
Abstract
Introduction
The glucose management indicator (GMI) and time-in-range (TIR) are important glycemic parameters calculated from continuous glucose monitoring (CGM) values. KARAZ, a hybrid Internet of things—artificial intelligence platform, was developed in Saudi Arabia to help manage diabetes mellitus. The complex nature of self-care and behavior changes associated with diabetes mellitus requires breaking large behaviors into achievable ones and related incentives.
Aim
This study explored how tiny habits as a behavioral intervention and incentive system affect glycemic control among KARAZ Platform users with diabetes mellitus in various age groups in Saudi Arabia.
Methods
This retrospective study included KARAZ Platform users and analyzed the effects of behavioral interventions and incentives on GMI and TIR as glycemic control parameters.
Results
Of 296 active users, 118 (40%) and 148 (50%) maintained a desirable TIR and GMI, respectively. Adult females aged ≥ 26 years who consistently followed tiny habits and behavior changes exhibited a significant reduction in the GMI (5%). Intrinsic motivation through behavioral modification was more effective than external incentives for maintaining glucose control.
Conclusion
The findings highlight how behavioral interventions can impact GMI, suggesting their effectiveness in promoting better health behaviors and improving glycemic control in the Saudi Arabian context. Further research should investigate how these habits and behaviors can be maintained sustainably without relying on external incentives. Recommendations discussed how children with Type 1 diabetes mellitus would benefit from CGM connection to KARAZ Platform iteration and the integration of a comprehensive diabetes care program within the Saudi health system.
Keywords
Introduction
The glucose management indicator (GMI) is among the glycemic control parameters calculated from average continuous glucose monitoring (CGM) values, which measure glucose in the interstitial fluid every 1–5 min. The GMI provides perspective on how hemoglobin A1c (HbA1c) is trending but in a shorter time window because it incorporates time spent within the target glucose range. 1 A randomized clinical trial (RCT) on adults with Type 2 diabetes mellitus (T2DM) who underwent CGM reported a 16% increase in time-in-range (TIR) over an eight-month follow-up period. 2 In contrast, a trial concluded the effectiveness of CGM in reducing times with hypoglycemia among children with type 1 diabetes mellitus (T1DM) in aged between 2 and 8 years. 3 Moreover, a clinical trial among older adults with T1DM who used CGM devices reported a significant increase in TIR by 8% over 52 weeks and a reduction in hypoglycemia. 4 In 2019, the international consensus on TIR recommended three key CGM measurements with cutoff points for actionable glycemic control: percentage of readings and time per day within the target glucose range (TIR), time below the target glucose range (TBR), and time above the target glucose range (TAR). Variations in targets based on individual profiles have been suggested for glycemic control assessment. 5
KARAZ can be identified as a hybrid Internet of Things (IoT)—artificial intelligence (AI) platform in Saudi Arabia, combining IoT for data collection from CGM devices and AI for data analysis and personalized health management. A recent study conducted in the USA reported that AI-assisted care targeting at risk individuals with DM can decrease DM-related hospital admissions by up to 19% by helping patients manage glucose levels more effectively. 6 Moreover, IoT are claimed to provide scalable healthcare solutions, making CGM technology more accessible, particularly in underserved areas. Furthermore, previous studies have revealed that IoT-enabled healthcare services, including CGM, could reduce healthcare costs by 25% and improve remote patient care access by 50%, particularly in rural locations.7–10
Regarding personalized management plans, an RCT in Japan concluded that IoT devices connected to glucose monitors and activity trackers facilitated real-time feedback to both users and providers. 11 Moreover, IoT systems improved HbA1c levels by integrating body weight, blood pressure, and activities and empowered individuals with T2DM to better manage their behavior and conditions over a 52-week follow-up period than the control group. 12 Furthermore, Internet-based devices provide interactive communication with automated data upload and have been reported to significantly decrease HbA1c levels from 7.86 to 7.55 in the intervention group compared with 7.81–7.70 in the control group. 11
Behavioral modifications have been applied in various contexts, including diabetes management, to encourage the adoption of healthier behaviors. However, the “tiny habits” framework has shown promise in increasing gratitude and psychological well-being. 13 The tiny habits framework suggests that behavioral modifications can be facilitated by breaking down desired behaviors into small, manageable actions, attaching these actions to existing routines in life and celebrating successes.14,15 However, its application in diabetes control remains limited. The information—motivational—behavioral (IMB) skills model, which emphasizes information, motivation, and behavioral skills, has been validated as a comprehensive framework for diabetes self-care. 16 Community-based diabetes management, which incorporates “tiny habits” principles, has been shown to be effective when patients are knowledgeable and self-efficacious. 17 However, various studies have also indicated that sustainable behavior changes in diabetes management are complex and influenced by various factors, including social support, education, and personal motivation.16,18,19 Literature suggests that a multifaceted approach, such as the IMB model, is more appropriate for addressing the complex nature of diabetes self-care behaviors.13,16,17,20,21
In addition, to a previous study on the technology acceptance model among patients with T1DM within Saudi arabia, 22 we could not identify any publications addressing the impact of IoT on glycemic control within the country. The significance of these studies is providing evidence for the effects of behavioral modifications and incentives on both the GMI and TIR, which can inform the development of more personalized interventions to improve glycemic control. 23
This study evaluated the impact of the “tiny habits” framework as a behavioral change framework on glycemic control, including TIR and GMI. Furthermore, this study analyzed the effects of the KARAZ incentive system on GMI, considering diverse age groups, sexes, and glucose impairment types among KARAZ users.
Methodology
This retrospective analytic study evaluated the effects of KARAZ Platform use on glycemic management and associated behavioral factors.
Participants
The study included active KARAZ Platform users who met the following inclusion criteria: used either device-based CGM or manual blood glucose monitoring systems associated with the KARAZ Platform for at least 90 days, demonstrated familiarity with the KARAZ Platform's self-management tools, and benefited from the KARAZ “Cherries” virtual and badge incentive system. The exclusion criteria were as follows: pregnant women with DM and individuals who reported comorbid conditions that could interfere with DM management or their ability to use the KARAZ Platform effectively.
Statistical analysis
All statistical analyses were performed using Statistical Package for the Social Sciences (version 16). Categorical variables are presented as frequencies and percentages. Continuous variables with nonnormal distribution are presented as medians and interquartile ranges (IQRs). The chi-square test was used to evaluate significant relationships between dependent and outcome variables. p-values < .05 were used to denote statistical significance. Correlation analysis was performed to explore the relationship between selected tiny habits, namely, “hits” and “misses,” and TIR. Furthermore, the relationship between the KARAZ incentive system, namely, “badges” and “cherries,” and TIR was explored. A regression model was applied to control for confounding factors and identify significant predictors of GMI. These predictors included “hits” and “misses” and “badges” and “cherries.” To ensure regression model stability, a current sample size of 296 observations was included, and three of the identified significant predictors within the study objective were included in the model. “Badges” and sleeping were excluded from the model because they exhibited low reporting values. Moreover, only a small proportion (3.7%) of users benefited from “badges.”
The GMI was calculated using the following equation
1
:

Data cleaning procedures included removing duplicates and anonymizing participant information by the KARAZ Platform's administrator. The 90-day platform use was selected to ensure the reliability of the GMI and TIR values. Variables were extracted using a custom-designed standardized Excel sheet and managed based on the following operational definitions: age reported in years; sex categorized as male, female, or not reported; KARAZ incentive system (“cherries” and “badges”) incentivizes healthy behaviors by awarding virtual “Cherries” for actions such as glucose monitoring, meal logging, and attending consultations. These points can be redeemed for tangible awards, such as discounts on healthy products, services, and well-being programs. Tiny habits were behavioral factors reported by the participants and included sleep duration (hours per day), insulin use adherence, and average number of daily “hits” (successful behaviors) and “misses” (unachieved targets).
Ethical considerations
Ensuring anonymization and maintaining privacy, KARAZ complies with Saudi government legal requirements for the following: data protection, data accuracy, and protecting users from harm. It complies with the regulations set by the Saudi Food and Drug Association (SFDA) and Ministry of Health for telemedicine and remote monitoring. 30 KARAZ Platform management ensures that all devices, such as CGM systems, meet SFDA standards. Furthermore, KARAZ is pursuing international certifications (ISO 14971:2019—MEDICAL DEVICES APPLICATION OF RISK MANAGEMENT TO MEDICAL DEVICES, ISO / IEC 27001:2013 Information Security Management Systems, ISO 13485:2016 Medical Devices—Quality Management System) and ISO 27001 for information security, ensuring quality management and data protection. Users of the platform obligated to consent approval on data collection and use for research purposes according to the KARAZ privacy policy https://karaz.app/privacy-policy/.
Ethical approval was obtained from the Institutional Review Board according to the following application number: UJ-REC-262 and under the following title: Impact of the KARAZ platform's behavioral interventions and incentives on diabetic glycemic control in Saudi Arabia. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist was used to ensure the compliance of quality of reporting combined cohort and cross-sectional studies.
Results
The study analyzed data from 296 participants residing in Saudi Arabia; these participants met the inclusion criteria. Most participants 218 (73.6%) were identified as having lifestyle glucose impairment or T2DM, whereas less than one-fifth were identified as having T1DM. Table 1 presents the detailed demographic and clinical profiles of the participants.
Profile of KARAZ beneficiaries (n = 296).

Glycemic control indicators
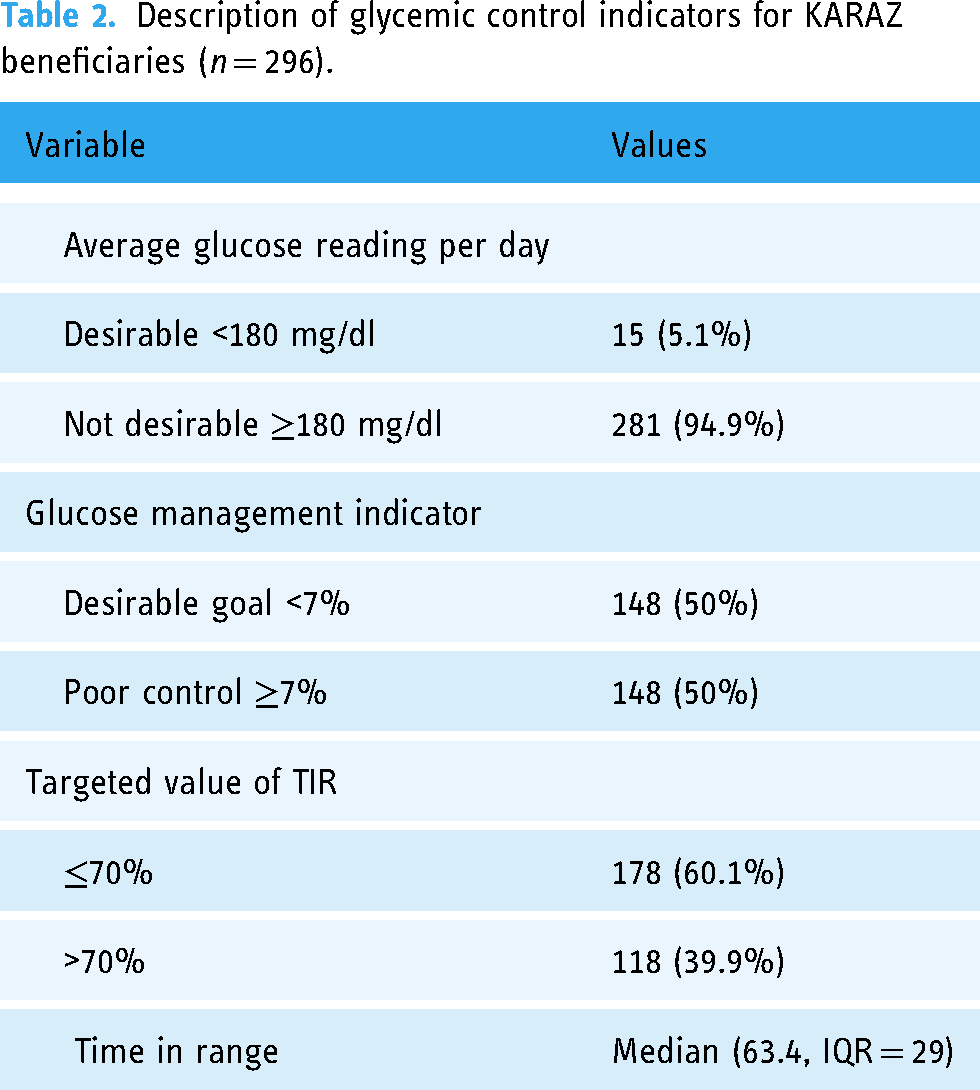
Regarding glycemic control, approximately half of the participants 148 (50%) achieved the desired GMI goal of <7%. For TIR, 118 (40%) participants maintained glucose levels within the target range of 70–180 mg/dL (Table 2).
Description of glycemic control indicators for KARAZ beneficiaries (n = 296).
Behavioral patterns and incentives
Only 59 (20%) participants reported their average daily sleep duration, of whom 47 (15.9%) reported sleeping at least 8 h per day. Insulin use was reported by 40 (13.5%) participants, with usage being highest among individuals with T1DM, particularly in the 4-year-old and 21–26-year-old age groups. The differences in insulin use across other glucose impairment types and age groups were statistically significant (Table 3). The participants reported a median of 1.73 successful behavior “hits” per day (IQR = 99.8) and a median of 99.6 behavior “misses” per day (IQR = 79.6). The mean number of “cherries” earned per day was 5.1 ± 2.31, and only 11 (3.7%) participants benefited from earning badges. The highest number of badges earned was 39, whereas the lowest was only one.
The pattern of insulin use among various age group, gender and glucose impairment type (n = 296).

Indicating significant difference in chi-square testing.
Age, sex, and glucose impairment patterns
The highest proportion of individuals with a desirable GMI (<7%) was observed among participants aged >26 years, with the differences between age groups being statistically significant (p < .018). Females exhibited a significantly higher proportion of individuals with a desirable GMI than males (p < .016), as shown in (Table 4).
The association between glucose management indicator value across age groups and gender.
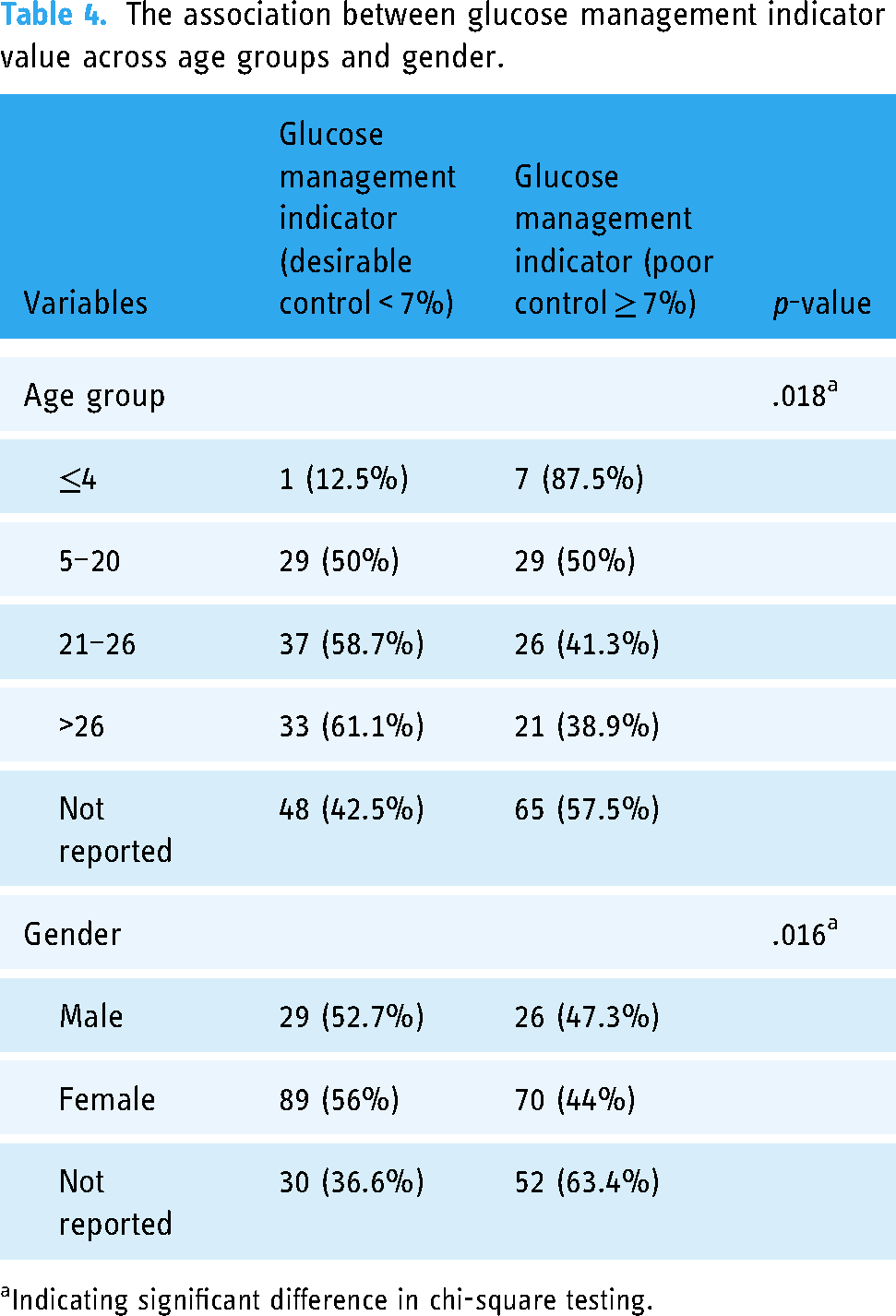
Indicating significant difference in chi-square testing.
The highest TIR (≥70% of the time) was reported among participants aged 21–26 years, followed by those aged >26 years, with differences across age groups being statistically significant (p < .004). TIR was equally high among males and females (p < .01), indicating good glycemic control compared with participants who did not report their sex. Although TIR was highest among individuals with T1DM, differences across glucose impairment groups were not statistically significant (Table 5).
The association between TIR value, age groups, gender and glucose impairment type.

TIR: time-in-range; T1DM: Type 1 diabetes mellitus; T2DM: Type 2 diabetes mellitus.
Indicating significant difference in chi-square testing
Association between behaviors, incentives, and glycemic control
A Spearman's rank-order correlation analysis was performed to evaluate the relationship between TIR and behavioral/incentive metrics. A strong and statistically significant positive correlation was observed between TIR and both average daily “hits” (rs = 0.86, n = 296, p < .001) and total “badges” earned (rs = 0.54, n = 296, p < .001). Furthermore, TIR exhibited a strong positive correlation with the total number of “cherries” earned (rs = 0.91, n = 296, p < .001). These findings suggest that higher TIR values are associated with increased adherence to desired behaviors and greater engagement with the incentive system.
Regression model's assumptions and findings
The key assumptions were tested before applying the regression model. The residual plots exhibited homoscedasticity, confirming the assumption of constant variance. However, the assumption of linearity was violated based on the scatterplots of residuals against predictors. To address this issue, logistic regression analysis was performed on the binomial outcome GMI. Residual diagnostics for linearity revealed that the residuals for “cherries” were normally distributed, supported by a straight Q-Q plot and the Shapiro–Wilk test (p = .086). However, residuals for “misses” and “hits” deviated from normality. All predictors (“hits,” “misses,” and “cherries”) exhibited relatively low variance inflation factor values (3.6, 1.9, and 5, respectively), indicating no multicollinearity. The results indicate that each additional unit increase in the average “hits” per day was associated with a significant decrease in GMI by 5% (p < .001). In contrast, each additional unit increase in the average “misses” per day is associated with a significant increase in GMI by 6% (p < .001). However, the total number of “cherries” earned was not a significant predictor of GMI (Table 6).
Logistic regression identifying tiny habits and incentive related effect size on glucose management indicator.

Indicating significant association.
Discussion
The largest proportion of KARAZ users in Saudi Arabia were classified as having lifestyle glucose impairment or T2DM 206 (73.3%).
Principal findings and comparison with previous studies
Of the 296 participants, 148 (50%) maintained the GMI goal of <7% over the 90-day use of the KARAZ Platform. The reported desirable GMI in this study was found to be highest among females and individuals aged >26 years. Considering that GMI offers insight into the trend of HbA1c, previous studies have considered it a surrogate for the targeted control value.27,28 Our findings exhibited better glucose control over a short period among females aged >26 years. This is potentially due to more established and consistent management practices among this group. The findings are consistent with broader literature indicating that age and sex can play critical roles in DM management, with older adults and females often demonstrating greater interest in enrolling in chronic disease prevention programs. 31 Females also have more stable glucose control, possibly due to higher insulin sensitivity and the protective effects of estrogen and receptor activation on adipose tissue and pancreatic beta cells.32,33 Moreover, self-care behaviors, quality of life, and treatment adherence were identified as influencing factors.34,35
This study exhibited disparities between lifestyle-related glucose impairments and/or T2DM and other glucose impairment categories, including T1DM. The findings highlight the need for targeted interventions and lifestyle modifications tailored specifically for individuals with T2DM. This aligns with that of previous research, which indicated that patients with T2DM often struggle with effective glycemic management due to insulin resistance and other metabolic factors, namely, beta cell dysfunction and obesity.36,37 Furthermore, discrepancy between TIR and GMI was observed. This could be due to variations in the methods of glucose monitoring, device calibration, measurement duration, and high variability in glucose values.1,38
The analysis revealed that the highest reported insulin use was among individuals with T1DM at the age of 4 years, comprising less than one-fifth of the sample. As shown in Table 3, despite the significant difference in insulin use observed across age groups and among glucose impairment patterns, the underrepresentation of T1DM within the study group made it challenging to conclude the direct impact of KAZAR Platform use on glycemic control compared with T2DM. The issue could be resolved using a randomized controlled design focused on children aged 2–8 years diagnosed with T1DM to assess TIR, GMI, and other glycemic control variables and evaluate the effectiveness of CGM devices integrated within the KARAZ Platform.
Effects of behavioral changes and incentive systems on TIR and GMI values
Many studies have considered TIR as a surrogate marker of long-term cardiovascular complications among individuals with DM. 39 Moreover, a review on TIR-driven CGM values identified an inverse relationship between TIR and diabetic nephropathy, diabetic peripheral neuropathy, and cardiac autonomic neuropathy. 40 The existing finding on the correlations of TIR with average “hits” per day and total number of “cherries” and “badges” earned by KARAZ users is statistically significant, suggesting a clear association between improved TIR and increased engagement in behaviors beneficial for glucose control among 40% of the study group. The application of logistic regression allowed controlling the confounding factors. Despite the current regression model limitations, the findings highlight how behavioral interventions, such as average “hits” per day habits and “misses,” can significantly impact GMI, suggesting their effectiveness in promoting better health behaviors and improving GMI in the Saudi Arabian context.
Our findings are consistent with those of previous studies, which concluded that regular physical activities have positive effects on insulin sensitivity and glucose control. Likewise, studies on habit formation have highlighted that developing behaviors such as consistent self-monitoring and meal tracking can improve long-term glycemic outcomes, often exceeding the benefits of external incentives.41–43 Regarding incentives, the Trial to Incentivize Adherence for Diabetes study conducted in Singapore highlighted the benefits of process-based financial incentives for individuals with T2DM. By focusing on specific behaviors, such as regular glucose monitoring and physical activity, these incentives proved to be more effective at improving HbA1c levels than outcome-based incentives. 44
In contrast, the total number of “cherries” earned as incentives was not a significant predictor of glucose regulation. This finding supports contradicting results regarding the effectiveness of incentives in lifestyle modification programs, as one RCT study concluded a significant reduction in HbA1c levels among incentivized adults with DM. 45 However, the effectiveness of incentives varied depending on cultural values and the level of acceptance. 46
Finally, the impact of the KARAZ Platform after measuring HbA1c levels with active involvement of physicians and/or providers is worth evaluating considering the extended patient follow-up period of at least 52 weeks. This approach can help prevent long-term disease complications. For children aged 2–8 years diagnosed with T1DM, future evaluations should consider using a randomized controlled design. The aim would be to assess TIR, GMI, and other glycemic control variables and to evaluate the effectiveness of CGM devices integrated with the KARAZ Platform.
Limitations
This study has some limitations to consider. Primarily, there may be variability in participant engagement with the digital platform and its associated incentive system. Such variability may lead to inconsistent data regarding the not reported predictors of insulin resistance, such as BMI, mental health status, and dietary factors. Furthermore, the variable's reliance on self-reported data for specific behaviors, such as reported steps per day, exercise, reported insulin use, and sleeping time, may introduce systematic biases. Variations in the participants' familiarity and comfort with technology may hinder their ability to fully engage with the resources available, ultimately affecting the overall efficacy of the incentive system intervention. Furthermore, disparities in digital literacy among the participants could impact the effective use of both the incentive system and the digital tools provided. The regression model's limitations include the potential impact of nonnormal residuals for “misses” and “hits” as predictors. Furthermore, important predictors, namely, “badges” and “sleeping,” were excluded due to low reporting values, which may have introduced omitted variable bias. Regression findings should be considered with caution because they may limit the generalizability of the results. Finally, the exclusion of other components of the KARAZ Platform may restrict the model's ability to fully capture the incentive system's dynamics. Future studies with larger samples and additional predictors are recommended. Finally, the retrospective study design has limitations, such as the inability to establish causal relationships, limited control over data collection, and the presence of confounding factors. These limitations should be addressed in future iterations of IoT-based CGM platforms or applications, with a particular focus on enhancing the reporting of behavior change data, refining incentive systems, and strengthening the connection to glycemic control assessment methods. These improvements will contribute to a more reliable identification of causative relationships in future research.
Conclusion
Despite the listed limitations, our findings highlight how behavioral change reporting can significantly impact GMI, suggesting its effectiveness in promoting better health behaviors and improving glycemic control within the Saudi Arabian context and among KARAZ Platform users. Further longitudinal studies are recommended to investigate how these habits and behaviors can be maintained sustainably without relying on external incentives. Recommendations discussed how children with T1DM would benefit from CGM connection to the KARAZ Platform and system integration into a comprehensive diabetes care program within the Saudi health system. This research is novel and breaks new ground by exploring the influence of AI and IoT data on the connections between behavior changes and incentives and their impact on glycemic control.
Footnotes
Acknowledgments
The authors acknowledge the contribution of all study participants. Also, authors acknowledge the use of ChatGpt 4o in the writing and editing process of this manuscript. The tool provided valuable assistance in drafting, proofreading, and enhancing the overall readability of the text.
Consent for publication
This study utilized deidentified health data, ensuring that no personal identifiers were present and that individuals cannot be reidentified from the data. The publication of results is based on aggregated data and does not contain any information that could identify individual participants. All ethical standards and privacy of the Saudi national law have been followed. The Saudi Data and Artificial Intelligence Authority, under the Personal Data Protection Law, defines personal data as any information that can directly or indirectly identify an individual. This includes, but not limited to, specific identifiers such as: a person's name, National Identification Number (e.g., Iqama or Saudi National ID), contact details like email addresses, physical residential addresses or geographic location, IP addresses, and unique device identifiers. Additionally, during data extraction phase, KARAZ administration adhered to the General Data Protection Regulation guidelines on anonymization, particularly focusing on pseudonymization and data minimization principles. The anonymization process included the following steps:
Removal of identifiers: Personal identifiers such as names, addresses, contact information, and other direct identifiers were completely removed from the dataset. Pseudonymization: Unique codes replaced sensitive attributes like patient ID numbers and replaces with user ID code, ensuring that no direct link between the code and the individual's identity. Generalization: Certain data fields, such as age or location, were generalized to reduce details (e.g., age groups instead of exact age, or counntry as Saudi Arabia instead of specific addresses). Suppression: Outlier data that could potentially lead to reidentification was either removed or suppressed. For example, outlier readings were excluded.
The possibility of reidentification through data combination has been minimized using the following strategies: (1) Removal of linkage variables: Any variables that could be linked to external datasets. (2) Risk reduction: No dataset released publicly or shared externally contains sufficient information to allow reidentification when combined with other datasets. In conclusion, the dataset has been anonymized using rigorous standards, and the likelihood of reidentification is negligible.
Consent to participate
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical consideration
Ensuring anonymization and maintaining privacy, KARAZ complies with Saudi Government legal requirements for the following: data protection, data accuracy, and protecting users from harm. It complies with the regulations set by the Saudi Food and Drug Association (SFDA) and Ministry of Health for telemedicine and remote monitoring. KARAZ Platform management ensures that all devices, such as CGM systems, meet SFDA standards. Furthermore, KARAZ is pursuing international certifications (ISO 14971:2019—MEDICAL DEVICES APPLICATION OF RISK MANAGEMENT TO MEDICAL DEVICES, ISO / IEC 27001:2013 Information Security Management Systems, ISO 13485:2016 Medical Devices—Quality Management System) and ISO 27001 for information security, ensuring quality management and data protection. The STROBE statement checklist was used to ensure the compliance of quality of reporting combined cohort and cross-sectional studies.
Ethical approval
Ethical approval was obtained from the Institutional Review Board according to the following application number: UJ-REC-262 and under the following title: Impact of the KARAZ Platform's behavioral interventions and incentives on diabetic glycemic control in Saudi Arabia.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.