
Abstract
Objectives
This study aims to investigate whether social networks and physical exercise mediate the relationship between new and constant use of intelligent virtual assistants (IVAs) and cognitive function in older adults in China and explore the potential differences across living arrangements and education levels.
Methods
This study utilized nationally representative longitudinal data from 2018 to 2020, including a sample of 8343 older adults aged 60–80. A path-analytic model was employed to examine the relationship between IVAs use and cognitive function, as well as the mediating roles of social networks and physical exercise.
Results
Constant and new IVAs use significantly affected cognitive function, mediated by social networks and physical exercise. For older adults living alone, both types of IVAs use had positive direct and indirect effects. Those living with children benefited mainly from new IVAs use, with indirect effects through physical exercise. Among less educated older adults, only new IVAs use showed significant effects through social networks. For those with higher education, both constant and new IVAs use positively impacted cognitive function directly and indirectly.
Conclusions
The use of IVAs can significantly improve cognitive function in older adults, with social networks and physical exercise being important mediating pathways. Policy suggestions were provided based on these results.
Introduction
In recent years, the rapid advancement of information and communication technologies has significantly transformed various aspects of daily life, including healthcare. 1 The development and proliferation of digital technologies have emerged as promising solutions for health promotion and disease prevention of older adults. 2 These technological innovations, encompassing smart wearable sensing technologies and smart home digital systems, offer numerous applications such as remote health monitoring, telemedicine, and digital health interventions, thereby addressing the unique health challenges faced by the aging population. 3 Several studies have explored the relationship between technology use and older adults’ health, highlighting their positive impacts on physical, cognitive, and social well-being.4,5 For instance, previous research has demonstrated that smart home devices can improve safety and independence, 6 while wearable health monitors can facilitate better management of chronic conditions. 7 Additionally, digital platforms for social interaction can mitigate feelings of loneliness and social isolation, further contributing to overall health improvements among older adults. 8
Intelligent virtual assistants (IVAs) are advanced artificial intelligence-driven systems designed to perform a wide range of tasks through voice, text, or gesture commands, often integrated with smart home systems. 9 Examples include popular platforms like Amazon's Alexa, Apple's Siri, and Google Assistant, as well as China's Baidu Xiaodu and Alibaba's Tmall Genie. IVAs can perform various functions such as setting reminders, controlling smart home devices, providing weather updates, and answering questions. 10 Despite their widespread adoption and diverse functionality, research on the health impacts of IVAs remains relatively limited. IVAs have the potential to support aging by assisting older adults in managing their daily health routines, providing reminders for medication, facilitating communication with healthcare providers, and offering cognitive exercises. 11 A few empirical studies have started to explore these possibilities. IVAs use has been proved to be associated with lower depression and loneliness of older adults living alone. 12 In a two-stage Delphi study, the experts agreed with the potential of IVAs to support older adults and be widely used as anamnesis, informational, self-therapy, and communication tools by patients and healthcare professionals. 13 A case–control cohort study demonstrated that the use of IVAs enhances memory, executive function, and working memory abilities, inhibiting cognitive decline in older adults. 14
Despite the promising findings, the mechanisms through which IVAs impact cognitive function remain underexplored. Existing research has established that social networks and physical exercise significantly contribute to the cognitive health of older adults. Social networks have been shown to enhance cognitive reserve, reduce the risk of dementia, and improve overall mental health. 15 Similarly, regular physical exercise is associated with better cognitive function, delayed onset of cognitive decline, and improved brain health. 16 Given these established benefits, it is plausible that IVAs use could positively influence cognitive function by promoting social interaction and encouraging physical activity. IVAs can facilitate communication with family and friends, provide reminders for social activities, and offer virtual companionship. 17 Additionally, IVAs can support physical exercise routines by offering reminders, tracking progress, and providing guided exercise programs. 18 Thus, the potential of IVAs to impact cognitive function through these pathways warrants comprehensive research to fully understand their benefits and mechanisms of action.
The potential impact of IVAs use on cognitive function can be understood through several theoretical lenses. The technological reserve hypothesis suggests that exposure to and engagement with technology can build cognitive resilience, relieving feelings of social isolation, and potentially enhancing cognitive function in later life. 19 In this context, IVAs may serve as a technological tool that contributes to cognitive reserve, strengthening social networks, and promoting physical exercise, thereby positively influencing cognitive function. According to cognitive plasticity theory, the brain undergoes structural and functional changes in response to new challenges or learning new skills, with these changes being more pronounced in the short term. However, if the stimuli remain constant, the neural system gradually adapts, leading to diminished effects over time. 20 As new users navigate the unfamiliar terrain of IVAs, they may experience more intense cognitive engagement than constant users who have already adapted to the technology. The uses and gratifications theory emphasizes that individuals actively choose and use media to satisfy specific needs, implying that the benefits derived from IVAs use may vary depending on individual circumstances and capabilities. 21 On the one hand, regarding living arrangements, older adults living alone often experience a lack of social interaction and face higher risks of depression and mental health issues. 22 For older adults living apart from their children, there is a greater reliance on external social tools to meet their social participation needs. IVAs can serve as a crucial tool for maintaining and enhancing social connections, thus potentially yielding stronger cognitive benefits. On the other hand, regarding education levels, older adults with lower education levels may face more challenges in understanding and adapting to new technologies, 23 making the cognitive benefits of IVAs use less apparent. In contrast, older adults with higher education levels have stronger learning abilities and adaptability to new technologies. 24 They can more quickly grasp and utilize various functions of IVAs, which may offer more diverse and complex cognitive engagement opportunities, resulting in more pronounced cognitive benefits compared with their counterparts.
Despite growing research on IVAs’ benefits for older adults, several limitations exist in current literature. Most studies use cross-sectional data or small-scale interventions, limiting understanding of long-term effects. Few have explored potential mediating mechanisms like changes in social networks and physical activity. The heterogeneity in IVAs’ effects across subgroups of older adults with varying living arrangements and education levels remain underexplored. Additionally, most research focuses on Western populations, leaving a gap in understanding how findings apply to other cultural contexts, such as China, where family dynamics and technological adoption may differ. This study uses a large-scale, longitudinal dataset from China to address these gaps through the following research questions:
What is the longitudinal relationship between constant and new IVAs use and cognitive function among older adults in China? Do social networks and physical exercise mediate the relationship between IVAs use and cognitive function? Do the effects of IVAs use on cognitive function vary based on living arrangements (not living with children vs. living with children) and educational levels (primary education and below vs. those with junior high education and above)?
Methods
Data and sample
This study utilizes data from the China Longitudinal Aging Social Survey (CLASS), a nationwide, longitudinal project covering 476 villages across 30 Chinese provinces. CLASS collects systematic data on the social and economic backgrounds of individuals aged 60 and above, aiming to understand aging challenges and assess the effectiveness of related social policies. The survey, initiated in 2014 with biennial follow-ups, provides crucial theoretical and empirical foundations for addressing aging issues in China. Since 2018, CLASS has included data on smart health aging product usage among older adults, offering a basis for formulating rational and effective smart aging policies. Written informed consent was obtained from all participants prior to their involvement in the survey.
For the current analysis, we included data from two waves in 2018 and 2020. Participants aged over 80 were excluded due to two primary reasons. First, health issues and cognitive decline are more prevalent in this age group, which could confound the analysis of smart health aging product usage. Second, older adults over 80 are generally less likely to adopt smart products, resulting in very low ownership rates (approximately 1.65%). These factors could introduce significant biases and affect the robustness of our findings. Given the considerable proportion (12.69%) of missingness in the depressive symptoms covariate, mean imputation was employed to address these missing values. For other variables where the extent of missingness was minimal, we applied listwise deletion, excluding cases with incomplete data on these variables. Additionally, 1479 participants were lost to follow-up between the two waves. To evaluate potential attrition bias, we performed a comparative analysis of baseline characteristics between the final analytical sample and participants lost to follow-up. The results of this analysis are presented in Table S1 in the Supplementary Material. Finally, 8343 samples were included in this study. Figure 1 shows the detailed procedure for the inclusion and exclusion of the participants.
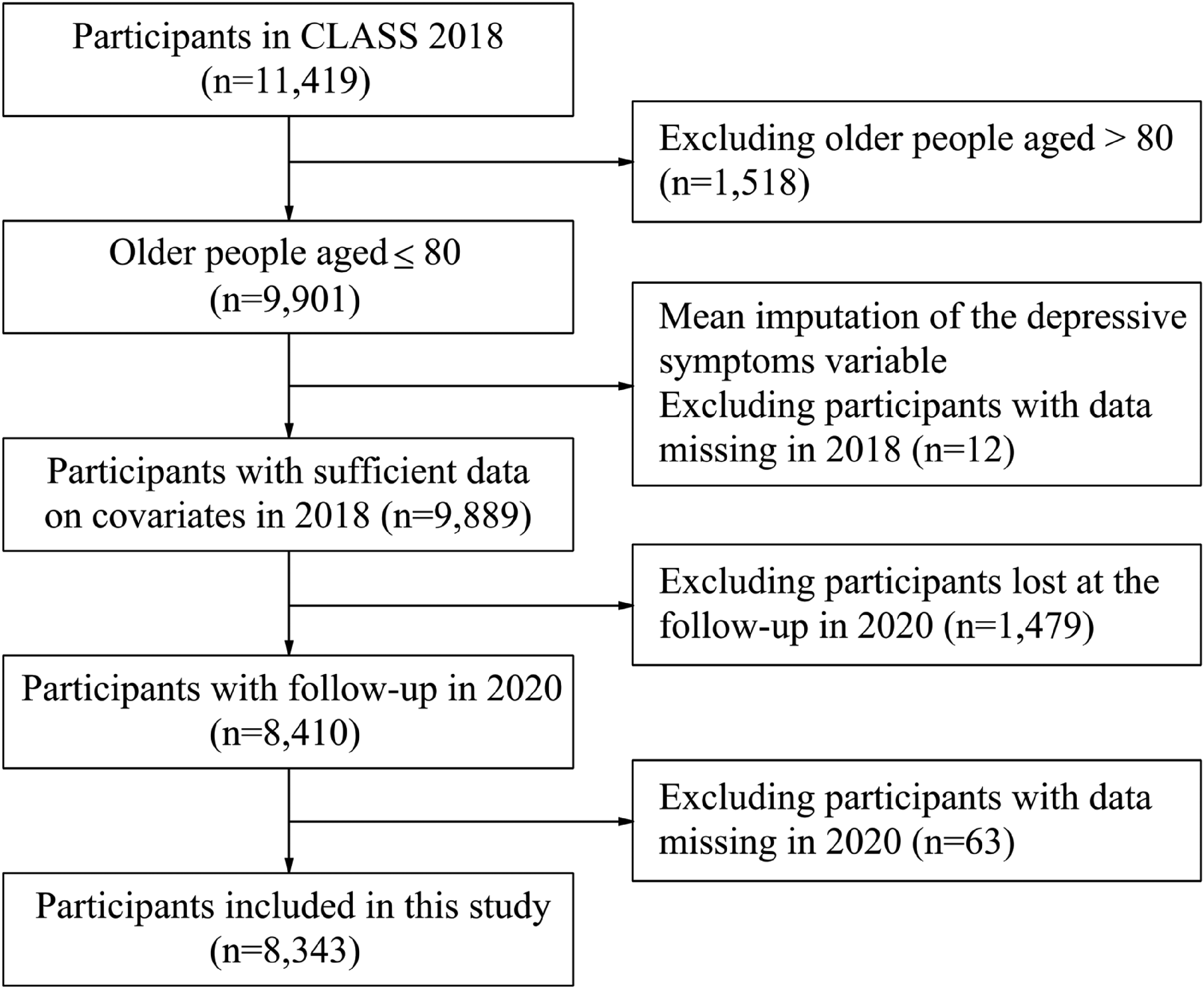
The flowchart of the inclusion and exclusion of the study population.
Measurements
Cognitive function
Cognitive function, including orientation, memory, and calculation, was assessed using a modified Chinese version of the Mini-Mental State Examination. 25 Orientation was evaluated with five questions, asking respondents for details such as the current date, the name of their village, the date of National Day, the current president's name, and the lunar calendar year. Each correct response earned 1 point, while incorrect responses scored 0, leading to an orientation score range from 0 to 5. Memory was tested using immediate and delayed word recall tasks. Participants were asked to recall three simple Chinese words right after hearing them and again after a few minutes. The scores from these tasks were summed, resulting in a total memory score range from 0 to 6. Calculation ability was measured by having respondents count backward from 100 by 7 s, repeated five times. This task was scored from 0 to 5. The aggregate of these three components—orientation, memory, and calculation—provided an overall cognitive function score ranging from 0 to 16, with higher scores indicating better cognitive performance. The Cronbach's α coefficient for the scale in 2020 was .827.
Use of IVAs
The use of IVAs was measured using a dichotomous variable derived from the survey question: “Do you use intelligent virtual assistants (such as Baidu's Xiaodu or Xiaomi's Xiaoai)?” Respondents who answered “yes” were assigned a value of 1, and those who answered “no” were assigned a value of 0. Following previous research, we operationalized it into categorical variables based on usage patterns over two survey waves. 26 The classification of IVAs use was defined as follows: “nonusers” were participants who reported not using IVAs in both the 2018 and 2020 surveys (i.e., answered “no” in both waves), “new users” were participants who reported not using IVAs in the 2018 survey but indicated usage in the 2020 survey (i.e., transitioned from “no” to “yes”), and “constant users” were participants who reported using IVAs in both the 2018 and 2020 surveys (i.e., answered “yes” in both waves).
Social networks
The social networks variable was measured using data from 2020, employing the Lubben Social Network Scale. 27 This measure consists of two dimensions: family networks and friend networks, which are combined to form the overall social networks score. Family networks were measured by three items: the number of people who were able to interact monthly, discuss personal issues, and seek help. Responses (none = 0; one = 1; two = 2; three to four = 3; five to eight = 5; nine or more = 9) were summed up into a total score, with higher scores indicating more robust family networks. Friend networks were measured similarly to family networks, using the same items and response coding. The total social network score was the sum of the family and friend network scores, reflecting the overall social connectivity of the respondents. The Cronbach's α coefficient for the scale was .858 in this study.
Physical exercise
The physical exercise variable was measured using data from 2020. Respondents were asked about the frequency of their participation in physical exercise with the question: “How often do you engage in physical exercise?” Responses ranged from “less than once a month” to “seven or more times a week,” scored on a scale from 1 to 9. Higher scores indicated more frequent participation in physical exercise. This variable was operationalized as a continuous variable to reflect the varying levels of exercise frequency among participants.
Covariates
Referring to previous studies,12,26 we controlled for three kinds of covariates that could potentially influence both IVAs use and cognitive function: (1) demographic characteristics, including gender (female = 0, male = 1), age (continuous variable of 60–80 years), years of schooling (continuous variable of 0–16 years), marital status (single, divorced, widowed = 0, living with a spouse = 1), residence patterns (not living with children = 0, living with children = 1); (2) socioeconomic factors, including hukou status (rural hukou = 0, urban hukou = 1), employment status (unemployed = 0, currently working = 1), pension coverage (has no pension = 0, has a pension = 1), internet access (noninternet user = 0, internet user = 1); (3) health-related factors, including body mass index (continuous variable of 15.03–36.00), self-rated health (continuous variable of 1–5), chronic disease (not have = 0, have at least one chronic disease = 1), T1 cognitive function (continuous variable of 0–16), and depressive symptoms (continuous variable of 0–18). It is important to note that we specifically included T1 cognitive function as a control variable to account for baseline cognitive abilities. This approach allows us to effectively control for the potential confounding effect of initial cognitive status on the relationship between IVAs use and subsequent cognitive outcomes. Depressive symptoms score was measured by the Centre for Epidemiologic Studies Depression scale, which is a short self-report scale with nine items based on the original Centre for Epidemiologic Studies Depression scale comprised of 20 items. 28 The total score ranges from 0 to 18, with higher scores indicating greater depression. The Cronbach's α coefficient for the scale was .918.
Statistical analysis
Descriptive statistics were calculated to compare the characteristics of nonusers, new users, and constant users of IVAs. Chi-square tests for categorical variables and t tests for continuous variables were used to assess differences between groups, with nonusers as the reference group. To examine the relationships among IVAs use, social networks, physical exercise, and cognitive function, we conducted a path-analytic model approach using structural equation modeling for observed variables. This methodology has been widely applied in numerous studies due to its ability to simultaneously estimate multiple relationships between variables and test complex mediation models. 29 The mediation models were examined with the lavaan package in the open source software R, 30 employing the maximum likelihood method for estimating model parameters. 31 In our path-analytic model, we controlled for all covariates not only for their potential effects on the outcome (cognitive function) but also on the mediators (social networks and physical exercise).
We first conducted a single-group path analysis on the total sample to test the hypothesized parallel mediation model. Multigroup path analyses then investigated potential differences based on residence patterns and educational level. For each analysis, we estimated direct, indirect, and total effects of constant and new IVAs use on cognitive function, with social networks and physical exercise as mediators. All path analyses controlled for relevant covariates. Standardized parameter estimates with 95% confidence intervals (CIs) were reported. The effect was regarded as statistically significant if the 95% CI excluded zero. Model fit was assessed using the following indices: comparative fit index, Tucker-Lewis index, root mean square error of approximation with 95% CI, and standardized root mean square residual.
Results
Descriptive findings
Table 1 compares the attributes of different IVAs users: nonusers, new users, and constant users, using nonusers as the reference group for statistical tests. The majority of the sample consisted of nonusers (n = 7977), while new users and constant users comprised smaller subgroups (n = 229 and n = 137, respectively). Compared to nonusers, both new users and constant users demonstrated significantly higher cognitive function scores (14.90 vs. 13.42 and 14.50 vs. 13.42, respectively), social networks scores (15.77 vs. 14.17 and 15.26 vs. 14.17, respectively), and physical exercise frequency (6.55 vs. 3.46 and 5.08 vs. 3.46, respectively).
Descriptive statistics of the sample characteristics (N = 8343).

Note: The reference group is nonusers. BMI: body mass index. *p < .05. **p < .01. ***p < .001. †p < .1.
Of three types of IVAs users, nonusers were the oldest group on average (mean age = 68.76 years) and had the fewest years of schooling (mean = 5.71 years). They were less likely to have an urban hukou status (42.74%) compared to the other two groups and had the lowest proportion of internet users (19.13%). In terms of living arrangements, nonusers had the lowest percentage of individuals living with a spouse (74.61%) and the highest percentage living with children (30.89%). They were more likely to be currently working (29.36%) compared to new and constant users but had the lowest pension coverage (74.40%) among the three groups. Regarding health-related factors, nonusers had the lowest cognitive function scores (mean = 13.30) at Wave 1 among the three groups. They had a lower average body mass index (mean = 22.40) and higher depressive symptoms (mean = 6.64) than new users. Their self-rated health (mean = 3.36) and chronic diseases prevalence (72.97%) was lower than new users but higher than constant users.
Single-group path analysis
A single-group path analysis was conducted to estimate the parallel mediation model. The fit indices demonstrated that the model had a satisfactory fit (comparative fit index = 0.998, Tucker-Lewis index = 0.902, root mean square error of approximation = 0.038, 95% CI = 0.021, 0.057, standardized root mean square residual = 0.003). Specifically, the model explains 46.6% of the variance in the cognitive function among older adults in China. Figure 2 presents the results for the standardized solutions based on the mediation model in the total sample. The direct, indirect, and total effects are presented in Table 2.

Standardized parameters for the mediation model in the total sample (n = 8343).
Standardized direct, indirect, and total effects in single-group path analysis (total sample).
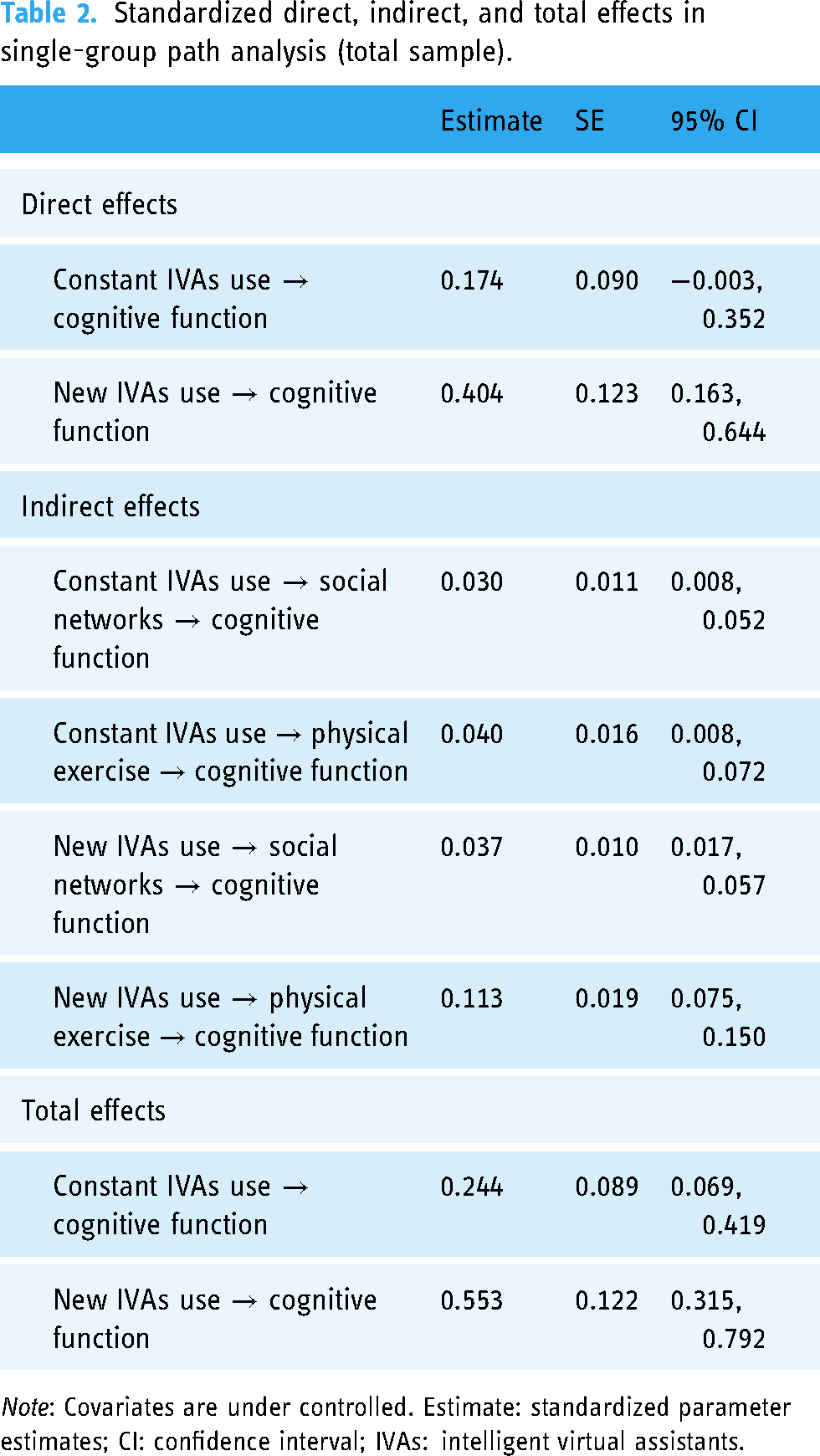
Note: Covariates are under controlled. Estimate: standardized parameter estimates; CI: confidence interval; IVAs: intelligent virtual assistants.
New IVAs use showed statistically significant positive direct effects on cognitive function (β = 0.404, 95% CI = 0.163, 0.644, respectively). Meanwhile, all indirect paths from IVAs use to cognitive function through social networks and physical exercise were statistically significant. For constant IVAs use, the indirect effects through social networks and physical exercise were 0.030 (95% CI = 0.008, 0.052) and 0.040 (95% CI = 0.008, 0.072), respectively. For new IVAs use, the indirect effects through social networks and physical exercise were 0.037 (95% CI = 0.017, 0.057) and 0.113 (95% CI = 0.075, 0.150), respectively. Moreover, statistically significant total effects of both constant and new IVAs use on cognitive function were observed. Constant IVAs use had a total effect of 0.244 (95% CI = 0.069, 0.419), while new IVAs use showed a stronger total effect of 0.553 (95% CI = 0.315, 0.792).
Multigroup path analyses
Multigroup path analysis for residence patterns differences
A multigroup path analysis based on residence patterns was conducted to examine whether the mediation effects of IVAs use on cognitive function through social networks and physical exercise differed between older adults not living with children and those living with children. The results are presented in Figure 3 and Table 3.

Standardized parameters for the mediation model in the group of those not living with children (n = 5803) and those living with children (n = 2540).
Standardized direct, indirect, and total effects in multigroup path analysis (not living with children vs. living with children).

Note: Covariates are under controlled. Estimate: standardized parameter estimates; CI: confidence interval; IVAs = intelligent virtual assistants.
For older adults not living with children, both constant and new IVAs use showed significant positive direct effects on cognitive function (β = 0.223, CI = 0.019, 0.427 and β = 0.483, CI = 0.209, 0.756, respectively). Constant IVAs use had significant indirect effects through social networks (β = 0.036, 95% CI = 0.009, 0.063) and physical exercise (β = 0.032, 95% CI = 0.001, 0.062). New IVAs use also showed significant indirect effects through social networks (β = 0.054, 95% CI = 0.025, 0.082) and physical exercise (β = 0.093, 95% CI = 0.053, 0.133). The total effects of both constant and new IVAs use on cognitive function were significant (β = 0.291, 95% CI = 0.088, 0.493 and β = 0.630, 95% CI = 0.358, 0.901, respectively). For older adults living with children, neither constant nor new IVAs use demonstrated significant direct or total effect on cognitive function. Most indirect effects were not significant, except for the indirect effect of new IVAs use on cognitive function through physical exercise (β = 0.165, 95% CI = 0.076, 0.254).
Multigroup path analysis for education differences
A multigroup path analysis based on educational level was conducted to examine whether the effects of IVAs use on cognitive function differed between older adults with primary education and below and those with junior high education and above. The results are presented in Figure 4 and Table 4.

Standardized parameters for the mediation model in the group of primary and below (n = 5436) and junior high and above (n = 2907).
Standardized direct, indirect, and total effects in multigroup path analysis (primary and below vs. junior high and above).
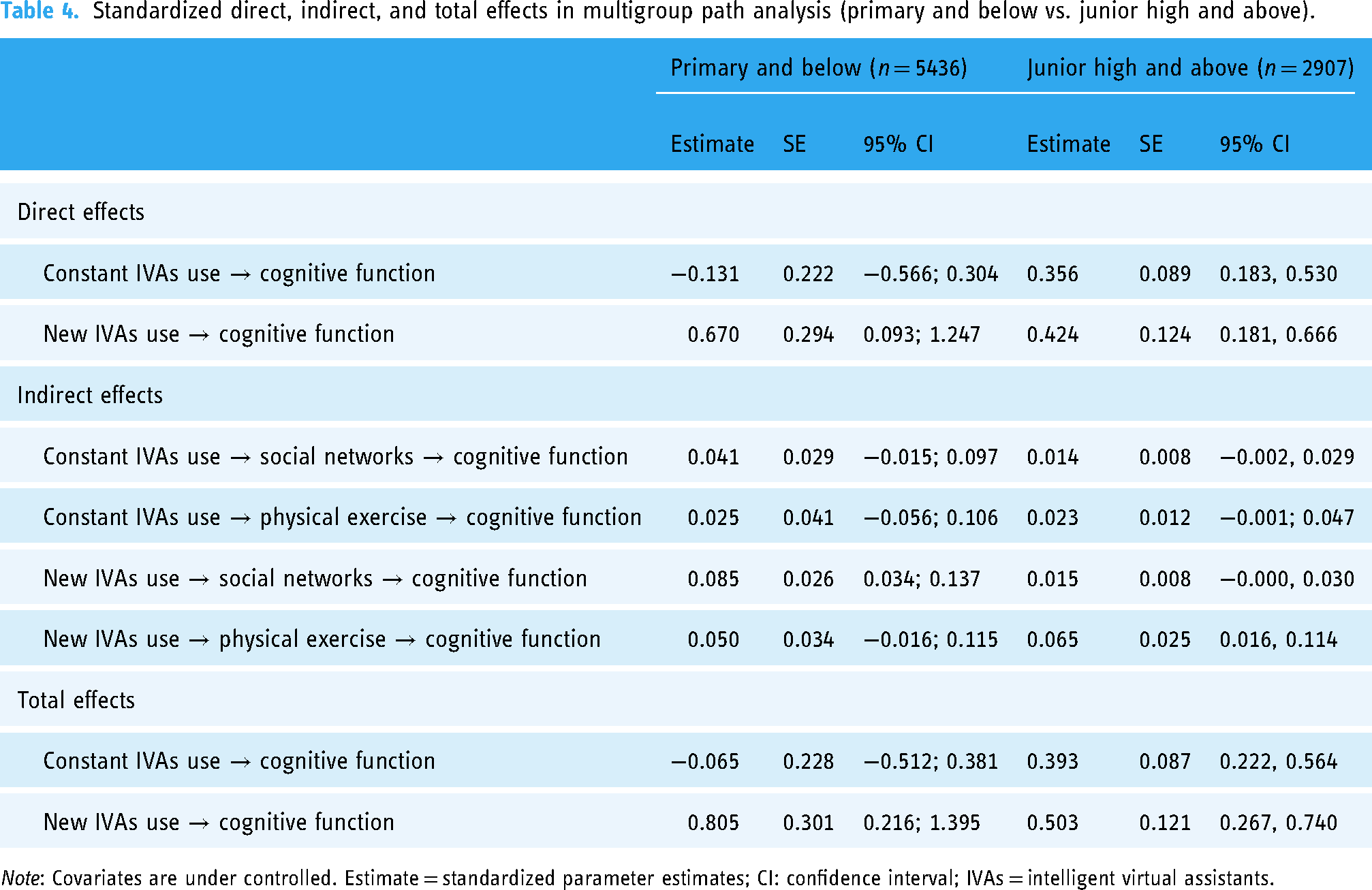
Note: Covariates are under controlled. Estimate = standardized parameter estimates; CI: confidence interval; IVAs = intelligent virtual assistants.
For older adults with primary education and below, constant IVAs use did not show a significant direct effect on cognitive function, while new IVAs use demonstrated a strong positive direct effect (β = 0.670, 95% CI = 0.093, 1.247). Most indirect effects were not statistically significant, except for the indirect effect of new IVAs use through social networks (β = 0.085, 95% CI = 0.034, 0.137). The total effect of constant IVAs use was not significant, but new IVAs use exhibited a strong significant total effect on cognitive function (β = 0.805, 95% CI = 0.216, 1.395). For older adults with junior high education and above, both constant and new IVAs use showed significant positive direct effects on cognitive function (β = 0.356, 95% CI = 0.183, 0.530 and β = 0.424, 95% CI = 0.181, 0.666, respectively). Only the indirect effect of new IVAs use through physical exercise was statistically significant (β = 0.065, 95% CI = 0.016, 0.114). The total effects of both constant and new IVAs use on cognitive function were significant (β = 0.393, 95% CI = 0.222, 0.564 and β = 0.503, 95% CI = 0.267, 0.740, respectively).
Discussion
This study examined the mediating roles of social networks and physical exercise in the relationship between IVAs use and cognitive function among Chinese older adults, considering differences in living arrangements and education levels. Both constant and new IVAs use significantly improved cognitive function, with new use showing stronger effects. Our research extends previous findings by demonstrating that social networks and physical exercise mediate this relationship, with varying strengths for constant and new use.
It is noteworthy that our descriptive statistics show a slight increase in mean cognitive function scores from T1 (13.36) to T2 (13.48). While this trend may seem counterintuitive given the expected age-related cognitive decline, it could be attributed to several factors. Primarily, our attrition analysis (detailed in the Supplementary Material) revealed selective attrition, with participants having lower baseline cognitive scores being more likely to drop out of the study. This selective attrition could have resulted in the retention of samples with relatively better health status, potentially artificially inflating the mean score at T2. Additionally, practice effects from repeated cognitive testing could contribute to this observation. 32 This unexpected trend underscores the complexity of longitudinal cognitive research and the importance of considering attrition effects in interpreting results.
As expected, both constant and new IVAs use had significant total effects on the cognitive function of older adults. This result agrees with previous studies and support further empirical evidence for technologically reserve hypothesis.4,5 Compared to constant IVAs use, new IVAs use showed a stronger direct effect on improving cognitive function. Interestingly, our findings contrast with a previous study which found that continuous internet use had a stronger positive effect on mental health compared to new use. 26 This divergence in results highlights the potential differences between IVAs and general internet use in terms of functionality and interaction modes. The theory of cognitive plasticity offers a possible explanation: new IVAs use introduces new environmental demands, leading to a mismatch between functional supply and environmental demand. 20 This mismatch prompts the brain to respond and adjust rapidly, resulting in significant cognitive function improvements in the initial stages. 33 The continual creation of new tasks and challenges by new IVAs use can maintain this state of mismatch, driving short-term cognitive improvements until the system reaches a new dynamic equilibrium. In contrast, for constant IVAs use, the brain's functional supply has gradually adapted to existing demands and environments, reducing the motivation for change and stabilizing performance, thus weakening the effects of cognitive plasticity compared to new IVAs use. From another perspective, Lövdén et al. 20 also differentiate between flexibility and plasticity. Flexibility refers to the ability to optimize performance within existing structural constraints, while plasticity involves structural changes, such as increased neural connections or alterations in brain regions. New IVAs use may more frequently trigger a combination of flexibility and plasticity, leading to more significant cognitive improvements. Our study applies and validates this theory in the practice of IVAs.
More importantly, this study revealed social networks and physical exercise as important mediating factors between IVAs use and cognitive function among Chinese older adults. The use of digital technology increases social contact for older adults, helping them overcome social and spatial barriers and becoming an essential means of staying connected with the outside world. 34 IVAs can help older adults communicate with family and friends, provide reminders for social activities, offer virtual companionship, and expand their social networks. 17 Moreover, the role of social networks in enhancing cognitive reserves, reducing dementia risk, and improving overall mental health has been confirmed by numerous studies.15,35 This research provides further evidence on the mediating role of social networks between IVAs use and cognitive function. In addition, constant IVAs use may have a relatively stronger positive effect on social networks than new use due to several factors. Over time, users develop deeper relationships, become more proficient with the technology, and establish regular communication patterns. 36 The cumulative effect of prolonged use gradually expands and strengthens social connections, particularly benefiting older adults who may need more time to fully adapt to digital social interactions. 26
Furthermore, the results indicate that physical exercise also plays an important mediating role between IVAs use and cognitive function improvement, especially for new IVA users. IVAs can provide exercise reminders, collect health data such as exercise duration and frequency, and share these data to help older adults monitor their physical function progress and provide encouragement. 18 Physical activity and exercise have been extensively studied and proven to enhance cognitive performance through various molecular mechanisms, including the stimulation of brain-derived neurotrophic factors, learning, and memory,37,38 and are closely related to better cognitive function, delayed cognitive decline, and improved brain health. 16 These studies suggest that the use of IVAs can significantly impact cognitive health by enhancing physical activity and exercise. Compared to constant IVAs use, new IVAs use shows more significant effects on physical exercise and cognitive function improvement. According to Bräuer and Mazarakis, 10 it can be inferred that new IVAs users, due to novelty, high motivation, initial behavior changes, and positive psychological feedback, exhibit more significant improvements in physical exercise and cognitive function.
Additionally, this study conducted multigroup path analyses to explore the heterogeneity in the cognitive health effects of IVAs use among older adults with different living arrangements and education levels. The results indicate that compared to those living with children, older adults living alone experience significant cognitive function improvements with IVAs use, with social networks and physical exercise playing significant mediating roles. Loneliness among older adults is characterized by a lack of social interaction, which is greater for those living alone. 22 Older adults living alone, due to the lack of face-to-face interaction, rely more on external social tools to meet their social needs. The study by Park and Kim 12 found that artificial intelligence-based smart speakers, through anthropomorphic interactions, can provide companionship to older adults living alone and help them establish social networks, thereby positively impacting mental health. Good mental health has been proven to be associated with higher participation in physical activities. 39 Additionally, IVAs, through voice reminders and motivational functions, can help older adults living alone to participate more actively in physical activities, further improving cognitive function. In contrast, for older adults living with children, only new IVAs use through physical exercise shows an indirect effect on cognitive function; other indirect and direct effects are not significant. A possible explanation is that older adults living with children usually have a strong family support system that provides emotional support and social interaction in daily life, reducing their reliance on external social tools.40,41 Therefore, the introduction of IVAs does not significantly increase their cognitive stimulation. The main role of IVAs is to increase the frequency and quality of physical activity among new users, indirectly promoting cognitive function improvement.
For older adults with different education levels, the relationship between IVAs use and cognitive function also exhibits heterogeneity. For older adults with primary education or below, constant IVAs use did not have a significant direct effect on cognitive function, whereas new IVAs use showed a significant positive direct effect on cognitive function. Additionally, new IVAs use also significantly impacted cognitive function indirectly through social networks. Older adults with lower education levels may face more challenges in understanding and adapting to new technologies. 23 Due to their unfamiliarity with and lower acceptance of technology, constant IVAs use may not provide sufficient learning motivation or cognitive stimulation. However, the introduction of new IVAs may spark their interest and engagement in the short term, leading to significant cognitive function improvements. For older adults with junior high education or above, both constant and new IVAs use have significant positive direct effects on cognitive function, and new IVAs use also has a significant indirect effect through physical exercise. Older adults with higher education levels have stronger learning abilities and adaptability to new technologies, 24 allowing them to quickly master and utilize various functions of IVAs. Therefore, both constant and new IVAs use can bring about significant cognitive function improvements. Furthermore, IVAs can promote physical exercise through reminders and motivation, particularly effective for those with higher health awareness. This group is more likely to accept IVA suggestions, indirectly enhancing cognitive function through increased physical activity.
Limitations
This study has the following limitations. First, the study's reliance on a simplified Mental State Examination scale, necessitated by data constraints, may inadequately capture the full spectrum of cognitive abilities, particularly visuospatial skills, executive functions, and processing speed. Future research should consider using more comprehensive cognitive assessment tools to provide a deeper understanding of cognitive abilities in older adults. Second, due to data unavailability in the 2018 CLASS, mediating variables at T1 have not been controlled in the multiple mediating model. This limitation potentially affects the interpretation of temporal relationships. Future studies should incorporate longitudinal data on mediators to facilitate more robust causal inferences. Third, there may be potential reverse causality between the use of IVAs and cognitive function. Although we controlled for cognitive function at T1 and a series of health-related covariates, endogeneity issues may still exist, as health status could influence IVAs use behavior. Due to data limitations, we were unable to obtain historical information about cognitive performance and technology use patterns. Future studies could address this limitation by incorporating questions about technology use history and prior cognitive performance in survey design while also employing more robust causal inference methods such as instrumental variable approaches. Fourth, considering the sample selection problem arising from attrition bias (discussed in more detail in Tables S1 and S2 in the Supplementary Material), future research needs to explore both methodological and data-driven solutions to address this issue comprehensively. Fifth, the current low adoption rate of IVAs among older adults results in an imbalanced sample distribution, particularly evident in the subgroup analyses (as detailed in Table S3 in the Supplementary Material). This imbalance may limit the statistical power and reliability of certain analyses. Future research should aim for larger, more balanced samples to enhance result robustness.
Conclusion
The proliferation of digital technology offers promising solutions for promoting the health of older adults. This study examined the relationship between constant and new IVAs use and cognitive function among Chinese older adults, exploring social networks and physical exercise as mediating pathways. The results showed that IVAs use, particularly new IVAs, significantly improved cognitive function in older adults. Social networks and physical exercise mediated this relationship. Subgroup analysis revealed that for older adults not living with children, IVAs use significantly enhanced cognitive function, with social networks and physical exercise playing crucial mediating roles. For those living with children, only new IVAs use showed indirect effects through physical exercise. Education levels also influenced outcomes: among those with primary education or below, only new IVAs use had significant effects, while for those with higher education, both constant and new IVAs use positively impacted cognitive function.
Based on these insights, we propose the following policy implications: first, policymakers should encourage technology companies to develop affordable, user-friendly IVAs through subsidies and tax incentives. Particular emphasis should be placed on the development of novel IVAs, supporting the creation of those with innovative interaction modes, advanced voice recognition technologies, and more intelligent personalized services. Second, given the significant mediating role of social networks, government and private sector entities should introduce and promote IVAs in community centers, nursing homes, and libraries while implementing targeted training programs to teach older adults how to use IVAs to expand their social networks and maintain connections with family and friends. Third, considering physical exercise as another crucial mediating variable, authorities should promote exercise programs for older adults, offering free or low-cost exercise classes through community activity centers and utilizing IVAs for personalized exercise plan formulation, reminders, and health data collection. Finally, differentiated support and training measures should be developed for older adults with varying living arrangements and education levels. For older adults living with children, family-oriented applications of IVAs that promote intergenerational interaction should be developed. For those with lower education levels, simplified versions of IVAs should be designed, accompanied by more basic, step-by-step training. For older adults with higher education levels, advanced IVAs function training can be provided, encouraging them to fully utilize various features of IVAs. By implementing these strategies, policymakers can improve the accessibility and usability of intelligent technological products, creating a more livable, age-friendly society and addressing the challenges of population aging.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251317355 - Supplemental material for Can intelligent virtual assistants improve cognitive function in older adults? A two-wave mediation study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251317355 for Can intelligent virtual assistants improve cognitive function in older adults? A two-wave mediation study by Tianxin Cai, Shilong Ma and Renyao Zhong in DIGITAL HEALTH
Footnotes
Contributorship
TC was responsible for conceptualizing the article, designing the framework, and writing the initial draft. SM handled the literature collection, data analysis, and also contributed to the initial draft. TC and SM jointly completed the review and revision of the manuscript. RZ supervised the project, conducted quality reviews, and was the grant recipient. All authors have read and agreed to the published version of the article.
Consent for publication
All personal data (including individual details, images, or videos) involved in this study have been granted informed consent for publication from the participants or their legal representatives.
Data availability statement
Declaration of Conflicting of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The survey was also conducted within the article 38, 39, and 40 of the Constitution of People's Republic of China and the legal framework governed by Chapter I, Article 9 from the statistics law of the People's Republic of China. Therefore, the study was not reviewed by ethics committee. Verbal informed consent was obtained from all individual participants included in the study. The design of this survey was within the article 38, 39, and 40 of the Constitution of People's Republic of China and the legal framework governed by Chapter I, Article 9 from the statistics law of the People's Republic of China. Verbal informed consent was acceptable and was not reviewed by ethics committee. Moreover, the interviewer also had documented the more details information on the process of obtaining informed consent, which included whether agree to attend this study, the time of agree to attend this study, the reasons of disagree to attend this study, and so on. The details of informed consent were stored by the Institute of Gerontology and National Survey Research Center at the Renmin University of China.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Major Project of National Social Science Fund of China: Strategic Research on Urban-Rural Coordination and Regional Coordinated Development of Social Pension Service Systems in Responding Positively to Population Aging” (Project Number 21AZD076) and National Social Science Fund of China (Grant Number 21AZD076).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.