
Abstract
Objectives
To describe a study protocol for a three-arm randomized controlled trial that will evaluate the effectiveness of an Aged Smart-Care (ASC) application program intervention for community-dwelling older adults in China.
Methods
This randomized controlled trial with three arms will be conducted at eight community health service centers. Participants will be randomly assigned to one of three groups: the interactive ASC (ASC + I) group, the regular ASC group, or the control group. The ASC + I group will receive management from a multidisciplinary medical team, while the regular ASC group will only utilize the ASC. The primary outcome will be assessed using the Medical Outcomes Study Short Form 36 (SF-36) Health Survey. The secondary outcomes include general self-efficacy, medication adherence, effectiveness of health behavior interventions, BMI, number of outpatient visits, and number of hospitalizations. Data will be collected at baseline, immediately post-intervention, 3 months, 6 months, and 1 year after the intervention. Generalized estimating equations model will be employed for data analysis.
Conclusions
This study clarifies the development process of the ASC and designs a three-arm randomized controlled trial to examine the efficacy of the ASC for older adults in the community. The results of the study will compare differences in the quality of life of participants in different groups. This will help community healthcare workers to choose appropriate interventions regarding the ASC. Furthermore, this provides scientific guidance for the Integrated Theory of Health Behavior Change theory in the field of mobile health tool development.
Introduction
The global trend in the ageing population poses a substantial public health dilemma.1,2 The proportion of the global population aged ≥ 65 is projected to increase from 10% in 2022 to 16% in 2050. 3 In China, the largest developing country, the older population is growing at the fastest rate, 4 and by 2022, the population of individuals aged ≥ 60 will reach 280 million. 5 The phenomenon of population aging poses serious challenges for family caregiving, allocation of medical resources, and economic and social development. The World Health Organization (WHO) reported that to ease the burden of older care in China, we must first address the health problems of older adults. 6 Nevertheless, as the primary screen for older health at the grassroots level, community health service centers often face challenges such as the dissemination of health resources, insufficient medical and nursing human resources, and limitations in home health monitoring. 7 The healthcare requirements of older adults have frequently gone unaddressed, causing health anxiety quandaries.8,9 Hence, the convenient implementation of fast and convenient health surveillance services is crucial for promoting active aging.
The high penetration rate of mobile phones has increased the popularity of mobile health (mHealth) services among older adults. 10 According to the 54th report of the CNNIC (CHINA INTERNET NETWORK INFORMATION CENTER), a total of 7.42 million new internet users were added, with the age group of 60 and above accounting for 20.8% of the new internet users. 11 Literature studies show that more and more older adults have a positive attitude towards using smartphones to manage their health in daily life more effectively. 12 Currently, research on the use of mHealth for managing the health of the older population can be directed toward two key aspects: First, the research and development and application of mHealth. For example, Wang et al. 13 developed a community-based health-monitoring system tailored for older adults. This system uses station-based monitors, wearable electric trackers, and gait behavior sensors to record and acquire daily activities, continuous vital signs, and gait behaviors of older adults. Subsequently, an integrated decision support system will be employed to analyze changes in data; provide alerts to older individuals, their family members, and caregivers; and make supplementary medical decisions based on the acquired information. Lee et al. 14 incorporated a remote-monitoring feature into the rehabilitation equipment used by older women with knee arthritis in the community, enabling the recording of their movement patterns and providing guidance and feedback through weekly video calls. These findings indicate that telemedicine rehabilitation–monitoring devices can effectively enhance the adherence of older individuals to interventions and improve their limb function recovery. However, these studies have often focused on single diseases, and the scope of implementation of mHealth is relatively limited in managing the complex and varied health conditions of older adults in the community, which requires an assessment of mHealth service demands and cost-effectiveness. For instance, Huang et al. surveyed older individuals in 720 communities and revealed that Chinese seniors preferred to access medical services via remote monitoring methods. 15 A separate study indicated that the older population exhibits a preference for remote technology designs and functionalities that align with their physiological characteristics and cater to their self-actualization needs. 16 Bashshur et al. 17 emphasized that the implementation of virtual consultation services and precision care services facilitated by mobile communications could significantly enhance the efficiency, service reach, and convenience of the healthcare industry while producing cost savings. Thus, the development of a universal mHealth tool for older adults in the community is crucial for addressing the diverse health needs of this demographic, enhancing their quality of life, and optimizing medical resource allocation.
The Integrated Theory of Health Behavior Change (ITHBC) provides a new theoretical framework for the design and implementation of intelligent care systems for older adults. The ITHBC theory posits that the promotion of health behavior change is contingent upon augmenting knowledge and beliefs, increasing social facilitation, and enhancing self-regulation skills and capacities. The modification of health behaviors is regarded as a recent outcome that ultimately affects overall health outcomes. 18 Furthermore, this theory encourages the participation of multidisciplinary teams in implementing health behavior change interventions to compensate for shortcomings such as poor compatibility and insufficient interaction of existing remote monitoring devices for older people with different health needs. Prior research has validated the beneficial impacts of mHealth, which was developed using the ITHBC theory on individuals in the middle to older age demographic. For instance, Chen et al. developed a WeChat mini program incorporating six functional modules grounded in this theoretical framework, 19 and by providing decision support, effective quality assessment, data upload, personalized health guidance, and feedback to the user, significant enhancements in nutritional and activity behaviors have been achieved. Drawing on the ITHBC theory, Bao et al. 20 developed a pharmacist-assisted mHealth system emphasizing knowledge and beliefs, self-regulation skills and abilities, and social facilitation. This system incorporates educational resources, weekly meetings, personalized pharmacist consultations, and self-monitoring of daily health behaviors to enhance users’ health self-management capabilities. While these studies validate the feasibility of applying the ITHBC theory in mHealth development, they primarily focus on single-disease populations, leaving a gap in evidence supporting its potential benefits for managing multiple chronic conditions. This study developed the Aged Smart-Care (ASC) Application Program using the MINA framework of WeChat Mini Programs, based on previous research 15 on the health needs of community-dwelling older adults and the ITHBC theory. We aim to design a three-arm randomized controlled trial to verify the application effects of the ASC in community-dwelling older adults. This will provide a new tool to promote healthy aging in China and improve the quality of life for senior individuals in the community.
Methods
Study design and setting
This parallel-group, 1:1:1 randomized, controlled, and assessor-blinded three-arm trial will be used to measure the effectiveness of ASC on the quality of life of community-dwelling older adults. To optimize the promotional impact of the program, the ASC will be conducted as a pilot trial at eight community health service centers in Jiangsu, Eastern China. This study will be performed following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines. The intervention will be reported using the CONSORT-EHEALTH statement (Consolidated Standards of Reporting Trials of Electronic and Mobile Health Applications and onLine TeleHealth). The study complies with the Declaration of Helsinki. The trial has been registered at ClinicalTrials.gov: ChiCTR2400092856.
Participants
The study population will consist of community-dwelling older adults. Inclusion criteria are: (a) age ≥ 60 years; (b) adequate cognitive and functional abilities, as assessed by the Mini-Mental State Examination and Activities of Daily Living;21,22 (c) being in a stable phase of chronic illness; and (d) ability to self-monitor. Exclusion criteria include individuals who: (a) are experiencing an acute phase of chronic illness; (b) have cognitive impairments or physical functional limitations; (c) lack sufficient motivation for engagement or the ability to consistently participate in the intervention; or (d) are illiterate, have difficulties with reading and writing, or do not have access to a smartphone.
Sample size
Using the quality of life dimension of the 36-item short-form health survey (SF-36) scale as the primary outcome measure, sample size calculations were conducted based on methodologies outlined in similar studies.23–25 We selected the effect size from references where the maximum sample size could be calculated. 23 Assuming a two-tailed α of 0.05, a β-error probability of 0.2 (90% power), an effect size of 0.847, and a standard deviation of 13.1, the sample size was determined. Using the preset parameters, the calculation was performed using the Multiple Comparisons within the Means menu of the SPSS 2021 software, resulting in 73 participants per group. Considering an expected attrition rate of 20%, at least 92 participants per group (totaling 276 participants) will be required.
Recruitment, randomization, and blinding
After obtaining approval from the community service center, we will begin the research at the site through open recruitment, utilizing poster displays and public presentations. All members involved in the recruitment process will receive comprehensive training and be equipped with a standardized set of protocols that include guidelines for research materials and dialog with potential participants. Research Assistant A will assess the eligibility of the participants and be responsible for data collection. The researcher will provide a comprehensive overview of the study's objectives, procedures, potential risks, and benefits before obtaining informed consent from each individual. Contact information will be exchanged, appointments will be scheduled for preintervention data collection, and necessary preparations will be made. Each participant will receive a sealed opaque envelope containing their randomly assigned sequence number generated by Research Assistant B using a random number generator in Microsoft Excel 2021 after completing the baseline surveys, ensuring that the measurement technicians responsible for data collection and coding are blinded to group allocation. Research Assistant C, who is not involved in the recruitment process, will randomly assign participants based on their enrollment order and the randomized code contained within the envelope in a 1:1:1 ratio. Because app use is difficult to blind, neither the recruited participants nor the intervention facilitator is blinded to the group assignment. Figure 1 shows a consort diagram of the study flow.

Consort diagram for study flow.
ASC development
Our research group has developed the ASC system based on the ITHBC theory to provide remote health monitoring and medical consultation services for older adults in the community. The ITHBC theory emphasizes the importance of individual cognition regarding disease knowledge and a strong belief in disease treatment, encouraging individuals to actively pursue behavioral change. Accordingly, the ASC includes a disease knowledge and medication reminder module. The theory also suggests that effective social facilitation positively impacts individuals’ engagement in modifying their health behaviors. As such, the ASC incorporates modules for health consultation, personal health files, intelligent health monitoring, and check-in clocks. Additionally, the ITHBC theory highlights the need for providing health advice and skill guidance to support individuals’ self-regulation skills. To promote risk prevention and enhance self-regulation, the ASC includes a risk prevention module (Table 1 and Figure 2). Following the identification of these modules, an expert meeting was convened to thoroughly evaluate the rationale and scientific validity of the module configurations. The expert panel included five geriatric specialists, a smart care expert, and an information engineer. The specific contents of the discussion are as follows.

ASC client functions.
Seven ASC modules and content.

Knowledge and belief
First, older adults’ acquisition of adequate disease knowledge and beliefs is a prerequisite for implementing healthy behaviors. The ASC designed in this study establishes a disease knowledge guidance module, which is included in the knowledge system for common chronic diseases in seniors. In addition, to promote the confidence of older adults in disease management, we provided a function for medication reminders, aimed at mitigating the issue of older individuals forgetting to take their prescribed medications. When dispensing medication to older individuals, community volunteers aid in enabling a background reminder setting function, establishing a specified time for medication intake, and delivering timely reminders to promote adherence. We aim to bolster patients’ confidence in the efficacy of disease treatment by augmenting their understanding of their condition and prompting adherence to medication dosages through our proprietary mobile application.
Social facilitation
The ITHBC theory posits social facilitation includes social influence and support. The concept of social influence involves the use of authoritative persuasion to impact the cognition and drive of individuals to enhance their adherence to health behavior interventions. In the ASC, this authoritative influence is supported by our multidisciplinary team of physician-nurse dietitians. In the health consultation module, the intervention offers users pertinent advice on health issues, with a focus on elucidating the influence of health behaviors on disease outcomes. Social support encompasses the emotional, instrumental, and informational assistance collectively provided by healthcare professionals, family members, friends, and other sources. In the ASC, we categorized personal health files, intelligent health monitoring modules, and check-in clock modules as tools and information support features. These include the following points. (a) The personal health file module will be used to document the medical history, medication status, and other pertinent information of older individuals, which is then synchronized with the community health management center corresponding to the user's location. (b) A health intelligence monitoring module will be designed to monitor the general health data of older adults, including heart rate, blood pressure, blood oxygen saturation, body temperature, sleep quality, weight, exercise steps, and blood sugar.26,27 Users are requested to selectively input the health metrics associated with their individual circumstances. The ASC uses a computerized decision model to screen for abnormal health data. (c) The check-in clock feature requires users to access the check-in page upon initial login to the ASC to enable intervention personnel to remotely monitor participant engagement frequency within the ASC. The configuration of these modules can offer continuous health tracking services to users and elevate their level of medical support.
Self-regulation skills and ability
Older individuals seeking to adopt healthy behaviors must develop self-regulating abilities and the capacity to implement their knowledge of the disease in their daily lives. To assist users in making health decisions, this study used real-time monitoring data to provide online health and risk assessments for users by multidisciplinary medical staff and feedback evaluation recommendations to the users. The ASC has a risk-prevention reminder module. When the health indicator is abnormal (e.g. blood pressure > 140/90 mmHg), the ASC client automatically displays the risk dialog box. When users click on the dialog box, they are warned about the high risks and preventive measures, including health promotion, medical assistance, and advice, if necessary.
The ITHBC theory advocates tracking and evaluating changes in health behavior before, during, and after an action. To ensure the smooth implementation of the ASC, the project will hold monthly summary meetings with members, including general practitioners, nurses, and dietitians. Theme of the conference: (a) Create a health plan for each user, including knowledge learning, diet, and exercise plans. A nurse will send the plan to the user through the ASC session window. (b) Nurses report common health inquiries from the ASC users and evaluate whether they lack understanding of the disease and the ability to cope with it and discuss how to improve this understanding through a health consultation module. (c) Adjustment of intervention measures and plan duration. The team discusses the implementation status of the diet with the user as feedback from the ASC and adjusts the intervention based on user feedback.
Intervention protocol
To ensure the inclusivity of the ASC, professional training will be provided to participants before the study begins. This training will cover topics such as registering for the ASC, transmitting intelligent health monitoring data, managing personal health files, activating consultation mode, and accessing health instructions from healthcare professionals. Each participant will receive approximately one hour of training until they are proficient in using the system. To aid retention, the training materials will be provided in the form of operating manuals and instructional videos. Additionally, professionally trained researchers will be stationed in the community to offer technical support as needed.
The intervention period for this study will be 24 weeks. We require users to log into the ASC at least five times a week to enter health data content on the intelligent health monitoring page. These data form a continuous dynamic health information in the personal health record module. After one week of consistent use, our team of researchers will provide individuals with health recommendations. Users and interveners can communicate in a virtual face-to-face environment and send text and voice messages, as well as emotional ICONS. We employ MD5 encryption to store sensitive user data securely, thereby mitigating the risk of information leakage. Before the submission of health data, users are required to complete and sign an informed consent form with our organization indicating their agreement to share user data with healthcare professionals.
ASC with interactivity (ASC + I) group
Participants in the study will be enrolled in an active intervention program led by a geriatric care specialist and general practice professional in collaboration with a clinical dietitian. This program will provide personalized health advice and continuous supervision throughout the entire process of using the ASC system.
ASC group
The ASC group will have full access to the app content. However, the participants in this cohort will not receive the same level of supervised services from the intervention as those in the ASC + I group. They are prompted to use their smartphones if they have not used the app for more than a week. If individuals encounter any health issues and seek advice from a nurse, they have the option to use the health consultation feature to inquire about their health concerns. After baseline measurements, the multidisciplinary team will provide health education programs specifically tailored to the older adults in this group.
Control group
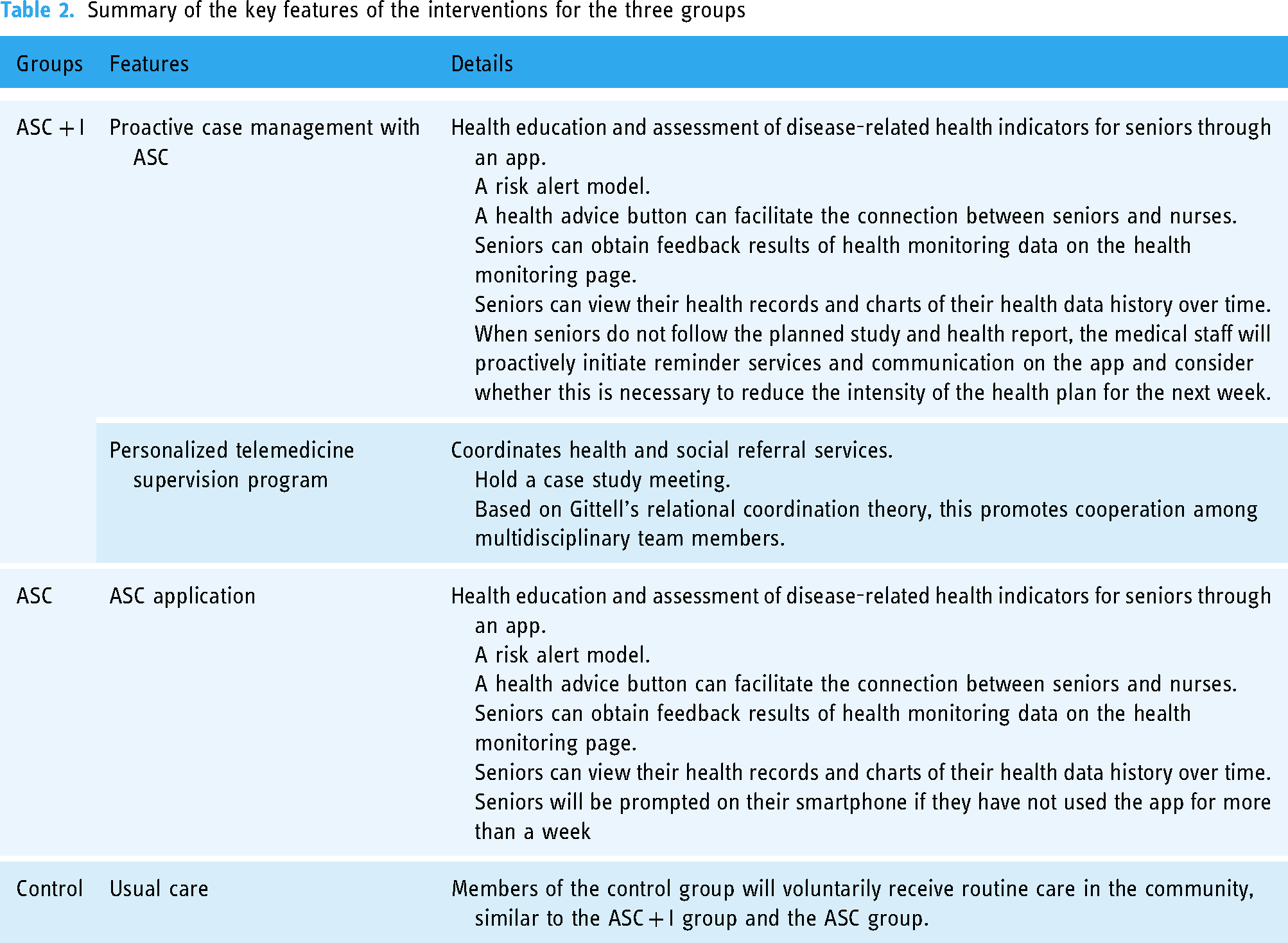
All the groups will be provided with community-based care. These services encompass health education, community outreach, management of chronic diseases, preventive healthcare interventions, and regular physical examinations. All participants must voluntarily participate in the study. Communities offer medical services and referrals to individuals in need; however, the availability of these services is inconsistent. Additionally, the control group will have unrestricted access to the internet to obtain health-related information while being unable to utilize the ASC. Table 2 provides a comprehensive overview of the primary characteristics of the three intervention categories.
Summary of the key features of the interventions for the three groups
Data collection
Data will be collected at five distinct time intervals: baseline before intervention (T1), immediately after intervention (T2), 3 months (T3), 6 months (T4), and 1 year after intervention (T5) to test the sustained intervention effect. For subjective data collection, including quality of life, self-efficacy, medication adherence, daily smoking amount, daily alcohol consumption, and satisfaction with ASC + I or ASC, a structured questionnaire has been developed. Data will be collected by Research Assistant A through offline, face-to-face interviews. Objective data collection includes exercise frequency/duration, body mass index (BMI), outpatient visits, and hospitalization records. Relevant information is automatically extracted from the ASC back office system through intelligent health monitoring and personal health files. This automated data export mechanism is designed to reduce potential information bias associated with subjective patient self-reporting.
Outcome measures
Nine sets of measures will be assessed: demographics, the SF-36, general self-efficacy scale (GSES), Morisky medication adherence scale (MMAS-8), the effectiveness of health behavior intervention, BMI, number of outpatient visits, number of hospitalizations, and satisfaction with the ASC + I or ASC.
Primary outcome
The main outcome is the quality of life of older people. The SF-36 is specifically designed for the comprehensive assessment of adult health and encompasses various dimensions to evaluate the physical and mental well-being of an individual. 28 This contains 36 items covering eight health dimensions: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, emotional role, and mental health. The responses to the individual questions will be transformed into a numerical score within the range of 0–100, and the overall score for each health domain will be computed based on the questionnaire items. The SF-36 comprises 35 subitems and an overall health assessment question. The responses to each question will be assigned a definite value based on health status, usually ranging from 0 to 5 or 0 to 6. The original dimension score will be obtained by adding the scores of questions in the same health field. Higher scores indicate better quality of life. The Cronbach's α of this scale is 0.895, which has been widely used in studies of communities of older people and is suitable for measuring the quality of life of older Chinese people.
Secondary outcomes
The self-efficacy scale will be used to assess individuals’ perceived capability to manage challenging circumstances or resolve personal issues. 29 The scale comprises 10 items, each using the Likert 4-level scoring method, with options for one point denoting complete incorrectness, two points indicating partial correctness, three points representing mostly correct responses, and four points signifying complete correctness. The total score ranged from 10 to 40 points. Higher scores indicated greater individual self-efficacy. Cronbach's α coefficient for this scale was 0.87, indicating high internal consistency. Currently, this scale is widely used among older individuals in both urban and rural communities in China, including those with chronic diseases.
The MMAS-8 is commonly used to evaluate patient adherence to prescribed pharmacotherapy regimens. 30 The scale questions will be designed to take the form of simple yes/no or level of agreement answers to quickly assess any compliance problems that patients may encounter. The MMAS-8 comprises eight questions, each designed to assess different aspects of medication behavior. For questions 1–7, no points are awarded for each “yes” answer and one point for each “no” answer. Question 8 uses a five-point scale: never (one point), occasionally (two points), sometimes (three points), usually (four points), and always (five points). A score of eight is categorized as demonstrating high medication adherence, six to eight falls into the category of moderate medication adherence, and less than six as low medication adherence. Cronbach's α coefficient of this scale was 0.876.
Other data
Effectiveness of health behavior interventions. The effectiveness of the intervention will be evaluated in this study using a set of key health-related behaviors. (a) Daily smoking amount: measured in cigarettes per day. (b) Daily alcohol consumption: quantified in mL per day. (c) Frequency of exercise: recorded as the number of exercise sessions per week. (d) Exercise duration: the length of each exercise session in minutes.
BMI is a mathematical formula used to evaluate the correlation between the weight and height of an individual and serves as an indirect indicator of body fat composition. BMI is widely used to assess whether a person falls within the healthy range of weight. In this study, we used the BMI classification criteria specific to the Chinese population: underweight (BMI < 18.5), normal range (BMI 18.5–23.9), overweight (BMI 24.0–27.9), and obesity (BMI ≥ 28.0).
The number of outpatient visits refers to how often an individual visits a healthcare provider during a given period. In this study, the number of outpatient visits refers to the number of visits within the most recent month at the time of the questionnaire.
The number of hospitalizations refers to the admission of an individual to a hospital for treatment within a specific period. In this study, the number of hospitalizations refers to the number of hospitalizations within the most recent month at the time of the questionnaire (details are listed in Table 2).
Satisfaction with ASC + I or ASC: Participant satisfaction with ASC + I or ASC will be measured using a Likert scale, with possible responses ranging from one (very unsatisfied) to five (very satisfied).
Data analysis
Intention-to-treat analyses will be used to analyze all available data. Additionally, the results of the per-protocol analysis will be reported to ensure its stability and robustness. Descriptive statistics will be used to analyze the sample characteristics. Continuous numerical variables will be described using means and standard deviations, whereas discrete numerical variables will be described using quartiles. Categorical and ordinal data will be described using frequencies and percentages. Differences in baseline characteristics among the three groups will be compared using Chi-squared or Fisher's exact tests for categorical variables. A one-way analysis of variance will be used for continuous variables that conform to a normal distribution. The Kruskal–Wallis H test will be used for variables that did not conform to the parameter test.
The generalized estimating equation will be used to assess the differences in the ASC + I, ASC, and control groups (between-group effects), as well as within-group (time) effects and their interactions. Given the 5 time points in this study, an exchangeable working correlation matrix will be used to emphasize the consistent spacing between repeated measurements for each patient. 31 Considering the effect of repeated measurements on the production of type I errors, p-values will be adjusted using the Bonferroni method. We will use IBM SPSS 25.0, and all statistical tests will be tested at a two-tailed alpha level of 0.05.
Monitoring and data management
The research team will convene monthly to assess the progress of participants in completing the program, to address any adverse events, and to make adjustments to the program tasks for the subsequent phase. The research team consists of a nursing scientist (PhD) who studied geriatrics, three medical doctors, and two PhDs who studied clinical nutrition.
Ethics and dissemination
The experimental protocol has been approved by the Ethics Committee of Xuzhou Medical University (XZHMU-2022032). Findings will be disseminated broadly via peer-reviewed empirical journals, articles, and conference presentations.
Discussion
Most countries worldwide are struggling to cope with the increasing challenges posed by aging populations. With the rapid increase in the number of older adults, relying on community healthcare management alone has proven insufficient in terms of human resources. 7 Due to geographical isolation and medical difficulties, a considerable number of older people in communities cannot receive effective healthcare services and thus face the risk of health damage.13,32,33 The project proposed in this study aims to build health management software for older adults based on the WeChat mini program MINA framework and to verify its effectiveness. This is expected to provide technical support for the future social health management of older adults. This study expands the evidence to examine whether the ASC is more beneficial when a multidisciplinary healthcare team is involved. Furthermore, in comparison with the short-term and medium-term durations (approximately 12 weeks) used in previous research, 34 This study extends the intervention to 24 weeks and a 1-year follow-up will be conducted to provide new evidence for exploring the long-term effects of digital tools in older adults.
The successful application of the ASC may be attributed to its distinctive benefits. First, the ASC is a mobile medical application specifically tailored for older adults in accordance with the ITHBC theory. Ryan's study provides empirical evidence that the ITHBC theory can significantly enhance individual self-efficacy and reinforce self-management behavior. 35 Second, the ASC operates on the WeChat platform. The latest data show that WeChat had over 1.38 billion monthly active users. 36 This advantage provides ASC with a favorable propagation path and convenient accessibility. In addition, the seven modules included in the ASC have been designed to address the healthcare requirements of older individuals in the community more effectively. The disease knowledge module enables users to access treatment measures for a range of chronic conditions, thereby providing older individuals with pertinent knowledge support within this module. Zhou et al. 37 demonstrated that adequate knowledge support can improve self-management. Second, Shade et al. contended that the use of mHealth programs facilitates adherence to medication regimens among patients. 38 Therefore, the medication reminder module established by the ASC is specifically tailored to assist older individuals in adhering to their prescribed medication regimens, thereby enhancing their confidence in managing their illnesses. Third, intelligent health monitoring and risk prevention modules can assist in documenting the health status of older individuals, dynamically monitoring their physical health data, and aiding them in mitigating high-risk events resulting from deficiencies in self-regulation skills and abilities. The module resembles the Smart-HF system developed by Yoon et al., 39 wherein patients input their vital signs, heart rate, and symptoms of heart failure, along with images of their daily dietary intake and physical activity. Subsequently, the program generates alerts based on a predefined algorithm that prompts patients to seek medical attention when unusual changes are detected. Finally, the collaboration between interdisciplinary teams offers a wide range of medical resources to ASC users, enhancing convenience and diversity. Jacob et al. demonstrated that interdisciplinary collaboration can address the intricate healthcare requirements of patients, enhancing their contentment with the delivery of care, and ultimately improving disease prognosis. 40
Strengths and limitations
ASC possesses several technical advantages. First, for users with sensory impairments, ASC is equipped with built-in voice search and content broadcasting features. These age-appropriate designs cater specifically to the needs of older users. Second, ASC includes a user feedback plugin, allowing technical staff to upgrade the system based on user feedback. Most notably, ASC is built on the MINA framework of WeChat mini programs, which significantly reduces development, promotion, and maintenance costs, making it a potentially highly cost-effective solution for implementation in communities, particularly in developing countries.
However, certain challenges may arise during the implementation of this study. To address these challenges and enhance the inclusiveness of the ASC, several strategies will be employed. First, a community initiative will be implemented in which project volunteers guide seniors through using the mobile app. This approach is designed to alleviate any stress associated with applying and learning the ASC system. When seniors encounter technical difficulties, volunteers will assist them in resolving these issues. The reliance on volunteer-assisted technology adoption, while pragmatic, may introduce intervention bias that could artificially amplify the intervention's effects. Improvements in health outcomes may, in part, be attributed to increased social interaction facilitated by volunteer engagement. Second, to reduce the high attrition rate, the ASC will include a routine reminder function, and feedback from continuous health reports will be sent to participants weekly, encouraging regular check-ins. Additionally, due to age-related declines in visual and auditory functions, some participants may face difficulties integrating technology with the ASC. To address this, the system's accessibility will be maximized by enlarging font sizes, enhancing video images, and adjusting the volume of multimedia content. However, greater accessibility does not necessarily mean that ASC is fully inclusive. While accessibility adaptations, such as font enlargement and audio adjustments, address sensory impairments, they may not entirely overcome fundamental barriers to technology adoption. Therefore, integrating new user guidance features and tutorial videos within ASC remains a critical technical challenge that requires urgent future updates.
Finally, researchers must consider the potential cultural sensitivities in different socio-cultural contexts that may affect the promotion of the ASC, particularly the limited international popularity of WeChat. To attract older individuals from diverse ethnic backgrounds, necessary adaptations will include the development of separate iOS and Android versions of the ASC. However, the costs of cultural adaptation may disproportionately impact resource-limited communities, potentially widening existing health disparities. Furthermore, the cross-cultural adaptation of ASC (covering the adaptability of language and icons, the integration of health behaviors and cultural values, as well as the compliance of laws and ethics) is also a technical difficulty to be solved in the promotion process.
Conclusion
The widespread promotion and use of mHealth can be attributed to its ability to transcend temporal and spatial constraints and optimize medical service resources. This facilitates timely access to medical services for older individuals conveniently, thereby mitigating potential adverse consequences associated with their limited capacity to seek prompt medical care. The results of this study will further enrich the practical guidance of the ITHBC theory in chronic disease management. The seven major intervention modules designed according to this theory may promote health outcomes such as the quality of life of users and help meet their needs. If the ASC demonstrates efficacy in promoting health and reducing healthcare expenditures, the use of mobile applications employing this interactive communication model may be perpetuated in pilot areas with the potential for expansion to other developing regions.
Footnotes
Acknowledgments
Availability of data and materials
The data of this study are available upon reasonable request to the corresponding author.
Consent for publication
All authors have reviewed and approved this manuscript as being submitted.
Clinicaltrials.gov Identifier
ChiCTR2400092856.
Contributorship
YX managed the trial, developed ASC, designed the study, and drafted the manuscript; QH drafted the manuscript and translated text; ST and YW provided nursing support for the ASC, and translated text; HS offered medical support; ML, MZ, and JL provided advice on the development of ASC; XT conceived the study and drafted the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical Conduct of Research: This study protects the privacy and identity security of the research subjects. All participants will be provided written informed consent. The study protocol has been approved by the Ethics Committee of Xuzhou Medical University (XZHMU-2022032). All methods were performed in accordance with the Declarations of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the Key Laboratory Project of Ministry of Education for Long-term Care of the Elderly (LNZDPY- 2023- 03) and General Project of Philosophy and Social Science Research in Colleges and Universities of Jiangsu Province (2024SJYB0814).
Guarantor
XT.