
Abstract
Objective
Rapid digitisation of health occurred during the COVID-19 pandemic worldwide. In October 2020, we conducted a survey on digital health technology use in Germany. This study aimed to conduct a second survey to investigate in more detail the internet use in health context and digital technology use for health promotion and disease prevention in Germany.
Methods
A cross-sectional, nationwide telephone survey was conducted in November 2022. Anonymous data on internet and digital technology use, digital health literacy, and sociodemographic characteristics were analysed using descriptive statistics and binary logistic regressions.
Results
The 1020 participants were aged 18–92 years, 53% were male, 62% completed primary or secondary education, 71% resided in large cities, and 45% reported a country-average net household income. Overall, 61% reported internet use in health context via 1–4 devices. Among those, more than 50% used the internet and apps to obtain general health information and less than 50% used digital technologies for physical activity promotion or cancer prevention. Overall, 34% were confident in using the internet for health decisions and 71% preferred to receive health information non-digitally (e.g. on paper). Internet, app, and digital technology use were associated with higher digital health literacy and income, and residence in larger cities. Digital technologies were used for physical activity promotion by younger and for cancer prevention by older participants.
Conclusion
The internet and digital technologies were predominantly used to obtain health information, but less often for health promotion and disease prevention in 2022 in Germany. While health app and digital technology use for physical activity promotion increased, the confidence in using online information for health decisions decreased in 2022 relative to 2020. Factors that promote confidence in online health information and digital technology use for health promotion and disease prevention need to be investigated in future studies.
Keywords
Introduction
Widespread internet access and the introduction of smartphones and other mobile devices since around 2009 have greatly contributed to the digitisation of health worldwide. 1 In addition to healthcare, digital technologies can be used in the public health context for health promotion and disease prevention, for example by providing access to health education and allowing self-monitoring of health-related behaviours. 2 Opportunities associated with increasing digitisation in these fields include greater reachability of people via commonly used digital technologies, such as smartphones or health websites, objective monitoring of health parameters, and widespread availability of health-related information. 3 However, digitisation in health context is associated with several challenges for public health research and action, such as ethical and legal aspects of data acquisition, storage, and usage, 4 or inequalities in the access to and use of digital health technologies (digital divide). 5
With the onset of the COVID-19 pandemic, the use of digital technologies for health-related purposes increased rapidly worldwide. 6 We investigated the attitudes towards and the use of digital technologies in any health context in Germany using a cross-sectional survey of internet users in October 2020. 7 The data were collected from 1014 internet users aged 14–93 years recruited nationwide from a consumer panel of residents in Germany. Although most participants (89%) expected that digitisation will be important for therapy and healthcare in the future, their interest in and the actual use of digital health technologies was relatively low (e.g. 26% planned to download health apps and 22% reported using digital technologies for physical activity promotion). 7 Furthermore, 43% were confident in using online information for health decisions. 7 Other surveys performed using large samples recruited from the general population in Germany during the COVID-19 pandemic also reported similar results. For example, the use of symptom checker health apps was low 8 and some participant groups reported difficulties in locating and evaluating health information online.9,10,11,12 Survey studies from other countries13,14,15 also reported that participants were motivated to use digital health technologies, although they also raised doubts regarding the quality of information and safety of these technologies.
While our first survey conducted in October 2020
7
provided an interesting snapshot of attitudes towards digital technology use in the health context in Germany, it is unclear if and how these attitudes have changed considering the rapid digitisation of health during the COVID-19 pandemic. This study aimed to conduct a second survey in Germany, two years after the first survey, to investigate in more detail the internet use in health context and digital technology use for health promotion and disease prevention. While in 2020 we investigated the general attitudes to digital health,
7
the focus of the second survey was on the details of the internet and app use in health context (e.g. devices for use and contextual factors, such as preferences and interest in digital health technologies that could be associated with such use) and digital health promotion and disease prevention (i.e. in COVID-19-context and for physical activity promotion and cancer prevention). The second survey aimed to answer five research questions:
What are the attitudes towards and the use of internet and apps in health context? What contextual factors (e.g. interest in digital health technologies) are associated with the internet use in health context? What are the attitudes towards and the use of digital technologies for health promotion and disease prevention focusing on COVID-19, physical activity promotion, and cancer prevention? What is the perceived digital health literacy in survey participants? Who uses the internet, apps, and digital technologies in health context based on their sociodemographic characteristics and digital health literacy?
Methods
Study design and protocol
This study is a cross-sectional survey with the same design and methodology as our first survey. 7 The study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline 16 (Table A1 in Appendix). A protocol for this study was prospectively registered. 17
Ethical considerations
This study was performed in collaboration with an international market research company (Cerner Enviza GmbH, Munich, Germany that is a former health division of Kantar GmbH and currently belongs to Oracle Cerner GmbH). Participants were recruited from a consumer panel that was set up and administered by Cerner Enviza GmbH. Panel members gave a verbal informed consent to be contacted for telephone survey purposes according to the Cerner Enviza GmbH data privacy policy. 18 Although such verbal consent was not formally documented according to the Cerner Enviza GmbH data privacy policy, 18 this study adheres to the ethical guidelines according to the Declaration of Helsinki 19 in terms of the lack of physical and psychological harm (i.e. short survey length and survey items on a non-sensitive topic of internet user preferences regarding digital technology use for promoting own health), the lack of deception, and the adherence to the data protection guidelines (i.e. anonymous data collection, no access to participant contact information by study researchers, fully anonymised dataset, and data storage on a secure server of an academic institution). Participation was voluntary, termination was possible at any time, and completing the survey did not pose any risks to the participants. We purchased a fully-anonymised dataset from Cerner Enviza GmbH. Since we did not have any contact with the participants, we did not seek an approval to analyse such anonymous data from our institutional ethics committee.
Participants
The survey participants were recruited from a consumer panel by Cerner Enviza GmbH. The consumer panel consists of a nationwide sample recruited from the general population of Germany with known sociodemographic characteristics, including age, sex, education, employment, household size and income, and residence region by population size and federal state. The inclusion criteria for this study were: (1) adult aged 18 years or older, (2) internet user, (3) residing in Germany at the time of data collection in November 2022, and (4) able to participate in the survey in German. The sample size of at least 1000 participants was chosen based on the first survey. 7
Procedure
The survey data were collected by Cerner Enviza GmbH in November 2022 using computer-assisted telephone interviews performed by experienced interviewers, as in the first survey. 7 Panel members were contacted via telephone using a random-digit-dial method, verbally invited to participate in a survey on the use of digital technologies to stay healthy or to improve health, and those who provided verbal informed consent subsequently participated in the survey. A dual-frame approach was used to reach landline and mobile-only users. The survey was conducted in German and took about 15 minutes per person.
Survey instrument
The survey instrument was a questionnaire with 30 items and additional sociodemographic items, including age, sex, education, employment, household size and income, and residence region by population size and federal state (Figure 1).

Topics in the survey instrument (questionnaire with 30 items).
Overall 15 items (Figure 1, topics 1–2) focused on the internet, app and digital technology use in any health context or specifically for health promotion and disease prevention. These items were adapted (i.e. revised in terms of content or answer options) from the first survey 7 or self-developed. The focus of digital health promotion and disease prevention items was especially on physical activity promotion that has evolved during the global pandemic, with online personal training or exercise classes, wearable technologies, and mobile exercise apps being identified among the top 20 global fitness trends in 2022. 20 We also included items on digital cancer prevention because some aspects of cancer care, such as screening or diagnostic procedures were partially disrupted during the COVID-19 pandemic in Germany. 21 Cancer prevention could be supported by digital technologies in terms of providing information on cancer types, risk factors, and screening. 22 Further 10 items (Figure 1, topic 3) assessed digital health literacy using the German version 23 of the eHealth Literacy Scale (eHEALS). 24 The eHEALS is an open-access scale with acceptable psychometric properties.23,24 It consists of eight items rated on a 5-point Likert scale (from 1 = strongly disagree to 5 = strongly agree) that measure a single construct of digital health literacy (i.e. the ability to search for, find, evaluate, and use internet-based health resources). 24 The digital health literacy was computed as the eHEALS sum score per participant that can range from 8 to 40 points (i.e. lowest to highest digital health literacy). Due to the lack of cut-off scores on the eHEALS, we classified digital health literacy into three groups (low digital health literacy: 8–19 points; moderate digital health literacy: 20–29 points; and high digital health literacy: 30–40 points). We also included two supplementary items for the eHEALS that assess the interest in using digital health measures in general. 24 Finally, we developed five new items (Figure 1, topic 4) to assess contextual factors associated with internet use in health context based on three elements of the Capability, Opportunity and Motivation to Behaviour (COM-B) model embedded in the Behaviour Change Wheel (BCW). 25 The BCW is a theoretical framework for understanding individual beliefs, social norms, and environmental factors that influence health behaviours. The new items did not test behaviour change per se, but rather addressed the factors that could facilitate or prohibit internet use in health context according to the three COM-B elements, including capability (i.e. knowledge and skills forming psychological and physical capacity to perform a behaviour), opportunity (i.e. physical and social environments that, as external factors, make a behaviour possible), and motivation (i.e. personal beliefs, emotions, and goals that drive or enhance the willingness to engage in a behaviour).
Among all items, there were mandatory, filter, and optional items (depending on the responses on the filter items) with single or multiple answer options. The answer options included binary responses (yes or no) or Likert scale ratings with 4 points (i.e. strongly disagree to strongly agree) or 5 points (i.e. including a neutral rating for the eHEALS items).
The survey instrument was pretested by Cerner Enviza GmbH and item content or answer options were revised by study authors where necessary. The final version of the survey instrument was developed (Figure 1) and uploaded open-access online at the Open Science Framework. 26
Statistical analysis
Anonymised data per participant were purchased from Cerner Enviza GmbH and stored on a secure server of the academic institution of the first author. The statistical analysis was performed on raw (unweighted) responses on all items in IBM-SPSS24 (IBM Corp., Armonk, NY, USA). We descriptively analysed the responses on all items using absolute and relative frequencies. We also computed Cronbach's alpha to measure the internal consistency of the eight eHEALS items. Furthermore, we computed four binary logistic regression analyses to investigate the associations between each of the four dependent variables (i.e. internet use in health context, app use in health context, digital technology use for physical activity promotion, and digital technology use for cancer prevention, each coded as yes or no) and seven independent variables (i.e. sociodemographic factors: age, sex, education, and household income; structural factors: residence region by population size and by federal state; contextual factor: digital health literacy). We chose the independent variables based on the pattern of associations observed in the first survey 7 and also included the residence region as a proxy for the internet access. Employment status and household size were not included in the regression analyses because they positively correlate with the household income (one of the independent variables already included in the regression analyses).
Results
Participant characteristics (N = 1020)
The data were obtained from 1020 internet users who resided in any of the 16 federal states in Germany in November 2022 (Figure 2). The survey was performed via landline (759/1020, 74%) or mobile telephones (261/1020, 26%).

Participant residence by federal state in Germany (N = 1020). Note. Own figure made in GIMP 2.10.36 XCF (copyright: Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany).
All 1020 participants reported their sociodemographic characteristics and were asked about the number of devices via which they use the internet to stay healthy or to improve their health. Participants who responded that they use 1–4 devices were classified as ‘internet users in health context’ (626/1020, 61%) and subsequently completed parts 1–4 of the survey (Figure 1). The rest of the participants (394/1020, 39%) did not report the number of devices via which they use the internet to stay healthy or to improve their health. These participants were classified as ‘internet users’ because they were not sure about their device or internet use in health context. This group subsequently completed parts 3–4 of the survey (Figure 1).
The characteristics of all 1020 participants and participants per group (n = 626 internet users in health context and n = 394 internet users) are reported in Table 1. All participants were aged 18–92 years. Age was categorised into three similar-sized groups based on presumed digital exposure and variable distribution: (1) younger age with higher digital exposure (18–49 years), (2) middle age with mixed digital exposure (50–64 years), and (3) older age with lower digital exposure (65–92 years). Most participants were male (53%), had low to middle level of education (62%), resided in large cities with at least 100,000 residents (71%) and in the states of the former West Germany (81%), were employed or seeking employment (58%), and lived in 1–2-person households (71%). Overall, 45% reported high household income, 76% good to very good health status, and 94% had a general practitioner.
Participant characteristics.

Note.aThe mean net household income in Germany was 3813 Euro/month in 2021. 27
Compared to internet users, internet users in health context tended to be younger, more educated, have higher income, be employed, and reside in large cities (Table 1).
Internet and app use in health context (n = 626/1020)
Internet use in health context
The 626 participants accessed the internet in health context predominantly via smartphones or tablets and computers or laptops (Figure 3). The reasons for internet use were predominantly to obtain general health or COVID-19 information. The accessed website types included any general websites or official health websites (e.g. from the federal Robert Koch Institute responsible for disease control and prevention in Germany).

Internet use in health context (n = 626/1020).
App use in health context
Among 626 participants, 63% (394/626) reported using health apps on their smartphones or tablets. Most app users (355/394, 90%) rated health apps as easy to use. The reasons for app use were predominantly to obtain information on COVID-19 (265/394, 67%) or general health information (248/394, 63%).
Digital technology use for health promotion and disease prevention (n = 626/1020)
COVID-19
The participants reported that they find online information on COVID-19 that may be inaccurate either often (137/626, 22%), sometimes (180/626, 29%), seldom (189/626, 30%), or never (86/626, 14%) while 5% (34/626) did not have an opinion.
Physical activity promotion
Among 626 participants, 44% (278/626) reported using any digital technologies to support physical activity. Most users (256/278, 92%) rated such digital technologies as easy to use. The use reasons were predominantly to measure own physical activity (207/278, 74%) or to find exercise ideas (158/278, 57%). The used devices were predominantly smartphones or tablets (213/278, 77%) and activity trackers or smartwatches (161/278, 58%). Most users reported weekly to daily use (254/278, 91%) and rated the feedback from digital technologies as helpful to be physically active (191/278, 69%).
Cancer prevention
Among 626 participants, 35% (217/626) reported using any digital technologies for cancer prevention. Most users (195/217, 90%) rated such digital technologies as useful. The use reasons were predominantly to obtain general information on cancer (188/217, 87%) and cancer risk factors (159/217, 73%).
Digital health literacy (n = 932/1020)
Among 1020 participants, 91% (932/1020) provided complete responses on all eight eHEALS items and were included in the analysis. The internal consistency of eHEALS was high in this study based on Cronbach's alpha value of 0.89.
Assessment of the individual eHEALS items revealed that more than 50% of participants (i.e. 65–84%) agreed or strongly agreed that they are able to search, find, and evaluate health-related information online on items 1–7 (Figure 4). However, less than 50% of participants (i.e. 34%, 317/932) agreed or strongly agreed that they are confident in using online information for health decisions on item 8. Based on the supplementary items, 70% (657/932) of participants agreed or strongly agreed that it is important to access health information online while 40% (377/932) agreed or strongly agreed that the internet is useful for making health decisions (Figure 4).

Digital health literacy (n = 932/1020).
Digital health literacy (i.e. the eHEALS sum score) was high with 30–40/40 points in 57% of all participants and in most (i.e. 69%) of the internet users in health context (Table 2). In contrast, digital health literacy was moderate with 20–29/40 points in most (i.e. 45%) of internet users (Table 2).
Digital health literacy by group.
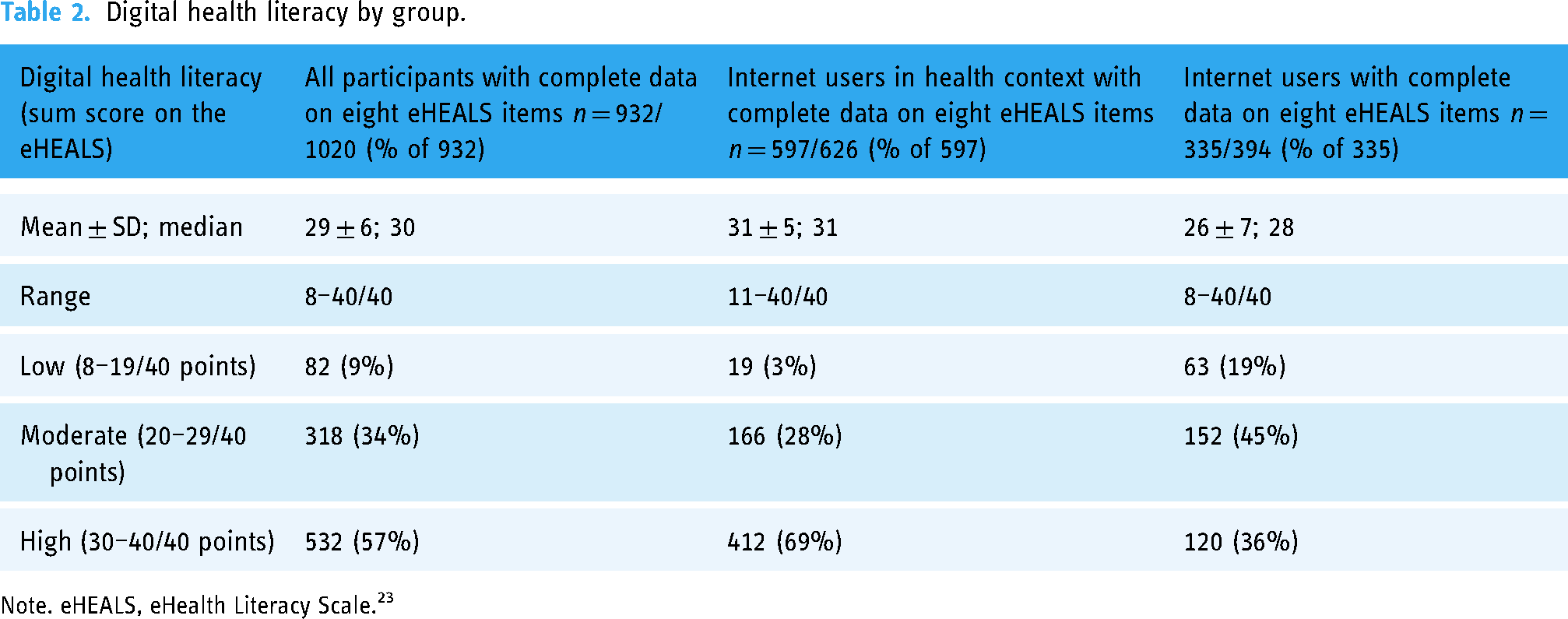
Note. eHEALS, eHealth Literacy Scale. 23
Contextual factors associated with internet use in health context (N = 1020)
Among 1020 participants, less than 50% agreed or strongly agreed that they trust health websites (39%), have people in their social network who rely on the internet for health information (35%), first consider the internet when needing health information (39%), and are interested in digital health technologies (40%; Figure 5). Most participants (71%) agreed or strongly agreed that they prefer to receive health information in non-digital formats, such as in personal consultation or on paper.
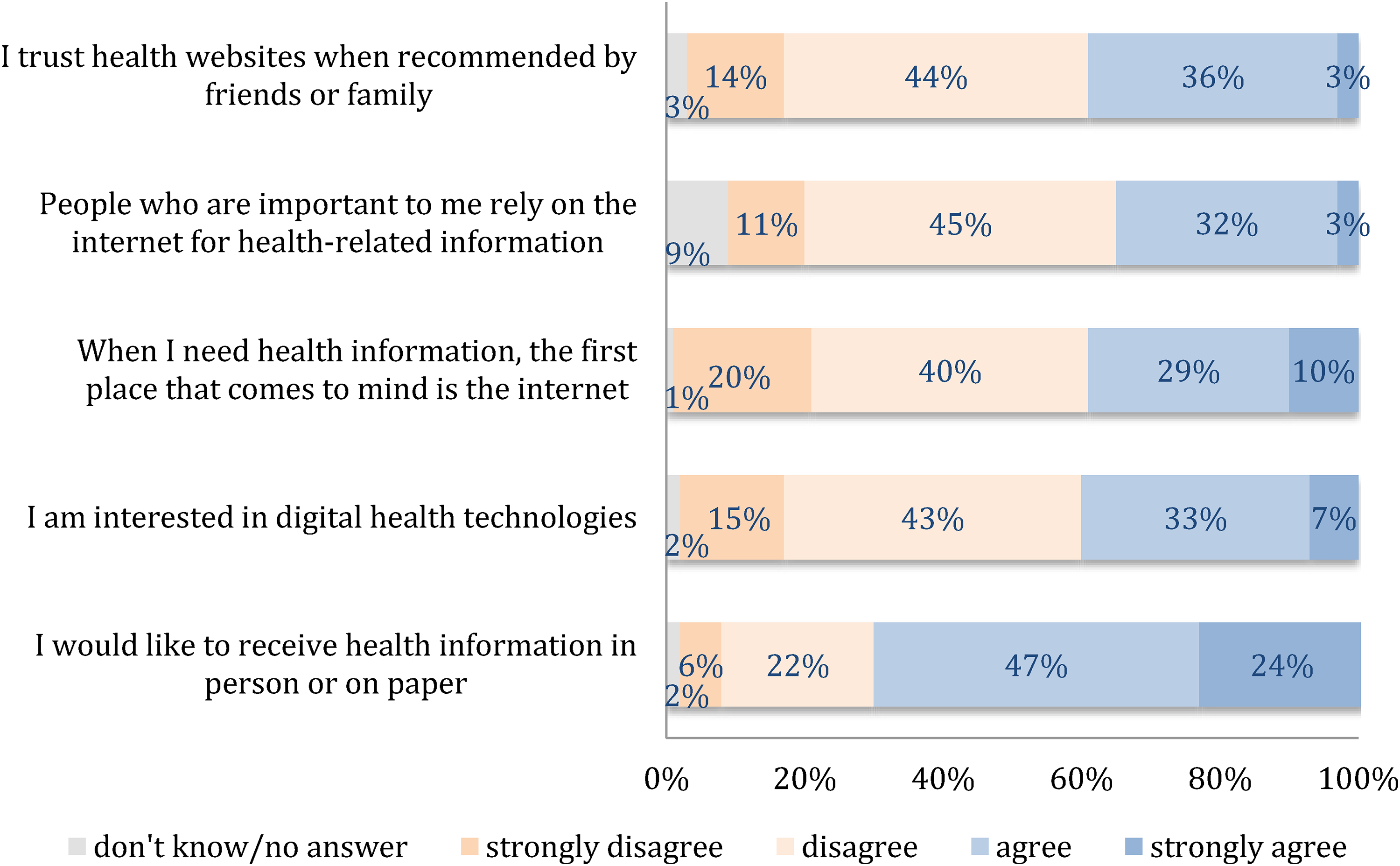
Contextual factors associated with internet use in health context (N = 1020).
Relative to internet users, more internet users in health context agreed or strongly agreed that they trust health websites, have people in their social network who rely on the internet for health information, first consider the internet when needing health information, and are interested in digital health technologies (Figure 6). In contrast, less internet users in health context than internet users agreed or strongly agreed that they prefer to receive health information in non-digital formats, such as in personal consultation or on paper.

Contextual factors associated with internet use in health context by group.
Who uses the internet, apps, and digital technologies in health context?
Four binary logistic regression analyses were computed to test the associations between the internet and digital technology use in health context and participant characteristics (Table 3). The statistically significant predictors identified in these analyses are visualised in Figure 7.

Characteristics of the internet and digital technology users in health context.
Associations between the internet and digital technology use in health context and participant characteristics.

Note. Results of four binary logistic regression analyses using data from participants with complete responses. Independent variables with small categories in Tables 1 and 2 were combined into single categories (i.e. primary and secondary education, low and middle household income, small and middle-sized cities, and low and moderate digital health literacy).
Abbreviations: Χ2, chi-square; CI, confidence interval; df, degrees of freedom; OR, odds ratio; R, reference category coded 0.
*p < .05.
Relative to internet users, internet users in health context were younger, resided in large cities, and had high digital health literacy, while app users in health context were wealthier (Table 3). Digital technologies were used for physical activity promotion by younger participants and those residing in large cities, and for cancer prevention by middle-aged to older participants and those with high digital health literacy (Table 3).
Discussion
Main results
This study investigated the internet and digital technology use in any health context and for health promotion and disease prevention among 1020 internet users in Germany. The survey data collected in November 2022 show that over half of the surveyed participants reported using the internet in health context via 1–4 devices, while the rest were not sure about their device or internet use in health context. The internet and digital technologies were predominantly used to obtain health information, but less often for health promotion and disease prevention. Interestingly, despite being internet users, less than half of the participants (34%) were confident in using the internet for health decisions and the majority (71%) preferred to receive health information non-digitally (e.g. on paper). Internet, app, and digital technology use were associated with higher digital health literacy and income, and residence in larger cities. Digital technologies were used for physical activity promotion by younger and for cancer prevention by older participants. Thus, this study highlights a complex role of digital technologies and their use in health context. The survey could be translated and adapted to investigate the use of digital health technologies beyond Germany.
Digital technology use in health context
Internet or digital technology use in the health context has hardly changed in Germany (i.e. was reported by 57% of 1014 survey participants in 2020 7 and 61% of 1020 survey participants in 2022). This result is somewhat surprising considering the widespread digitisation of daily life that occurred during the COVID-19 pandemic. Despite such digitisation, some survey participants in 2022 were either unsure if they use the internet in health context or might have been reluctant to use the internet due to the overabundance of false health information online (the so-called ‘infodemic’ 10 ). A further barrier to the internet or app use in health context could be insufficient information about privacy and data use. Thus, users are often unclear about what data are collected, who has access to their data, and how the data are processed by third parties.4,5,6 However, some participants may have underestimated or did not consider their online behaviour, such as searching for general health information, as internet use in health context. As expected, those who reported the internet use stated that they use the commonly owned devices (i.e. smartphones, tablets, or computers) predominantly to obtain general health information. Furthermore, compared to relatively low interest in health apps in 2020 (i.e. reported by 26% of participants 7 ), the health app use was reported by 63% of internet users in health context in 2022, most likely due to the use of COVID-19-tracing apps during the pandemic. Interestingly, more than half of participants in 2022 reported using official health websites. Further research should focus on the evaluation of official or verified health websites to determine how the users find, use, and rate such resources online. Furthermore, a sufficiently high level of digital health literacy is necessary to promote digital technology use in health context. 11 In general, digital health literacy consists of confidence in finding, using, evaluating, and applying online information in health context. 28 Our results show that among the digital health literacy items on the eHEALS especially the confidence in using online information for health decisions decreased from 43% in 2020 7 to 34% in 2022. We can only speculate that such lower confidence is indeed a positive development because it might reflect that the general population is more aware of the need to assess the online health information as a consequence of the infodemic. As suggested by others,9,12 various aspects of digital health literacy should be addressed by interventions that aim to improve the capacities to seek and evaluate health information online. Despite their internet use, most participants in 2022 preferred to receive health information non-digitally (e.g. on paper). As suggested in another survey in Germany, 8 people who have a general practitioner (i.e. the majority of this survey participants) might prefer to consult healthcare professionals rather than digital health technologies. Qualitative methods could be used to investigate in more depth the reasons for low confidence in online information for health decisions and whether such confidence depends on the type of health decisions.
Digital health promotion and disease prevention
Digital technology use for health promotion and disease prevention (i.e. in the context of physical activity promotion and cancer prevention) was reported by less than 50% of participants in 2022, although such use in the context of physical activity promotion increased from 22% in 2020 7 to 44% in 2022. Since users rated such technologies as useful and easy to use in 2022, digital technologies could support health promotion and disease prevention by delivering health information (e.g. on cancer prevention via apps 22 ) and encouraging healthy behaviour. In fact, high satisfaction with device feedback and the ability to measure physical activity were reported in the context of physical activity promotion in this study. Digital technologies with such unique features, including wearables and mobile exercise apps were also included among the top 20 global fitness trends in 2022. 20 If the use of such digital technologies in daily life leads to a long-term behaviour change, including an increase in physical activity, then this could contribute to a lasting improvement in health. 2 Further research is needed to evaluate the benefits and also identify any potential risks of using digital technologies for health promotion and disease prevention. 29
Factors associated with internet use in health context
This study supports the argument that the internet use in health context depends on the three components of the COM-B model (i.e. capability, opportunity and motivation). 25 Specifically, the internet use in health context was associated with higher capability (e.g. higher interest in using the internet when needing health information), higher opportunity (e.g. more digitised social network), and higher motivation (e.g. the interest in digital health technologies). Thus, these components of the COM-B model are the potential determinants of (digital) health behaviour change that may occur as a consequence of internet use in health context according to the Theoretical Domains Framework (TDF).30,31,32,33 Furthermore, patterns of digital technology use observed in this study may reflect the interests of different age groups (e.g. younger for physical activity promotion and older for cancer prevention), but also be attributable to digital divide that arises when more privileged people use and potentially benefit from digital health technologies. 34 Indeed, internet and digital technology use in health context were associated with higher digital health literacy, higher income, and residence in larger cities as a proxy for better internet access in 2022. Furthermore, internet users who reported the number of devices that they use to access the internet in health context tended to be younger, more educated, have higher income, be employed, reside in large cities, have higher digital health literacy, have more digitised social network and interest in digital health technologies relative to internet users who were not sure about their device or internet use in health context. Thus, this study provides some evidence for the inequalities in the access to and use of digital health technologies (i.e. digital divide) meaning that only some population groups (i.e. those more privileged) appear to use and may benefit from the digital health technologies. 5 Further research is needed to examine the individual interests and structural factors, such as the internet access in the context of digital health technology use.
Strengths and limitations
The main strength of this study is the large and age-diverse sample of internet users who were recruited nationwide in Germany to participate in the survey. There were several limitations in this study. First, this study is based on data purchased from an external provider (a market research company, Cerner Enviza GmbH). Thus, we could not evaluate the scientific quality of participant recruitment or data collection procedures. In general, the participants had little motivation to purposefully bias the responses on all survey items, although general biases associated with any surveys (e.g. social desirability bias) cannot be ruled out. The advantage of working with an experienced market research company is that a large sample of participants was recruited and participated in the survey over a short time period (i.e. in November 2022). Thus, any biases related to certain time periods, such as changes in COVID-19 restrictions or in physical activity during different seasons, could be reduced. Second, since the data were collected by an external provider based on their data privacy policy 18 and we did not have any contact with the participants, we did not seek an approval to analyse such anonymous data from our institutional ethics committee. In general, the study follows the ethical guidelines according to the Declaration of Helsinki 19 although the verbal informed consent to participate in the survey was not documented. Third, our results cannot be generalised to the general population in Germany. Although we did not evaluate the sample representativeness, our study population was, in general, well-educated, wealthy, residing in urban regions, with good health status, and sufficient German language proficiency. We were unable to statistically weigh the answers based on these sociodemographic factors because not all participants completed all survey items due to filter and optional items. Furthermore, we classified our participants into three age groups and digital health literacy groups based on variable distributions rather than standardised cut-off scores. In doing so we could only assume that the younger participants had a higher digital exposure and participants with the lower eHEALS scores had lower digital health literacy. Fourth, our survey is based on a self-developed questionnaire that was not validated. This procedure was chosen because the survey aimed to assess the general attitudes towards digital health technology use. However, it cannot be ruled out that some self-reported behaviours in this study (e.g. digital technology use or digital health literacy) may have been under- or overestimated due to recall and social desirability biases. Fifth, the comparison between both surveys (the first 7 and the second survey) could only be done narratively due to item revisions and different populations that were recruited for both surveys. Due to insufficient funding we were unable to recruit and compare the responses of the same participants in both surveys or to determine if any participants were included in both surveys since they were recruited from the same consumer panel. In general, participation in both surveys was unlikely to bias the data due to item revisions and the two-year time-lag between both surveys. Sixth, the survey data were collected cross-sectionally during the COVID-19 pandemic. It is possible that some survey results were affected by any remaining restrictions related to the pandemic, such as provision of online fitness courses in addition to, or as a replacement of, in-person classes. While the data in both surveys were collected during various phases of the COVID-19 pandemic, the results might not be generalisable to pre- or post-pandemic periods. Finally, the survey topics were not investigated in depth (e.g. by using more items or more detailed items in the survey instrument) due to insufficient financial resources. For example, participants rated their app use in general or reported their use of any health websites without providing specific examples of apps or websites. In general, an online survey with a larger number of more detailed items could have been more appropriate to collect data on internet and digital technology use than a telephone survey. Qualitative responses could also have been included to gain more insight into the use of specific digital technology types (e.g. apps or wearables) and activities in the context of health promotion and disease prevention that could be supported by such technologies.
Future directions
In line with our findings, this study opens the door to several intriguing topics for future research. Qualitative research methods might provide deeper insights into experience with digital health technologies and the reasons for the low confidence in using online health information. Studies in different cultural contexts and languages are needed to uncover cross-cultural variations in digital health technology adoption. Longitudinal research could be used to study the dynamics of digital health technology adoption and to draw causal inferences by tracking changes in attitudes and usage patterns over time and assessing the changes in health outcomes in the long-term. The practical implications of our study extend to healthcare policy and practice. Given the varying attitudes and usage patterns across demographic groups, it is essential for healthcare systems to adapt and provide targeted digital health resources and support. 35 This may involve initiatives to improve digital health literacy among specific communities, 36 policies to boost the quality and trustworthiness of online health information, 37 and strategies to bridge the digital divide. 38
Conclusion
The internet and digital technologies were predominantly used to obtain health information, but less often for health promotion and disease prevention in 2022 in Germany. While health app and digital technology use for physical activity promotion increased, the confidence in using online information for health decisions decreased in 2022 relative to 2020. Factors that promote confidence in online health information and digital technology use for health promotion and disease prevention need to be investigated in future studies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241301457 - Supplemental material for Digitisation and health: Second nationwide survey of internet users in Germany
Supplemental material, sj-docx-1-dhj-10.1177_20552076241301457 for Digitisation and health: Second nationwide survey of internet users in Germany by Karina Karolina De Santis, Saskia Muellmann, Chen-Chia Pan, Stephanie Hoffmann, Jacob Spallek, Ulrike Haug and Hajo Zeeb in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank the project partners at Cerner Enviza GmbH for critical comments on the survey items. We thank our colleagues at BIPS (Dr Hermann Pohlabeln, Kirsty Cameron, and Sophia Brüssermann) and the University of Bremen (Prof. Dr. Benjamin Schüz) for assistance with the study. The publication of this article was funded by the collaboration fund of the Leibniz ScienceCampus Digital Public Health Bremen (LSC DiPH), Bremen, Germany and the Lausitz Center for Digital Public Health (LauZeDiPH), Brandenburg University of Technology Cottbus-Senftenberg, Senftenberg, Germany.
Contributorship
KKDS supervised and administered the project, acquired funding, conceptualised the study, developed the methodology, developed the survey items, processed and analysed the data, visualised the results, wrote the first draft of the manuscript, and reviewed and edited the manuscript.
SM administered the project, acquired funding, conceptualised the study, developed the methodology, developed the survey items, wrote the first draft of the manuscript, and reviewed and edited the manuscript.
C-CP developed the survey items, wrote the first draft of the manuscript, and reviewed and edited the manuscript.
SH developed the survey items, wrote the first draft of the manuscript, and reviewed and edited the manuscript.
JS developed the survey items, wrote the first draft of the manuscript, and reviewed and edited the manuscript.
UH acquired funding, conceptualised the study, and reviewed and edited the manuscript.
HZ acquired funding, conceptualised the study, developed the methodology, and reviewed and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Participant recruitment and data collection were performed by an external provider (market research institute, Cerner Enviza GmbH) according to their data privacy policy. 18 The study followed the ethical guidelines according to the Declaration of Helsinki, 19 although the verbal consent to participate in the study was not documented by Cerner Enviza GmbH. The ethical approval to analyse the anonymous data purchased from Cerner Enviza GmbH was not sought from our institutional ethics committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Leibniz ScienceCampus Digital Public Health Bremen (LSC DiPH), project number: DigitHEALTH2022, approved on 24 March 2022. LSC DiPH is jointly funded by the Leibniz Association (W4/2018), the Federal State of Bremen, Germany and the Leibniz Institute for Prevention Research and Epidemiology-BIPS, Bremen, Germany. The project report for the funder is available online in German. 39
Guarantor
KKDS
Supplemental material
Supplemental material for this article is available online (Appendix 1: STROBE checklist).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.