
Abstract
Background
The journey of any new treatment begins in the lab and through a clinical trial. Clinical trials have become an important means to promote public health causes. In digital age, e-health usage (EHU) might be a key factor to promote clinical trials. However, how consideration for clinical trial participation is impacted by EHU remains unclear.
Method
Secondary analyses were conducted on data from the Health Information National Trends Survey 2020 (HINTS 5, Cycle 4). This study proposed and tested a serial mediation model linking EHU to consideration for clinical trial participation, mediated by patient-centered communication (PCC) and cancer-related self-efficacy (CS). Analysis was performed using a sample survey targeted at individuals with chronic disease and/or family cancer history, conducted in 2020 in the United States (N = 3292).
Result
This study found that EHU exerted positive effects on clinical trial participation directly. Furthermore, their relationship can be mediated by PCC and CS. Only when PCC serves as the first mediator did CS exert the serial meditation effect. Annual household income significantly moderates the path from CS to consideration for clinical trial participation. For low-income groups, an increase in CS significantly expends their consideration for clinical trial participation.
Conclusion
EHU can improve PCC and CS. This can be considered as motivators for increasing participation to clinical trials. Based on the finding, information related clinical trials should be promoted through e-health channels and the information should gain better patients’ understanding. Those findings throw out suggestions on building trust, addressing concerns and alleviating fears to clinical trial participation.
Keywords
Introduction
Clinical trials are the cornerstone of clinical research and the key to discovering new treatments and improving health outcomes. 1 The journey of any life-changing treatment begins in the lab and through a clinical trial. 2 Clinical trials have important impacts on many diseases, especially “cancer” and “chronic diseases.” For “cancer,” clinical trials drive advancements in precision medicine, immunotherapy, and targeted treatments that significantly improve survival rates and quality of life. 3 For “chronic diseases,” clinical trials explore innovative interventions to manage symptoms, prevent progression, and enhance long-term health outcomes, addressing the growing global burden of these conditions. 4 The National Comprehensive Cancer Network maintains that clinical trials provide some of the best treatment options to eligible patients. Ensuring equitable access to and participation in clinical trials is crucial for improving health outcome disparities, particularly among members of racial and ethnic minority groups. 5 In this study, consideration for clinical trial participation (CCTP), defined as the process of thinking carefully before potential participants decide to join a clinical trial, is key to improving the outcome of clinical trial enrollment and promoting public health. 6 Individuals who contribute to the clinical trial help to address an unmet medical need, ensure the safety and efficacy of the new treatment and promote the development of cutting-edge medical technologies for protecting public health. 7 The success of a clinical trial depends largely on keeping the number of participators recruited into the study to a maximum and the number of participants dropping out to a minimum. The increase inadequate numbers of participations lead to clinical trials fail, 8 resulting in wasted resources, missed opportunities for scientific progress, and reduced public trust. Therefore, improving public participation willingness of clinical trials has become an important challenge.
In the digital era, e-health usage (EHU) plays an increasingly role in shaping individual's health decision-makings, including clinical trial. EHU refers to the use behavior of information and communication technologies (ICT) in support of health and health-related fields, 9 such as health services and information delivered or enhanced through the Internet and related technologies. 10 It encompasses multiple interventions, including tele-health, telemedicine, mobile health (M-Health), electronic medical or health records. 11 In the past, doctors, hospitals, and specialized mass media were regarded by patients as the primary source of medical information. Nowadays, with the popularization of digital devices such as computers and smartphones, higher accessibility of digital health information has created a new way for patients to better understand their own health.12,13 It has revolutionized the way people search for health information, transformed health behavior, and impacted the delivery of health care.
Related study found that e-health use (i.e. using e-devices for health purposes) is linked to improved health outcomes, including active participation in healthcare. 14 EHU has the potential to enhance clinical trial participation. For instance, higher levels of EHU lead to better understanding of clinical trials. It subsequently increased likelihood of clinical trial participation. 1 Meanwhile, previous studies point out that the barriers to clinical trial participation are mainly related to protocols, patients, or doctors. The main reasons include: lack of clinical trials knowledge; 15 worries about the medical environment; dislike for randomized trials; complexity and stringency of protocols; potential side effects; fear that the participation would negatively affect their relationship with doctors; the doctor's attitude toward the trial.16,17 However, it still remains unclear how consideration for clinical trial participation is impacted by EHU. In detail, are there mediating factors impact their relationship, or how consideration for clinical trial participation could be positively changed? To figure out the impact mechanism, this study examined how EHU is associated with consideration for clinical trial participation. It proposed and tested a serial mediation model linking EHU to consideration for clinical trial participation, mediated by patient-centered communication (PCC) and cancer-related self-efficacy (CS).
Hypothesis
Previous literature has established a direct association between e-health and clinical trial. 18 In recent years, sponsors, investigators, research organizations, as well as academics have increasingly recognized the importance of e-health technologies in revolutionizing clinical trials and enhancing participant and patient engagement. 19 The term “M-Health” was mentioned in 185 clinical studies that were posted to clinicaltrials.gov between 2013 and 2015. Since 2016, the number of studies has more than doubled to 371. 19 It is expected to increase given the steady development of related technologies in these areas as highlighted above. These tools or services including mobile devices as well as apps can support clinical trials in myriad number of ways. 20 For example, patients with difficult may selectively pay attention to e-health service that can alleviate health problems (such as looking for new therapies and new drugs). Meanwhile, they may selectively understand the value and significance of participating in clinical medical trials and make positive responses to them. As a research shows the use of mobile phone-based interventions in cardiovascular disease had an added benefit during COVID-19 pandemic as participants could be monitored safely from home. 20
PCC may play as potential mediator linking e-health use and clinical trial. PCC is defined as inviting and encouraging patients and their families to actively participate in and negotiate all decisions about their health care needs, treating patients with dignity and respect. 21 It enables both doctors and patients to effectively express their needs and requirements for medical activities. In this process, patients no longer passively accept medical treatment and nursing, but more focus on “the right to know.” Research on human-to-human transmission has shown that the quality of doctor–patient interaction negatively affects clinical trial participation. It shows an asymmetry between clinical diagnosis and information obtained by patients outside the clinical setting. 22 The asymmetry may damage the doctor–patient relationship and decreasing willingness to participate in clinical trials. However, more studies showed conflicting results. For instance, an empirical study 12 pointed out that the interaction and communication between patients and doctors can give full play to patients’ initiative and change their knowledge, beliefs, and behaviors about health. Particularly, PCC strengthens patients’ trust in doctors and leads them to cooperate more actively with the doctors.1,23,24 Moreover, patient–doctor relationship can be improved, resulting from EHU. For instance, internet use for health information increases the frequency of health professional contact. Patients who got health information were more likely to seek health information from health professionals and to visit them for disease treatment. 25
In addition, CS, defined as the individual's confidence or capability to execute behaviors necessary to produce specific achievement (e.g. acquiring cancer-related advice or information, managing the problems caused by cancer or related treatment.).26–28 It can be influenced by previous positive or negative experience, physiological arousal, emotional state, and persuasion.28–31 For instance, e-health provides a convenient way of health information communication with its interactive media forms; 32 PCC characterized by mutual persuasion, 33 also has potential to improve CS. From this perspective, CS could potentially be the second mediator. Promoting the EHU could incorporate strategies to improve PCC and CS. The importance of EHU and PCC should be emphasized. Especially in the context of clinical trials, the information from e-health and doctors may intend to shape, reinforce, or change patients’ attitudes towards a new therapy, then help them to make a rational decision. E-health information provides clear explanations, which can increase patient knowledge and shared understanding, then motivate patients to follow through with treatment recommendations. PCC plays a direct role in popularizing health knowledge, improving health awareness, changing health attitudes and behaviors, and carrying out health interventions. 34 It improves patients’ confidence in clinical trial participation. Therefore, by EHU and PCC, individuals achieve improvement of CS. They are more involved in medical treatment plans and related clinical trials. 35
Based on the existing evidence, the following direct and indirect relationships between EHU and consideration for clinical trial participation were proposed:
H1: EHU lead to further CCTP, mediated by PCC.
H2: EHU lead to further CCTP, mediated by CS.
H3: EHU lead to further CCTP, mediated by PCC and CS.
H4: EHU lead to further CCTP.
Based on social stratification theory, socioeconomic status (SES) influences individuals’ health decision-making behaviors through the unequal distribution of resources and opportunities. Annual household income (AHI) is one of the core indicators of SES and significantly impacts individuals’ behaviors, cognition, and decision-making processes. 36 Research has shown that individuals with an AHI of $40,000 or below are less willing to participate in clinical trials compared to those with an AHI between $40,000 and $80,000. 36 Therefore, this study will also examine the moderating effect of household annual income within the chain mediation model. The research question is as follows:
Q: How AHI influence individual's consideration for clinical trial participation?
Methods
Study design and sampling
Data analyzed in this study was drawn from National Cancer Institute's Health Information National Trends Survey in 2020 (HINTS 5, Cycle 4). It is a nationwide survey. For Cycle 4, the topics of special interest focused on clinical trials. Specific content included: knowledge about clinical trials, sources and trust in information about clinical trials, willingness to participate in clinical trials, history of clinical trial participation for cancer. The survey design and sampling procedures for HINTS have been explicated extensively in previous studies 37 and this study is a secondary analysis of the HINTS data. It was conducted from 24 February to 15 June 2020. There were 3865 completed responses with a response rate of 36.7%. Missing data was dealt with listwise deletion. Given there is a clear understanding of the importance of clinical trials for specific diseases, this study further selects individuals with a family history of cancer and/or chronic diseases as the research sample. In order to screen the sample, respondents were asked to report: have any of their first-degree or second-degree biological relatives (parents, brothers and sisters, children, grandparents, aunts and uncles, and nieces and nephews) ever had cancer? Has a doctor or other health professional ever told them that they had any of the following medical conditions: (1) Diabetes or high blood sugar? (2) High blood pressure or hypertension? (3) A heart condition such as heart attack, angina, or congestive heart failure? (4) Chronic lung disease, asthma, emphysema, or chronic bronchitis? Responses (0 = “no”, 1 = “yes”) were used for analysis, with 0 indicating that they did not have any family history of cancer and/or chronic diseases. The final sample is 3292. With stratified random sampling, it sampled noninstitutionalized, U.S. citizens aged from 18 to 104 years old (Mean = 58.42). 40.89% respondents were male and 59.11% respondents were female.
Ethical consideration
Secondary data was used in this study. Data from HINTS meet strict ethical standards and have been approved by the ethics committee. All participants provided informed consent, and all methods were carried out according to relevant guidelines and regulations.
Measurement
EHU was measured with four items, which is similar to measurement in previous studies.38,39 Respondents were asked whether in the past 12 months, they used electronic means to (1) search for health or medical information; (2) contact a doctor or a doctor office; (3) access to medical test results; (4) schedule an appointment with a healthcare service. Responses (0 = “no”, 1 = “yes”) were summed together for analysis, with 0 indicating that they did not use any electronic means to acquire health information, and 4 indicating that they used electronic means in these four conditions.
PCC was accessed by seven items. The same measurement was applied in studies related to cancer survivors’ experience, e-health information exchange patterns.40–42 Respondents were asked to report during the past 12 months, how often did their doctors, nurses, or other health professionals (1) give them the chance to ask all the health-related questions they had; (2) give the attention they needed to their feelings and emotions; (3) involve them in decisions about their health care as much as they wanted; (4) make sure they understood the things they needed to do to take care of their health; (5) explain things in a way they could understand; (6) spend enough time with them; (7) help them deal with feelings of uncertainty about their health or health care. The answer to each question was categorized by 4 scores (1 = “never” to 4 = “always”). The higher score represented higher level of PCC.
CCTP constructed based on previous literature6,43 was measured by eight items. Participants were asked to evaluate how clinical trial participation will be considered by them with the questions: if they had a health issue and they were invited to participate in a clinical trial for that issue; how much their decision to participate in the clinical trials will be influenced? Eight items were used for evaluating: (1) they would be helping other people by participating; (2) they would get paid to participate; (3) they would get support to participate such as transportation, childcare, or paid time off from work; (4) if their doctor encouraged them to participate; (5) if their family and friends encouraged them to participate; (6) they would want to get better; (7) they would get the chance to try a new kind of care; (8) if the standard care was not covered by their insurance. Each item was answered on 4 scores (1 = “not at all” to 4 = “a lot”). The higher score represented higher level of willing for clinical trials participation.
CS was used to test the individual perceptions of physician communicative behaviors. It composed of one single item, similar to previous studies.26,28 Respondents were asked to report how confident are they that they could get advice or information about cancer if they needed it? A 5-point Likert scale was used (1 = “not confident at all” to 5 = “completely confident”). The higher score indicated higher level of CS.
AHI was measured by the following question: “Thinking about members of your family living in this household, what is their combined AHI, meaning the total pretax income from all sources earned in the past?” The answers of respondents were code as: 1 = Less than $20,000, 2 = $20,000 to < $35,000, 3 = $35,000 to < $50,000, 4 = $50,000 to < $75,000, 5 = $75,000 or more.
Furthermore, demographic variables were used as controls to reduce confounding effects. Demographic variables included age, gender, education, and race. Respondents were asked to answer what is their age? On their original birth certificate, were they listed as male or female? What is the highest grade or level of schooling they completed? (1 = “less than high school” 2 = “high school graduate” 3 = “some college” 4 = “college graduate or more”). What is their race? (0 = “no-white,” 1 = “yes”).
P-value and effect size measures
P < .05 for statistical acknowledgment. p < .05, in this study, is regarded as a prescreen, passing which allows to analyze the types and the sizes of the estimated effects. Therefore, this study refers to p = .05 as “statistically acknowledged” instead of “statistically significant.”44–46
Percentage coefficient (bp), a regression coefficient, is calculated when both independent and dependent variables are on 0–1 percentage scale (ps). Equation (1) can be used to transform variables that are not on a percentage scale into ones that are. Here, sp is percentage score after transformation, sos is original score, scx is conceptual maximum on the original scale, and scn is conceptual minimum on the original scale.
46

Descriptions of key variables (n = 3292).

Data analysis
The serial mediation model was tested using SPSS. 47 First, a common measurement scale of 0 to 1 was used for all focal variables to allow comparison. To compare and explain the effect size of all pathways in this model, this study adopts percentage coefficients (bp), a min–max scaling normalization to rescales all coefficients from the original interval (e.g. 5-Likert scale (1, 5)) to the interval (0, 1)).48,49 Second, in this analysis, EHU was entered as the independent variable, CCTP as the dependent variable, PCC as the first mediator, CS as the second mediator. Chronic disease, age, gender, education, race, and AHI were included as covariates in the model. See Figure 1 for a representation of the proposed model.

The mediation effect of patient-centered communication and cancer-related self-efficacy on the relationship between e-health usage and consideration for clinical trial participation.
Results
Preliminary analyses
Descriptive statistics for the main variables (in original scales and the 0-1 percentage scales) were shown in Table 2, including EHU (M = 2.13, SD = 1.46), PCC (M = 3.42, SD = 0.64, Cronbach's α = 0.93), CS (M = 3.89, SD = 0.97) and Consideration for Clinical Trial Participation (M = 2.81, SD = 0.726, Cronbach's alpha = 0.84) The zero-order Pearson correlation among all the study variables are reported in Table 3. Here, most of the main variables were significantly correlated with each other.
Variable percentization (n = 3292).

CCTP: consideration for clinical trial participation; EHU: e-health usage; PCC: patient-centered communication; CS: cancer-related self-efficacy; AHI: annual household income.
See Table 1 and Figure 1 for variable abbreviations.
Demographic variables are displayed in Table 4. The average age was 57.42 (SD = 16.44), its missing values were substituted by Median 59. The statistics show that about 41% of participants were male. It shows that 44.68% of participants received a college degree or above. As for AHI, almost a half of participants had an AHI above 50,000 USD. In addition, about 77% of participants were white race.
Descriptive statistics (weighted) for control variables.

Zero-order Pearson correlations (N = 3292).
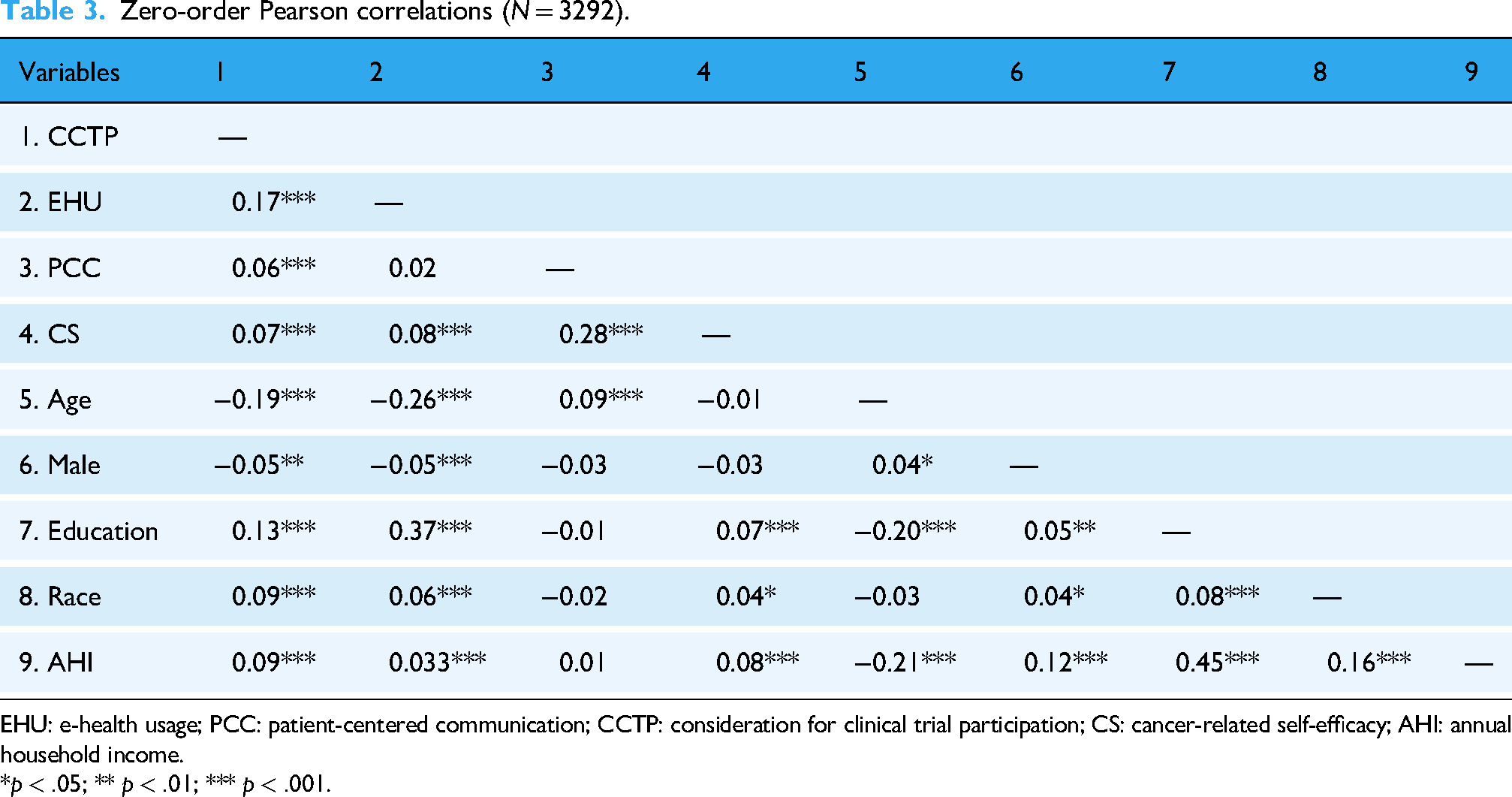
EHU: e-health usage; PCC: patient-centered communication; CCTP: consideration for clinical trial participation; CS: cancer-related self-efficacy; AHI: annual household income.
*
Demographic variables have impacts on the consideration of clinical trial participation. Consistent with previous studies,50–52 the correlation analysis revealed that, compared with white individuals, nonwhite individuals are less likely to consider participation in clinical trials; older persons are also less likely to be enrolled in clinical trials; Furthermore, individuals with lower levels of education and AHI are less likely to consider participation than others.
Hypothesis testing and addressing the research question
Hypothesis 1 predicted EHU would increase CCTP, mediated by PCC. As seen in Table 5, EHU had statistically acknowledged (aka. significant) positive relationships with PCC (
Summary of mediation and moderation effects.

EHU: e-health usage; PCC: patient-centered communication; CCTP: consideration for clinical trial participation; CS: cancer-related self-efficacy; AHI: annual household income.
b: Standardized beta; bp: percentage coefficients; CI stands for confidence interval.
*p < .05; **p < .01; ***p < .001.
Hypothesis 2 assumed that EHU would increase CCTP, mediated by CS. As seen in Table 5 and Figure 1, EHU was positively associated with CS, with a significant acknowledged 0-1 regression coefficient (
Hypothesis 3 assumed EHU would increase CCTP, mediated by PCC and CS. As shown in Table 5 and Figure 1, PCC had statistically acknowledged positive relationship with CS (
Hypothesis 4 assumed HEU would lead to further CCTP. As shown in Table 5 and Figure 1, EHU had statistically acknowledged positive relationship with CS (
This study raises a research question: how AHI influence individual's consideration for clinical trial participation? The research results indicate that AHI only moderates the relationship between CS and CCTP (

The moderation effect of annual household income on the relationship between cancer-related self-efficacy and consideration for clinical trial participation.
Effect size analysis
While reporting hypothesis-testing results, this study interpreted the effect size indicators. The following are some overall indicators that are highlighted and compared.
Percentage coefficient bp = 0.064 for the EHU → CCTP total effect indicates that a wholescale increase in EHU was associated with an increase in CCTP by nearly six and half percentage points, as the theoretical 100%. In the analysis of the parts and the process, the total effect estimation provided the baseline for the analysis of the mediation process. The total r2 for the two equations (II and VI) predicting CCTP, r2 = 0.256 and r2 = 0.246, suggest that many factors that may predict or influence CCTP have been excluded. These overall statistics place possible contribution of this study in perspective, which needs to be modest.
It is noted that the indirect effect (PCC, a1 × b1 path) contributed about2.5% of the EHU → PCC → CCTP total effect (p < .05; Figure 1); indirect effect (CS, a2 × b2 path) contributed only 0.94% (p > .05; Figure 1) of the EHU → CS → CCTP total effect; indirect effect (PCC and CS, a1 × b3 × b2 path) contributed 0.63% (p < .05; Figure 1) of the EHU → PCC → CS → CCTP total effect. Considering that PCC and CS are two factors that may mediate the EHU → CCTP relation, such a contribution by a single mediator may be considered significant substantively, but not just statistically. That the direct-and-remainder (d) path contributed 96.88% of the total effect calls for more work to identify the other mediators.
Of the mediated path, the a1 path contributed about 31.76% less than the b1 path in EHU → PCC → CCTP indirect effect; the a1 path contributed about 74.74% less than the b3, and 2.60% less than the b2 path in EHU → PCC → CS → CCTP indirect effect; the effect of a2 path was not statistically acknowledged. The multiplicative relationship between these paths implies that the different paths leverage each other. An indirect path is similar to a teamwork between two members; the member who contributes less leverages more.
Discussion
The current study has broken new grounds by exploring mediating roles of PCC and CS on the association between EHU and consideration for clinical trial participation. Detailed findings are discussed below.
First, there is a positive association between EHU and PCC. E-health technology constructs liberal communication space, which is filled with information redundancy and information noise. Patients thus tend to cross-verify the information from multiple dimensions after they use e-health. E-health tools such as mobile apps, patient portals, information repositories and online consultations, 53 which facilitate real-time interaction and collaboration between patients and healthcare providers. This increased access to information can facilitate PCC by enabling patients to ask informed questions and participate more meaningfully in discussions with healthcare providers. This highlights the potential importance of EHU in enhancing PCC.
Second, this study demonstrates that e-health is positively associated with consideration for clinical trial participation directly and indirectly. Echoing to previous findings, 54 e-health can promote individuals willing's to clinical trial. It is plausible that e-health enables real-world data collection outside of the traditional clinical context and allows more patient-centered approaches. More importantly, this study explores the underlying mechanism linking EHU and consideration for clinical trial participation. Doctor–patient communication and CS play serial mediating roles. E-health can enhance patients’ CS through PCC, and thus promote participation of U.S. adults in clinical trials. Traditional interpersonal interaction theory assumes that doctor–patient communication occurs at two aspects: content (i.e. transmission of information) 26 and relationship (i.e. how doctors and patients think about each other and establish relationships through interpersonal interaction).26,55 The result of this study adds to the emerging evidence that PCC plays a pivotal role in the successful implementation of improving CS and clinical trial participation. When individuals feel heard, respected, and well-informed, they are more likely to make a thoughtful decision about whether to participate in a clinical trial. However, PCC can facilitate better understanding, build better trust, address concerns, alleviate fears among individuals considering participation in clinical trials. By PCC, individuals further believe in their ability to navigate the complexities of clinical trials, understand the potential risks and benefits, and actively contribute to research efforts. They obtain higher CS, then they are more likely to view clinical trial participation as a meaningful and empowering opportunity to take control of their decision. Therefore, to improve the participation willingness of conical trials, medical institutions should place importance on improving CS by better PCC.
Third, socioeconomic variables, such as race, AHI and educational level, are critical factors influencing access to and skills for using ICT (e-health). The correlation results in this study are consistent with previous studies, the nonwhite race, and individuals with lower levels of education and AHI are less likely to consider participation than others. Furthermore, it is worth mentioning that AHI significantly moderates the path from CS to consideration for clinical trial participation, with the moderating effect showing income stratification differences: for low-income groups, an increase in CS significantly expend their consideration for clinical trial participate; whereas for high-income groups, the impact of increased self-efficacy on consideration to participate is less and exhibits a negative relationship.
This study has important practical implications. First, given the importance of e-health use behaviors to PCC and CCTP, it is necessary to provide more supportive e-health service, more instructive and accurate information. Educations campaigns aimed at improving patients’ e-health literacy is also important. For instance, authorized public service programs for medical literacy purposes can be produced; social benefits related to clinical trials and individual benefits of participating in clinical trials can be emphasized. Second, PCC should place importance on enhanced understanding and informed decision-making regarding clinical trial participation. It aims to build trust, then address concerns and alleviate fears related to clinical trial participation. Third, besides guiding the patients to high-quality e-health service, it is equally important to continuously improve the communication skills for both doctors and patients. Doctors are encouraged to express their empathy, give emotional support, and respect patients’ perspective of clinical trial participation. This can enhance individual's CS, which develop resilience in the face of challenges, positive expectations, and outcome anticipation in clinical trial participation. While individuals are also responsible to express their concerns, active discuss with doctors regarding the clinical trial participation decisions. It is possible that a combination of high-quality e-health service and productive PCC could exist to build a professional-guided participatory process before conducting clinical trials.
In addition, it is known that the underrepresentation of low-income groups in clinical trials is a pressing issue. Enhancing their willingness to participate in clinical research has long been a key concern for the international community. 56 This study reveals that when individuals have a stronger sense of CS, they are more likely to give further consideration for clinical trial participation. This conclusion aligns with findings from previous studies. 57 This finding has important implications for policymakers and promoters of e-health service: the complex effects of income disparities on individual behavior should be fully considered when designing e-health interventions. For low-income individuals, the focus should be on enhancing their CS, such as providing targeted health education and psychological support. For high-income individuals, more publicity strategies about clinical trials are needed to help them realize the scientific value and potential benefits of trials, so as to make more rational decisions.
Several limitations of this study should be noted. First, although HINTS used data from a nationally representative sample of 3865 U.S. adults, the data were collected through self-reported, cross-sectional surveys and based on limited questions in the questionnaire. Therefore, longitudinal studies in the future are called for. Second, due to the constraints of secondary data, the construction of variables is limited. Future studies should use more mature and validated scales to measure and examine the relationships between these variables. For instance, CS was assessed using a single-item measure. While it was used in previous studies, it may not fully capture the multidimensional and nuanced nature of self-efficacy, particularly in the context of cancer. Future research should consider employing multidimensional scales to better assess CS (e.g. its emotional, behavioral, and cognitive aspects). Third, there are likely other potential mechanisms linking EHU to clinical trial participation and were not fully explored in this study. The more advanced analytical approach, such as structural equation modeling (SEM) can offer the advantage of accounting for the dichotomous nature of variables and capturing the interplay among multiple pathways simultaneously. So it should be emphasized that future research should employ SEM or similar approaches to better understand these multifaceted relationships. In addition, the serial mediation model was conducted in an America context, which may not be applicable to all countries. To test its applicability, future research should further examine the model in other sociocultural contexts.
Conclusion
The less consideration for clinical trial participation has long been a challenge to many healthcare systems. The EHU may offer a communication channel to address this issue. The current study investigates how EHU can lead to further consideration for clinical trial participation. The findings stressed the importance of e-health and PCC. In order to improve clinical trial participation, information related clinical trials should be given extensive selective exposures and the information should gain better patients’ selective understanding. Moreover, PCC skills training should be strengthened to help medical care providers discuss the benefits and risks of clinical trials with patients in an effective way. This enables the patients to easily access available clinical trial information (e.g. through ClinicalTrials.gov), which can reduce the burden on patients. Understanding these can help the healthcare system better navigate and utilize the health information environment to improve the willingness of clinical trial participation, which is a key factor of successful clinical trials.
Footnotes
Contributors
Siying Gong conceptualized the study and wrote the original draft of the manuscript. Luxi Zhang conducted data analysis, reviewed and revised the manuscript, and acted as the project administrator. Xinshu Zhao acted as the guarantor for the research and funding supporter. All authors have approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants of University of Macau (Grant Nos. CRG2021-00002-ICI, ICI-RTO-0010-2021, CPG2021-00028-FSS, and SRG2018-00143-FSS), Xinshu Zhao PI; Macau Higher Education Fund (Grant No. HSS-UMAC-2020-02).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.