis of the guidance of theory. Their main purpose is to increase children's engagement in the VR environment and influence their HB through appropriate stimulation. Although these strategies are grounded in established theoretical frameworks and are not exclusive to VR, the unique features of VR—such as immersion, VE, convenience, and high interactivity—provide a better platform for implementing these strategies. VR also offers opportunities for innovation, such as the introduction of virtual avatars, enabling these interventions to be more engaging and impactful. The effectiveness of VR interventions is often attributed to the collaborative integration of multiple design strategies informed by theoretical frameworks. The diversity and adaptability of these strategies are critical to ensuring the success of the intervention and promoting the development of healthy habits in children. For instance, integrating goal-setting strategies based on SCT into a VR system allows children to plan their daily diet and PA, enhancing self-efficacy through positive feedback.11,45 In addition, the overlapping effects between different design strategies are also significant. 24 Strategies such as pop-ups and goal tracking,30,41,44 which primarily provide feedback and support, have similar effects on children's perceptions of VR environments, although they are used in different studies.
However, not all design strategies have a positive impact. Improper strategy use may lead to adverse effects. For example, time-limited tasks may reduce engagement and increase stress. 24 Additionally, incorporating too many strategies and stimuli can overwhelm children, deviating from the intervention's purpose. Indeed, there is concern that VR may produce adverse psychological effects, such as anxiety or decreased motivation, especially when children are exposed to overly complex and stimulating VR games without adequate supervision. 49 To avoid these negative experiences caused by VR, some studies have improved by assessing participants’ enjoyment and preferences in VR.26,30,36 However, there are currently no guidelines to systematically assess participants’ experience, as few studies have used standardized measures or conducted long-term follow-up to evaluate the experience of VR-based health interventions.50,51 Future studies should also implement rigorous qualitative and quantitative methods to assess children's experience, preferences, and barriers to use in VR, whenever possible. This will help reduce the potential psychological burden and risks for children.
Effectiveness of VR in promoting healthy dietary habits and PA among children (RO4)
As the digital age progresses, VR is increasingly integrated into health and education. Since 2013, studies on VR promoting healthy dietary habits and PA among children have increased. On the basis of these analyses, VR has the potential to be an effective tool for promoting HB among children. 45 Compared with no intervention or traditional intervention (e.g., treadmill running and face-to-face lessons), VR has shown significant potential in increasing PA time, intensity, and healthy food consumption.11,25 In addition, studies have also measured the impact of VR by evaluating mediating factors such as psychological and cognitive changes. For example, studies by Wang et al. and Bell et al. showed that VR interventions could significantly improve children's motivation for F&V intake and self-efficacy for PA.32,36 Other studies have assessed participants’ enjoyment of exercise,26,31 which may be an important factor in promoting long-term adherence to exercise. These psychological factors such as changes in motivation, enjoyment, and self-efficacy can serve as an important supplement to changes in health behaviors, thereby more comprehensively evaluating the overall impact of VR on children's health behaviors.
Most children preferred exercising in the VE and liked combining VR with PA. 29 Children in the treatment group increased their PA by 60% compared to the control group. Some studies have shown that there is no significant difference in treatment effect between VR interventions and traditional interventions; however, VR interventions resulted in a significant increase in HR from before to after treatment, indicating higher engagement or exertion levels.35,39 This finding shows that VR interventions can be used as alternatives to traditional interventions since they can help improve children's motivation to persist in PAs, control the experimental space, and save experimental resources to a certain extent. In terms of VR improving children's healthy diet, research has shown that children under the virtual pet condition also consume more F&V than those under the computer condition alone.
Studies comparing different types of VR interventions provide additional insights. For example, Georgiou et al. 24 studied the difference between nonimmersive VR and semi-immersive VR in children's acquisition of nutritional knowledge. The results revealed no significant difference in knowledge scores between the two interventions, but children perceived nonimmersive VR games as more user-friendly. This finding suggests that while more immersive VR may provide greater engagement and realism, it is not always feasible or necessary when nonimmersive or semi-immersive interventions can achieve similar outcomes. In addition, practical challenges such as expensive equipment, spatial constraints, and the discomfort or motion sickness some users experience when using HMDs often result in it being underutilized. 52 Nonetheless, fully immersive VR has the potential to enhance motivational and behavioral outcomes, particularly for interventions with high levels of interactivity and immersion. 53 Another study revealed that, compared with video games without narrative elements, video games with narrative elements could increase children's moderate-vigorous PA time without causing negative feelings such as fatigue. 29 Compared with the episode narrative, the suspension in the serial narrative increased children's interest and motivation. Although the episode narrative initially attracted children's attention, it lacked sustainability in promoting PA. 28 This means that VR is not inherently superior due to its immersive qualities; rather, the success of the intervention depends on the careful integration of design elements that work with children's preferences and environments.
While VR-based interventions have great potential for promoting HB in children, their use is also problematic and controversial, particularly when applied in nonclinical settings such as home or school.54,55 For example, there are concerns about prolonged screen time, the potential for motion sickness or fatigue. These risks may be magnified in immersive environments, as children are highly engaged and may lose track of time.56,57 Research should consider these wider impacts, using rigorous methods to track children's experience, comfort, and continued interest, and ensure that VR use is both appropriate and responsible.
Overall, VR interventions are effective in influencing children's attitudes toward healthy eating and PA and have great potential to change children's HB. Well-designed VR systems increase children's satisfaction and engagement, meaning that children may stay engaged in the intervention longer. Through long-term intervention, there is greater hope for promoting healthy dietary habits and PA to promote child health.
Gaps and future research recommendations (RO5)
Most studies have a short-term duration. While one study lasted more than three months, most studies lasted 3–5 weeks or involved single interventions of up to 30 min. In some theory-based studies, such as those utilizing SDT emphasize that intrinsic motivation can cause long-term behavioral changes. However, owing to the limited research duration, this long-term effect has not been well verified. While short-term improvements in PA and dietary preferences were observed, these findings do not necessarily translate to lasting habit formation or measurable physical changes. Longitudinal studies spanning a longer period are critical to determine whether VR-induced behavioral changes persist. Future research should prioritize extended follow-ups to evaluate sustainability and health impact. Small sample sizes also reduce the generalizability of the findings. Furthermore, only one of the included studies compared the effects of different levels of VR immersion.
24
Different types of VR may have unique advantages. For example, nonimmersive and semi-immersive VR may be more accessible and cost-effective, while fully immersive VR may provide a higher level of engagement or realism. By comparing, researchers can better determine which features are most effective in promoting PA and healthy eating behaviors in children. Besides, the included studies used a variety of study designs, ranging from randomized controlled trials11,23–30 to nonrandomized31–39 and single-group pre- and posttest studies.40–46 The limited number of rigorously controlled trials weakens the ability to judge the causal effectiveness of VR interventions. In the absence of adequate randomization, appropriate control groups, and long-term follow-up, it is difficult to conclude that the observed changes in diet and PA can be directly attributed to the VR intervention. On the basis of the results of this review, some recommendations are formed that may be helpful for future research and practical applications:
Conduct long-term studies with larger sample sizes to investigate the long-term impact of VR interventions on childhood HB. Research can focus on comparing and evaluating different types of VR interventions to determine their respective advantages and optimal use contexts. Conduct more randomized controlled trials to rigorously test the effectiveness of VR interventions in addressing healthy dietary habits and PA. Future research should also use rigorous qualitative and quantitative research methods as much as possible to conduct in-depth analysis of children's experience and potential usage problems in VR.
Limitations
Although this systematic review provides useful insights into VR interventions in promoting healthy eating habits and PA in children, the following limitations must be acknowledged. First, only one study demonstrated that an intervention developed in the United States was applicable to children in Hong Kong, China, 45 and most studies did not significantly differ in socioeconomic status among participants11,28,29,32,36 or did not consider it as a major factor. 35 This lack of information makes it difficult to assess how socioeconomic and cultural factors might influence intervention effectiveness and thus limits the generalizability of the findings to more heterogeneous populations or underresourced settings. In particular, the impact of these factors may vary significantly across different socioeconomic statuses and cultural contexts, affecting the potential success of VR-based health interventions. Second, the included studies showed significant heterogeneity in terms of intervention content, duration, measurement indicators, and VR type, which increased the difficulty of summarizing and comparing the results of the studies, thereby limiting the ability to clearly define best practices for VR interventions. Finally, this review only included studies published in English, which may introduce publication bias and exclude relevant studies in other languages or unpublished data. This may lead to a biased understanding of the existing evidence. 58 Overall, by identifying these limitations, we provide a more cautious perspective for the interpretation of research findings and propose directions for future research.
Conclusion
This systematic review demonstrates the potential of VR in promoting healthy dietary habits and PA among children to promote health. From 25 studies published between 2013 and 2023, key theoretical models such as SCT and SDT were identified, with self-efficacy playing a central role in driving behavior change. Effective integration of design strategies is crucial in engaging children and influencing their behaviors. The included studies showed the effectiveness of VR interventions in increasing children's PA time and intensity, as well as improving healthy food consumption and nutritional knowledge acquisition. While VR interventions show promise, they are constrained by short study durations, small sample sizes, and the use of a single VR type without comparison. Future research should address these gaps by conducting long-term studies to assess the sustainability of HB changes, implementing rigorous randomized controlled trials to establish stronger causal relationships, and exploring comparisons between different VR types to identify their unique advantages and optimize intervention strategies. These insights will aid in the development of more effective VR interventions, contributing to future child health strategies aimed at promoting sustainable HB.
Supplemental Material
sj-xlsm-1-dhj-10.1177_20552076251331794 - Supplemental material for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review
Supplemental material, sj-xlsm-1-dhj-10.1177_20552076251331794 for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review by Yuqi Zhang, Amirrudin Kamsin, Nur Amani Natasha Ahmad Tajuddin and Siti Idayu Hasan in DIGITAL HEALTH
Supplemental Material
sj-xlsm-2-dhj-10.1177_20552076251331794 - Supplemental material for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review
Supplemental material, sj-xlsm-2-dhj-10.1177_20552076251331794 for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review by Yuqi Zhang, Amirrudin Kamsin, Nur Amani Natasha Ahmad Tajuddin and Siti Idayu Hasan in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251331794 - Supplemental material for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review
Supplemental material, sj-docx-3-dhj-10.1177_20552076251331794 for Effectiveness of virtual reality interventions in promoting healthy eating and physical activity among children: A systematic review by Yuqi Zhang, Amirrudin Kamsin, Nur Amani Natasha Ahmad Tajuddin and Siti Idayu Hasan in DIGITAL HEALTH
Footnotes
Acknowledgments:
This research was financially supported by the Ministry of Higher Education through the Fundamental Research Grant Scheme (FRGS/1/2022/SSI07/UM/02/21), with Grant ID Number FP051-2022. We thank the editor and anonymous reviewers for their insightful comments and suggestions that helped us improve the manuscript.
Guarantor
AK
Ethical considerations
Ethical approval was not required for this systematic review as it involved analysis of published literature.
Author contributions/CRediT
Yuqi Zhang, Nur Amani Natasha Bt Ahmad Tajuddin, and Amirrudin Kamsin conceived the study. Siti Idayu Hasan, Nur Amani Natasha Bt Ahmad Tajuddin, and Yuqi Zhang reviewed and performed quality assessment. Yuqi Zhang wrote the first draft of the manuscript. All authors reviewed and revised the manuscript and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education Malaysia (grant number FRGS/1/2022/SSI07/UM/02/21, with Grant ID Number FP051-2022).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.