
Abstract
Background
Understanding human behaviors has been the subject of several studies. Their main goal was to inform behavior change interventions aimed at promoting positive behaviors and improving negative ones. However, as a non-expert in behavioral science, it is extremely difficult for researchers from other disciplines to design and develop evidence-based behavior change interventions. Moreover, all existing frameworks stop at the conceptual stage and do not provide instructions for developing digital-based behavior change interventions.
Objective
We present an end-to-end framework for the design and development of mHealth-based behavior change interventions by drawing on the synergy of theory, practices, and evidence from previous research.
Methods
We reconcile the frameworks most used in the literature for the design of behavior change interventions. Therefore, the authors examined the steps of each framework, and the mapping between these steps was carried out through several iterations to obtain five common steps.
Results
The proposed framework includes five steps: (1) Definition of the scope of the intervention. (2) Understanding and explanation of behavior. (3) Definition of the intervention content and strategies. (4) Implementation of the intervention. (5) Evaluation of the intervention. Each step is explained in detail, while providing researchers with examples and the necessary materials that will boost the success of their interventions.
Conclusion
This work provides a framework that will guide researchers in the design and implementation of mHealth-based behavior change interventions. It differs from its predecessors in that it goes beyond the conceptual level of intervention design by providing details about the technical implementation of mHealth solutions. Also, explanations and examples for different steps are provided to help researchers and practitioners and design, implement, and evaluate their mHealth-based behavior change interventions.
Keywords
Introduction
Human behavior is influenced by a synergic combination of psychological, physiological, social, economic, and cultural factors that collectively form individuals’ perceptions, decisions, and actions. Consequently, the complexity of changing any human behavior arises from the complexity of the behavior itself. Moreover, health-related behaviors require special attention given the importance of human health and its influence on people’s lives. 1 Therefore, addressing the change of any behavior requires powerful strategies based on evidence from theories and practices. This will help in the development of effective interventions that promote positive and improve negative behaviors.
Behavior Change Interventions (BCIs) for health, especially in developing countries, are challenging. First, the lack of a standardized common approach to developing interventions is a source of confusion for researchers. In addition, the lack of awareness regarding the importance of theories in interventions' design is challenging. 2 Moreover, some barriers hinder the success of interventions, such as poverty, funding issues, the spread of illiteracy, and lack of qualified human resources for the execution of the interventions. That's why, mHealth-based BCIs have the advantage of providing immense potential for reaching larger populations and fostering sustainable behavioral change. However, many existing mHealth solutions lack scientific evidence and customization, hindering their effectiveness.
Over the years, researchers and practitioners have developed several frameworks and models to guide BCIs, of which the most important are the Intervention Mapping (IM), 3 Behavior Change Wheel (BCW), 4 EAST framework, 5 and BASIC framework. 6 All of these frameworks have the same finality, which is to provide researchers with the steps to follow for the design of BCIs. However, there are some differences that influence their adoption in effective interventions. First, each identified framework involved different steps. In addition, one step in some frameworks is mapped to several steps in others. Furthermore, all frameworks stop at an abstract level of the design of the intervention by providing only the conceptual elements of behavior change and do not provide enough details regarding the concrete implementation of the intervention, especially in the case of those that are digital-based. Moreover, while all interventions discuss implementation and evaluations of the intervention, they provide general directives to recruit participants and evaluate the outcomes of the intervention, but ignore the Mode of Delivery (MoD) of the intervention that has a direct impact on how the intervention will be implemented and evaluated.
To address these issues, this paper presents a guide for designing, implementing, and evaluating evidence-based mHealth behavior change interventions. The proposed guide will assist researchers and practitioners in developing tailored interventions through a step-by-step process that integrates theory, practices, and digital innovation.
The remainder of this paper is organized as follows. The second section describes the methods used to synthesize existing frameworks for designing BCIs. The third section presents the different steps deduced from the synthesis of previous studies. Finally, the last section presents conclusions and future work.
Methodology
To have a unified process for developing BCIs, we conducted an integrative review by synthesizing previous empirical and theoretical studies and incorporating our experiences in developing behavior change interventions. Mainly, we provide a reconciliation between the commonly used frameworks of behavior change, namely, the Intervention Mapping (IM) framework, behavior change wheel (BCW), EAST framework, and BASIC framework.
Intervention mapping was developed primarily to plan health promotion programs such as HIV prevention, asthma management, and helping postpartum women stay off cigarettes. 3 The behavior change wheel (BCW) is a systematic method for intervention development centered on the COM-B Model, 4 it overcome the limitations of the existing methods and models for intervention development, and approximately 19 frameworks were selected to combine them into one framework. The EAST framework 5 employs four key principles (Easy, Attractive, Social, and Timely) to influence behavior effectively, emphasizing simplicity, attractiveness, social influence, and the appropriate timing of interventions. Finally, the BASIC framework, 6 introduced by the Organization for Economic Cooperation and Development (OECD), translates behavioral insights into actionable interventions for behavior change.
To conduct the mapping between different frameworks, we used an iterative approach, integrating the knowledge, experience, and skills of each of the authors. Therefore, the first and second iterations of mapping between several frameworks were conducted by the second and third authors. The first author then conducted a final iteration for the validation and correction of the proposed mappings. During each iteration, the authors examined in detail the different steps and stages of each framework, specifically reviewing what each step entails (the sub-steps,), and reviewing examples of their application to find similarities between different frameworks. Table 1 presents the mapping between the different frameworks, which provides five major steps. The first step is defining the scope of the intervention that will present all aspects of the intervention (target behavior, target population, context of the intervention) before proceeding with its design and implementation. The second step is devoted for the understanding and explanation of the behavior by referring to a behavior change theory. The third step involves defining the intervention content and strategies by providing a conceptual design for the intervention. The fourth step will proceed with the implementation of the intervention by translating the conceptual design into an effective mHealth solution. The fifth step is devoted to the evaluation of the intervention. Table A1 provides a concise description of the five steps with information about the sub-steps, options, and needed material.
Reconciliation between different steps in common frameworks of behavior change.

The next section describes in detail each step resulting from the mapping process between different frameworks, with some examples that will simplify their implementation for real use cases.
Results
Definition of the scope of the intervention
The first step in developing a behavior-change intervention involves a meticulous definition of the behavior to change. This step entails identifying the target behavior, the intended population for behavioral change, and the specific context in which the intervention will operate. Therefore, the intervention should encompass a clear understanding of the behavior to be altered (what behavior is the focus of change?), specific population to whom the intervention is directed (for whom is the behavior change intended?) and the contextual setting in which the desired behavior change occurs (under which circumstances is the behavior change sought?). To facilitate this process, researchers could conduct a preliminary studies to discover the features of the population concerned with the behavior. The following research questions are proposed to conduct the preliminary studies:
RQ1: What are the characteristics of the population affected by behavioral changes? RQ2: What are the overall characteristics of individuals in the population who have succeeded in changing their behavior? RQ3: What are the overall characteristics of individuals in the population who have failed to change their behavior? RQ4: Does the current state of the behavior/population necessitate the implementation of behavior change interventions?
Subsequently, researchers should provide a concise description of the scoop of their behavior change interventions. Researchers can use the Actor, Action, Context, Target, Times (AACTT) framework, 7 which considers human behavior as an action to be carried out by actors toward specific target in a specific context and during a specific timeframe.8,9 Below are three examples of the scope of intervention using the AACTT framework.
Example 1: Tobacco cessation
Actor: Adult smokers aged 18 and above Action: Quitting tobacco Context: The Workplace Target: Not applicable Time: During work hours
Example 2: Engagement in physical activities
Actor: Adult individuals Action: Doing regularly moderate-intensity sports Context: Anywhere Target: Not applicable Time: At least 10 min continuously
Example 3: Compliance with hygiene measures
Actor: All medical staff Action: Use alcohol-based hand gel Context: Patient room Target: Patient receiving care at the hospital Time: Before and after touching a patient
Understanding and explanation of the behavior
The most important step in the development of BCIs is the identification of behavioral determinants and understanding how they positively or negatively influence individuals’ motivation, decisions, and actions. Cane et al. 10 identified 112 theoretical constructs that characterize several behavioral aspects. Moreover, they categorized them into 14 theoretical domains. However, owing to the large number of constructs, researchers have developed many theories linking them to human behaviors. For instance, Michie et al. 11 identified 83 behavior change theories that can be used to understand and explain many human behaviors. However, few theories have been applied to behavioral health. Therefore, based on many literature reviews,12–22 we provide in Table 2, the theories that are the most used in different fields related to behavioral health. Specifically, for digital-based behavior change interventions, Taj et al. 23 identified the most used theories, namely, the social cognitive theory (29%), the transtheoretical model (10%), the self-determination theory (7%), the health belief model (5%), the theory of planned behavior (5%), and habit formation (5%). To identify fields related to behavioral health, we used the taxonomy proposed by Nudelman and Shiloh, 24 who performed hierarchical clustering of all existing health behaviors. Two main categories were identified: physical health behaviors and psychosocial health behaviors. The physical cluster comprises three sub-clusters: health maintenance, nutrition and exercise, and risk avoidance, while the psychosocial cluster includes one sub-cluster, known as general well-being.
Common theories for health behaviors.

Theories most reported in digital-based behavior change interventions.
Researchers have two options to obtain behavior explanations based on a theory of change. One common approach involves conducting a survey to assess the behavior. Alternatively, researchers can choose to conduct a meta-analysis of studies that have already used this theory to explain the behavior. 8
In the survey approach, researchers should develop or use a questionnaire to measure targeted behavior and its candidate determinants. Therefore, several studies have proposed guidelines for developing questionnaires based on many theories of change and for several health behaviors.7,25–29 The collected data from the survey will be fitted to the theory model to gain a good understanding of the possible connections between the behavior and its potential determinants.
In the meta-analysis approach, researchers should synthesize and integrate the results of all relevant studies that have already used the theory to understand targeted behavior. The results of the meta-analysis are presented in terms of the weighted effect sizes between the behavior and its candidate determinants.
Based on the results of the survey or meta-analysis, researchers should select the key determinants of the behavior with respect to the criteria of relevance that refers to the strength of the evidence for the association between each candidate determinant and the behavior. Crutzen et al. 30 provided a practical approach for selecting determinants based on the visualization of confidence intervals for the means and correlation coefficients for all determinants simultaneously.
Definition of the intervention content and strategies
Defining a process of change
Depending on the result of the previous step, the intervention designer may be solicited to define a process of behavior change that describes how the identified key determinants will conduct the user’s progression from one state to another until they reach the desired behavior. Therefore, the process of behavior change comprises different states and transitions, for which key determinants serve as essential activators. 31 Figure 1 illustrates a generic process of change in which the transition from state A to state B is achieved through transition evaluation. This evaluation can be conducted either directly by assessing behavior or outcomes, or indirectly by assessing one or more determinants. The assessment can be conducted by direct observation and monitoring of individuals or by asking them questions about the behavior or activators of the transition. If the assessment reveals that the transition can be established, we move on to the next transition.
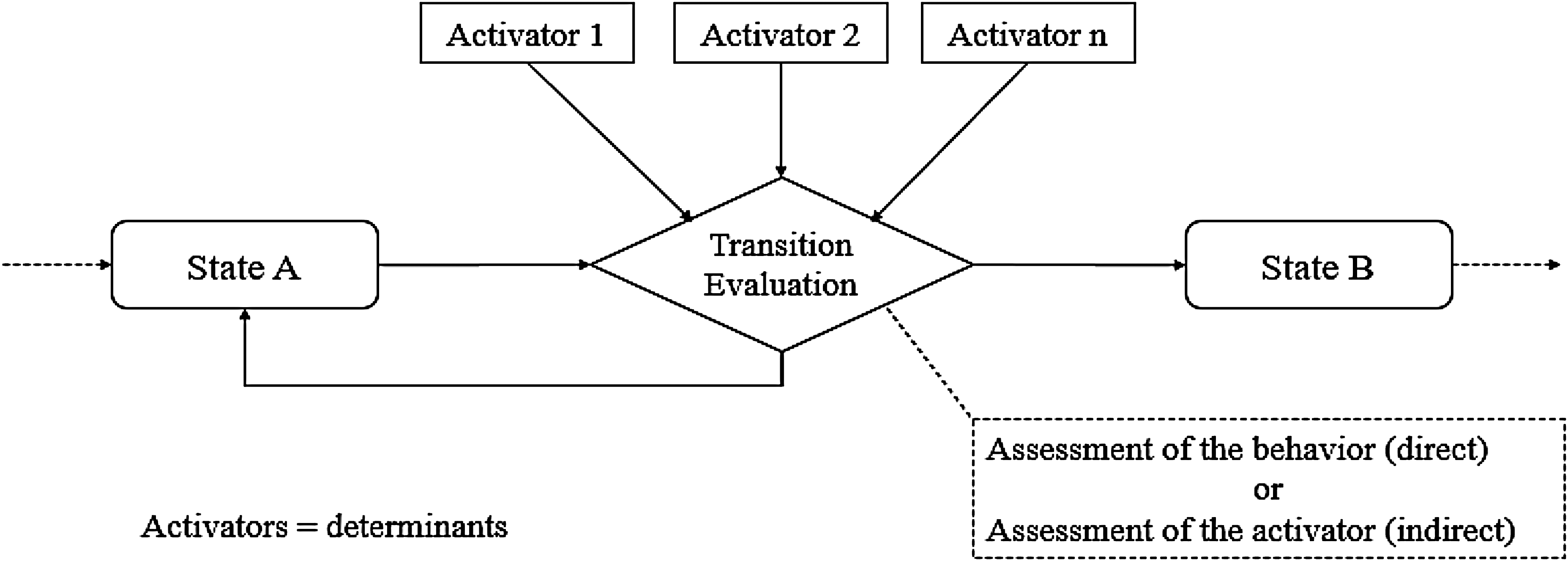
Synthesized model of the standard process of change.
Fenicio and Laurillau 31 emphasized that the process of change should be tailored by the theory that was used to understand the behavior, they also described the processes of change for some change theories. For instance, Figure 2 is an example of the process of change related to the theory of planned behavior (TPB). The first transition from intention not formed to intention formed is directed by three determinants (activators): attitude, subjective norms, and perceived behavioral control (PBC). Afterward, the second transition to the state “behavior performed” is moderated by PBC. Indeed, intervention designers should carefully define the roles that control the realization of transitions from one state to another by the moderation of activators.
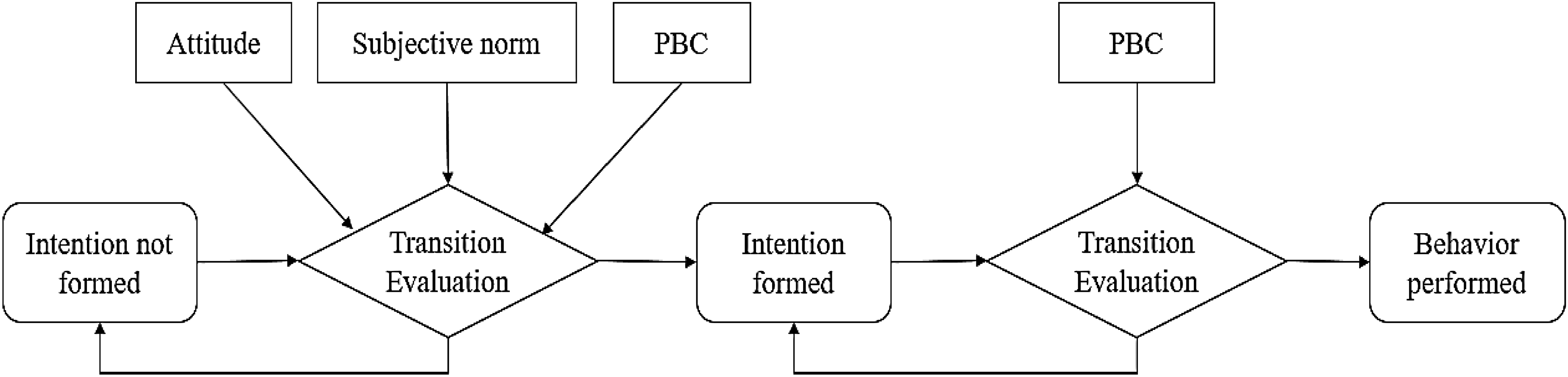
Example of the process of change related to TPB.
Selection of behavior change techniques
BCT Taxonomy:
After defining the process of change, the designer should select appropriate intervention components that will be used concretely for behavior regulation and improvement. These components will be considered as inducers of different activators (key determinants) and represent the building blocks of the behavior change intervention. For this purpose, Michie et al. 4 developed a taxonomy of 93 behavior change techniques (BCTs) by which behaviors can be changed. 32 The selection of the most appropriate BCTs should consider the key determinants of behavior, characteristics of the targeted behavior (physical or psychosociall), the features of the target population (gender, age, culture, etc.), and the selected mode of delivery (MoD) for the intervention.
Michie et al. conducted several studies to identify relevant links between BCTs and all behavioral constructs derived from theories. First, they identified 26 mechanisms of action (MoAs) that represent all relevant behavioral constructs corresponding to the 14 theoretical domains of the theoretical domains framework (TDF), in addition to 12 constructs derived from the 83 theories of change. Subsequently, they identified links between BCTs and MoAs based on published intervention articles and expert consensus. Consequently, they identified 92 BCT–MoA links covering 75 BCTs and 26 MoAs.
33
BCTs adapted to target Behavior: BCTs adapted to target population: BCTs adapted to the MoD:
For targeted behavior, a common approach is the consideration of evidence from previous studies (experiments, meta-analyses, correlational studies, meta-regression, and meta-CART) to select the appropriate BCTs. Therefore, many previous studies have provided the most popular BCTs for several behaviors such as smoking,
34
physical activity,35,36 sleep,
37
driving behavior,38,39 and work.
40
For the target population, the criteria of acceptability can be assessed for each relevant BCT.
8
If applicable, intervention designers can conduct a survey or interview with a sample of the target population and/or stockholders to provide a final list of appropriate BCTs for each determinant of behavior.
For the possible MoDs of behavioral interventions, Marta et al.
40
developed a mode of delivery ontology that contains 15 main categories with several subcategories, from which one subcategory is dedicated to electronic mods of delivery with a total of 16 MoDs, including mobile application mode of delivery. In addition, Abraham and Michie
41
provided BCTs that were adapted to several modes of delivery. However, Van Genugten et al.
42
conducted a study to determine possible combinations of BCTs and MoDs and they concluded that there were no synergistic effects for MoDs combined with BCTs. Subsequently, intervention designers are free to choose any BCT-MoD combination for the implementation of their behavioral intervention.
For mHealth-based interventions, and based on previous literature studies,42–46 we noticed that only 12 of the 93 BCTs are the most used for the design of interventions, and only six were identified in interventions reported as effective in changing behaviors. The decision on effectiveness was based on the information reported in studies.42,44,45 Table 3 describes the 23 most used BCTs for mHealth-based BCIs.
Synergic combinations of BCTs:
The most used BCTs for mHealth-based behavior change intervention.

To identify synergic combinations of BCTs, Dusseldorp et al. 47 and Van Genugten et al. 42 conducted meta-analyses of the results obtained from several intervention studies. They affirmed that the combination of several BCTs in the same intervention maximized its effectiveness. However, their results do not provide large choice of BCTs for future interventions because most of the 93 BCTs have not yet been tested in real interventions. Consequently, intervention designers should not be limited to the results of these meta-analyses and should consider all BCTs that are adapted to their intervention characteristics.
Implementation of the intervention
Preliminary study
During the implementation step, the intervention designer should inspect the context in which the intervention will be conducted by considering the laws that might have to be respected, ethical issues, and the cultural and social aspects that might constitute barriers to the eventual implementation of the intervention. Also, the intervention designer should plan strategies to overcome all the estimated barriers. For instance, the designer can adopt one of the well-known ethical guidelines, namely, the International Behavior Analysis Organization’s (IBAO) Ethical Guidelines, the American Psychological Association (APA) Ethical Guidelines, the World Health Organization (WHO) Ethical Guidelines, or the National Institutes of Health (NIH) Guidelines.
In addition, the designer should estimate the necessary human and financial resources; this estimation is crucial for the success of the intervention and ongoing support. For example, a digital intervention might need a budget to pay for certain services, or it might need human resources to aid in the management of incidents related to the digital solution that constitutes the intervention. 3
Afterward, the intervention designer and development team should assess the adequation of proposed BCTs with contextual features of the implementation of the intervention (ethical issues and human and financial resources) and reconsider choices that are inadequate. Therefore, the APEASE (Affordability, Practicality, Effectiveness and cost-effectiveness, Acceptability, Side-effects/safety, and Equity) criteria can be used to determine which BCTs are most appropriate to the intervention. 48 Possibly, this evaluation can be conducted at an early stage of the design of the intervention by looking at similar interventions that have been implemented and/or expert evaluation. 48 Table B1 describes the APEASE criteria, while Table B2 provides an example of the APEASA grid for assessing the adequation of intervention elements.
Finally, the designer should provide the requirements specifications of the solution by providing both the system and user requirements. This is frequently described in the form of functional and non-functional requirements. Functional requirements describe the functions of a system that satisfy user needs. However, non-functional requirements rely on constraints to be fulfilled by the system, such as reliability, availability, security, maintainability, and portability.
BCT operationalization
During the implementation step, the development team will follow a user-centric design strategy by considering the heterogeneity of users from an earlier stage of the implementation process. This can be achieved by developing a self-adaptive mHealth solution that should autonomously handle variations in the environment and system and ensure the monitoring of user actions. 49 To implement these specifications, the self-adaptive mHealth solution is enriched with dynamic components and equipped with adaptable features to enhance user experience.49,50 These components can automatically and continuously be added, changed, or removed depending on the user’s goal. Figure 3 shows a typical flow of handling user progression through various behavior states.

Flow example of user progression.
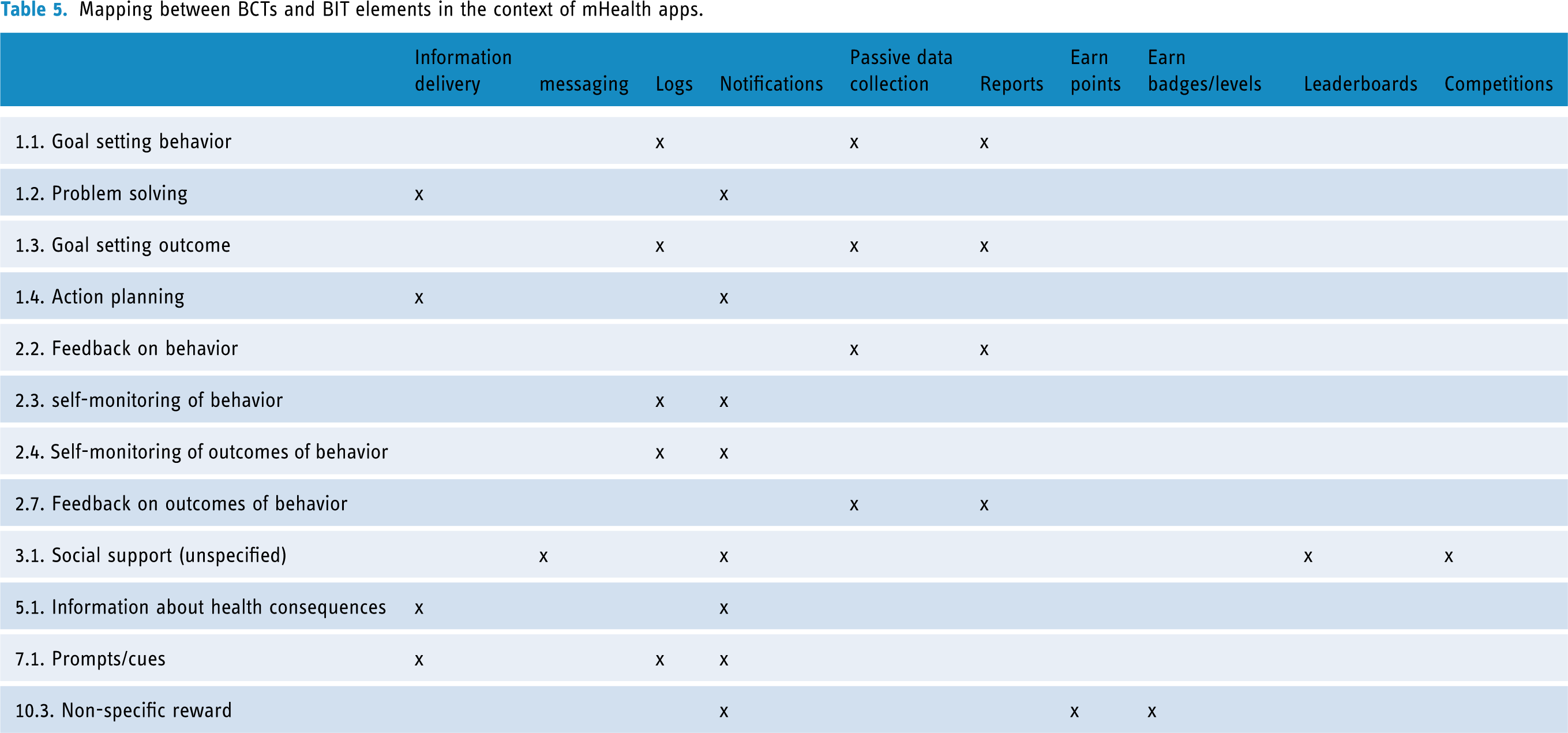
The components correspond mainly to the operationalization of BCTs to behavioral intervention technology (BIT) elements, which correspond to technological components that will concretely implement conceptual BCTs. In the literature, we identified six principal BITs that are adapted to mobile applications: information delivery, messaging, logs, notifications, passive data collection, and reports.51–54 Moreover, Dugas et al. 45 suggested the addition of gamification elements (earn points, earn badges/levels, Leaderboards, and Competitions) to enhance the effectiveness of mHealth solutions in changing behaviors. Also, several studies have demonstrated the effectiveness of gamification elements in improving individuals’ motivation and engagement.55–58 Table 4 presents descriptions of the BIT elements adapted to mobile applications. In addition, Table 5 provides possible operationalizations of the 12 BCTs most commonly used with mHealth interventions to BITs and gamification elements.
The BITs adapted to mobile apps.

Mapping between BCTs and BIT elements in the context of mHealth apps.
Development and testing of the mHealth solution
The development team will proceed with the implementation of the designed mHealth solution by providing friendly user interfaces and ensuring a good user experience. In addition, before delivering the developed mobile app to the largest target population, the intervention designer and development team can provide an early evaluation of the intervention by assessing APEASE criteria (using Table B1). This will help in detecting barriers to the success of the intervention and resolving them early, so they do not hinder the achievement of desired outcomes of the intervention.
Eventually, before delivering the developed mobile app to the largest target population, it should be tested on a smaller scale. Therefore, a representative sample of the target population is considered when performing several preliminary tests throughout the project lifecycle. Afterwards, the intervention team should provide a usability assessment of the application by using one of the commonly used usability metrics for mobile apps, for instance, mGQM, 59 ISO9241, 60 and PAQMAD. 61
Evaluation of the intervention
Evaluation criteria
Evaluation is a crucial element in behavior change interventions. This involves assessing the impact and effectiveness of the delivered intervention. This is accomplished through the integration of a monitoring system within the mHealth solution, which enables the evaluation of the intervention success. The key questions addressed in this step include measuring and assessing the outcomes of the intervention and whether it has achieved its intended effect. 39 The APEASE criteria are used again at this stage. However, as shown in Table B1, the assessment of different criteria will differ from the design and implementation stage. Therefore, the criteria of affordability, practicability, and acceptability can be assessed through surveys or administrative information. However, the criteria for effectiveness, side effects, and equity can be assessed through randomized or non-randomized trials. 62 Most interventions focus on effectiveness, side effects, and equity as principal elements for measuring intervention outcomes.
Measuring the outcomes of the intervention
The outcomes of the intervention, whether primary or secondary, can be collected automatically from the mobile app or by providing questionnaires to the intervention participants. The primary outcome measure will assess either directly or indirectly the targeted behavior. However, secondary outcomes are used to provide a deeper interpretation of the primary outcomes. For example, in interventions for physical activities, primary outcomes will be related to the current engagement of individuals in physical activities; however, secondary outcomes will be related to body mass index (BMI), blood pressure (BP), and mental health. It should be noted that outcome measurements will be conducted while respecting ethical issues, mainly by respecting the privacy of participants and anonymizing collected data. Table 6 presents an example of the outcome measurement of the intervention for promoting physical activity.
Example of outcomes measurement of intervention about engagement in physical activities.

Adapted from the GPAQ. 63
Assessing the outcomes of the intervention
Before proceeding to the collection of data on the outcomes of the intervention, it is crucial to choose an adequate method to assess the effectiveness, side effects, and equity of the delivered intervention. Usually, two methods are used: randomized controlled trials (RCT) 64 and before-and-after methods. 65
A Randomized Controlled Trial (RCT) consisted of randomly choosing people to evaluate the outcomes of the intervention and comparing the results with a control group. Participants are randomly assigned to two groups to ensure greater reliability in the assessment of the outcomes of the intervention.
Before-and-after method (also called pre-post method) considers only one group of individuals for which we provide an evaluation of the behavior before and after the intervention. Any change in the outcomes can be attributed to the intervention. Although RCT is more reliable than the before-and-after method, it is not always possible to perform it. This is mainly because RCT are more expensive and less flexible than the before-and-after method.
After the evaluation of the intervention, designers should report the intervention findings by following common reporting guidelines. For instance, the Consolidated Standards of Reporting Trials (CONSORT) 66 is recommended for randomized studies. However, Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) 67 is recommended for nonrandomized studies.
Conclusion
This study provides a comprehensive framework for the design and implementation of mHealth-based behavior change interventions. First, we reconciled common frameworks of behavior change by mapping their different steps. The reconciliation provided five steps: definition of the scope of the intervention, understanding and explanation of the behavior, definition of the intervention contents and strategies, implementation of the intervention, and evaluation of the intervention.
Moreover, based on our experience in developing behavior change interventions in the health field, we provide explanations and examples for different steps by referring to theories, taxonomies, materials, tools, and techniques that will help designers and developers in the implementation of their interventions.
By following the steps of the proposed framework, researchers and practitioners will be able to design, implement, and evaluate mHealth-based behavior change interventions, guided by theories and evidence from previous research. However, researchers and practitioners should develop their own experiences in the design and implementation of behavior change interventions. This indicates that they should choose from the different options proposed in the framework that are adapted to their goals, experiences, target behaviors, and target populations.
Footnotes
Acknowledgments
Not applicable.
Author note
Ali Idri is also affiliated with Mohammed VI Polytechnic University, Ben Guerir, Morocco.
Contributorship
TR: conceptualization, investigation, writing—original draft, and writing—review and editing. AE: investigation and writing—original draft. MA: investigation and writing—original draft. AI: validation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
TR.
Informed consent
Not applicable. The study does not require consent, as it does not involve patients’ participation.
Appendix A
Steps for developing mHealth-based behavior change interventions.

| Steps | Substeps | Description | Options/material |
|---|---|---|---|
| Step 1 Definition of the scope of the intervention |
1.1. Conduct the primary studies to discover target behavior and target population. | Responds to the following Research questions:
RQ1: What are the characteristics of the population affected by the behavior to be changed? RQ2: What are the overall characteristics of the individuals in the population who have succeeded in changing their behavior? RQ3: What are the overall characteristics of the individuals in the population who have failed to change their behavior? RQ4: Does the current state of the behavior/population necessitate the conduction of behavior change intervention? |
|
| 1.2. Define the scope of the intervention by using the AACTT framework. | Define the following elements:
Actor: individual(s) performing the action Action: Description of behavior to be changed or to be maintained. Context: physical location, emotional context or social settings in which the action is performed. Target: individual(s) with/for him the action is performed Time: when the action is performed |
||
| Step 2 Understanding and explanation of the behavior |
2.1. Choose appropriate behavior change theory for the understanding of the behavior. | Conduct a literature review for the determination of the adequate theory | See Table 2 about common theories for health behaviors. |
| 2.2. Identify the key determinants of the behavior. | Use of the selected theory for the understanding and explanation of the behavior. | 2.2.1. Conducting a survey for the assessment of the behavior. | |
| 2.2.2. Conducting a meta-analysis of studies that have already used the theory to explain the behavior | |||
| Step 3 Definition of the intervention content and strategies |
3.1. Define a process of change for the target behavior. | Define the flow of transitions between different states of the behavior. | |
| 3.2. Identify candidate BCTs for each key determinant of the behavior. | BCT-MoA tool: https://theoryandtechniquetool.humanbehaviourchange.org/tool |
||
| 3.3. Select appropriate BCTs for each key determinant. | Exclude BCTs that aren’t adequate with intervention properties. | 3.3.1. Exclude BCTs not appropriate to target behavior. | |
| 3.3.2. Exclude BCTs not appropriate to target population. | |||
| 3.3.3. Exclude BCTs not adapted to the chosen MoD. | |||
| Step 4 Implementation of the intervention |
4.1. Determine, ethical issues | Determine laws, ethical issues, cultural and social barriers for the implementation of the interventions and how to overcome them. | Use one of the following guidelines :
IBAO Ethical Guidelines APA Ethical Guidelines WHO Ethical Guideline NIH Guidelines |
| 4.2. Evaluate necessary human and financial resources. | |||
| 4.3. Evaluate selected BCTs according to APEASE criteria. | Use material in Appendix B | ||
| 4.4. Describe functional and non-functional requirements. | Provide Software requirement specifications document | ||
| 4.5. Provide general design/architecture of the mobile app. | |||
| 4.6. Implement the mobile app. | |||
| 4.7. Provide testing of the mobile app on a small scale | Recruit some typical profiles for providing primary testing of the mobile app | 4.7.1. APEASE criteria | |
| 4.7.2. Usability criteria | |||
| Step 5 Evaluation of the intervention |
5.1. Measuring the Outcomes of the intervention | Collect data about primary and/or secondary outcomes of the intervention | 5.1.1. Use of mobile phone sensors/smartwatch/smart bracelet to measure outcomes of the intervention. |
| 5.1.2. Through questionnaires. | |||
| 5.2. Assessing the outcomes of the intervention | Assessing the outcomes of the intervention by using randomized or nonrandomized trial | APEASE criteria | |
| 5.3. Reporting of the result of the intervention | Reporting and dissemination of the results of the intervention | 5.3.1. Using CONSORT guidelines for reporting randomized studies. | |
| 5.3.2. Using TREND Guidelines For Reporting Nonrandomized Studies. |
Appendix B
Matrix to assess APEASE criteria.

| Intervention or Intervention elements (BCTs, MoDs) | Affordability |
Practicality |
Effectiveness |
Acceptability |
Side-effects |
Equity |
Does the intervention (element) meet the APEASE criteria? |
|---|---|---|---|---|---|---|---|