
Abstract
Objective
Pre-frailty is prevalent and linked to diminished physical function and heightened healthcare needs. This study explored feasibility and preliminary effects of a structured 12-week exercise programme for pre-frail older adults and its impact on physical performance.
Methods
A multi-centre, prospective quasi-experimental study with single-arm pre-post design was conducted from April 2022 to September 2023 across four regional primary care clinics in Singapore. Participants aged ≥65 years, with Clinical Frailty Scale (CFS) score of 3 or 4, were enrolled in a 12-week program consisting of nine supervised in-person and three asynchronous remote exercise sessions (via pre-recorded videos). Each session lasted one hour and targeted functional strength, balance, mobility, and endurance. Primary feasibility outcomes included recruitment, retention, adherence, fidelity, satisfaction, and safety; clinical outcomes were considered secondary. Physical performance was assessed using Short Physical Performance Battery (SPPB), 30-Seconds Sit-to-Stand (30CST), and handgrip dynamometry at baseline and at 3 months (post-intervention). Changes in physical activity levels were evaluated using interviewer-administered International Physical Activity Questionnaire-Short Form (IPAQ-SF) at baseline, 6 months, and 12 months.
Results
Of 227 eligible participants, 162 started the programme (attended ≥1 session), and 139 completed the 3-month follow-up. The recruitment rate was 71.4%, and the retention rate was 85.8% (139/162) among those who started. The program achieved overall 81.9% average attendance rate across 12 sessions, with 64% of participants attending at least 10 sessions. Participants demonstrated an increase in SPPB scores (mean: +0.76 points; 95% CI: 0.48–1.04; p < 0.001) and in 30CST repetitions (mean: +2.82; 95% CI: 2.27–3.41; p < 0.001) from pre- to post- intervention. Female participants showed improved right-hand grip strength (mean: +0.65 kg; 95% CI: 0.16–1.14; p = 0.010), although male grip strength did not significantly change. No significant increase in total physical activity was observed at 6 or 12 months (IPAQ category shifts: p = 0.136 and 0.050 respectively), despite a positive trend towards higher activity levels. All respondents expressed satisfaction with the overall programme, and 93% were satisfied with the remote sessions. No exercise-related adverse events occurred. Qualitative feedback highlighted improved confidence and social engagement as added benefits.
Conclusion
The structured hybrid exercise program was feasible in a primary care setting and associated with improvements in physical function among community-dwelling pre-frail older adults. Feasibility was demonstrated through strong attendance, completion rates and participant satisfaction. Despite no significant change in self-reported physical activity, the combination of in-person supervision and home-based exercise appears promising for scalable pre-frailty management. This pilot study's positive findings support further evaluation in a controlled trial and suggest that such hybrid models can be implemented to engage pre-frail seniors in regular exercise.
Introduction
Globally, life expectancy is increasing, with projections indicating that by 2030, one in six people will be aged 60 years or over. 1 As people age, the accumulation of damage at the cellular level results in a gradual decrease in physical and mental capacity, increasing the risk of age-related diseases and frailty.2–4
Frailty is a geriatric syndrome characterised by unintentional weight loss, low muscle strength, feeling of exhaustion, reduced physical activity capacity and slower gait speed. It is significantly associated with adverse health-related consequences, including poor physical health, increased hospitalisation, risk of falls, increased institutionalisation and mortality. 5 The global prevalence of pre-frailty and frailty among community-dwelling older adults ranges from 34.6% to 50.9% and 5.8% to 27.3%, respectively. 6
In Singapore, the pre-frailty and frailty affect approximately 37% and 6.2% of older adults respectively. 7 With residents aged 65 years and above accounting for up to 18.8% of the total resident population, Singapore is one of the fastest-ageing societies in Asia. 8 The increasing number of frail older adults requiring more care places a significant socioeconomic burden on families and the healthcare system. 9 Hence, supporting older adults in maintaining physical functional independence and good health to prevent or delay the onset of disease and disability is important. 10
Early identification and targeted interventions can prevent progression from pre-frailty to frailty in older adults. 11 Evidence-based strategies include targeted medical and medication review for reversible medical causes of frailty, nutritional counselling and tailored exercise programmes. 12 Physical exercise interventions are among the most effective strategies for delaying the progressing of frailty, or mitigating frailty indicators, especially when conducted in group-based settings.11,13–15 Group-based programmes not only improve physical outcomes, but may also offer additional psychosocial benefits through peer support and social engagement. In contrast, individual or one-to-one interventions, hormone supplementation, and cognitive training have shown limited or inconsistent effectiveness. 11 Moreover, economic evaluations have demonstrated that community-based exercise programmes, when compared to usual care, are cost-effective, particularly for very frail older adults.16,17
Amidst a rapidly ageing population in Singapore, implementation of frailty intervention programmes within community settings is critical. Community-led approaches that reduce dependency on healthcare professionals will also address existing service gaps. Digital health innovations present an opportunity to extend the reach of such interventions. Recent studies have shown that tele-rehabilitation and ‘blended’ exercise programmes (combining centre-based sessions with remote exercise) can be feasible and effective for older adults.18,19 The COVID-19 pandemic further accelerated acceptance of remote exercise options among seniors, highlighting the need for flexible delivery modes. Hybrid models align with modern digital health frameworks emphasising accessibility and scalability of interventions. We conceptualised a hybrid model leveraging Singapore's widespread internet access among seniors and the healthcare infrastructure that supports community programmes. In Singapore's primary care system, public polyclinics serve as accessible touchpoints for older residents, making them ideal hubs to pilot community exercise initiatives.
Pre-frail older adults are a particularly suitable population for such hybrid digital interventions. They remain independent enough to engage with technology, and preventive exercise at this stage can delay or reverse frailty progression. We initiated the Functional Strength Building of Older Persons (FABULOS) programme in 2020, co-developed by primary care clinicians and a local health promotion social enterprise. The programme was a 12-week structured group exercise programme aimed at improving physical function and promoting sustained physical activity among community-dwelling pre-fail older adults.
Given the pilot single-arm design, we acknowledge that our study is exploratory and cannot establish efficacy; feasibility and acceptability are the central focus. This study primarily aimed to evaluate the feasibility of implementing FABULOS – including recruitment, adherence, retention, fidelity, participant satisfaction, and safety – and secondarily to assess changes in physical performance outcomes. The primary feasibility objective was to determine if key benchmarks (e.g., ≥70% session adherence, ≥70% completion of follow-up) could be met. Secondary objectives included examining changes between baseline and 3-month follow-up in physical performance measures (SPPB score, 30CST repetitions, and handgrip strength), as well as changes in self-reported physical activity levels at 6- and 12-months post-programme and participant satisfaction levels. We hypothesised that the programme would be feasible (with high attendance and positive feedback) and would be associated with improvements in functional measures, providing preliminary data to inform future controlled trials.
Methods
Study design and study sites
This study was a multi-centre, single-arm prospective intervention feasibility study conducted between April 2022 and September 2023 at four public primary care clinics in the eastern and north-eastern regions of Singapore. These clinics serve large residential communities totalling approximately 730,000. 20 The clinics were selected based on their substantial older patient population and existing facilities for group activities, ensuring a suitable environment for programme implementation. Study conduct and reporting was done in adherence to the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines. 21
Study population
Participants were community-dwelling older adults, aged 65 years and above, who had attended any of the participating clinics. Eligibility criteria included a Clinical Frailty Scale (CFS) score of 3 or 4, and willingness to complete a 12-week structured exercise programme. The CFS is a validated tool designed to quantify the degree of disability from frailty. 22 A score of 3 (‘managing well’) indicates individuals have their medical problems under control but are not regularly active beyond routine walking, and 4 (‘vulnerable’) indicates individuals have symptoms that limit their activities, such as feeling slowed down or tired during the day but are not yet dependent on others for daily help. These categories were chosen to capture pre-frail individuals at risk of becoming frail. 23 Individuals were excluded if they had medical contraindications to exercise or clinical symptoms that made exercise unsafe (e.g., unstable angina, severe joint pain, or acute illness) as determined by their physician, or if they had cognitive impairment precluding informed consent. Cognitive impairment was pragmatically defined by physician judgment and known diagnoses on the National Electronic Healthcare Records (NEHR); patients with diagnosed dementia were not enrolled, ensuring participants could follow instructions safely.
Potential participants who met eligibility criteria were referred by their attending physician to the study team. Among those who consented, participants who were enrolled had their baseline assessment performed on the same day at the start of the first exercise session.
Sample size calculation
A priori sample size calculation was performed. Based on pilot data and literature, we estimated a small-to-moderate effect size of d ≈ 0.25 for improvement in SPPB scores over 3 months. Using Cohen's criteria and a two-tailed α = 0.05, we determined that 100 participants would provide 80% power to detect this change. 24 To account for potential attrition of up to 30%, we aimed to recruit at least 143 participants. Sample size calculations were performed using GPower (Version 3.1.9.4). As this study was intended as a feasibility trial, all participants received the exercise intervention, and our focus was on estimating changes and assessing programme implementation metrics.
Intervention: the FABULOS structured exercise programme
Participants took part in a 12-week structured exercise programme consisting of weekly sessions. Nine sessions were conducted in person in the clinic or at a nearby community venue, and three sessions were delivered remotely via a pre-recorded online video. Each session lasted one hour and targeted major muscle groups with an emphasis on functional strength, balance, mobility and endurance.
In-person sessions
Participants were grouped into classes of 10–15 and guided by one primary exercise physiologist and one assistant. Open and closed kinetic chain exercises, focusing on strength, stability, mobility and balance, were conducted and detailed in Appendix 1. Exercise regimes were tailored for each participant depending on their existing functional strength and mobility, as assessed by the exercise physiologist. For example, if a participant could easily perform a standard exercise, an advanced variant or additional repetitions were given; those with difficulties were given simpler alternatives. Generally, participants progressed to more challenging versions or increased resistance when they could perform 10–15 repetitions of an exercise with good form.
There was no difference in the exercise program syllabus for both the in-person and remote sessions.
Remote sessions
Three custom exercise videos were produced by the team's exercise physiologists to mirror the content of the in-person sessions.25–27 Participants were guided to access the exercise video, which was hosted on the healthcare institution's YouTube channel. The videos were reviewed by the study team for quality and safety. They were filmed in high-resolution with clear audio, and instructions were given in both English and Mandarin to cater to our predominantly bilingual Chinese participants. Subtitles and visual cues were included for accessibility.
At the start of the video, Figure 1 shows an exercise physiologist introducing common household items to use as exercise equipment (a stable chair, two 0.5-L water bottles as light weights, a towel and resistance bands).
Exercise physiologist showing required training equipment for remote session.
As shown in Figure 2, the exercise regime was offered in both ‘standard’ and ‘easier alternative’ options to accommodate differing mobility and effort tolerance of the participants.

Exercises conducted in both ‘standard’ and ‘easier alternative’ options.
Figure 3 illustrates the embedded break times, which were included between different sets of exercise, to ensure participants had adequate time to rest and prepare for the next activity. This was aimed to reduce injuries, enhance recovery and ensure that participants were able to maintain a sustainable and effective exercise routine.

Break times are embedded within online video.
As shown in Figure 4, countdown timers were added to provide participants with a visual cue of progress. Knowing that the end is approaching can motivate individuals to push through and stay focused, giving a sense of accomplishment as the timer decreases.

Countdown timers are added during exercise sets.
Participants were instructed to perform the video session during the designated week. Remote advice and assistance were available. If participants had difficulty accessing the video or performing the exercises, they could call a provided hotline. A team member would guide them through technical issues or clarify exercise techniques over the phone. Additionally, participants were reminded via phone or messaging to complete their remote session. Attendance for remote sessions was tracked by self-report and confirmed during the follow-up call or next class.
Throughout the programme, participant safety and correct form were emphasised. Exercise physiologist provided feedback and modified exercises as needed for individuals during the in-person sessions. For remote sessions, participants were encouraged to exercise with a family member present if they felt unsure, and to ensure a safe environment during the exercise. Some participants had reported needing assistance for the home sessions and would typically require a family member's help to start the video or exercise alongside them for encouragement. This indicates that while the videos were user-friendly, a portion of participants benefitted from additional support during remote exercise.
Measures
Primary feasibility outcomes
We defined a set of primary outcomes related to feasibility and acceptability, measured throughout the study: (1) Recruitment rate – the proportion of eligible individuals who enrolled and had their baseline assessment performed at the first exercise session; (2) Retention rate – the proportion of enrolled participants who completed the programme and 3-month follow-up; (3) Adherence – attendance to exercise sessions (recorded for each session), including overall attendance percentage and completion of ≥10 out of 12 sessions (defined as successful programme completion, ≥70% adherence; ≥70% retention); (4) Intervention fidelity – whether the programme was delivered as planned, monitored through session checklists and consistency of content (all planned exercises were delivered in all classes, and remote videos followed the standardised syllabus); (5) Acceptability – participant satisfaction, measured via a post-programme survey and (6) Safety – any adverse events during the study.
Secondary clinical outcomes
Physical performance measures
Physical performance was measured at the start of the first session (baseline) and at the end of the 12th week (post-programme). Trained assessors, who were not the exercise class instructors, conducted these tests in a standardised manner across all sites.
The SPPB is a reliable and valid tool used to assess physical performance among older adults. 28 It assesses the functional mobility of an older adult's lower extremities in three domains (static balance, gait speed and chair stands). Balance is evaluated via the duration which participant can maintain side-by-side, semi-tandem and tandem stances. Gait speed refers to the time taken by the participant to walk 3 m at their usual pace. Lower limb strength is assessed with the chair stand test, which records the time taken to complete five consecutive sit-to-stand movements from an armless chair with arms folded across the chest. Each component is scored from 0 to 4, with a total possible score of 12, where higher scores indicate better physical performance, while a score lower than 10 is predictive of all-cause mortality.29,30 Assessors were trained to administer SPPB uniformly (using the same verbal instructions and timing device).
Grip strength is a measure of overall muscular strength and functional capacity. It is assessed using a handgrip dynamometer, with participants’ elbows flexed at 90° with the forearm in neutral position, squeezing the device as hard as possible with their left and right hands. The average recorded value from two measurements was used for analysis of this study. 31 Low handgrip strength is recognised as <28 kg in men and <18 kg in women in Singapore. 32
30CST is a measure of lower limb strength, endurance, and functional fitness. It is performed by recording the maximum number of times a participant can stand up fully and sit down from an armless chair within 30 s, with their arms folded across their chest. A higher number of repetitions indicate better functional capacity. 33 We included 30CST because our participants’ generally high baseline function meant that the SPPB's 5-repetition chair stand (which is part of SPPB) might not capture all improvements; 30CST provides a more sensitive gauge of gains in muscular endurance for those near the SPPB ceiling.
International physical activity questionnaire-short form (IPAQ-SF)
Self-reported physical activity was measured via the IPAQ-SF, administered by interview at baseline, 6 months and 12 months from programme start. At baseline, this was done face-to-face during the enrolment visit. At 6 and 12 months, it was done through structured telephone interviews.
The IPAQ-SF is a validated instrument that measures physical activity level.34,35 Its eight items assess the frequency and duration of physical activity such as sitting, walking, moderate-intensity activities and vigorous intensity activities. The total metabolic equivalent (MET)-minutes per week is calculated for categorisation into low, moderate, or high physical activity levels (Low <600 MET·min/week; Moderate 600–2999; High ≥3000). 36 The IPAQ-SF has acceptable validity for ranking physical activity in older adults, though it is prone to overestimation and recall bias. We acknowledge that without objective monitoring, reported increases should be interpreted cautiously. To maximise accuracy, our interviewers used standardised prompts and examples to help participants recall their activities.
Follow-up calls
Participants who completed the structured exercise programme received a follow-up call at 6 and 12 months to complete the IPAQ-SF.
Participants who withdrew from the programme early received a follow-up call at 12-week interval to gather feedback on their reasons for dropping out and any suggestions. We logged any reasons provided.
Satisfaction survey
At the 3-month post-programme follow-up, participants completed a satisfaction questionnaire developed for this study. This survey included Likert-scale questions on various aspects: satisfaction with session content, instructor effectiveness, class pacing, venue convenience, session timing and the exercise regimen overall. It also asked if participants noticed improvements in their health or physical abilities and whether they would recommend the programme to others. Though not a validated instrument, it was designed to capture multi-dimensional feedback.
Adverse event
Adverse events were monitored throughout. Participants were instructed to report any injuries, falls, or health problems during the study period. Instructors also observed and noted any issues during sessions (e.g., dizziness, undue fatigue). All adverse events were reviewed by the study team's clinician to determine relatedness to the exercise programme and severity. We planned that any serious adverse event related to the intervention would trigger a review and potential modification or termination of the programme for safety.
Blinding and bias mitigation
Given the nature of the intervention, participants and instructors could not be blinded to receiving the exercise program. However, outcome assessments were performed in a standardised manner by assessors who were not involved in delivering the intervention, to minimise bias. The assessors followed identical written protocols at each site and were trained together, ensuring consistency.
Participants did not have access to their baseline results, so they would not be biased by knowledge of prior performance during follow-up tests. We included all participants with any available outcome data in the analysis. We acknowledge that the lack of a control group means certain biases (e.g., Hawthorne effect, learning effect) may influence results and these are addressed in the Discussion.
Analysis
All data was audited for completeness and accuracy prior to analysis. Descriptive statistics in terms of frequency (n), percentage (%), mean and standard deviations (SD) were used to summarise baseline characteristics and feasibility metrics. Only participants with at least one pre- or post-data point for the primary outcome (SPPB) were included in the main analysis of change scores (n = 139). The characteristics of participants included in the analysis were compared with those who withdrew using Chi-square tests for categorical variables or t-tests for continuous variables.
Linear mixed models (LMM), with participants as a random effect, were used to assess changes in the SPPB, 30CST and hand grip strength. The LMM approach accounts for within-subject correlations and can handle missing data under a missing-at-random assumption by using all available data points. Each outcome (SPPB, 30CST, grip strength) was analysed with time (pre vs post) as a fixed effect. We included relevant baseline covariates as fixed effects: age (continuous, in years), gender, frailty status (CFS 4 vs 3), number of sessions attended (as a proxy for dose) and baseline physical activity level (IPAQ category: moderate or high vs low). These covariates were chosen a priori because older age, sex differences, higher baseline frailty, differing adherence and baseline activity could all influence outcome changes independent of the intervention. We checked for multicollinearity among covariates and for any non-linear effect of age. The covariance structure for repeated measures was set to compound symmetry (given only two time points). From the LMM, we obtained the estimated mean change (β for Post vs Pre) with 95% confidence interval and p-value. A significant positive β indicates improvement from baseline. We also looked at interactions (e.g., Time × Age) to see if improvement differed by subgroup. No formal adjustment for multiple comparisons was applied, given the exploratory nature of this pilot study and the limited sample size.
Sensitivity analyses were conducted by comparing the results from the LMM with those from t-tests and regression analyses for the same outcome measures. For categorical data, the McNemar test was applied to hand grip categories, while the McNemar-Bowker Test of Symmetry was used to evaluate changes in 30CST and IPAQ-SF.
No imputation was performed for missing data. For the 6- and 12-month IPAQ outcomes, analyses were based on available cases at each time. We acknowledge that attrition at these follow-ups was high, which could bias long-term physical activity findings, and will address its implications in the Discussion. All analyses were performed using STATA 13.0, with a significance level set at α = 0.05.
Results
Between April 2022 and September 2023, 227 participants were screened as eligible. Figure 5 presents the CONSORT-style flow diagram. Of these, 65 (28.6%) did not start the program or had their baseline assessment performed due to inability to attend any sessions (e.g., schedule conflicts, personal reasons). Thus, 162 participants attended at least one session. During the 12-week programme, 23 participants voluntarily withdrew, citing reasons such as lack of time, or family obligations. This resulted in a final analytical sample of 139 participants who completed the intervention and had at least baseline or follow-up data for analysis. The recruitment rate was 71.4% and the retention rate was 85.8%.

Flow diagram of participant progress through the study.
Appendix 2 compares baseline characteristics between those who withdrew and completed the study. Notably, participants who withdrew or never started the programme were older (mean 77.0 vs 74.4 years, p = 0.003), more frequently CFS 4 (45.5% vs 30.9%, p = 0.027) than completers, and were more likely to have been recruited from Sengkang or Tampines clinics, indicating that our analysed sample skewed slightly younger and fitter than the initially enrolled group. There were no significant differences in sex, baseline SPPB or baseline physical activity level between the groups. This suggests our analytic sample was slightly younger and fitter than those who did not complete, indicating a potential survivorship bias.
Table 1 shows the demographic and health profile of the 139 participants included in analysis. The mean age was 74.4 (SD 5.3) years. The majority were female (76.3%) and of Chinese ethnicity (95.0%). A small number were Malay (3.6%) or Indian (0.7%), reflecting the possible local catchment demographics, and language or cultural factors in program uptake. Most participants had primary or secondary education (78.3% with ≤ secondary education) and lived in public housing (73.4% in 1–5 room HDB flats). Only 8.6% were still working, and 78.4% were married, indicating a largely retired, community-dwelling senior cohort.
Baseline demographics of study participants.

One participant had missing data.
Only individuals with valid IPAQ activity classifications, based on the official scoring protocol, are included. Participants who selected ‘Don't know’ or left any fields blank were excluded.
Regarding health status, the mean Body Mass Index (BMI) was 23.9 (SD 3.8). The prevalence of chronic conditions was high: 64.0% had hypertension, 77.0% hyperlipidemia and 28.1% diabetes. About 32.4% had multimorbidity, defined as three or more chronic conditions. About 69.1% were rated CFS 3 and 30.9% CFS 4 at baseline. Baseline physical function was moderately high. Mean SPPB was 10.6 (out of 12), and baseline physical activity (IPAQ) classification was ‘Low’ in 48.1% of participants, ‘Moderate’ in 39.8% and ‘High’ in 12.0%.
Feasibility outcomes
Recruitment and retention
As referrals were made by physicians of participants who were attending the clinics for either acute or routine chronic care appointments, physicians referred only eligible participants for enrolment. All 227 participants were assessed to be eligible and scheduled for the FABULOS programme. However, due to the overwhelming uptake rate and limited availability within each class size of 15 participants, some participants had their class scheduled only 3 to 6 months after being screened for eligibility. This could have resulted in the subsequent mismatch in the availability of the participants, leading to 65 participants withdrawing before their baseline assessment were performed. Thus, the recruitment rate was 71.4%.
By the end of the 12-week programme, 23 participants withdrew, leading to a retention rate of 85.8%.
Attendance and adherence
Figure 6 shows the average attendance rate across the 12-sessions exercise programme was 81.9%, with the average attendance for physical session and remote session at 83.3% and 77.7%, respectively. The proportion of participants who completed at least 10 out of 12 sessions was 64.0%. Sessions 6, 8 and 10 were conducted as remote sessions.

Attendance rate of study participants.
Intervention fidelity
All sessions (in-person and remote) were delivered according to the planned curriculum. Instructors at all sites followed the standardised exercise regimen, which were verified via session checklists. Remote session fidelity was confirmed by participant self-reports and follow-up checks. There were no deviations such as session cancellations or protocol changes.
Acceptability (participant satisfaction)
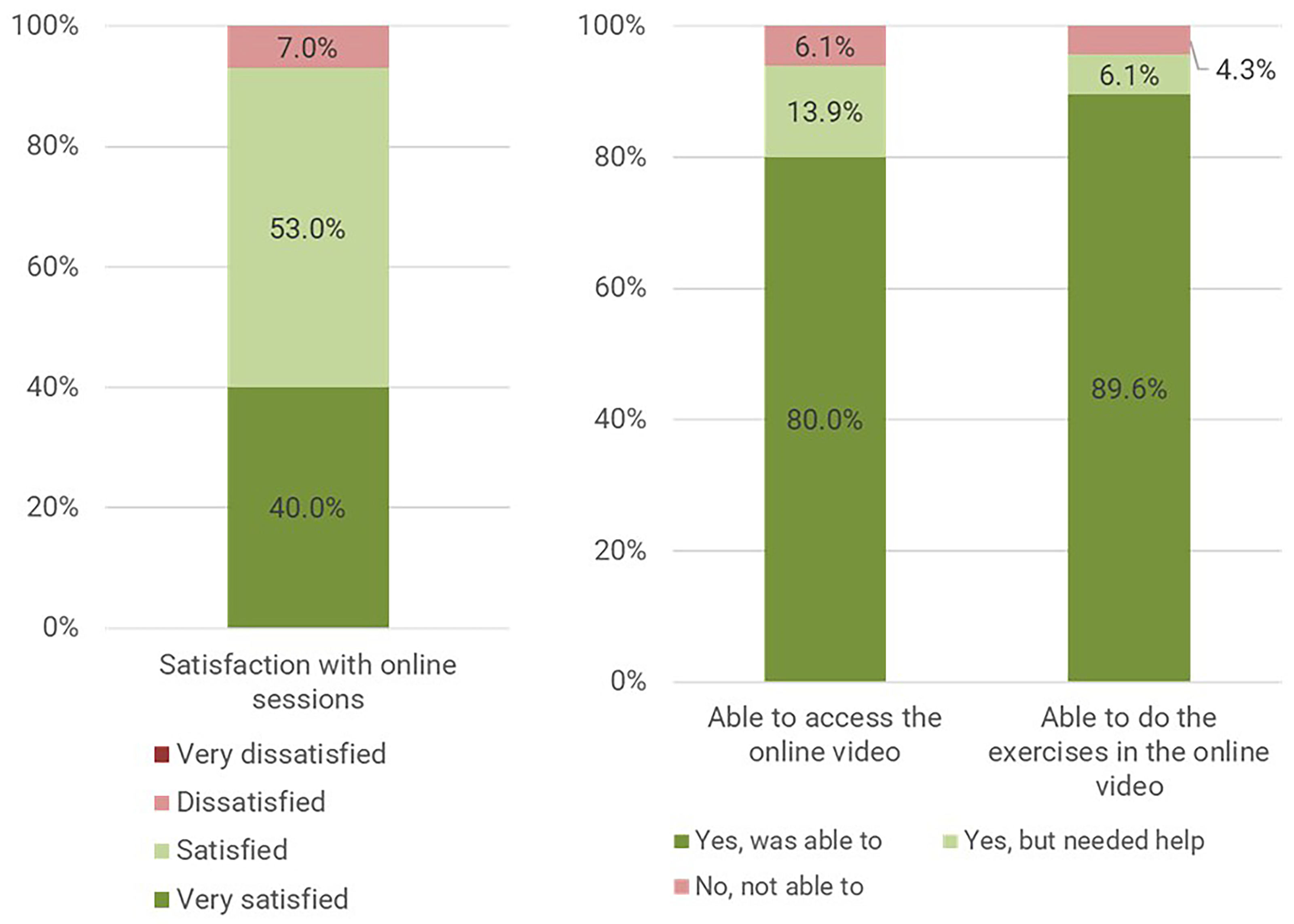
Figures 7, 8 and 9 demonstrate all participants (100%) expressed satisfaction with the 12-week structured exercise programme and 93% were satisfied with the remote sessions.

Satisfaction level of participants on overall programme and in-person sessions.
Satisfaction level of participants on remote sessions.

Qualitative feedback on overall programme.
About 80% of participants said they could access the exercise videos easily and 89.6% said they were able to perform the exercises in the online video on their own. However, a significant minority of participants faced technological or self-efficacy barriers and would likely benefit from additional support during remote exercise.
Majority reported perceived improvements in their lower limb strength and balance, felt that the intervention reduced their fall risk, improved their knowledge of exercises and widened their social networks. Furthermore, more than 80% of participants were likely to recommend the programme to their family and friends, as shown in Figure 9. Overall, these results demonstrate high acceptability of the hybrid programme.
Safety
One adverse incident was reported in the study period but was evaluated to be unrelated to the exercise programme. This involved a participant whose chair overturned while she was leaning back, resulting in a fall. This occurred prior to the start of the exercise session, while the participant was waiting for registration. The participant was evaluated, noted to have sustained no serious injuries, and continued with the exercise session without issues. The study team determined this event was not related to the exercise sessions, as it occurred outside the context of exercising and was due to an environmental trip hazard.
Clinical outcomes
Physical performance
The mean (SD) SPPB score increased from 10.6 (1.8) at pre-test to 11.4 (1.5) at post-test (P < 0.001). In Table 2, linear mixed model (LMM) analysis, adjusted for covariates, showed a statistically significant improvement in SPPB scores post-intervention (β = 0.76; 95% CI: 0.48–1.04; p < 0.001). A 0.76-point increase corresponds to d ≈ 0.42, and falls within the range of a small to moderate clinically important difference. 37
Changes in SPPB scores from pre-test to post-test and its associations in an adjusted linear mixed model analysis (n = 139).

Gender was not significantly associated with SPPB score changes (β = 0.30, 95% CI: −0.38 to 0.99, p = 0.385). Increasing age was inversely associated with SPPB scores (β = –0.05, 95% CI −0.10 to −0.01, p = 0.017). Frailty status (CFS: β = –0.14, 95% CI −0.73 to 0.45, p = 0.646) and the number of exercise sessions attended (β = 0.02, 95% CI −0.09 to 0.12, p = 0.770) were not significantly associated with changes in SPPB scores. Compared with participants with low physical activity levels, those with moderate (β = 0.37, 95% CI −0.13 to 0.87, p = 0.147) and high activity levels (β = –0.81, 95% CI −1.92 to 0.30, p = 0.153) did not show significant differences in SPPB score changes.
We note a potential ceiling effect in SPPB. At baseline, many participants were already at 10–11 points, leaving limited room for improvement to the maximum of 12 points. This suggests some participants may have improved in ways not fully captured if they were near the top of the scale initially.
We analysed grip strength separately for women and men, given their different baseline distributions and the significant interaction of gender on grip change as an exploratory analysis.
Among female participants, no statistically significant difference was observed in left-hand grip strength following intervention. However, right-hand grip strength demonstrated a significant improvement, increasing from 16.5 kg (4.1) to 16.9 kg (3.9) (p = 0.008). The adjusted linear mixed model showed a mean increase of 0.65 kg (95% CI: 0.16 to 1.14; p = 0.010), d≈0.2, in Table 3.
Changes in grip strength amongst females from pre-test to post-test and its associations in an adjusted linear mixed model analysis (n = 106).

Increasing age was negatively associated with left-hand grip strength (β = −0.14, 95% CI −0.26 to −0.02; p = 0.024), but not with right-hand grip strength (β = −0.13, 95% CI −0.29 to 0.02; p = 0.094). There were no statistically significant associations between grip strength and frailty status, number of exercise sessions attended, or baseline physical activity levels.
Among male participants, there was an increase in both left (Pre: 21.6 kg (5.5), Post: 22.7 kg (5.3)) and right-hand grip strength (Pre: 24.1 kg (5.0), Post: 25.0 kg (4.2)) from pre- to post-test, but these changes were not statistically significant. As presented in Table 4, no significant associations were found between grip strength and age, frailty status, exercise session attendance or physical activity levels.
Changes in grip strength among males from pre-test to post-test and associations in an adjusted linear mixed model analysis (n = 33).

Table 5 shows participants had significant improvement in 30CST from pre-test to post-test (Pre: 13.5 repetitions (3.6), Post: 16.5 repetitions (4.5); adjusted β = + 2.82 repetitions, 95% CI 2.27–3.41, p < 0.001). This corresponds to d≈0.8, a large effect size, and suggests clinical significance whereby participants on average could perform ∼20% more chair rises in the same time, likely reflecting better muscular endurance and perhaps confidence in the movement.
Changes in 30-second chair stand performance from pre-test to post-test and associations in an adjusted linear mixed model analysis (n = 139).

Age was negatively associated with 30CST, with each year of age resulting in a decline of 0.17 repetitions (adjusted β = −0.17 repetitions, 95% CI −0.26 to −0.08, p < 0.001).
Although the IPAQ high activity group showed a reduction in repetitions post-test (adjusted β = −2.05 repetitions, 95% CI: −4.03 to −0.08, p = 0.042), this result should be interpreted with caution due to possibly a ceiling or regression to mean effect.
No significant associations were found for sex, frailty status or the number of exercise sessions attended.
Physical activity level assessment
Table 6 summarises the IPAQ-SF categorical results at baseline compared with 6-month and 12-month follow-ups. At baseline (n = 133 with valid IPAQ), 48.1%, 39.8% and 12.0% of participants were in low, moderate and high activity level, respectively.
Changes in IPAQ activity categories from pre-test to 6 and 12 months.

At 6-month follow-up (n = 62), changes in IPAQ categories did not reach statistical significance (p = 0.136). Among participants initially classified as having low physical activity, 53.6% transitioned to the moderate activity category, and 10.7% to the high activity category. In the moderate baseline group, 56.0% remained in the same category while 24.0% progressed to high activity. Similar trends were observed in the high activity group, although changes were not statistically significant.
At 12-month follow-up (n = 45), no significant change was observed (p = 0.050). Among participants initially classified as having low physical activity, 52.2% progressed to moderate activity, and 17.4% to the high activity category. The moderate activity group also exhibited a shift towards higher activity, with 17.6% advancing to high activity category. Although statistical significance was not achieved, the results suggest a positive trend towards increased physical activity over time.
However, this result should be interpreted with caution as the proportion of participants responding at 12-month follow-up is only one-third (33.8%) of the original, and is likely biased towards the more engaged participants.
Discussion
This study demonstrates that a structured 12-week exercise program, incorporating in-person and remote sessions led by exercise physiologists, is feasible in the primary care settings and contributes to measurable improvements in lower extremity function among pre-frail older adults. All feasibility indicators were positive. We achieved strong adherence to the exercise sessions, excellent participant satisfaction and no occurrence of serious adverse events. These results suggest that even within busy public primary care clinics, such a hybrid model can be implemented successfully, engaging seniors in regular exercise.
High participant satisfaction and willingness to recommend the program underscore its acceptability and potential for sustained engagement.38,39 The group-based format fostered motivation, social connection and improved self-efficacy, which are crucial for adherence and long-term behaviour change. 40 Evidence of continued physical activity after the program suggests lasting impact, highlighting the importance of integrating follow-up support and community linkages.
The programme also hinted at psychosocial benefits, whereby participants reported widened social networks and improved knowledge about exercises. Many formed friendships in the class and continued to encourage each other. Social health is often an overlooked domain of frailty interventions. Our overwhelmingly positive satisfaction rates and qualitative feedback hint at possible additional benefits such as improved mood, increased social interaction and reduced isolation, which are important in the well-being of older adults. Future community exercise programmes can thus address both physical and social dimensions of health, a synergy that can be leveraged in public health planning. Additionally, successful multi-centre implementation supports the program's scalability and generalisability.
Our study demonstrates the feasibility of a hybrid delivery model in engaging older adults in exercise, leveraging the advantages of in-person supervision as well as the flexibility of home-based activity delivered digitally. In today's healthcare landscape, amplified by the COVID-19 pandemic experience, remote and digitally delivered services have gained traction for their convenience and accessibility. Our results suggests that older pre-frail adults are able to embrace and benefit from digitally enabled exercise formats, echoing the findings of recent studies which demonstrated that remotely delivered exercise programs for older adults are feasible and can yield significant health benefits.41,42 Although there is a minority of participants who needed technical assistance, nearly all managed to engage with the online videos. This indicates that with adequate support, such as a readily available hotline, family help and user-friendly content, technological barriers can be overcome even in a senior population. Future programmes might incorporate brief training on how to use online resources or provide tablets to those without access, to further lower barriers.
The single-arm design does not allow for causal inference about efficacy, but the observed improvements in SPPB and 30CST after the program are encouraging and consistent with the hypothesis that guided exercise can improve function. The increases in SPPB scores and 30CST repetitions suggest that interventions with a relatively low frequency can have a positive impact on essential functional capacities. Improved lower extremity strength and balance are key factors in mitigating frailty-related risks such as falls and the loss of independence.29,43 The magnitude of improvement we observed, with +0.76 points in SPPB and +2.82 additional chair-stands in 30CST, aligns with those goals, as even small gains in these measures have been associated with reduced disability and fall risk in older adults.
Our findings align with previous studies showing that structured physical exercise can improve physical performance and reduce frailty progression among older adults.44,45 This underscores the potential for such programs to be both impactful and scalable in community settings.
Significant gains in grip strength were observed among female participants but not among males. This discrepancy may reflect inherent differences in baseline muscle mass or motivation patterns during exercise. Female participants, who on average had low baseline grip strength (∼16.5 kg), benefited from our program's resistance training, showing a ∼0.65 kg improvement in grip strength. Men had higher baseline strength (∼24 kg) and may have required a more intensive resistance stimulus to achieve additional strength gains. 46 In our programme, all participants used the same equipment (light weights, resistance bands), hence, the training might have been close to optimal for women but subthreshold for many men. While our study was not powered to conclusively examine gender differences, the result highlights an interesting consideration for future research as exercise regimes could be tailored by gender or initial strength level to maximise benefit. We note that gender was not a significant factor in SPPB or 30CST improvements. Those functional gains applied to both men and women, which suggests the aerobic and balance aspects of the programme were effective across genders, whereas upper-body strengthening needs more customisation.
Strengths and limitations
Key strengths of this study include its real-world primary care setting and multi-site design, which enhance the generalisability of the results to similar community healthcare contexts. By embedding the programme in local polyclinics and community centres, we demonstrated that such interventions can be integrated into routine care workflows (e.g., referrals from doctors, use of clinic space during off-peak hours). We targeted a practical subset of older adults who are often seen in primary care and for whom preventative interventions are most needed.
Another strength lies in the integration of remote sessions, which provided flexibility for participants with mobility or transportation challenges and ensured continuity during periods when attending in-person sessions was not feasible. This hybrid model takes advantage of increasing digital health adoption among older adults, and our high remote-session completion rate demonstrates feasibility. The exercise programme was tailored to individual abilities, offering standard and easier alternatives. This personalisation likely contributed to the high adherence and positive outcomes, as it accommodated varying fitness levels within the group. We also employed objective functional measures as outcomes, lending credibility to the findings, and adhered to recommended reporting guidelines (TREND), ensuring transparency in our methodology. The inclusion of a structured satisfaction survey and gathering of qualitative feedback provided valuable insight into participant perspectives, a component often under-reported in feasibility studies.
However, several limitations merit consideration. First, the study's quasi-experimental single-arm design limits our ability to attribute improvements solely to the intervention. Without a control group, we cannot definitively rule out that some of the observed gains were due to other factors such as learning effects or Hawthorne effects. Participants might perform better on follow-up tests simply from having done them before, and their awareness of being in a study could have transiently boosted their activity or effort. Regression to the mean may also explain part of the improvement, especially for measures like 30CST where extremely low baseline performers tended to improve toward average on re-test. We attempted to mitigate bias by standardising assessments and keeping assessors consistent, but the lack of randomisation means our internal validity is limited. Future studies should employ randomised controlled trial designs to confirm efficacy and more clearly delineate the programme's effect from spontaneous changes.
Second, there is potential selection and survivorship bias. Participants who volunteered for and completed the program may be inherently more health-conscious, motivated or physically robust than the general pre-frail population. As participants who withdrew early were older and frailer on average, the observed improvements may overrepresent the fittest and most adherent individuals among the pre-frail. Strategies to better engage and retain the more vulnerable subset (e.g., more intensive coaching, caregiver involvement or addressing barriers like transport) should be considered in future iterations to ensure the programme can benefit a broader range of pre-frail elders. Additionally, our sample was predominantly female and largely of a single ethnicity and similar socioeconomic stratum. This demographic homogeneity limits generalisability, and the findings might not apply to older men or to more ethnically/culturally diverse groups who might respond differently or have different preferences.
Third, the study relied on self-reported physical activity for long-term follow-up, which introduces recall and social desirability biases. Participants who knew they had been through an exercise programme might report higher activity levels at follow-up because they believed they were supposed to be more active. Furthermore, we saw a large attrition at 6 and 12-months follow-up due in part to difficulty reaching participants or loss of interest after programme end. This attrition could lead to an overestimation of sustained activity as those who remained engaged and responded likely were the ones who continued exercising, whereas those who fell back into sedentariness might have been less inclined to pick up our calls. The nearly significant improvement in IPAQ at 12 months (p = 0.050) must thus be interpreted with caution due to the missing data and potential biases. For future studies, using wearable activity trackers or pedometers would provide objective data on activity change and maintenance. Additionally, implementing strategies to keep participants in the loop post-program (like monthly check-in calls or refresher sessions) might improve long-term follow-up rates and help sustain activity. We acknowledge that our lack of objective activity measurement and the high drop-off in survey response are limitations that temper conclusions about long-term impact.
Finally, an inherent limitation in our outcome measures was the ceiling effect observed in SPPB. The average participant started with a median SPPB score of ∼10.6 points, which is relatively high. Hence, some participants could not improve much because they were already near the maximum score of 12. This likely underestimated the programme's effect for those individuals.
Implications in deployment of FABULOS programme in the community
The findings from this study provide a valuable foundation for integrating structured exercise programs into primary care for frailty prevention. The hybrid approach seems particularly promising in an urban, tech-ready environment like Singapore as it leverages in-person resources and multiplies reach via remote content. In other countries or more rural settings, adaptations, such as the use pre-loaded videos on tablets or DVDs, and training of lay volunteers instead of engaging an exercise physiologist, might be needed.
Future studies should employ randomised controlled trial designs to rigorously assess the efficacy and cost-effectiveness of such interventions compared to standard care. Additionally, longitudinal studies are also needed to determine the sustained impact of these exercise programmes on fall prevention, hospitalisation rates and overall quality of life.
Conclusion
This feasibility study demonstrates that a structured, 12-week hybrid exercise program is practical, safe and well-received among pre-frail older adults in the primary care. We observed meaningful improvements in physical function, aligning with what would be expected from exercise, although confirmatory trials are needed. High adherence rates and participant satisfaction suggest that such programmes are acceptable. Hybrid models leveraging digital tools alongside traditional classes can extend reach and convenience, which is especially pertinent in a post-pandemic era of healthcare. With further research and refinement, such programmes could be integrated into routine primary care as a strategy to prevent frailty and promote healthy ageing, so as to enable seniors to maintain strength and confidence to delay disability, reduce falls and improve quality of life.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261425399 - Supplemental material for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study
Supplemental material, sj-docx-1-dhj-10.1177_20552076261425399 for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study by Alon Tan, Rebecca Ong, Vanessa Toh, Lay Khim Lim, Nicole Soh, Christine Kho, Navpreet Kaur, Kee Tung Tan and Pei Lin Hu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261425399 - Supplemental material for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study
Supplemental material, sj-docx-2-dhj-10.1177_20552076261425399 for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study by Alon Tan, Rebecca Ong, Vanessa Toh, Lay Khim Lim, Nicole Soh, Christine Kho, Navpreet Kaur, Kee Tung Tan and Pei Lin Hu in DIGITAL HEALTH
Supplemental Material
sj-doc-3-dhj-10.1177_20552076261425399 - Supplemental material for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study
Supplemental material, sj-doc-3-dhj-10.1177_20552076261425399 for A structured hybrid exercise programme for pre-frail older adults in primary care: A feasibility and pilot study by Alon Tan, Rebecca Ong, Vanessa Toh, Lay Khim Lim, Nicole Soh, Christine Kho, Navpreet Kaur, Kee Tung Tan and Pei Lin Hu in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to acknowledge ProAge and its team of exercise physiologists, who collaborated with SingHealth Polyclinics to design and implement the exercise sessions, as well as the Care Managers from the participating Polyclinics, who assisted in enrolling participants and providing the latter with regular reminders regarding the exercise sessions.
Ethical approval and informed consent statement
The study was approved by the SingHealth Centralized Institutional Review Board (Reference: 2020/3036) and carried out in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants before the start of the study.
Consent for publication
Author contributions
AT: conceptualisation, data analysis and writing. RO: conceptualisation, data analysis and critical review. VT: data collection and reviewing. LKL: data collection, reviewing. NS: data collection, reviewing. CK: data collection and reviewing. NK: data collection and reviewing. KTT: data collection and reviewing. PLH: conceptualisation, data analysis, critical review and supervision of the study. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the SingHealth Regional Health System Population Health Development Programme Fund (Project Reference: PH012). The funder supported the financial costs of the exercise sessions, and provided expertise for programme evaluation. The funder had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. The publication cost was supported by SingHealth Polyclinics - Centre Grant: CG21APR3006 (NMRC/CG3/001/2022-SHP).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The datasets used and analysed during the current study will be available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.