
Abstract
Objective
Research over the past decade has extensively covered the benefits of electronic health records in developing countries. Yet, the specific impact of their limited access on doctors’ workload and clinical decision-making, particularly in Bangladesh, remains underexplored. This study investigates current patients’ medical history storage mechanisms and associated challenges. It explores how doctors in Bangladesh obtain and review patients’ past medical histories, identifying the challenges they face. Additionally, it examines whether limited access to digital health records is an obstacle in clinical decision-making and explores factors influencing doctors’ willingness to adopt electronic health record systems in such contexts.
Method
An online cross-sectional survey of 105 doctors with Bachelor of Medicine, Bachelor of Surgery/Bachelor of Dental Surgery (MBBS/BDS) degrees and at least 2 years of experience was conducted, covering (a) personal information, (b) workload, (c) patient history challenges, and (d) decision-making.
Results
Out of 105 participants, 51.4% of them use paper-based methods with 56% facing challenges, versus 20% using digital methods. Most (94.3%) interview patients directly, and 80.9% are interested in a web-based, comprehensive medical history system. An ordinal regression model identified that the physicians’ disciplines, workload, and efficiency level of the current workplace in facilitating patient history-taking variables significantly affected willingness to adopt the described electronic health record in the survey.
Conclusion
Doctors in Bangladesh encounter significant challenges related to workload and clinical decision-making, largely attributed to restricted access to patients’ past medical histories. Despite the prevalent use of paper-based records, there is a notable willingness among these medical professionals to embrace electronic health record systems, indicating a potential shift towards more efficient healthcare practices in the region.
Keywords
Introduction
The World Health Organization (WHO) reports that ∼ 3.5 billion individuals, or nearly 50% of the global population, do not have access to necessary health services. 1 With recent advancements in technology, the digitization of healthcare has become increasingly relevant. The International Organization for Standardization (ISO) describes electronic health record (EHR) as a secure, digital repository for patient information. This data, safely shareable and accessible by various authorized users, includes a broad spectrum of patient data covering past, present, and future medical information. The primary goal is to support continuous, efficient, and high-quality healthcare that is seamlessly integrated. 2 As defined by Menvielle et al., 3 digital health is the application of technology to deliver healthcare services or to facilitate better health. The potential benefits of digitization in healthcare are significant. These include standardizing patient care, reducing medical errors, and improving diagnostic processes, all of which are essential for enhancing human life quality. Particularly in developing countries, digitization in healthcare could be a game-changer, enabling doctors to reach a wider patient base and potentially reducing their workload. 4 Over the past few years, there has been an escalating interest in the implementation of electronic medical records (EMRs) and EHR across various developing countries. This trend is largely driven by the increasing acknowledgment of how essential robust health information technology (HIT) is for delivering higher-quality healthcare at more affordable costs. 5 Numerous studies in diverse healthcare settings have indicated that EHRs are key to minimizing medical errors, achieving effective care coordination, and enhancing overall safety and quality in healthcare, while also reducing its costs.6–9
Recent studies have shown that 80% of medical data is still unstructured. 10 This includes the patient's past medical history that is on paper and the digitized past medical history that is not usable because it's too challenging to interpret.
Decision-making is a crucial aspect of nearly every area of life, but in healthcare, it becomes especially complex due to its significant impact on individual well-being. 11 In healthcare, deciding on treatment involves several steps. It requires understanding the information, evaluating the evidence, and using knowledge to select treatments that are safe and effective for patients. 12 Effective clinical decision-making often relies heavily on a patient's past medical history. The history provides critical information about their current health status, including chronic conditions, previous treatments, and potential risk factors, which is invaluable for physicians in making informed decisions about diagnosis, treatment, and prevention. 13 Therefore, limited access to a patient's past medical history can considerably complicate clinical decision-making processes.
Current status of EHR adoption: Global view
Digital health technologies, including telehealth, Internet of Things (IoT)-enabled devices, virtual reality (VR), artificial intelligence (AI), and wearable sensors, hold immense potential to revolutionize healthcare delivery worldwide. These advancements offer transformative opportunities to fight both communicable and non-communicable diseases, enhancing the quality of life and extending life expectancy. 14 A study by Katsaliaki and Kumar 15 discussed that global life expectancy has steadily increased since 2000, from 67.2 to 73.5 years in 2019.
In response to evidence highlighting the benefits of EHRs in enhancing healthcare quality, the United States enacted the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009.16,17 Data from 2019 to 2021 reveals that 86% of non-Federal general acute care hospitals had implemented a 2015 Edition certified EHR. In comparison, the adoption rate for the same EHR edition was markedly lower in other types of hospitals: only 40% of rehabilitation hospitals and a mere 23% of specialty hospitals had embraced this technology. 18
Similarly, South Korea has demonstrated a notable uptake in EHR usage. According to the Health Insurance Review and Assessment Service (HIRA), as of 2017, 93.6% of hospitals and 91.6% of private clinics in South Korea had integrated EMR systems.17,19
In African developing countries, the adoption and utilization of EHR systems are still in their early stages, with widespread implementation remaining a long-term objective. In these regions, the absence of EHR systems or centralized patient medical record databases often forces clinicians to rely on patient-provided records, which may be incomplete or inaccurate, thus compromising the quality of patient care. These records are typically maintained using paper-based methods. However, the scenario varies across countries. For instance, a recent study focusing on Nigeria's healthcare system indicates a readiness to embrace EHRs and EMRs. Despite this readiness, the study also brings to light several critical challenges that need addressing for these technologies to be successfully implemented and adopted. Key among these are concerns about the system's usefulness, its ease of use, data security measures, and the necessary infrastructure. 20 Another study in Kenya found that on average, 18.1% of authorized users actively engaged with the KenyaEMR (KeEMRs) system across various facilities, with a standard deviation of 13.1% and a statistical significance (p-value) of < 0.001. The same study suggested that most of the EHRs use areas assessed need improvement, especially in relation to active usage of the system and data exchange readiness. 21
Current status of EHR adoption: Bangladesh's view
Bangladesh introduced District Health Information Software (DHIS2) in 2009, a comprehensive web-based platform for managing health data. The system, integrating functionalities for data collection, validation, and analysis, has become the cornerstone of the national health information management system. The Management Information System of the Directorate General of Health Services (MIS-DGHS) in Bangladesh is developing a shared health record (SHR) system for a national electronic health records archive, accessible across all health facilities. This system eliminates the need for patients to carry personal health files, enabling doctors to easily retrieve and update medical records. 22 With built-in security measures, the SHR, piloted in select hospitals, is now expanding nationwide. Additionally, in recent developments, there has been a shift towards utilizing open-source software. Notably, the adaptation of OpenMRS (Open Medical Record System) and its customized local version, OpenMRS+, signify this trend. OpenMRS+ in Bangladesh is an amalgamation of several modules, including OpenMRS, Odoo, OpenELIS, and dcm4chee, catering to diverse healthcare IT needs ranging from medical records to clinical image archiving. 23 OpenMRS+ in Bangladesh is seamlessly integrated with the national SHR system, enabling interactive data exchange and storage of up-to-date patient files in a central repository. This system is currently in use by numerous health facilities, and both public and private entities are encouraged to adopt this free software, joining the nationwide health facility automation network. In remote areas, the portable health clinic (PHC) has been introduced. It provides primary care and diagnostics through telemedicine. 24 Despite these improvements, challenges persist, such as system availability and healthcare professionals’ attitudes towards digital health. A study indicates mixed feelings among professionals: 46% fear job loss due to digitization, 68% believe it might lead to skill erosion, while 91% cite the need for user-friendly systems, 92% point out high costs, and 75% note doctors’ reluctance as significant hurdles to digitization. 25
Over the last 20 years, there has been a notable rise in the time hospital clinicians dedicate to documentation and clerical tasks, which has consequently reduced the time they can spend on direct patient care and interactions with patients and their families. This shift is linked to burnout among healthcare professionals, which is known to adversely affect the quality of care and lead to increased healthcare costs. 26 Both of the two studies investigating the transition from pre- to post-EHR systems observed an increase in staff time allocated to documentation following EHR implementation. The first study by Asaro and Boxerman 27 assessed documentation periods at the outset and six months post-EHR introduction, whereas the second by Banner and Olney 28 compared these times at baseline and 12 months after EHR adoption. These findings imply that while EHR systems initially heighten documentation demands and disrupt established workflows, over time, they can enhance overall efficiency in work and information flow, thereby improving direct patient care and communication between healthcare providers. In two sequential studies at the same hospital, the first by O’Leary et al. 29 during the initial phase of transitioning to a fully integrated EMR system and the second 4 years later by Tipping et al. 30 during complete EMR implementation, notable shifts in hospitalists’ workflows were observed. The latter study showed a 5% reduction in physicians’ documentation time, an increase in communication time (from 24% to 26%), and a decrease in time for indirect care (from 69% to 64%), compared to the initial study. These changes highlight a successful adaptation to the EMR system, leading to more efficient documentation and improved communication without affecting the time dedicated to direct patient care.
Related work
A study in Ghana identified issues related to the use of e-healthcare through qualitative and quantitative assessments, including interviews and surveys with healthcare providers and consumers. Among the 23 fundamental issues identified and 107 valid responses, the lack of information and communication technology (ICT) infrastructure, financial sustainability, and privacy concerns were highlighted as key reasons for low adoption. These factors were rated on the Likert scale (from 1 to 7), where a lower average score indicates a higher priority issue, with average scores of 1.18, 1.71, and 1.70, respectively. 31 An online survey was done on 44 public health workers from 16 countries in Asia and Africa to determine the adaptation and acceptance of ICT in healthcare. While 93% of the participants positively reacted to the effectiveness of ICT guidelines and implementation, the lack of technology and its high prices along with the fear of increased workload were observed as potential barriers. 32 Osop and Sahama 33 conducted elaborate research on the perceived usability of EHR data in effective decision-making, through an online survey for doctors in Singapore. 96.6% of the respondents agreed that EHR systems helped in accessing patients’ diagnosis, medication, treatment, and laboratory test results. A study in Hong Kong conducted semi-structured interviews with 23 physicians and clinical assistants highlighting factors affecting the adoption of EMR systems. System complexity, financial and time cost, additional workload and its effect on regular clinical workflow, trust in technology, clinician-technology interaction, and infrastructural accommodation are some of the important determinants in the adaptation of technology. 34
Research gap and objectives
While many studies have looked at the benefits of EHRs,35–37 there's not much information on how limited access to digital health records affects doctors in similar contexts, such as Bangladesh. Hossain et al. 38 used the UTAUT (Unified Theory of Acceptance and Use of Technology) model to identify factors influencing the physician's adoption of the EHR systems in Bangladesh. This research utilized the partial least square (PLS) approach, a form of statistical analysis rooted in structural equation modeling (SEM), for examining the data gathered. The findings revealed that factors such as social influence (p < 0.05), facilitating conditions (p < 0.05), and personal innovativeness in information technology (p < 0.05) significantly impacted doctors’ intention to use the EHR system. Conversely, elements like performance expectation (p > 0.05), effort expectation (p > 0.05), and resistance to change (p > 0.05) did not exhibit a significant effect.
Therefore, our understanding of the effect of limited access to digital health records on healthcare professionals’ willingness to adopt such systems remains limited. Thus, the objective of this study has been to:
Investigate current patients’ medical history storage mechanisms and the associated challenges. Explore how doctors in contexts such as Bangladesh obtain and review patients’ past medical histories, and the challenges. Identify whether limited access to digital health records plays a role as an obstacle in clinical decision-making. Explore the factors influencing doctors’ willingness to adopt EHR systems in such contexts.
Understanding the above can help in improving EHR systems and encourage more doctors to use them. This is important because EHRs can make healthcare services safer and more efficient.
Method
This section describes the study design, data collection mechanism, study setting, criteria, sample size, and demographic profiles of the respondents.
Study design and data collection
This study employs an online cross-sectional survey method for data collection. The survey is structured into four sections, containing 22 questions in total. The first section gathers personal information, with five questions dedicated to this purpose. In the second section, the survey explores the respondents’ workload through four specific questions. The third section contains eight questions about challenges in taking patients’ medical histories. The fourth section lists five questions regarding the challenges faced by physicians in decision-making. For data acquisition, the questionnaire was set up in Google Forms and presented in English. In this study, the participation of the respondents was completely voluntary. On the consent page of the survey, participants were provided with an overview of the purpose of the study and their rights as study participants. These rights included the option to withdraw from the survey at any time without penalty, assurance that their responses would be kept confidential, and that the data would be used solely for research purposes.
Study setting, criteria, and sample size
Time duration and place: The data collection for the study was conducted over a period of 2 months, from July to August 2023. Participants from various health organizations in Bangladesh completed the survey online.
Inclusion and exclusion criteria: Participants were included if they had a degree equivalent to a Bachelor of Medicine, Bachelor of Surgery, or Bachelor of Dental Surgery (MBBS/BDS), at least two years of professional experience, and experience working in health organizations in Bangladesh. Exclusion criteria included lack of relevant professional qualifications or insufficient work experience.
Sample size: The sample size was determined based on the number of available and willing participants who met the inclusion criteria. Participants were selected through a combination of purposive and convenience sampling methods. Purposive sampling ensured that participants met specific criteria relevant to the study, such as having a degree equivalent to MBBS/BDS, at least 2 years of professional experience, and experience working in health organizations in Bangladesh. Convenience sampling included those who were readily available and willing to complete the survey. The study ultimately gathered responses from a sample size of 105 participants.
Data analysis
All the fields in the questionnaire were compulsory for each participant. Therefore, there were no missing values, nor were there any incomplete forms. All 105 forms qualified for the analysis. Python was used for data pre-processing, visualization, and model training. The pre-processing step involved utilizing pandas and numpy libraries for data manipulation and transformation. Feature engineering was conducted using techniques like one-hot encoding and label encoding. For visualization, tools such as pandas, matplotlib, plotly, and seaborn were employed. The construction of the ordinal regression model was facilitated using the statsmodels and sklearn libraries.
Participant demographics
Table 1 provides an overview of the survey's specifics and the demographics of the respondents. The survey revealed that 75.2% of the participants were male and 23.8% were female. Notably, respondents with over 20 years of experience form the largest group, representing 44.8% of the total. A substantial 55.2% of the doctors are employed in medical college hospitals. Moreover, a significant majority of the participants, accounting for 68.6%, are from urban areas. Additionally, Figure 1 illustrates the different specialties of the participating doctors. Although the questionnaire listed 77 specialties, including “Other.” “Other” ended up being the most mentioned among doctors. This was followed by pediatrics with 12 doctors, public health with 10 doctors, dentistry with nine doctors, and cardiology with seven doctors, among others. More details can be seen in Figure 1.

Distribution of clinical specialties among participating doctors.
Participants’ demography ( N = 105).

For “a” categories, multiple selections were allowed. Frequency shows choice counts, and percentage reflects the respondent share for each option.
Results
This section describes the major findings from the survey data analysis.
Observation-1: Data management methods
Figure 2 illustrates that only 4.8% of doctors store patients’ medical records digitally, while 51.4% go with paper-based archiving. A further 21.9% do not maintain any records, and an equal percentage of 21.9% utilize both digital and paper methods for storing records.

Distribution of data management methods.
The survey, as shown in Figure 3, investigated the challenges doctors face in clinical decision-making due to the absence of a comprehensive past medical history. Among doctors who rely solely on paper-based records, 56% report consistent challenges. This might be because paper records are hard to organize and access. In comparison, 52% of doctors who do not use any form of data storage also face similar challenges, likely due to the complete lack of historical patient data, which is crucial for informed decision-making. Interestingly, the number drops to 39% for doctors who utilize both paper-based and digital records, suggesting that the integration of digital methods might mitigate some difficulties associated with paper records alone. In clear contrast, only 20% of doctors using exclusively digital record systems face frequent difficulties, underscoring the advantages of digital records such as improved accessibility, organization, and efficiency in patient information management, crucial for clinical decision-making. Notably, if the EHR system is user-friendly, this percentage could be even lower. Supporting this, a study on health professionals’ perceptions in Bangladesh towards health sector digitization found that 91% believe the lack of user-friendly systems is a major barrier to digitization. 25
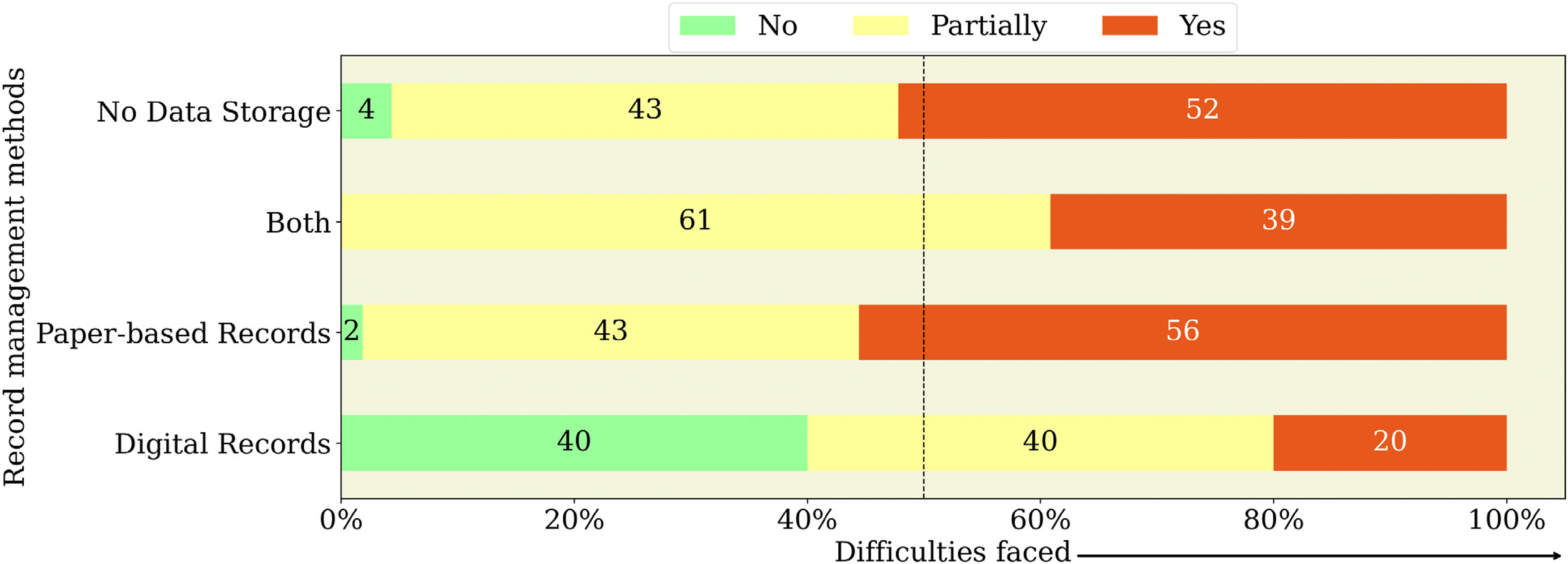
Impact of record management methods on clinical decision-making challenges.
The survey further investigated how doctors’ workload perceptions, measured on a Likert scale from 1 (“Never”) to 5 (“Every Time”), relate to their methods of maintaining past medical histories (Figure 4). Notably, doctors employing both digital and paper records reported higher workloads, with 39% indicating experiences of “Almost Every Time” or “Every Time.” A similar proportion (39%) of doctors without any data storage systems also reported high workloads as “Almost Every Time.” Conversely, those relying solely on paper-based records showed a slightly lower figure (35%) in the “Almost Every Time” and “Every Time” categories. In stark contrast, doctors using digital records predominantly reported lower workloads, often categorizing them as “Almost Never” or “Occasionally/Sometimes.” This trend suggests that efficient EHR systems may contribute to a more manageable workload, offering streamlined and less time-consuming processes for clinicians who adopt them.

Impact of record management methods on workload.
Observation-2: Obtaining and reviewing patients’ past medical history
The study, as depicted in Figure 5, investigates how doctors gather and review past medical histories. The majority (94.3%) primarily use direct patient interviews, a method that, while necessary, depends on patients’ memory and health literacy, impacting information accuracy. Approximately half (48.6%) use paper records, valued for their familiarity but vulnerable to damage and loss. A smaller group (18.1%) opts for structured medical history forms, which offer organization but can suffer from incomplete data due to patients’ limited knowledge. Lastly, 14.3% of doctors delegate the collection of patient histories to their assistants, a practice that saves time and allows for more patient interaction, but heavily depends on the accuracy of the assistants’ work, a key factor in the doctors’ decision-making process.

Methods used by doctors for obtaining patients’ medical records.
Figure 6 illustrates varying levels of decision-making challenges among doctors based on their methods of obtaining and reviewing patients’ past medical histories. It shows that 40% of doctors who primarily rely on assistants for patient history collection encounter occasional challenges, and 60% face these challenges frequently. Additionally, 53% of those using paper-based documents also frequently experience difficulties. In contrast, doctors who collect medical histories directly from patients or through filling out forms report fewer issues, with 4% experiencing no difficulties at all in these scenarios. This trend suggests that direct involvement in collecting medical histories leads to fewer decision-making challenges for doctors. Direct patient interactions or structured forms likely yield more accurate information, essential for sound clinical decision-making. These results highlight the value of personal engagement in medical practice and the drawbacks of indirect data collection.

Impact of medical records review methods on clinical decision-making.
Figure 7 shows increased workloads for doctors regardless of how they collect medical histories, whether it's through assistants, forms, direct interviews, or paper-based methods. Notably, 33% of doctors using assistants and 25% relying on paper report high workloads consistently. This could be attributed to the additional time spent reviewing paper-based records and verifying data collected by assistants, who may have limited medical knowledge—a point we’ll discuss later. In contrast, only 16% of those using forms face such workloads regularly. This pattern suggests that in places like Bangladesh, where doctor shortages are common, these collection methods contribute to significant workload stress.

Impact of medical records review methods on workload.
Facing the challenge of allocating enough time per patient while managing many others, doctors endure heightened workloads and stress.
Observation-3: Difficulties in doctors’ decision-making
To gain deeper insights, the survey asked doctors about various obstacles they encounter in clinical decision-making. They were given five options: insufficient past medical history, patients’ health literacy, unavailability of digital medical history, unavailability of summarized medical history, and lack of smart assistant. Figure 8 reveals significant insights into the challenges doctors face in clinical decision-making. A striking 81% of doctors identify the unavailability of past medical history as a primary obstacle, underscoring its importance in effective care. Additionally, 67.7% of doctors consider patients’ health literacy a significant challenge, indicating the need for clear communication in healthcare settings that do not rely solely on the patient’s memory or health literacy. The unavailability of summarized medical history is noted by 56.2% of doctors as an impediment, while 50.5% point to the lack of digital medical history, highlighting the growing need for digitization in medical record-storing. Interestingly, 34.4% of doctors identify the lack of a smart assistant as a barrier, marking a critical area for technological innovation.
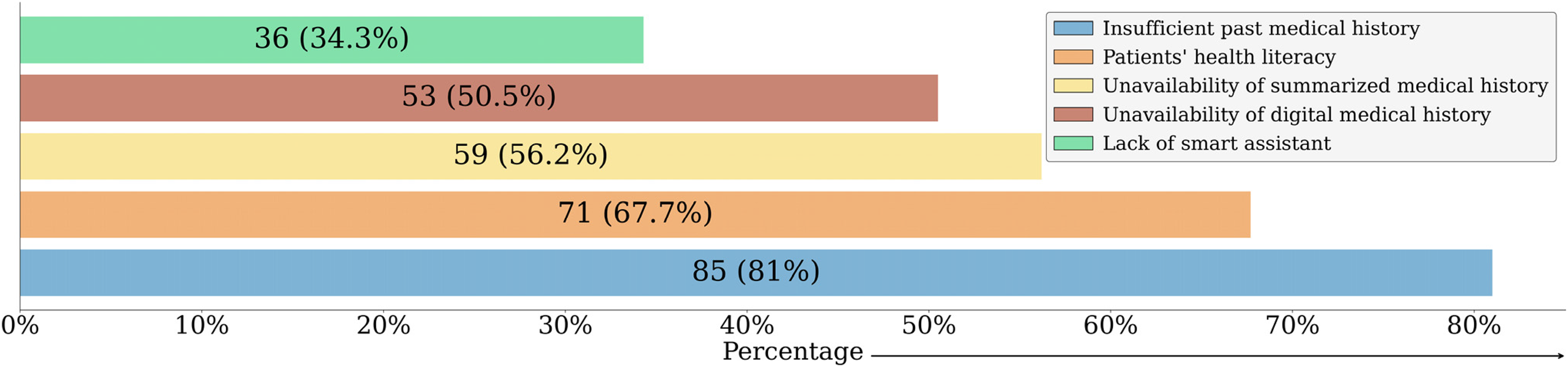
Challenges in clinical decision-making within healthcare settings.
For analytical clarity, “Insufficient past medical history,” “Unavailability of digital medical history,” and ‘Unavailability of summarized medical history’ were grouped under the collective term “Unavailability of medical history” as shown in Figure 9. In correlating these challenges with doctors’ workload ratings, a clear pattern was observed: those citing a lack of smart assistance predominantly report higher workloads, with 45% experiencing it almost every time and 25% every time. Similarly, doctors acknowledging patients’ health literacy as a hurdle also face considerable workloads (45% almost every time and 25% every time). Regarding the unavailability of medical history, 41% encounter high workloads almost every time and 26% every time. These findings are further elaborated in Figure 9. These findings suggest that the lack of smart assistance and challenges in patients’ health literacy might contribute more significantly to doctors’ workload than the absence of medical history. This observation leads to the potential utility of solutions like the Smart Health Gantt chart discussed in the study by Hossain et al. 39 Such a tool could significantly reduce workload by providing doctors with immediate access to comprehensive patient histories. Furthermore, it could serve as a valuable resource for assistants, enhancing their ability to support doctors effectively.

Impact of clinical decision-making challenges on workload.
Observation-4: Factors influencing doctors’ use of patient lifelong medical history
The survey queried doctors’ willingness to use a simplified, web-based system offering a one-window overview of a patient's lifelong medical history.39,40 They responded on a Likert scale ranging from “Not at All Interested” to “Extremely Interested.” As illustrated in Figure 10, a notable 64.7% of doctors expressed an extremely high level of interest in this system, and an additional 16.2% displayed very high interest. Further analysis in Figure 11 examines the correlation between this willingness and the challenges they encounter in clinical decision-making. Among those who identified the lack of a smart assistant as a challenge, 72% are extremely interested in the system. Similarly, 63% of doctors who pointed to patients’ health literacy as an issue are also extremely interested. Additionally, 66% of those facing challenges due to the unavailability of medical history showed an extremely high level of interest in this system.

Doctors’ willingness to adopt the proposed electronic health record system.

The role of clinical decision challenges in accepting new healthcare systems.
Furthermore, it was important to comprehend the factors influencing doctors’ willingness to utilize the described system. The dependent variable, representing doctors’ willingness to use the described system, is ordinal in nature, ranging from 1 to 5. Given that information and the categorical nature of the independent variables, ordinal regression is the most appropriate model for our analysis. Before the model training phase, a correlation analysis was performed to evaluate the relationships between different variables. The analysis was guided by established thresholds for interpreting correlation strength as described below.
Very strong correlation: 0.9–1.0 (or −0.9 to −1.0) Strong correlation: 0.7–0.9 (or −0.7 to −0.9) Moderate correlation: 0.5–0.7 (or −0.5 to −0.7) Weak correlation: 0.3–0.5 (or −0.3 to −0.5) Weak/no correlation: 0–0.3 (or 0 to −0.3)
In line with these criteria, the inclusion of any two variables in the model together was avoided if their correlation exceeded 0.4, to minimize the risk of multicollinearity. The outcomes of this correlation analysis are presented in a heatmap in Figure 12. For this analysis, the corr method from the pandas library was employed, selecting the Spearman option due to the inclusion of ordinal and non-normally distributed variables in the dataset. Additionally, the decision was made to remove Q7 (daily working hours) from the set of independent variables due to its high correlation with Q8 (actual hours worked per day), observing an enhancement in the model's performance without it.

Correlation heatmap.
Additionally, the statsmodels library in Python was utilized for the implementation of the Ordinal Regression Model. This model was instrumental in evaluating the influence of our independent variables on the dependent variable, that is, the willingness to use the proposed system, and assessing their statistical significance. The results, as shown in Table 2, reveal that three independent variables, namely Q2 (physicians’ disciplines), Q9 (workload ratings), and Q17 (efficiency level of the current workplace in facilitating patient history-taking), each had a p-value below 0.05. This indicates a statistically significant positive relationship with the dependent variable. The model's results suggest these associations are not due to random chance.
The model results.

Discussion
The main objective of this study was to examine the influence of digital health record systems on clinical decision-making and doctors’ workload in Bangladesh. It provided a comprehensive analysis of the current state of data management methods in the Bangladeshi medical community and their implications for clinical decision-making and workload, as well as the willingness of doctors in these contexts to use EHR systems. Our findings revealed that only 4.8% of the surveyed doctors exclusively used digital records, while 51.4% relied on paper-based methods. Additionally, 21.9% did not maintain any records, and another 21.9% used both digital and paper methods. The survey results indicated that doctors using paper records or no records at all faced substantial challenges in clinical decision-making due to the lack of accessible and organized patient history. Conversely, doctors utilizing digital records reported significantly fewer challenges, highlighting the efficiency, organization, and improved accessibility that digital systems offered. The study also examined how doctors gathered and reviewed patients’ past medical histories. A vast majority (94.3%) relied on direct patient interviews, which could be unreliable due to patients’ memory and health literacy. About 48.6% used paper records, which, while familiar, were prone to damage and loss. Only 18.1% used structured medical history forms, and 14.3% depended on assistants. The challenges associated with these methods were evident, as doctors using assistants and paper records frequently experienced difficulties in decision-making. This trend was less pronounced among those using digital records or structured forms, emphasizing the importance of direct involvement and reliable data collection methods in reducing decision-making challenges. The survey identified several critical obstacles in clinical decision-making, including insufficient past medical history (81%), patients’ health literacy (67.7%), unavailability of summarized medical history (56.2%), and lack of digital medical history (50.5%). These challenges significantly impacted doctors’ workload, with those lacking smart assistance or facing health literacy issues reporting the highest levels of workload stress. The absence of comprehensive medical history further exacerbated these issues, suggesting that solutions like the Smart Health Gantt chart described in the survey could alleviate these burdens by providing immediate access to complete patient histories. The willingness of doctors to adopt a simplified, web-based system for accessing lifelong patient medical history was remarkably high, with 64.7% expressing extreme interest. This interest correlated strongly with the challenges they faced in clinical decision-making, particularly the lack of smart assistance and patients’ health literacy issues. The ordinal regression model analysis showed a significant positive relationship between doctors’ willingness to use the system and factors like workload rating, physicians’ disciplines, and the efficiency of current workplace practices in facilitating patient history-taking. The findings of this study provide valuable insights into the current challenges faced by doctors in a developing country like Bangladesh and highlight the potential benefits of adopting EHR systems.
Scholarly and policy implications
This study highlights the challenges of non-digital patient record management, with only 4.8% of doctors using digital records. Doctors using digital records face fewer challenges (20%) compared to those using paper records (56%), which can lead to problems such as lost records, difficulty sharing information, and damage. These findings emphasize the benefits of EHR systems for data management and clinical decision-making. Limited access to comprehensive past medical histories increases doctors’ workloads and decision-making challenges. These results underscore the need for EHR adoption to improve healthcare efficiency and inform policy initiatives promoting digital health records. From a policy perspective, the findings emphasize the need for initiatives promoting the adoption of EHR systems. Policymakers should consider measures such as grant programs to support EHR implementation, streamlined regulations for EHR-adopting facilities, and funding for training programs to ensure healthcare professionals are equipped to utilize EHRs effectively.
Limitations and future research
Like any other study, this research has its limitations. This study used a combination of purposive and convenience sampling for survey data collection, rather than a random sampling approach, and included a relatively small sample size. Consequently, caution is needed before applying these findings more broadly. Additionally, considering the demanding schedules of experienced doctors in Bangladesh, a formal sample size calculation was not performed. Instead, the final sample size was determined by the number of participants who met the inclusion criteria and agreed to participate within the data collection period. This approach was necessary to accommodate practical constraints and ensure the participation of qualified doctors. Moreover, the questionnaire has not been previously validated, and no pilot testing was conducted. This may affect the generalizability of the data collected. Despite these limitations, the insights gained are still valuable, particularly given that participants were required to have at least MBBS/BDS degrees and a minimum of two years of experience in Bangladesh. Moreover, to our knowledge, this is the first study that investigates the impact of different medical record methods on doctors’ workload and decision-making in Bangladesh. Future research should address these limitations by employing random sampling methods and larger sample sizes to enhance the generalizability of the findings. Additionally, pilot testing and validation of the questionnaire should be conducted to improve the reliability of the survey instrument. Further studies could also explore the long-term impacts of EHR adoption on clinical outcomes and healthcare efficiency. Investigating the cost-effectiveness of implementing EHR systems in developing countries like Bangladesh would provide valuable insights for policymakers. Lastly, comparative studies between different regions or countries could help identify best practices and inform more effective EHR implementation strategies.
Conclusion
Our study highlights the importance of having EHR systems in contexts such as Bangladesh. Doctors face substantial challenges in clinical decision-making due to limited access to comprehensive medical records, with most relying on paper-based methods or having no formal data storage. This reliance increases workloads and complicates decision-making, compounded by patients’ memory limitations and variable health literacy. Our findings reveal that these difficulties are often exacerbated by patients’ health literacy and the lack of smart assistance, rather than just the unavailability of medical histories. There is a strong preference among doctors for adopting EHR systems, influenced by their disciplines, workload, and current workplace efficiency. EHR adoption is anticipated to improve clinical decision-making, streamline processes, and enhance healthcare delivery. Policymakers should consider phased implementation, training programs, and leveraging existing infrastructure. Future research should validate EHR effectiveness and explore cost-effective implementation strategies in resource-limited settings like Bangladesh.
Footnotes
Acknowledgements
The authors extend their gratitude to the members of the SocialTech Lab at Kyushu University for their valuable feedback and support throughout the development of this paper.
Contributorship
MMB, FH, PP, and MR collectively conceived and designed the study. AA was added as a supervisor. FH and MR collaborated on the development of the questionnaire and were responsible for data collection. MMB and PP conducted data analysis and drafted the initial manuscript. RI provided feedback on the data analysis, and NN provided feedback from a medical point of view. AA provided valuable feedback and played a substantial role in editing, preparing, and reviewing the manuscript. All authors reviewed the manuscript and approved its final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MMB.