
Abstract
Objective
Digital health technologies offer great potential to improve access and adherence to cardiovascular disease secondary prevention measures such as regular physical activity (PA). However, the use and perceptions of digital technology (DT) among cardiac rehabilitation (CR) patients are not well understood. The aim of this study was therefore to explore the use of DT in former CR patients’ daily lives, for PA and for health information; and to gain insight into patient perceptions of DT for PA, including barriers, facilitators and requested features.
Methods
A cross-sectional postal survey was conducted between May 2022 and January 2023. Five Austrian CR centres contacted 500 former patients who had completed a phase 2 CR programme from January 2019 onwards. One-hundred seventeen patients (mean [SD] age, 69 ± 10 years, 22% female) responded. Descriptive and thematic analyses were conducted for closed and open-ended questions, respectively.
Results
Results indicated high DT usage for communication and informational aspects, and to a large extent also for PA and health information seeking. Main facilitators of DT use for PA were attributed to health and behavioural monitoring. Main barriers were lack of perceived need, lack of interest and poor usability. Most frequently requested features included pulse and blood pressure measurement, step count and compatibility to other devices.
Conclusions
Patients generally used and perceived DT as beneficial in daily life and for secondary prevention purposes such as PA. The survey identified facilitators, barriers and feature requests, which may inform the design and implementation of digital health interventions for CR patients.
Keywords
Introduction
Globally, cardiovascular diseases (CVDs) remain the leading cause of death. 1 Cardiac rehabilitation (CR), a secondary prevention model classified as a class 1 level A indication for treatment of CVDs, has been shown to reduce morbidity and mortality, and increase health-related quality of life.2–4 The major goal of CR is changes in lifestyle behaviours, e.g., increased physical activity (PA), to reduce the likelihood of disease progression, recurrent cardiac events and hospitalisations. 5 However, CR is often underutilised, and recommended behavioural changes, such as PA engagement, are often not sustained over time.6–10
Digital health technologies offer great potential to support patients with behavioural changes. For instance, digital health interventions – including web-based, telemonitoring and mobile health (mHealth) applications – can provide physiological and behavioural tracking capabilities, motivational feedback and access to educational materials; and have been shown to achieve desired changes in behavioural, health and patient satisfaction outcomes.11–14 Despite these benefits, the acceptability and use of digital health technologies among CVD patients remain suboptimal. For one, many digital health developments are often driven by technology and fail to adequately incorporate perceptions and needs of patients during the development process. 15 Moreover, previous studies investigating outcomes of digital health technologies often excluded individuals without access to internet or mobile devices (e.g., individuals not owning a smartphone), or recruited comparatively young study samples (mean ages 50–65 years). 14 Therefore, insights obtained from these studies may be biased towards more digitally skilled or younger individuals and not generalisable to all CVD patients, especially older adults who face the greatest burden of CVD 16 but typically use digital technology (DT) less.17,18
As such, if digital health interventions are intended to be used for CVD secondary prevention, the use and perception of DT in a typical, older aged sample is a necessary step to investigate. The aim of this study was therefore to explore the use of DT in former CR patients’ daily lives, for PA and for health information; and to gain insight into patients’ perceptions of DT for PA, including barriers, facilitators and requested features.
Methods
Procedure
We conducted a cross-sectional survey using a postal questionnaire. In the reporting of the study, we adhere to the STROBE guidelines. 19 Between May 2022 and January 2023, a total of 500 postal questionnaires were distributed from five CR centres (100 questionnaires per centre) located in four Austrian federal states (Carinthia, Vorarlberg, Upper and Lower Austria). Questionnaires were posted to the home addresses of patients who had completed a phase 2 in- or outpatient CR programme starting from January 2019 in chronological order. Participants returned completed questionnaires to the research institute by post using a prepaid envelope. Participation in the survey was voluntary. As an incentive, participants could choose to enter a random draw for four fitness trackers. For individuals who preferred to complete the survey online, the link and quick response code for an online version (LimeSurvey©) were provided.
Materials
We developed a customised pen-and-paper questionnaire for self-completion in German language, as no existing published questionnaire was available to address the study aim. Questionnaire content was informed by qualitative interviews with 25 former CR patients conducted in 2020 (unpublished data).
The questionnaire included seven sections (demographic information, general health information, CR history, internet use for health information, DT use in daily life, DT use for PA and data privacy) composed of altogether 46 items with multiple-choice, Likert scale or free-text response options. Most items were newly developed or adapted from the Austrian National Health 20 and information and communication technology (ICT) use surveys.21,22 The questionnaire also incorporated two short, standardised instruments (EQ-5D-5L 23 and Rapid Assessment of Physical Activity [RAPA]24,25).
The questionnaire underwent iterative development and rigorous pilot testing by members of the research team and seven cardiac patients. The questionnaire can be accessed via the Open Science Framework platform (https://osf.io/8ec2j).
Inclusion criteria
Participants were included if they were ≥18 years old, resided in Austria, and had completed in- or outpatient CR phase 2 starting from January 2019 at one of the participating CR centres. During that time, the use of digital tools such as mHealth applications had not been established at any of the participating CR centres, except for the use of wearable heart rate sensors to monitor exercise training intensity. Participants without proficient German language skills were excluded.
Data analysis
All returned questionnaires were anonymised and manually transferred to an online format (LimeSurvey©). From there, data were exported to Microsoft Excel files and analysed in R (version 4.2.1).
Statistical analysis was conducted primarily using descriptive analysis of central tendency (mean or median depending on distribution), measure of spread (standard deviation and interquartile range [IQR]) and frequencies and percentages (n, %). Two exploratory inferential analyses were conducted (McNemar test with Bonferroni correction for multiple comparison) to assess paired differences in DT use between daily life and PA and use of internet sources versus judgement of their trustworthiness.
To assess the free-text responses, a content analysis with inductive approach was conducted to describe the frequency of themes (e.g., barriers/facilitators).26,27 Specifically, the following steps were performed by the first author (HM): an initial reading of the responses to identify emerging themes; categorisation into overarching themes and subthemes; points of diversion regarding overarching themes and sub-themes discussed with the last author (STK); and frequency count of the confirmed themes and sub-themes.
Ethical considerations
The study received ethical approval from three regional research ethics committees, and one regional committee waived the need for formal ethical review. In conjunction with the postal questionnaire, patients received written information about the study. For this anonymous self-completed postal survey written consent was not required, but self-completion and return of the questionnaire were taken as implied consent and so approved by the research ethics committees.
Results
Demographics
One-hundred and seventeen former CR patients (mean age, 69 ± 10 years, 22% female, 74% retired) participated in our survey (response rate 23.4%). Fifty-six percent had participated in inpatient CR phase 2, 50% in outpatient CR phase 2 and 25% also participated in outpatient CR phase 3 prior to the study (with more than one type of former CR possible). Patients’ cardiovascular history consisted of mainly coronary heart disease (including angina pectoris, myocardial infarction, percutaneous coronary intervention and coronary bypass surgery) (73%), heart failure (16%) and heart valve surgery (10%). Table 1 presents participants’ socio-demographic and clinical characteristics.
Participants’ socio-demographic and clinical characteristics.

CR, cardiac rehabilitation; RAPA, Rapid Assessment of Physical Activity questionnaire.
* Multiple responses permissible.
Physical activity
The sample was predominantly physically active (66% as determined by the RAPA questionnaire) and healthy (median [IQR] perceived health score, 80 [60, 85] out of 100). The median [IQR] weekly frequency and duration of PA were 4 [3, 5] times per week and 4 [2, 8] hours per week.
Use of DT in daily life and for PA
We compared respondents’ use of DT in daily life (i.e., for all purposes) and specifically for PA. For exercise-specific DT such as pedometers and fitness trackers, this distinction would indicate whether the device is worn throughout the day (in daily life) or whether it is applied only for the purpose of tracking a planned PA or exercise session. Internet and DT usage were highly prevalent in respondents’ daily lives. Eighty-three percent used the internet for personal use, and 96% used DT for daily life. Depictions of internet and DT use are presented in Figure 1(a) and 1(b), respectively. Most frequent use of DT related to email (77%), calling (74%) and use of the internet (69%), but with overall few weekly hours of internet use.

Use of digital technology in daily life and for physical activity: (a) Response rate to question ‘If you think about your internet use (including Apps on your smartphone or tablet), how many hours do you use the internet for personal use in a typical week?’ (b) Most frequently (≥20% of participants) recorded uses of technology in response to ‘I use digital technology for…’ (less frequent responses were ‘Other Apps’ and ‘Status update posting’) (c) Comparing response rates of question ‘What digital technology do you use most frequently in daily life?’ to question ‘What digital technology do you use for physical activity and exercise?’ For (b and c), multiple responses were permissible *p < .001.
Seventy-seven percent of respondents used some type of DT for PA. Ownership of a smartphone or smartwatch in this sample was 77% and 27%, respectively. The smartphone was the most popular device for both PA (35%) and daily life (66%) (Figure 1(c)). The smartphone was used significantly more in daily life than for PA purposes (unlike step counters, fitness trackers and smartwatches) but was still the most popular device for PA, suggesting its preference over more exercise-specific DT. In fact, nearly half of all smartphone users (49%) also used the smartphone for PA. Twenty-five percent of patients used either a step counter or a fitness tracker in daily life, and 40% of patients reported using either or both types of devices frequently in daily life. In contrast, significantly more respondents did not use DT for PA (23%) as compared to not using DT in daily life (4%) (Figure 1(c)). Therefore, we see a near ubiquitous integration of DT in patients’ daily lives, but to a lesser extent in PA.
Use of the internet for health information
The majority of respondents (73%) had searched online for health information in the past three months. The most frequently searched topics are displayed in Figure 2(a). Searching for health information online was primarily motivated by personal health concerns or general interest (75–100%) and to a lesser extent on someone else's behalf (up to 25%). Besides the health topics listed for multiple choice, 33 additional topics were reported in optional free-text responses, including (long) COVID, polyneuropathy, blood pressure, dizziness and cholesterol.

Use of internet for health information, N = total sample size (multiple responses permissible): (a) Eight most frequently searched health topics in response to question ‘During the past 3 months, which of the following health information did you obtain from the internet and for what purpose?’ (b) Comparing response rates of question ‘In the past 3 months, what sources of information on the internet have you used to obtain health information, and how would you rate the information you found?’ to response ‘Yes, trustworthy information’.
Types of online sources and their respective trustworthiness ratings are depicted in Figure 2(b). YouTube, social networks, forums and blogs were rated least trustworthy, while the greatest discrepancy between frequency of use and trustworthiness rating was observed for Wikipedia and YouTube. Other sources of health information reported in optional free-text responses included health magazines and other print media, television, information from doctors, testimonials from other patients, Google and webinars.
Lastly, in terms of using online information to contact health professionals in the past three months, one third of respondents (32%) reported using the internet to search for a health professional, and 26% reported having contacted a health professional because of health information found online.
Perceptions of DT for PA purposes
Ninety-three respondents (79%) provided free-text answers expanding on their reasons for or against DT use for PA (Figure 3(a) and 3(b), respectively). Here, measurement of pulse or heart rate, monitoring of PA, monitoring of general health status and self-monitoring for motivational reasons were the top-reported facilitators for DT use. Trust in the accuracy of measurements (e.g., pulse, step count) was generally high, with a median [IQR] of 6 [5, 6] on a 7-point Likert scale (higher ratings indicating greater trust). The top barriers to DT use were considering oneself already physically fit, having no need for DT, disliking DT or finding DT too complicated.

Perceptions of digital technology for physical activity purposes (schematic diagram according to thematic analysis of free-text responses); multiple responses permissible per participant (N = total sample size, n = number of response occurrences): (a) Response to question ‘State your personal reasons for using digital technologies for physical activity’; (b) ‘Give your personal reasons why you do NOT use digital technologies for physical activity’; (c) ‘If you could wish for an ideal digital technology to help you engage in regular heart-healthy exercise and sports, what would it look like?’.
Thirty-one respondents (26%) provided free-text answers regarding their ideal imagined DT for PA (Figure 3(c)). The most popular requests were an easy to use/operate technology, sharing similarities to existing fitness apps, inclusion of blood pressure and pulse measuring capabilities and comfort when wearing a DT. These themes align with multiple-choice responses indicating a high demand for blood pressure and pulse measuring capabilities (Figure 4). Additionally, although compatibility/connectivity features were only requested by about half of participants (48%), among those that did, the smartphone was the most requested item for compatibility/connectivity purposes (81%).
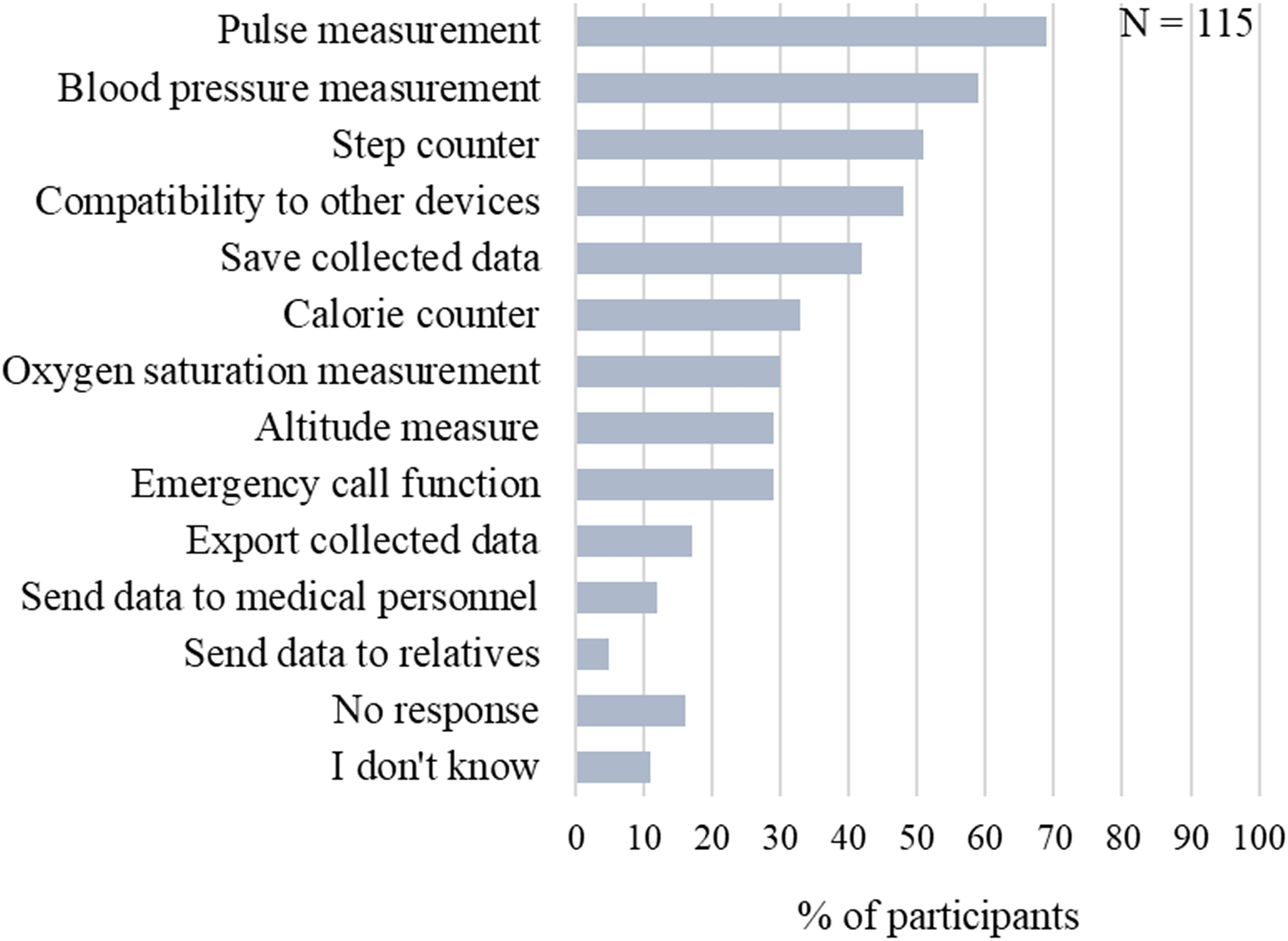
Responses to multiple-choice question ‘What features should a digital technology ideally have so that you would use it to support your physical activity?’.
Data privacy
Responses to data privacy questions are reported in Figure 5. Overall, participants indicated variable familiarity with current data protection regulations and terminology (Figures 5(a)–5(c)) but found current data protection regulations generally understandable (Figure 5(d)). Participants reported a tendency to skip over data protection statements before agreeing to them (Figure 5(e)) and indicated that information on data protection was worded in an incomprehensible way (Figure 5(f)).
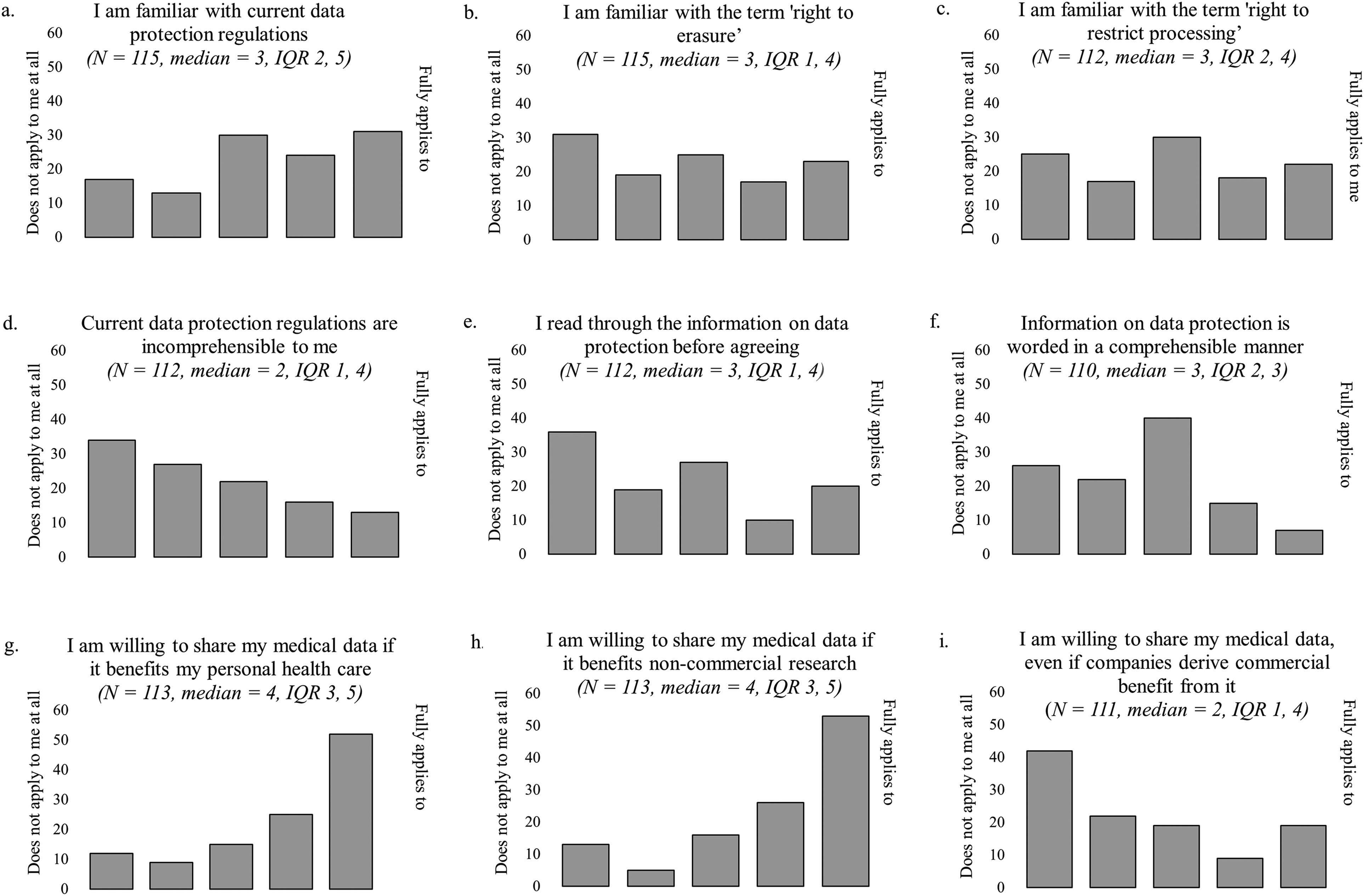
Response distribution of data privacy questions. Responses provided on a 5-point Likert scale from 1 (does not apply to me at all) to 5 (fully applies to me) in response to the question ‘Please indicate to what extent the following statements apply to you’. Frequency count (number of participants) is reported on the y-axis.
Respondents reported high willingness to share medical data for personal health benefits (Figure 5(g)) or non-commercial research (Figure 5(h)) but not for commercialised reasons (Figure 5(i)). However, in an optional open question, 37 respondents (32%) expanded on circumstances under which they would share medical data for commercialised use: if it benefits others (patients or the general public) (n = 12), if it confers a personal medical advantage (n = 7), if anonymity is ensured/personal information is excluded (n = 4) and if it is helpful for research (n = 3).
Discussion
This study found that DT use – specifically smartphone use – was highly prevalent in CR patients’ daily lives, and to a large extent also for PA purposes. DT use in daily life was primarily focused on communication and informational aspects (i.e., email, calling and internet use), whereas use of DT for PA was focused on measurement of pulse or heart rate, monitoring of PA, monitoring of general health status and self-monitoring for motivational purposes. The main barriers to DT use for PA were perceived lack of need, lack of interest and poor usability. The majority of patients searched online for health information and displayed a willingness to share medical data dependent on a motivation to contribute to health care, research and patient outcomes.
Representativeness of the sample
We compared our study findings to approximate age-matched population data (age groups 45–74 years old) from the 2019 Austrian National Health Survey 20 and the 2020 and 2021 Austrian National Information and Communication Technology (ICT) survey.21,22 While only 19.6% of 45–59-year-olds and 21.3% of 60–74-year-olds in the Austrian general population meet the World Health Organisation PA recommendations for both endurance and muscle strengthening exercise, the percentage in our survey sample was somewhat higher (27.6%). Nevertheless, this finding indicates a gross lack of long-term adherence to PA recommendations among CR patients, corroborating results from the EUROASPIRE V survey from 27 European countries which reported that only 34% of patients performed regular PA (≥30 min on average five times a week) around one year following an acute coronary event. 9
With regards to ICT use, the percentage of internet and smartphone users in our survey sample was similar to the Austrian population (approximately 85% and 70%, respectively), but there was a higher percentage of smartwatch users in our sample by approximately 10%, possibly due to a greater perceived need for CVD patients to self-monitor their health. We also compared DT use specifically among internet users (83% in our survey) against Austrian national ICT survey data. Instant messaging (text and video/image) was used by approximately 72% in both groups. More respondents in our survey engaged in calling (phone and/or video calling), email use and online banking (by 40%, 15% and 10%, respectively), while more respondents in the general population reported using social networks (by 10%). Because our sample included older age groups (≥75 years old) than the Austrian national population surveys, these differences may be related to age-related preference. For instance, prior literature reported calling to be a preferred form of communication over text messaging among older adults in contrast to younger segments of the population. 28 Therefore, our findings highlight certain discrepancies in preferred communication forms, which could be related to age but also to changes in patients’ preferences over time. In summary, we see that survey respondents were somewhat more physically active and used ICT and DT more than the Austrian general population.
Digital health literacy
Digital health literacy, or electronic health literacy, describes the ability to seek, find, understand and appraise health information from electronic resources and to apply this information to address a health problem. 29 Searching for health information online was common in our sample and approximately 30% more prevalent than in the Austrian general population, 21 despite our sample including older adults who are typically reported to use the internet less for health information than younger adults. 18 This is likely related to our sample consisting of individuals with significant chronic health conditions who have been reported to show greater health information seeking behaviour. 30 Thus, DT for health information purposes may be particularly valuable and useful for CR patients. Additionally, as our findings indicate that less than half of patients used trustworthy online sources such as general health information sites or official institutional websites, there is scope to increase access to vetted information materials and offer training in digital health literacy skills. 31
Development and implementation of digital health interventions
In terms of DT use in daily life, the smartphone was the most commonly used device and may be targeted opportunistically by intervention developers as the most prevalent conduit for digital health interventions. We saw a preferred use of more traditional communication forms (e.g., email and calling) as compared to newer communication forms (e.g., video calling and social media use). As our sample was comprised of mostly older adults, this could reflect age-related preferences or barriers to social technology use (e.g., communication preferences, low self-efficacy and fear and/or physical constraints of DT use) as reported in prior literature. 32 As such, technology preferences and barriers are necessary aspects to consider when developing digital health technologies for – typically older-aged – CVD patients.
The main reported reasons for DT use for PA in our findings suggest that DTs are largely perceived as beneficial for health and behavioural monitoring by end users. Specifically, comments such as ‘to verify my performance’ and ‘control for myself personally’ suggest a sense of perceived knowledge gain and self-efficacy as primary facilitators of DT use. Our findings, therefore, echo those of a previous review by Whitelaw et al. which found ‘perceived usefulness’ and ‘empowerment’ to be important facilitators for DT uptake among cardiac patients. 33 Additionally, we also report common themes between our findings and those of Whitelaw et al. relating to ease of use and personalisation, which emphasises how ensuring user-friendliness and incorporating options for personalisation may facilitate use of digital health interventions.
Our findings regarding patient requests for DT to support PA again highlight the importance of user-friendly design of monitoring features for mainly pulse/heart rate and blood pressure. This is in alignment with prior literature which shows that meeting the desired functionality and enhancing ease of use contribute to digital health intervention uptake in both older adults and CVD patient samples.33,34 DT for pulse/heart rate and blood pressure measurement are currently not integrated into smartphones but require the use of separate wearable sensor devices, often in conjunction with a smartphone app. This may explain why in our survey compatibility of digital devices was the fourth most frequent feature request.
The main reasons for not using DT for PA in our survey – lack of perceived need, lack of interest and difficulty of use – correspond with previously reported barriers by Whitelaw et al. 33 and present challenges for digital intervention developers. Increased communication and education on the benefits and features of digital health interventions can explain the need and create interest in DT, particularly in patient groups who struggle with managing behavioural changes and who feel indifferent or undecided about DT. However, it is also necessary to cater to those who deliberately reject the use of DT for PA, which includes involving these groups in intervention development processes to identify how the possibilities and benefits afforded by DT may still be utilised in such user scenarios.
Overall, our survey findings support the key message that user-centred co-design – involving patients in the development of digital health interventions – is of importance to ensure optimal feature fit and user-friendly design 35 and to maximise the likelihood of DT adoption and spread from the perspective of the individual technology user. 36 Such user-centred co-design may be implemented under different academic traditions. For example, in the field of human-computer interaction, user-centred co-design methods have long been part of DT developers’ toolbox37,38 and are now increasingly applied in more nuanced and differentiated ways to address the requirements of different segments of DT development such as mHealth. 39 These established co-design methods include specific techniques for the entire development cycle from needs analysis to prioritisation of requirements, ideation, rapid prototyping, user feedback and formative and summative evaluation. In health services research, co-production and co-creation have become familiar methodological terms describing approaches for shaping health services jointly and in collaboration with users (i.e., patients and their informal carers).40,41 This links with the patient and public involvement approach which aims to open up research and health service design to the intended user groups in order to take direction from those who should eventually benefit from the design 42 and is increasingly reflected also in the digital health domain. 43 In sum, these academic traditions offer a spectrum of perspectives on the practice of user-centred co-design, ranging from specific co-design techniques and methods to overarching methodologies that value the close collaboration between developers (including designers, researchers and healthcare providers) and users (including patients, informal carers and members of the public).
Data privacy
The collection and use of individuals’ health data presents a pressing issue in the digital transformation of healthcare systems. While the possibility of ubiquitous data collection via smartphones, apps and wearables promises untapped potential for patient management and research, this needs to be balanced against justified data privacy concerns. 44 With the General Data Protection Regulation, the European Union has created a strict regulatory framework that also applies to digital health. 45 Our findings demonstrate that respondents had varied knowledge and understanding of this, and only a minority tended to peruse data protection statements. Moreover, reading through data protection statements prior to agreeing was approximately 20% less prevalent in our sample than in the Austrian general population, 22 coupled with over half of respondents indicating that information on data protection was worded in an incomprehensible way.
A lack of understanding may lead to data privacy concerns and subsequent resistance to digital health technologies. 34 Transparency about data usage and storage is critical. This is particularly supported by our finding that respondents were generally willing to share medical data, provided that it is known who benefits from the data and that data are anonymised. Beyond individual patient care, these findings also have implications for the big data agenda in health as it is currently being advanced through the European Health Data Space initiative. 46 Concerted efforts to design highly accessible and user-friendly data protection statements for digital health technologies, e.g., incorporating pictorial and audio-visual designs, 45 will support patients’ digital health literacy and foster trust in data processing organisations.
Limitations
This study was limited due to the self-selected nature of our sample, leading to possible response bias with higher responses from more health-literate (e.g., physically active) or digitally skilled individuals. We attempted to counter this by using a postal paper-and-pencil questionnaire, recruiting patients from a geographically diverse area and including in- and outpatients CR centres (whereby the latter tend to serve somewhat younger and physically fitter patients). The response rate of 23.4% may be regarded as fair, considering that patients were approached three to four years after their episode of care at the respective centres. Of note, it was considered important to collect data from patients several years after their CR, to inform the use of DT for supporting long-term PA behaviour in the secondary prevention of CVD. A further limitation relates to the lack of psychometric validation of those questionnaire items which were developed anew for this study (as opposed to those questionnaire items which were incorporated from national surveys and standardised instruments). Lastly, the study was limited by the lack of a prospective sample size calculation. While aiming to recruit as large a sample as feasible, the sample size for this exploratory and descriptive survey was guided by considerations of cost and resources.
Conclusions
Digital health technologies have the potential to greatly improve CVD secondary prevention, but their usefulness depends on their perception and likelihood to be utilised by patients. Our results demonstrate that DTs – especially the smartphone – play an integral part in former CR patients’ daily lives and are frequently used to support PA. Thus, our findings not only suggest the potential use and benefit of DT for CVD secondary prevention but also highlight current barriers of DT use and suggestions for developers of digital health interventions.
Footnotes
Acknowledgements
The authors thank Helmut Peherstorfer, Arno Strohmeyer, Gertraud Waldenberger, Franz Waldenberger and Ingrid Unger for their assistance in piloting the questionnaire. The authors thank the collaborating cardiac rehabilitation centres for distributing the survey questionnaires. The authors are grateful to the patients who took the time to participate in the survey.
Contributorship
STK, RC and JN conceived the study and designed the protocol. JG, KM, VL, RC and STK developed the survey questionnaire. STK, JN, AB, MF, SG, VG, DK, KM, MM and AP were involved in gaining ethical approval, patient recruitment and data collection. VL and HM entered and cleaned the data. HM analysed the data. HM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was granted ethical approval from the following regional research ethics committees: Ethikkommission des Landes Kärnten (reference M2022-27), Ethikkommission der Medizinischen Fakultät der Johannes Kepler Universität (reference 1078/2022) and Ethikkommission für das Bundesland Niederösterreich (reference GS1-EK-4/795-2022). One regional research ethics committee (Ethikkommission des Landes Vorarlberg) waived the need for formal ethical review. In conjunction with the postal questionnaire, patients received written information about the study. For this anonymous self-completed postal survey, written consent was not required, but self-completion and return of the questionnaire were taken as implied consent and so approved by the research ethics committees.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Ludwig Boltzmann Institute for Digital Health and Prevention, Salzburg, Austria.
Guarantor
STK.