
Abstract
Objective
This study aimed to investigate the potential of LINE, a major messaging app and social media platform in Japan, as an effective tool to enhance the health and dietary behaviors of young Japanese women who face health and dietary challenges.
Methods
A 6-week randomized controlled trial employing an intention-to-treat analysis was conducted on first-year female students (age range, 18–23 years) from one university and two junior colleges in Mie Prefecture. The participants were allocated to either an intervention group (n = 54) or a control (n = 55) group. The intervention group received health information focusing on proper intake and intake methods to maintain an appropriate weight and dietary balance via LINE 18 times over 6 weeks (3 times per week), whereas the control group continued their usual lifestyle without any additional intervention.
Results
The results revealed a significant increase in the percentage of participants in the intervention group who rated their health as “unhealthy” (from 25.9% to 40.3%). This may be attributed to increased health awareness among the participants, which led to more critical self-assessments—a phenomenon often referred to as the “health awareness paradox.” Despite this increase in perceived unhealthiness, the intervention group showed a significant increase in the intakes of iron, vitamin C, dietary fiber, and potassium, indicating improved nutritional behavior.
Conclusion
The provision of health information through LINE over a 6-week period demonstrated potential as a tool for health education among young Japanese women. However, the observed increase in “unhealthy” self-rated health underscores the complexity of such interventions, suggesting that while nutritional behavior may improve, increased health awareness can paradoxically lead to more negative self-assessments. Further research is needed to explore the optimal duration and content of health information delivered via social media apps to maximize their effectiveness for health interventions.
Introduction
It has been reported that the prevalence of underweight among young women in Japan is relatively high compared with other countries. 1 The 2019 National Health and Nutrition Survey conducted by the Ministry of Health, Labour and Welfare of Japan found that 20.7% of women in their 20s in Japan have the “thin (low body weight)” body type (defined as a body mass index [BMI] < 18.5 kg/m2). 2 Low body weight has been associated with several health issues, including eating disorders, irregular menstruation, and a future risk of giving birth to low-birth-weight infants.3–5 Furthermore, studies have shown a significant negative relationship between BMI and self-rated health (SRH), which is the subjective perception of an individual's overall health, in young women who are lean or who try to lose weight despite having an average weight. 6 The 2019 National Health and Nutrition Survey also revealed that the highest proportion of both male and female respondents answered “interested but not intending to improve” concerning their intention to improve their dietary habits. Notably, among these respondents, women aged in their 20s showed the highest rate, at 30%, surpassing all other age groups. 2
Although there is some evidence from longitudinal studies suggesting that eating habits established in childhood are likely to continue into adulthood,7,8 which highlights the importance of early interventions, university and college students aged 18–24 years tend to undergo significant lifestyle changes 9 and experience a critical period during which their preexisting habits may be disrupted during the transition from adolescence to adulthood. 10 Food patterns established at this age are likely to be maintained in later life and may have a significant and long-lasting influence on their future health and that of their families.11–14 However, they are often ambivalent about their future health and the role that nutrition plays. 15 Therefore, university and college students transitioning from adolescence to young adulthood, especially female college students, need to be more fully educated about future health and the importance of adequate and healthy nutrition.
Social media comprises interactive platforms that allow anyone to transmit information and interact with others easily over the Internet. Typical examples include blogs, social networking services (SNSs), video-sharing sites, and messaging apps. 16 In 2023, it was estimated that over half of the world's population (51%) have used social media, with Facebook, YouTube, Instagram, and WhatsApp being the most popular. 17 Previous systematic reviews on interventions made through these social media sites have shown that they can positively influence physical activity and diet-related behaviors.18–21 Moreover, social media provides an effective channel for engaging young adults, a target population that has been difficult to engage in public health practice. A review by Chau et al. 22 found that social media was a promising avenue for nutrition interventions for adolescents and young adults.
The Japanese population also uses social media to gather information. Facebook, Twitter, and Instagram are used as tools for disseminating information that contributes to improving mental health and maternal and child health. However, it should be noted that LINE, a messaging app that is also considered part of social media, is used by about 90% of both regular and nonregular users of social media in Japan.23,24 The LINE app is a Japanese mobile messaging service operated and developed by the LINE Yahoo Japan Corporation, a member of the SoftBank Group. This application allows users (both individuals and groups) to talk and make voice and video calls. In particular, it has market share in Japan, Taiwan, Thailand, and Indonesia. According to the FY2019 Survey Report on Usage Time of Information and Communications Media and Information Behavior released in 2020 by the Information and Communication Policy Research Institute of the Ministry of Internal Affairs and Communications, the LINE usage rate was 86.9% for all age groups and 95.7% for those in their 20s, making LINE the most popular messaging app among young Japanese people. 25 Therefore, the use of LINE, which has a wider reach in Japan than Facebook, Twitter, or Instagram, to disseminate nutritional information among the young Japanese population should be considered. However, to our knowledge, only a few reports have investigated the association between eating behaviors and the use of the LINE.
In this pilot study, we conducted a 6-week intervention study among Japanese female university students to determine whether LINE can be an effective tool to influence the health and dietary habits of young Japanese women.
Hypotheses
We hypothesized that (1) disseminating information via LINE would change the eating behaviors of young women, and that (2) the intervention would have an effect even if the period was short. Confirming these hypotheses would suggest that LINE could be an effective tool for disseminating nutrition education to young women who have little interest in their diet.
Methods
Study design
The participants in this randomized controlled intervention study were categorized into two groups: (1) an intervention group, and (2) a control group. Assessments were conducted at baseline and 6 weeks. The data were analyzed on an intention-to-treat basis.
Participants
During the 2019 school year, 395 first-year female students (age range, 18–23 years) from one university and two junior colleges in Mie Prefecture were recruited through mass advertising (i.e. posters on campuses). Among these 395 students, 132 applied to participate in the study. Students majoring in nutrition or who had an unbalanced diet were excluded. In this study, an “unbalanced diet” was defined as a dietary pattern that significantly deviated from recommended nutritional guidelines. This includes diets that may be deficient in essential nutrients, excessively restrictive, or overly reliant on certain food groups. For instance, individuals following vegetarian or vegan diets were categorized as having an unbalanced diet if they did not adequately compensate for potential deficiencies in nutrients such as protein, iron, and vitamin B12. Similarly, diets high in processed foods and low in fruits, vegetables, and whole grains were also considered unbalanced. To ensure accurate classification and address any potential nutritional gaps, a registered dietitian reviewed the diet assessments provided by the participants. After excluding students who did not show up for the interviews (n = 14), 109 students were finally enrolled in the study. The respondents were interviewed separately and briefed on the study's purpose and intervention duration. Written informed consent was obtained from all participants. The study design and informed consent procedure were approved by the Institutional Review Board of Tsu City College (approval no.: 20) on 20 June 2019. This trial was registered as no. UMIN000048071 under the UMIN Clinical Trials Registry (UMIN-CTR). This study was conducted in accordance with the principles of the Declaration of Helsinki.
The sample size was calculated using an effect size of 0.5, an alpha of 0.05, and a power of 0.95. 26 We estimated that enrolling 109 participants would provide the study with over 90% power to detect a difference of at least 30 percentage points in the primary end point (total score on the SRH scale) at a two-sided alpha level of 0.05 between the intervention and control groups, assuming that 25% of the participants in the control group would respond and 20% of the participants would withdraw. The power calculation was based on the overall score of the SRH scale, with a 30% change in the total score considered as representing a meaningful difference in self-perceived health status. This approach ensured that the study had adequate statistical power to detect this level of change with the predetermined level of significance.
The baseline survey was conducted in September 2019. The participants were randomized to the intervention or control group in a 1:1 ratio using a random number function in Excel.
In this study, the blinding process for the participants was conducted as follows. The participants in the control group were informed that no specific dietary advice or intervention would be provided. This information helped maintain transparency regarding their group status, but also posed a risk of unintentional awareness of their lack of intervention. The participants in the intervention group were instructed not to share any details of the dietary advice or intervention with the students in the control group. This instruction aimed to prevent information from being leaked between groups and mitigate the risk of the control group learning about the intervention, which could influence their behavior or perceptions. Despite these measures, it is acknowledged that complete blinding of participants in dietary studies is difficult. As such, the potential for participants to be aware of their group allocation cannot be denied. Efforts were made to minimize this awareness, but the study design inherently limits the degree to which participants can be fully blinded. Therefore, the intervention group to not share the information with others, but no further measures were taken to prevent information sharing among participants. On the other hand, the data collectors were not blinded. The follow-up assessments were completed in October 2019, 6 weeks after the start of the randomized controlled trial. The participants were assessed using the same questionnaire as that at baseline (Figure 1).

Flow diagram of study participants.
Intervention delivery
The intervention was delivered over 6 weeks through a digital platform using LINE. The intervention group received regular health information, guidance, and feedback tailored to their dietary habits and nutritional needs. This included a series of educational messages that covered topics such as appropriate weight management, dietary balance, and specific nutrients (calcium, iron, vitamin C, dietary fiber, salt, and lipids). Each topic was presented in a sequence of two messages: the first provided essential information, while the second reinforced the content through quizzes and practical advice. These materials were developed and provided by registered dietitians affiliated with the Mie Prefectural Government and university organizations.
Educational messages
The educational messages were structured to provide clear, actionable information. For instance, participants received messages explaining the calculation of BMI, the importance of a balanced diet, and practical tips on how to meet the recommended intake of essential nutrients. 27
Each message was designed to be easily understandable and engaging, incorporating visual aids such as the Japanese Food Guide Spinning Top 28 to illustrate balanced eating patterns (Figure 2).

Example of content of the LENE on health and diet intervention program (1 page).
Feedback and engagement
The intervention groups received individualized feedback at baseline and follow-up based on their responses to the Brief Self-Administered Diet History Questionnaire (BDHQ). 29 This feedback included personalized advice on how to improve their dietary habits to align closely with nutritional guidelines. 30
To maintain engagement and ensure comprehension, the intervention included quizzes at the end of each topic. The participants were required to verify their understanding by taking these quizzes, with answers provided in subsequent messages. This interactive component helped reinforce the educational content.
Monitoring and support
The intervention also involved periodic check-ins through LINE to monitor the participants’ progress and address any questions or concerns they might have. This approach ensured ongoing support and encouraged adherence to the recommended dietary changes.
The participants were instructed not to share any details of the intervention with the control group to prevent contamination of the study. Despite these measures, it is acknowledged that complete blinding in dietary studies is challenging, and the possibility of participants becoming aware of their group allocation cannot be entirely ruled out.
Data classification
The participants completed a questionnaire that assessed their habitual dietary intake and lifestyle at baseline. A high score on the SRH scale is strongly associated with general well-being and psychosomatic symptoms,31,32 and SRH assessments among adolescents are an effective way to evaluate their own health self-perception.33,34 Therefore, the participants’ SRH scale scores were also assessed using the Global SRH scale,35–37 which comprises the item, “How would you rate your overall health?,” with five response choices ranging from excellent to poor (i.e. excellent, very good, good, fair, and poor). These five categories are dichotomized into either good health (excellent, very good, or good) or impaired health (fair or poor). Health Promotion Act which was enacted in 2015, requires the labeling of nutritional ingredients to promote health. The 2015 National Health and Nutrition Survey assessed whether nutrition labels were checked, and found that both men and women in their 20s were less likely than other generations to refer to nutrition labels. Therefore, we used the same questions as those in the 2015 National Health and Nutrition Survey to assess changes in health awareness. 38 The respondents who answered that they “always refer to” or “sometimes refer to” the nutrition labels were classified as “Yes,” whereas those who said that they “do not refer to” or “do not always refer to” the nutrition labels were classified as “No.” In the lifestyle assessment, the participants were asked whether they were consuming enough or too much of the nutrients listed in the individual result form of the BDHQ. The individual result forms were concerned with subjective eating behavior, inadequate intake (calcium, iron, vitamin C, dietary fiber, and potassium), and excessive intake (salt, fat, and saturated fatty acids). 30
Data analyses
The participants’ demographic characteristics, SRH, responses regarding nutrition labels, and subjective and nutrient intakes were presented as the means (standard deviation) or median (confidence interval) for continuous variables and frequency (percentage) for categorical variables, and then compared by group using the chi-square and Mann–Whitney U tests. Moreover, to confirm the effectiveness of the intervention, data regarding SRH, nutrition labels, and subjective intake for each nutrient (categorical variables) were compared between groups using McNemar's test. Changes in nutrient intakes from baseline to after the intervention (continuous variables) were compared between groups using the Wilcoxon signed-rank test. An analysis of outcomes was conducted on an intention-to-treat basis (all participants who were randomized to groups). The sensitivity analysis of the participants, excluding those who dropped out during follow-up, yielded similar results.
All statistical analyses were conducted using JMP 14.2.0 (SAS Institute Inc., Cary, NC, USA).
Results
Of the 109 participants who were registered, 109 successfully completed the study.
Characteristics of the subjects analyzed before the intervention
None of the items showed significant differences between the intervention and control groups at baseline (Table 1), including BMI. Although a p-value of 0.05 was observed for baseline BMI, it was not considered statistically significant. Additionally, the p-value of 0.12 for the BMI categories indicates no significant differences between the groups.
General characteristics of the participants.

BMI, Body mass index; n, Number; Values are represented as average and standard deviation, or n (%).
The mean age of all participants was 18.4 years (SD of 0.6), with a mean age of 18.3 years (SD of 0.5) for the intervention group and 18.4 years (SD of 0.7) for the control group. Note that there was no change in weight or BMI between baseline and 6 weeks later (Figure 3).
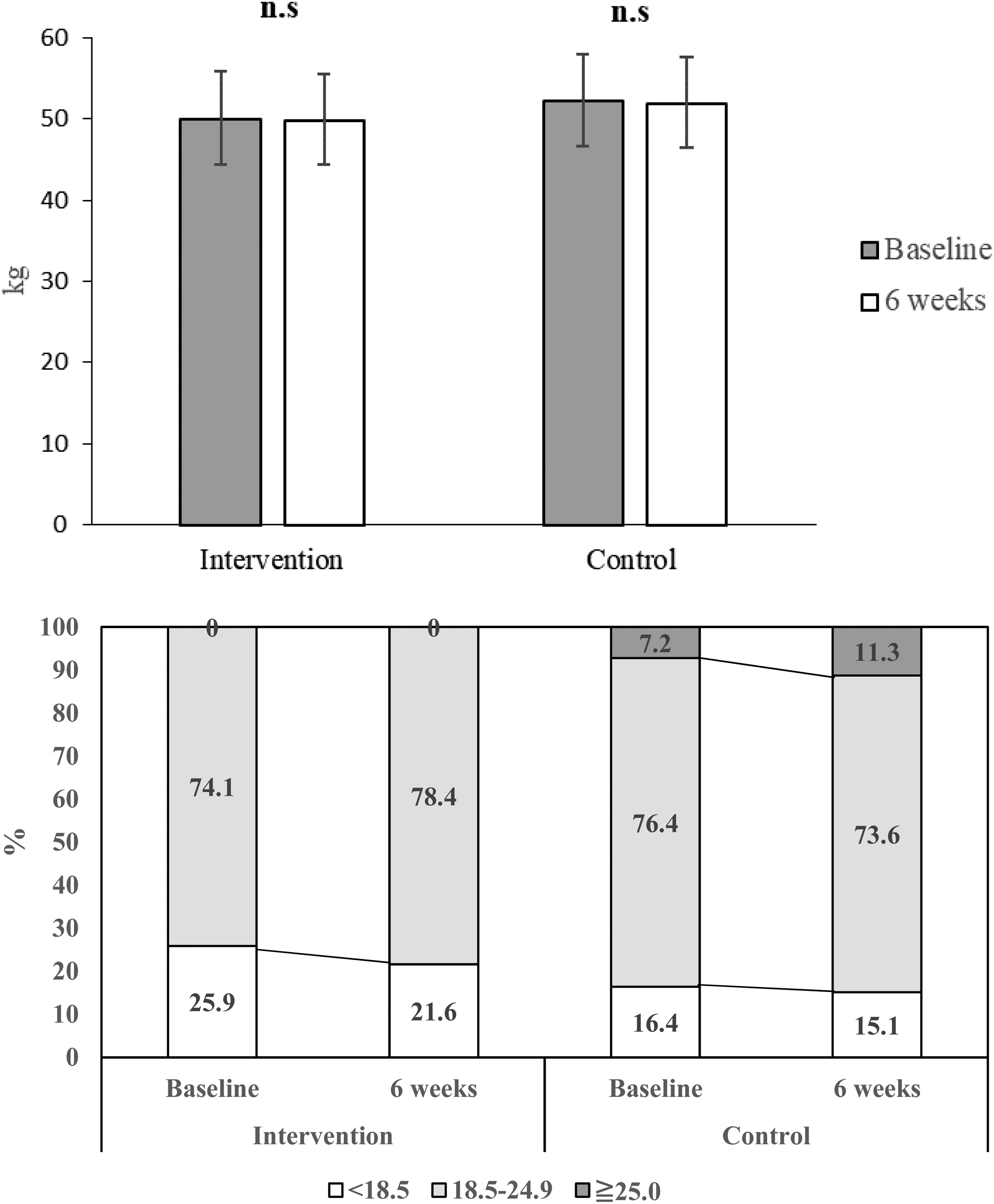
Weight and body mass index (BMI) at baseline and after 6 weeks.
Changes before and after the intervention and examination of the effects of the intervention on SRH and dietary awareness
No differences in any of the variables were observed in the comparisons between the intervention and control groups at baseline and after 6 weeks.
Figure 4 shows the changes in SRH and dietary awareness after the 6-week intervention. Within-group comparisons of the intervention group showed a significant increase in the number of “impaired health” responses on the SRH scale, indicating that the participants perceived their health as not healthy. A significant increase in the number of “no” responses to the question “Do you get enough of the following nutrients?” for dietary fiber was also seen, highlighting concerns about insufficient intake (Figure 5). On the other hand, no within-group differences were observed between the two groups regarding the excess intake of nutrients of concern.

Self-rated health (SRH) and nutrition labeling at baseline and after 6 weeks.

Subjective intake for each nutrition at baseline and after 6 weeks.
SRH. P values for changes within groups between baseline and 6 weeks were analyzed using the McNemar test. * p < 0.05.
The proportion of individuals who answered “Yes” or “No” to the question, A: “Are you consuming enough of the following nutrients?” or B: “Do you consume too much of the following nutrients?” P values for changes within groups between baseline and 6 weeks were analyzed using the McNemar test. * p < 0.05.
Intake of nutrients
Although a difference in dietary fiber intake was observed between the intervention and control groups at baseline, no differences were found in dietary fiber intake after 6 weeks. No differences between groups at baseline and after 6 weeks were found for the intake of other nutrients.
Table 2 shows the changes in nutrient intake after the 6-week intervention based on responses to the BDHQ. With regard to nutrient intake, the intragroup comparison of the intervention group revealed increased consumption of iron, vitamin C, total dietary fiber, potassium, and the salt equivalent. Moreover, a decrease in saturated fatty acid consumption was observed in both groups.
Baseline and changes in nutrient intakes after the intervention.

95% CI: 95% confidence interval; n: number. The Wilcoxon signed-rank test analyzed p values for changes within groups between baseline and 6 weeks.
Nutrients that differed between groups.
Discussion
LINE has a uniquely high penetration rate in Japan and other parts of Asia, making it deeply integrated into the daily lives of users, unlike other platforms. This high penetration rate is a crucial factor in LINE's ability to reach the target audience effectively. 25 Moreover, the user-friendly interface and multifunctionality of LINE play a significant role in encouraging user participation. For example, a study has shown that health interventions delivered via LINE significantly enhance user engagement, particularly among younger demographics. 39 This contrasts with text messaging or Instagram, which often lack similar levels of functionality or user engagement, highlighting why LINE may be particularly effective. Although LINE is not a telemedicine system, it functions as a culturally resonant platform that is deeply rooted in the social context of the target population and has the potential to increase engagement and effectiveness in health communication.
The present study assessed the effectiveness of a 6-week intervention (information provision) using communication through LINE to improve the health awareness and eating habits of female university students. To our knowledge, this is the first pilot intervention study conducted to assess the usefulness of LINE in improving health and dietary awareness among young Japanese women. The results revealed that while SRH and subjective dietary fiber intake worsened in the intervention group, the intake of iron, vitamin C, total dietary fiber, and potassium increased.
The results also revealed that SRH significantly worsened after the intervention. Margareta et al. 40 found that healthy habits and a high motivation for a healthy lifestyle were associated with poorer health among female students. SRH is known to correlate with cortisol responses to stress. 41 For female college students, a high interest in health-related activities may indicate an additional stressor in already stressful situations, which could negatively impact their SRH. Moreover, one possible explanation for these findings is that the intervention led to heightened health awareness, making participants more critical of their own health. This effect, where increased exposure to health information can lead to more stringent self-assessments, which is known as the “health awareness paradox,” has been documented in the literature. 42 Therefore, the results of this study suggest that the information about healthy eating habits provided to the participants may have caused them to lose confidence in their own health. However, in Japan, higher SRH among the younger generation is strongly associated with more frequent breakfast consumption and a preference for home-cooked meals. 43 Furthermore, higher SRH among adolescents is associated with healthier eating habits, 44 which must be improved to enhance SRH. One factor shown to be associated with more positive evaluations of SRH 45 is self-compassion—a kind, nonjudgmental, open-minded, and caring attitude toward oneself in the face of failure or difficulty. 46 Given that SRH decreased in this study, LINE content that promotes self-compassion and other aspects of health information needs to be developed and distributed in the future.
The results from the BDHQ indicated a significant increase in fiber intake after 6 weeks; however, the subjective perception of fiber intake decreased during the same period. This suggests that the participants’ perception that they “were not eating enough fiber” may have been a misinterpretation of their actual intake. Lyly et al. 47 reported that most Finnish consumers could link the effects of fiber intake on the body to its preventive function and understand the importance of fiber for health. Additionally, a comprehensive review of nutrition education interventions targeting medical students found declines in knowledge and self-efficacy following follow-up evaluations/measures after the intervention. This finding is of concern because the majority of interventions included in this scoping review were delivered as one–off events, primarily during the preclinical phase (some in the first and second years of medical school), with no opportunity for reinforcement. 48 Therefore, during the 6-week intervention, the fact that participants learned the actual target amount of dietary fiber through LINE might have led to a more appropriate conclusion that insufficient fiber intake has negative health impacts. However, because this conclusion was not further reinforced, it is possible that it worsened the participants’ subjective assessments of their fiber intake. This is an important consideration, as self-reported dietary behaviors often do not align with measured intake. According to dietary guidelines, the recommended daily intake of dietary fiber for adults is typically 20–25 g. 27 While the results of the BDHQ suggest that the intervention group achieved a significant increase in fiber intake, whether this increase precisely met the target range remains unclear because of the limitations of the BDHQ in providing exact values. In the future, objective methods such as biomarkers could offer a more accurate assessment, reinforcing whether the intervention effectively brings participants closer to or within the desired range of fiber intake. 49
During the intervention, among the nutrients included in the feedback to the participants completing the BDHQ were increased intakes of iron, vitamin C, total dietary fiber, and potassium, which are nutrients for which deficiency is a concern. This study used images and text to provide information about the worsening health consequences of an excess or deficiency of the targeted nutrients, which is consistent with the findings of previous studies revealing that presenting images of negative health outcomes encourages healthier choices. 50 However, the participants’ calcium levels were not affected, and thus, the content of the information provided for each nutrient needs to be examined in the future. An increase in the salt equivalent, which is a concern for overconsumption, was also observed. Excessive salt intake is a serious nutritional problem in Japan. Therefore, in the future, when using LINE to provide information that contributes to the health of female university students, it would be practical to provide not only information regarding food products, but also seasonings designed to reduce salt intake.
The results of this study suggest that using LINE can influence the health and dietary habits of young women; however, they also highlight the complexity of such interventions. While the intake of certain nutrients improved, the decline in SRH suggests the need for careful consideration of how health information is presented.
Limitations
This study has several limitations. First, the content of the information provided to the intervention group was related to the appropriate weight and dietary balance, and multiple nutrients were included in the feedback to the BDHQ. Thus, we were unable to analyze exactly which factor affected the participants, or to what extent. Second, the subjective nutrient intake questionnaire was developed based on feedback from the BDHQ and has not yet been validated; therefore, caution should be exercised when using it. Third, we did not collect detailed information regarding how the young women in the study obtained and prepared their food. Understanding their food sources and preparation methods is crucial to gauge the level of control they have over their diets. For instance, it would be helpful to know whether they primarily eat in dining halls, cook in dormitories, rely on convenience foods, or live with their family. Because this study did not assess these aspects, it is difficult to understand fully the constraints and choices influencing their dietary habits. Future research should consider including an assessment of food sourcing and preparation methods to provide a more comprehensive understanding of the participants’ dietary environments. Referring to previous literature or publicly available information from the schools could also offer valuable context in this regard. Fourth, in this study, it was technically difficult to know how much information confirmed or answered questions for the students in the intervention group, and because the information was provided unilaterally, it was not possible to assess the correlation with the amount of information obtained. Therefore, a program that can track how frequently participants engage with LINE content needs to be developed. Fifth, although we asked the intervention group not to share study information with the control group until the end of the study, we cannot deny the possibility that information bias may have occurred as a result of sharing information. Sixth, the intervention period may have been too short to improve the students’ ingrained food habits. Therefore, future studies on the effects of long-term interventions are needed. Seventh, this study focused solely on first-year female students from a specific region, which may limit the generalizability of the findings to other populations or age groups. Future research should consider including a more extensive and diverse sample, including all genders, and a better index for promoting the health of the participants. Finally, since the verification was performed using only LINE, the effectiveness of the program in raising awareness about the health and dietary habits of young women needs to be investigated further by comparing and combining the program with other SNS, such as Facebook, YouTube, Instagram, and WhatsApp.
Conclusion
The findings of the present study indicate that LINE can influence young women's health and dietary habits, although the complexity of such interventions cannot be denied. While the intake of certain nutrients improved, the decline in SRH suggests the need for careful consideration of how health information is presented. Future research should focus on optimizing content and delivery methods to enhance the effectiveness of mobile health interventions, ultimately promoting healthier lifestyles among young Japanese women and potentially broader populations.
Supplemental Material
sj-zip-1-dhj-10.1177_20552076241300740 - Supplemental material for Evaluating the effectiveness of LINE-based health interventions on dietary habits and health perceptions among young women: A pilot randomized controlled trial
Supplemental material, sj-zip-1-dhj-10.1177_20552076241300740 for Evaluating the effectiveness of LINE-based health interventions on dietary habits and health perceptions among young women: A pilot randomized controlled trial by Makoto Ohtsuki, Ai Komada, Hiromi Okada, Kanako Furuta, Yuki Aikawa and Yoriko Umehara in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank all participants of this study.
Authors’ contributions
MO, AK, HO, KF, YA, and YU designed the study. MO, AK, KF, and YU conducted the experimental work. MO, HO, and YA analyzed the data, prepared the figures, and drafted the manuscript. All authors participated in data interpretation and revised the manuscript. The final version of the manuscript was approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study design and informed consent procedure were approved by the Institutional Review Board of Tsu City College (approval number 20) on 20 June 2019. The trial is registered at the UMIN-RCT, UMIN000048071. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Institute for Food and Health Science, Yazuya Co., Ltd.
Guarantor
MO
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.