
Abstract
Background
To address the lack of mental health practitioners in developing countries, the current study explored the feasibility of a newly developed self-guided digital intervention program TEA (training for emotional adaptation) in alleviating depressive and anxiety symptoms, as one of a few studies which adapted from theoretical models with effective intervention techniques.
Methods
The first part of this study involved 11 professional mental health practitioners giving feedback on the feasibility of the TEA; while the second part involved a mixed-method single-arm study with 32 participants recruited online, who went through the seven intervention sessions within 14 days. The questionnaires were collected before, after, 14 days after, and 30 days after intervention. Additionally, 10 participants were invited to semi-structured interviews regarding their suggestions.
Results
Practitioners thought that the TEA showed high professionalism (8.91/10) and is suitable for treating emotional symptoms (8.09/10). The generalized estimating equation model showed that the TEA significantly reduced participants' depressive and anxiety symptoms, while the effects of the intervention remained 30 days post intervention (Cohen's d > 1). Thematic analysis revealed three main themes about future improvement, including content improvement, interaction improvement, and bug-fixing.
Conclusions
To address the current needs for digital mental health intervention programs to account for the insufficient availability of mental health services in China, the current study provides preliminary evidence of the effectiveness of TEA, with the potential to address the urgent need for remote mental health services.
Trial registration
The study was registered at the Chinese Clinical Trial Register (ChiCTR), with number [ChiCTR2200065944].
Introduction
Psychological distress refers to an individual's negative emotional reaction to stressors, including depressive and anxiety symptoms. 1 It has become a serious public health problem and causes an enormous burden for youth and the society in recent years. For example, the prevalence of depressive and anxiety symptoms increased sharply during the COVID-19 pandemic.2,3 In China, the prevalence of mental health problems has reached 17.5%. 4 However, the availability of mental health services is far from sufficient for individuals with emotional problems, especially in developing countries, in which 79–93% of individuals with depressive symptoms and 85–95% individuals with anxiety symptoms struggle to access effective mental health intervention. 5 Therefore, it is of great importance to develop mental health interventions that are easily accessible and cost-efficient.
According to a meta-analysis, habitual use of various emotion regulation techniques significantly correlated to symptoms of depression or anxiety, where adaptive emotion regulation skills negatively associated with these symptoms, and maladaptive emotion regulation skills positively associated with mental health problems. In particular, depressive and anxiety symptoms were found to positively correlate with emotion regulation techniques such as avoidance and rumination, and negatively correlate with acceptance. These results underscore the importance of interventions that develop adaptive emotion regulation techniques in improving symptoms of depression and anxiety. 6 Furthermore, the ubiquitous existence of the internet and smartphones provides a new opportunity to increase the accessibility of mental health services through smartphone-based online platforms. 7 Especially during the COVID-19 pandemic, the feasibility of attending in-person mental health services has been repeatedly reduced, while digital mental health intervention (DMHI) provides us with an alternative. 8
The significant imbalances of mental health professionals in China also implies the need for extensive and scalable mental health interventions such as DMHI. For example,well-trained mental health professionals tend to gather in psychiatric hospitals in urban areas, leaving a shortage of accessible mental healthcare in rural areas. 9 However, some of the existing DMHI programs still involve mental health practitioners to offer additional support either online or in-person,10–12 those with the prerequisite of having mental health practitioners on stand-by is not feasible, given the lack of sufficient mental health professionals. Therefore, a cost-effective, self-help intervention DMHI program could be more suitable to meet people's mental health needs in China.
Previous studies have validated the effectiveness of online DMHI for emotional problems and suggested that emotion regulation techniques from cognitive behavioral therapy (CBT) and mindfulness-based cognitive behavioral therapy (MBCT) are effective in treating emotional disorders digitally.13,14 Among the existing DMHI for emotional disorders, intervention techniques including psychoeducation, behavioral activation, relaxation techniques, cognitive restructuring, and mindfulness are most frequently involved10,11,15,16,17,18 Nevertheless, as noted by recent systematic reviews, the majority of existing DMHIs for treating emotional problems in China mainly focus on treating schizophrenia 9 and depressive symptoms, 13 while other common mental health problems such as anxiety received inadequate attention. Given the high prevalence of co-morbid depressive and anxiety symptoms in China, the need to develop a DMHI that addresses these emotional problems is ever more pressing. 19
Gross 20 proposed a process model of emotion regulation, which suggests that individuals may struggle to regulate their emotions if they fail at any of the following stages. The first stage is identification, where an individual becomes aware of a situation that evokes their emotional feelings. Then, they might choose an appropriate regulation strategy to apply in the situation. Finally, in the implementation stage, the individual must decide on specific actions to take. In other words, facilitating an individual's ability at each stage is necessary to ensure effective emotion regulation, and thus to alleviate their emotional distress. Given the undeniable significance of emotion regulation in the treatment of emotional disorders, it is imperative to integrate evidence-based CBT techniques with a solid theoretical foundation to address the underlying causes of emotional problems.21,22,23
The training for emotional adaptation
Therefore, we developed a digital self-guided intervention for emotional problems in line with the process model of emotion regulation. The training for emotional adaptation (TEA) is a self-help digital mental health intervention program that combines effective CBT techniques with the process model of emotion regulation. The TEA consists of multiple components and starts with training on emotional identification skills. Participants are guided to recognize and understand their emotional experiences, and to gain insight into the underlying causes and triggers of their emotions. This stage helps individuals to develop greater awareness and insight of their emotional states. The program then focuses on expanding the repertoire of emotional strategies by considering both short-term and longer-term approaches. Short-term strategies aim to provide immediate relief that helps individuals to cope with acute emotional distress. This may include techniques such as deep breathing exercises, grounding exercises, and distraction techniques. On the other hand, longer-term strategies concentrate on cognitive changes. These strategies may involve cognitive restructuring, building mindfulness, and self-awareness.
TEA users will be encouraged to apply learned techniques and strategies in their everyday lives when they face challenging situations that evoke emotional distress. By actively implementing these skills in real-life situations, individuals can refine their skills, strengthen their emotional adaptability, and incorporate effective emotion regulation exercises as part of their daily routines. The combination of the process model of emotion regulation and effective CBT techniques has the potential to be highly effective in alleviating emotional distress among TEA users.21,22,23
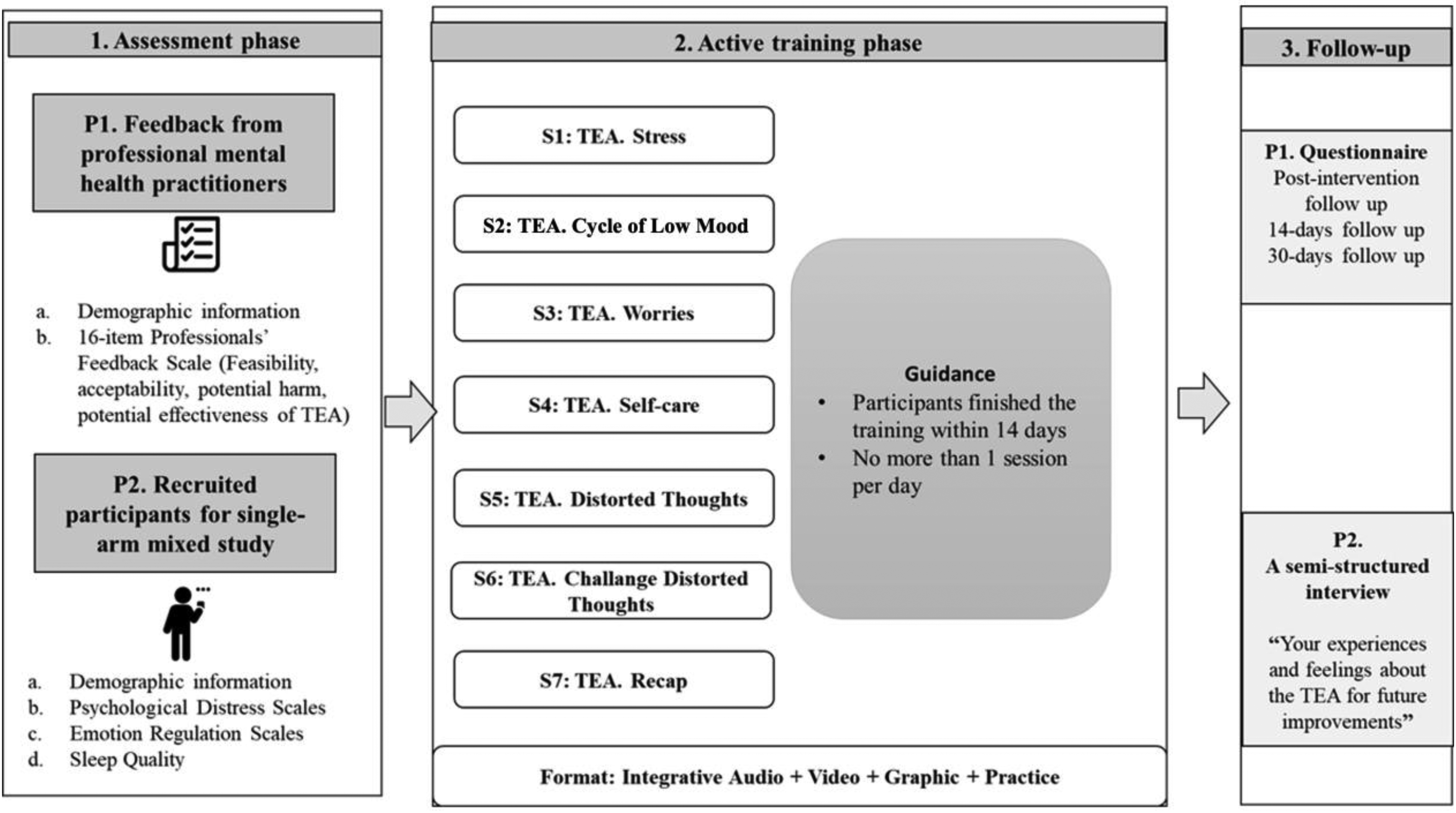
Specifically, the TEA consists of seven sessions constructed through the online platform of WeChat mini program, in which the structure of the seven sessions mimics the whole process model of emotion regulation. Following the themes of each stage of the process model, a series of CBT and MBCT techniques were assigned to each session. The intervention was delivered online via a combination of verbal and graphical information, intervention videos, audio instructions, and interactive practices.
Aims
The current study aimed to investigate the feasibility and preliminary effect of the TEA program for emotional problems including depression and anxiety symptoms. We hypothesized that participants would show a reduction of symptoms of depression and anxiety via measures. We also explored the effects on sleep quality and emotion regulation strategies as well as the participants’ satisfaction and subjective evaluation of the intervention.
Methods
Sample
The current study consisted of two parts. The first part involved collecting professional mental health practitioners’ feedback regarding the feasibility of the TEA as an online intervention for emotional disorders. The second part involved a single-arm study to test the effectiveness of the TEA on alleviating emotional disorder symptoms.
The feasibility of TEA
For the professional's feedback, our final sample involved 11 professional mental health practitioners as participants. These mental health professionals were recruited by online convenience sampling, eligibility criteria were that they received academic degrees in clinical/applied psychology/psychiatry, and currently working in a mental health setting. Furthermore, in order to gain feedback from clinicians with diverse working experience, we included practitioners at various stages of their career paths, ranging from those who just started working, to those that have worked for 27 years as clinicians.
The single-arm study
For the single-arm study, our final sample involved 32 participants, aged 18–36 (mean age = 25.38). The eligibility criteria include the following: (1) Participants aged 18–39; (2) Participants who can participate in our study through smartphones or other electronic devices; (3) Participants who are identified as having mild or more severe depression or anxiety symptoms by 9-item Patient Health Questionnaire (PHQ-9) or 7-item Generalized Anxiety Disorder (GAD-7) questionnaire (PHQ-9 > 5 or GAD-7 > 5). The exclusion criteria include the following: (1) Participants who refuse to give consent; (2) Participants who report having suicide risk within 1 week prior to the start of our study; (4) Participants who report having been diagnosed with psychotic disorders (e.g. schizophrenia, schizophrenic disorders), bipolar disorders, or other disorders co-occur with schizophrenic disorders; and (5) Participants who report receiving other psychological intervention programs. Please refer to Figure 1 for the flow of participant recruitment.

The flow chart of participant recruitment.
Data collection
The feasibility of TEA
Mental health professionals first went through the contents of the TEA WeChat mini program in 2 days. After that, they completed an online questionnaire that consisted of demographic information, a brief introduction of the TEA program, as well as a measure to gather feedback on professionals’ perceptions of the TEA program through an online questionnaire platform in July 2022. No further data were collected from them in the rest of the study. Based on professionals’ feedback, the TEA program was refined.
The single-arm study
Participants were recruited in July 2022 via online poster. They indicated their interest in participation by scanning the quick response code provided with the flyer and completing the online eligibility test questionnaire. Participants who met the eligibility criteria were contacted by researchers. A short video of the user's guide along with a brief instruction of the study procedure was provided before participation. Then, participants completed the pretest questionnaire online and started participating in the TEA. The TEA involves seven sequential sessions, in which the participants were required to complete the seven sessions in 14 days, while being limited to complete one session per day. Upon the completion of the seventh session, participants completed the post-test questionnaire online and indicated their interest in participating in a voluntary one-to-one semi-structured interview. On the 14th day after completion of the seventh session, participants completed the 14-day follow-up questionnaire online, while 10 participants were interviewed by team members online with experience with qualitative methods (i.e. semi-structured) through video conferencing software (TencentMeeting Video Communications) regarding “your experiences and feelings about the TEA for future improvements.” Investigators explained the study's aim, and all of the content was recorded by audio (i.e. after obtaining the consent from participants) and then transcribed verbatim by a transcription service provided by Tencent Meeting and deidentified by interviewers later.
On the 30th day after completion of the seventh session, participants completed a 30-day follow-up questionnaire online. In total, 50 CNY (1 CNY = 0.14 USD) was given to each participant who completed the whole research process, to increase their intention of participation (see Figure 2 for the flow of this study).
The flow chart of the current study.
Ethical considerations
The current study received ethical approval from Tsinghua University. All participants were debriefed about the study and gave consent online before participation, while they were aware of their rights to withdraw at any point of the study with no harm. For participants who indicated recent suicidal ideation or suicide attempt, we provided professional help-seeking information when removing them from participation. All data were safely stored in password-protected hardware, with only the relevant researchers having access to it. All personal information was kept confidential. Participants were given unique ID numbers for participant identification throughout the study. The study was registered at ChiCTR, with number [ChiCTR2200065944].
Measurements
The feasibility of TEA
Demographic information
For the professionals’ feedback, participants self-reported their demographic information prior to the introduction to the TEA through online questionnaires. That includes age, gender, education level, professional title, and mental health-related work experiences.
Professionals’ feedback
Professional mental health practitioners’ opinions of the TEA were measured through a 16-item Professionals’ Feedback Scale specifically designed for the current study. That includes participants’ opinions about the feasibility, acceptability, potential harm (reverse score), and potential effectiveness of the TEA. Participants self-reported their opinions through an 11-point Likert scale for each item ranging from 0 (e.g. “Very ineffective”) to 10 (e.g. “Very effective”). See the details of the Professionals’ Feedback Scale in Supplemental Appendix 1.
The single-arm study
Demographic information
For the single-arm study, participants self-reported their demographic information at eligibility test and pretest. This includes age, assigned gender, sexual orientation and gender identity, education level, socioeconomic status, occupational status, marital status, religion, ethnicity, psychiatric diagnosis, the current situation regarding COVID-19-related restrictions and previous experiences of DMHI.
Psychological distress
Depressive symptoms were measured through the PHQ-9 24 at eligibility test, post-test, 14-day follow-up test, and 30-day follow-up test. Participants self-reported their depressive symptoms through a 4-point Likert scale for each item ranging from 0 (“Not at all”) to 3 (“Nearly every day”), with a maximum possible total score of 27. The recommended cutoff point for clinically significant depression was set at 9, 25 while a score below 5 was indicated as not having depression symptoms. 23 The PHQ-9 has good reliability and validity for measuring depressive symptoms in Chinese people. 26
Anxiety symptoms were measured through the GAD-7 27 questionnaire at eligibility test, post-test, 14-day follow-up test, and 30-day follow-up test. Participants self-reported their anxiety symptoms through a 4-point Likert scale for each item ranging from 0 (“Not at all”) to 3 (“Nearly every day”), with a maximum possible total score of 21. The recommended cut-off point for clinically significant depression was set at 8, 28 while a score below 5 was indicated as not having anxiety symptoms. 27 The GAD-7 has good reliability and validity for measuring anxiety symptoms in Chinese people. 29
Emotion regulation
Emotion regulation abilities were measured through the 6-item short Emotion Regulation Questionnaire (ERQ-6) 30 at pre-test, post-test, 14-day follow-up test, and 30-day follow-up test. The ERQ-6 was developed by extracting three items from the cognitive reappraisal domain and three items from the expressive suppression domain of the original Emotion Regulation Questionnaire. 31 Participants self-reported their emotion regulation abilities through a 5-point Likert scale for each item ranging from 1 (“Strongly disagree”) to 5 (“Strongly agree”), with a maximum possible total score of 15 for each domain. For each domain of the ERQ-6, higher scores indicate greater trait strength by which the individual regulates emotion in the respective manner. The ERQ-6 has been shown as having good reliability and validity for measuring emotion regulation abilities. 30
Sleep quality
Insomnia was used as a reversed indicator of sleep quality. Insomnia was measured through the 7-item Insomnia Severity Index (ISI-7) 32 at pre-test, post-test, 14-day follow-up test, and 30-day follow-up test. Participants self-reported their insomnia severity through a 5-point Likert scale for each item ranging from 0 (e.g. “No problem”) to 4 (e.g. “Very severe problem”), with a maximum possible total score of 28. The cutoff point for having insomnia symptoms was set as 8. 32 The ISI-7 has been shown as having good reliability and validity for measuring sleep quality in Chinese people. 33
Statistics
All quantitative statistics were conducted using R-4.1.0. 34 Demographic information was collected for professional mental health practitioners and participants in the single-arm study separately. Descriptive statistics were conducted for each item of the professional feedback scale. We calculated the mean, standard deviation, median and range for continuous variables, and percentages for categorical variables.
We applied generalized equation (GEE) models to explore the predictive effects of measurement time points and depression symptoms, anxiety symptoms, cognitive reappraisal emotion regulation, expressive suppression emotional regulation, and sleep quality, which reflect the impacts of the TEA intervention on these mental health characteristics.
Demographic information was controlled for in the GEE models. Post-hoc within-participant t-tests were conducted to explore the differences between these mental health statuses at four time points, which provides us with additional information about when the intervention impacts emerged and how long they remained. Bonferroni corrections were applied to reduce the risk of false positives. A post-hoc power analysis was conducted to test if the participants we reached can provide adequate statistical power.
For qualitative statistics, detailed verbatim transcriptions were refined and cross-checked by three researchers (CC, JA, and LDY). Word software was used for coding and analysis of transcripts. The thematic analysis method followed the steps proposed by Clarke et al. (2015), followed by one question, “how to future improve the TEA from your own experience.” Taken together, (1) for team members, including two who had previous experience with qualitative methods (CC and JA), familiarization with the data, independently reviewed the two transcripts and created an initial codebook (framework), by using comparison and consensus. (2) Then, the codebooks were collaborated and refined by four team members (CC, JA, LDY, and ZX), and any disagreements and possible solutions were identified and evaluated at the research group meeting. Codes were grouped into themes iteratively until without further modification. (3) Then, themes about the “future improvements of the TEA” were extracted and refined by two researchers from all transcripts (CC and JA), and cross-checked by two researchers (LDY, and ZX). (4) Examples were translated and double-checked by researchers who are fluent in both Mandarin and English (CC and LDY).
Results
Descriptive statistics can be found in Table 1. Our final sample includes 32 participants in the single-arm study (mean age = 25.38, 87.5% female, 6.3% gender minority, 40% students, 6.3% with previous psychiatric diagnosis), and 11 mental health professionals (mean age = 37.73, 63.6% female, mean year working in mental health service = 12.55). A post-hoc power analysis with the final sample size of 32, a significant level of 0.05, and the smallest effect size of the significant effects of 0.66 indicated that the current sample provides a statistical power of 95% for the current study.
Demographic information of the participants.

Professional's feedback
The results of the Professionals’ Feedback Scale are presented in Table 2. Overall, professionals’ evaluation of the TEA was positive. The professionalism of the TEA (i.e. the accuracy of how CBT techniques and illustrations were used) received the highest score (mean = 8.91, SD = 0.94), while the extent to which behavioral changes can be induced by the TEA received the lowest score (mean = 7.18, SD = 0.87). Based on professionals’ feedback, the TEA program was refined.
Training for emotional adaptation (TEA): professional's feedback.

Qualitative analysis of intervention effects
The results of the GEE model and post-hoc within-group t-tests are presented in Table 3. Generally, participants’ mental health symptoms reduced significantly after completing the TEA intervention, in which the symptom levels remained low a month after intervention (as illustrated in Figure 3).

Intervention effects of the training for emotional adaptation (TEA).
Intervention effects of the training for emotional adaptation (TEA).

GEE: generalized equation modeling; Bonferroni corrections were applied.
***p < 0.001; **p < 0.01; *p < 0.05.
Positive value indicates worsening of symptoms.
Positive value indicates greater trait strength.
Specifically, for depressive symptoms, the GEE model indicated significant intervention effects of the TEA on depression symptoms (β = −1.49, p < 0.001). The post-hoc t-tests showed that compared to pre-intervention, depression symptoms significantly reduced after intervention (t = −4.29, p < 0.001), while the intervention effect remained at 14-day follow-up (t = −4.85, p < 0.001) and 30-day follow-up (t = −6.37, p < 0.001).
For anxiety, the GEE model indicated significant intervention effects of the TEA on anxiety symptoms (β = −1.46, p < 0.001). The post-hoc t-tests showed that compared to pre-intervention, anxiety symptoms significantly reduced after intervention (t = −3.91, p = 0.007), while the intervention effect remained at 14-day follow-up (t = −4.55, p < 0.001) and 30-day follow-up (t = −6.45, p < 0.001).
For cognitive reappraisal emotion regulation, the GEE model indicated significant intervention effects of the TEA on cognitive reappraisal (β = 1.63, p < 0.001). The post-hoc t-test showed no significant change in cognitive reappraisal between pre-intervention and post-intervention measurements (t = −1.74, p = 1.365). However, cognitive reappraisal significantly increased at 14-day follow-up (t = 4.67, p < 0.001), while the intervention effect remained at 30-day follow-up (t = 5.03, p < 0.001).
For expressive suppression emotion regulation, the GEE model indicated significant intervention effects of the TEA on expressive suppression (β = −2.03, p < 0.001). The post-hoc t-test showed no significant change in expressive suppression between pre-intervention and post-intervention measurements (t = 0.15, p = 1.323). However, expressive suppression significantly decreased at 14-day follow-up (t = −7.61, p < 0.001), while the intervention effect remained at 30-day follow-up (t = −6.12, p < 0.001).
For sleep quality, the GEE model indicated significant intervention effects of the TEA on sleep quality (β = −1.32, p < 0.001). The post-hoc t-tests showed that compared to pre-intervention, insomnia severity significantly reduced after intervention (t = −3.73, p = 0.012), while the intervention effect remained at 14-day follow-up (t = −4.02, p = 0.005) and 30-day follow-up (t = −5.24, p < 0.001).
Qualitative analysis of future improvements
The results of the thematic analysis of the semi-structured interview are presented in Table 4. Participants’ suggestions about future improvements of the TEA were classified and combined into three larger themes, including “content improvement,” “interaction improvement,” and “bug-fixing.”
Training for emotional adaptation (TEA): participants’ improvement suggestions.

Overall, participants’ suggestions are mainly about user experience. In the content improvement theme, participants suggested to improve user engagement through gamification and more encouraging reinforcement. For example, “You can modify the existing contents into interactive games, like Super Mario that involves different sessions and tasks,” and “The current virtual rewards given (upon completing each session) are not encouraging enough.”
Additional contents were suggested to include more detailed examples, review sessions and the marking completion section. For example, “You can provide me with a detailed list that includes the activities I can do in a week … so I know what (activities) to do to improve my emotional states,” “Although I have the willingness to change, I probably need to repeat (the training), or have recap sessions, as we only have seven sessions,” and “You can create a marking section for me to mark the activities I should complete, to help me make behavioural changes.” Few participants also indicated a desire for optional more detailed and difficult contents for people who find the existing contents too shallow. For example, “If anything, I would like to have some deeper contents. I think the current content is relatively shallow. You can have the contents graded (from easy to difficult).”
In the interaction improvement theme, participants suggested to improve multimedia interactions and add daily reminders for completing the sessions. For example, “The audio recording at one page sometimes contains information on the next page.” Participants also indicated desire for better communication experiences both with peers and with staff. For example, “To set up a message board, for us to record some of our puzzles, and then maybe we can answer them next time.” In the bug-fixing theme, participants mainly reported program crashes and content-saving problems that need to be fixed. For example, “Every time I want to go back to the previous page, I slide back to the previous page from left to right, sometimes I find that I just quitted.”
Discussion
Main findings
The current study confirmed a significant impact of the TEA program on reducing emotional problem symptoms through a two-step process. In the first study, feedback was gathered from mental health professionals to assess the feasibility, acceptability, potential harm, and effectiveness of the TEA. Based on professionals’ feedback, the TEA program was refined. Second, the single-arm study used mixed methods to not only collect and compare quantitative data at pre-intervention, post-intervention, and 14-day follow up, and 30- day follow up, but also gathered qualitative data through semi-structured interviews from TEA users. Overall, our results supported the feasibility and preliminary effectiveness of the TEA in alleviating emotional symptoms including depression and anxiety, and these findings are in line with similar studies previously conducted in other countries. 35
Our results from the single-arm study indicated a significant reduction of both depression and anxiety symptoms upon the completion of the intervention, in which the intervention effect lasted for a month. Compared to other digital interventions for depression and anxiety, which generally showed small to moderate intervention effects, 36 the TEA showed moderate intervention effects for both depression (d = 0.76) and anxiety (d = 0.69) post-intervention. Moreover, compared to pre-intervention, the TEA showed large intervention effects for both depression and anxiety at follow-up, which indicated a great potential for TEA to be applied as a self-guided digital intervention for depression and anxiety. From professionals’ feedback, the TEA was also rated highly for professionalism, practicability, effectiveness in treating emotional disorders, and feasibility for online intervention, which guaranteed its potential in treating depression and anxiety as a self-guided digital intervention program.
Strengths of the current study
One of the strengths of the TEA is that it illustrated a theory-practice link by systematically integrated intervention techniques based on corresponding factors outlined in the emotion regulation process model. Another strength of the TEA is that our results illustrated the impacts of the TEA not only on emotional problems but also on physiological and cognitive changes. For example, significant improvement in sleep quality was found after the intervention and at follow-up measures. An abundance of previous studies has found significant associations between sleep quality and both depression and anxiety.37,38,39 Previous studies have supported the effectiveness of digital CBT on insomnia comorbid with depression,40,41 which aligns well with our results showing reduced insomnia symptoms along with emotional problems. Through the integration of grounding techniques including relaxation training and mindfulness that have been shown to reduce sleep disturbance, 42 the TEA showed a potential to alleviate emotional problems by improving sleep quality. However, the underlying mechanisms between sleep quality and emotional problem symptoms require further clarification.
Moreover, from the cognitive perspective, our results indicated a significant improvement in participants’ ability in cognitive reappraisal, which supported the impact of the TEA on improving user's emotion regulation as conceptualized in the process model of emotion regulation. 43 One meta-analysis concerning the effective components of intervention programs developed based on the process model of emotion regulation found that cognitive change has the largest intervention effects among all aspects of the emotion regulation process. 23 The TEA has two sessions devoted to improving cognitive restructuring skills, hence facilitates reduction in emotional problems through inducing cognitive reappraisal ability. Another finding is that expressive suppression scores decreased among TEA users, and since expressive suppression has been identified as a maladaptive coping strategy that damages one's mental health,44,45 this provided further support on the effectiveness of TEA in reducing emotional symptoms. Finally, it was found that neither cognitive reappraisal nor expressive suppression scores changed significantly immediately after the intervention, but significant changes were found at 14-day and 30-day follow-ups. This indicated delayed impacts of the TEA on emotion regulation strategies, which is also in line with previous studies finding cognition as stable and difficult to change. 46 This also supported the importance of incorporating a comprehensive process of emotion regulation in an intervention program. However, future studies are in need to examine the effects of different intervention components of the TEA.
Limitations
While the TEA has been demonstrated as an effective intervention program for depression and anxiety symptoms, a few limitations need to be considered. First of all, the current study utilized a single-arm design, which undermines the strength of evidence in support of the intervention effects of the TEA. Moreover, the current study failed to explore the impacts of each intervention component on mental health outcomes, which means that we cannot draw a conclusion on whether the moderate-to-large impacts of the TEA on mental health outcomes is a result of incorporation of techniques targeting the whole emotion regulation process. Furthermore, while the current sample provided adequate power for our statistical aims, we acknowledge that we only had a limited number of participants due to our inability to follow a large number of participants, which restricted the capability of the current study to testify to the feasibility of the TEA in reaching potential users needing the interventions. Nevertheless, 502 participants attended the initial eligibility test, which indicates the potential of TEA to reach a greater number of potential users. Therefore, future randomized controlled trials with more comprehensive measures and a large participant group are necessary to further verify the intervention effects of TEA on mental health symptoms.
Implication for future studies
Based on the feedback gathered from participants in the semi-structured interviews, further versions of the program need to be developed to address existing problems, such as adding individualized contents, improving users’ experiences through the interactive user interface, as well as bug fixing. Although the intervention effects are encouraging, preliminary results from the feasibility test should be interpreted with caution, and a future randomized controlled trial with a large sample size should be conducted to further evaluate the intervention effect of TEA on psychological distress. Furthermore, considering the enormous user population of WeChat (i.e. over 1.2 billion monthly active users), making the TEA a highly cost-effective and easily accessible tool for people to utilize, and support them to potentially cope with anxiety and depression symptoms more effectively. As about 10% of WeChat users are international users, 47 the TEA could also be beneficial for individuals who are not currently living in China (e.g. Chinese people studying, working, or living abroad).
Conclusions
To address the current needs for digital mental health intervention programs due to the insufficient availability of mental health services in China, the current study investigated the feasibility of the Online Emotion Regulation Training Camp (TEA) as a self-help digital intervention for emotional disorders. Through the combinations of feedback from mental health professionals, a one-month single-arm study and semi-structured interviews, our results provide preliminary evidence supporting TEA as an effective intervention program for alleviating depression and anxiety symptoms, and the intervention effects remain stable across a month. However, future RCT studies are warranted to affirm the intervention effects of the TEA.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231187476 - Supplemental material for Process model of emotion regulation-based digital intervention for emotional problems
Supplemental material, sj-docx-1-dhj-10.1177_20552076231187476 for Process model of emotion regulation-based digital intervention for emotional problems by Diyang Qu, Dongyu Liu, Chengxi Cai, Xuan Zhang, Jiaao Yu, Quan Zhang, Kunxu Liu, Ziqian Wei, Jiajia Tan, Zaixu Cui, Xiaoqian Zhang and Runsen Chen in DIGITAL HEALTH
Footnotes
Contributorship
DQ was responsible for study conceptualization, methodology, investigation, data curation, visualization, and manuscript writing/editing. DL was responsible for methodology, investigation, data curation, formal analysis, validation, visualization, resources, and writing the original draft. CC was responsible for investigation, data curation, formal analysis, resources, and manuscript editing. XZ was responsible for investigation, validation, and manuscript writing/editing. JY was responsible for investigation, formal analysis, and validation. QZ was responsible for software. KL was responsible for investigation. ZW was responsible for investigation. JT was responsible for resources. ZC was responsible for resources. XZ was responsible for resources and supervision. RC was responsible for study conceptualization, methodology, manuscript editing, and funding acquisition. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The current study received ethical approval from Tsinghua University. Ethics Approval Reference: 20220107. Note: The current study obtained participants’ informed consent through participants’ online responses to an Agree/Not-agree choice. By selecting “Agree,” the participants could indicate that they agree with the following statement: “I have read this informed consent carefully and had the opportunity to ask questions, and the researchers have explained to me in detail and answered my relevant questions. I understand that participation in the study is voluntary, that I can withdraw at any time without giving a reason, and that my medical and legal rights are not affected. I have given sponsors, researchers, and health inspectors access to my medical records, knowing that sponsors will take all reasonable steps to protect my privacy. I agree to participate in the study.”
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was funded by the research fund of the Vanke School of Public Health, funding number: 100009001. Tsinghua University ‘Chun Feng' Fund for Domestic Research Special Project, funding number: 2021Z99CFY039. Shuimu Tsinghua Scholar.
Guarantor
RC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.