
Abstract
Objective
Engagement with self-monitoring is crucial for success in digital behavior change interventions for weight loss, but little is known about trajectories of engagement, nor valid predictors of these trajectories. This exploratory trajectory analysis identified engagement patterns based on multiple trajectories of engagement with self-monitoring of weight, diet, and activity in a website-based weight loss intervention over 12 months among adults with overweight/obesity (N = 363).
Methods
Latent class growth modeling with a mixture layer used self-monitoring data including number of days tracking weight, diet, and activity on the study website, summed across four 3-month intervals, to identify groups based on engagement trajectories. Regression models examined the association between engagement patterns, demographic variables, and percent weight loss at 12 months.
Results
Four engagement patterns emerged: never-engagers (23%), low/declining engagers (48%), early-engagers (13%), and sustained-engagers (16%). Trajectories of engagement were similar across self-monitoring behaviors within the same class. Age, race, and baseline body mass index were associated with likelihood of engagement class membership. Percent weight loss was clinically significant at 12 months for both sustained-engagers (−10.4%) and early-engagers (−5.1%), but not for low/declining (−1.3%) or never-engagers (−0.5%).
Conclusion
Promoting early self-monitoring engagement may be of equal or greater importance than promoting sustained engagement to achieve desired weight loss outcomes in a digital behavior change intervention for weight loss. Given the high proportion of low/declining engagers who did not achieve clinically significant weight losses, there is a need to characterize and identify these participants early on to promote engagement with self-monitoring.
Keywords
Introduction
Over 70% of US adults live with overweight or obesity, 1 which increases their lifetime risk for chronic illnesses such as heart disease, stroke, diabetes, and cancer.2,3 Behavioral weight loss interventions reliably produce clinically significant average weight losses of 5–10% of starting body weight over 6 months.4,5 Although such programs are effective, they are not implemented widely because of the high demands of both time and cost. 6 Digitally delivered programs are promising because they provide more flexibility than the standard approach, have improved scalability to reach more individuals, and are more cost-effective.4,6 Studies have demonstrated that digital behavior change interventions (DBCIs) for weight loss are comparable to traditional face-to-face approaches and can produce clinically significant weight losses of ≥5% of starting body weight.7–11 A meta-analysis by Beleigoli and colleagues found that compared to offline interventions, DBCIs for weight loss led to greater short-term weight loss among overweight and obese adults 12 ; however, high disengagement (i.e., nonusage attrition) rates across studies suggest that engagement is a major issue in digital interventions.13–15
Engagement, or the extent of meaningful usage and interaction with the interface of a DBCI, 15 is critical to intervention efficacy 16 and studies have established relationships between engagement in DBCIs and improved health outcomes across a wide range of behaviors and disease types.17–23 Engagement with self-monitoring of weight-related behaviors, such as diet, physical activity, and weight, is fundamental to behavioral weight control programs, whether digital or in-person.24–27 In DBCIs for weight loss, participants with higher frequency of self-monitoring lose more weight.7,8,28,29 Burke and colleagues conducted a systematic review on self-monitoring of diet, exercise, and weight in behavioral weight loss studies. They consistently found that self-monitoring was significantly associated with weight loss. 24 One possible explanation comes from self-regulation theory, which suggests that self-regulation efforts are more successful when individuals self-monitor and evaluate current behavior compared to goals, which either reinforces the behavior or allows for self-correction.30,31 However, engagement with self-monitoring in DBCIs for weight loss consistently declines over time.8,23,29,32
Previous research has detected qualitatively distinct patterns of engagement in DBCIs for weight loss and other behaviors based on basic website usage data such as logins, page views, and average time spent on a page.19,20,23 Power and colleagues identified four different engagement patterns based on overall number of website logins in a 12-month Internet weight loss (IWL) intervention for postpartum women, including nonusers (0–11 logins), low-engaged (12–47 logins), high-engaged (48–96 logins), and super-users (97 + logins). 23 In an Internet-based diabetes self-management intervention, Glasgow and colleagues found large variability in website use over 4 months based on summary usage variables (i.e., total visits, time spent online, percent of days of self-monitoring, number of page visits). In an online depression treatment trial, 20 Donkin and colleagues identified low, medium, and high engagement patterns by trichotomizing usage metrics (i.e., count of log-ins, modules completed, time spent online, and activities completed). 19 The variable-centered approaches used in these studies, while useful for describing relationships among variables, are not focused on the relationships among individuals or individual response patterns. Grouping individuals by individual response patterns, such that individuals within a group are more similar than individuals between groups, could be a useful approach for understanding how individual use of an intervention is associated with outcomes.
The purpose of this secondary analysis was to use a data-driven approach to identify patterns of engagement with self-monitoring of weight, diet, and activity in a website-based DBCI. This study's guiding aim was to quantify patterns of trajectories of multiple measures of engagement that emerge across participants in an effective DBCI for weight loss and identify demographic characteristics and intervention outcomes associated with these trajectory patterns. Examining multivariate trajectories of usage over time could elucidate which usage patterns are most beneficial and help researchers make recommendations for future program use. Additionally, understanding potential time-invariant variables that could be used to predict a trajectory pattern could help researchers tailor DBCIs for weight loss, thereby improving the efficacy of such interventions.
Materials and methods
This is a secondary data analysis using data from a parent intervention study. The parent study design and website-based intervention, as well as methodology of this secondary data analysis, are described below.
Parent study design
The parent study was a cluster randomized controlled trial evaluating the effect of integrating two IWL programs into primary care settings compared to usual care with evaluation over 12 months. 32 This clinical trial was registered (NCT01606813) and approved by institutional review boards at both study sites and was conducted between 2012 and 2016 at Penn State College of Medicine (Hershey, PA) and the University of North Carolina at Chapel Hill (Chapel Hill, NC). Briefly, the trial recruited 27 primary care providers (PCPs) and 550 patients ages 21–70 with a body mass index (BMI) between 25 and 50 kg/m2. Other eligibility criteria for patients included Internet access at home or work, plans to see their PCP within the year, and not lost 5% of their body weight in the past year. 32 Each PCP was randomly assigned to refer their patients to 1 of 3 treatment groups: (1) IWL intervention only, which was assigned to use the study's eHealth website; (2) the intervention plus physician feedback (IWL + PCP), which was assigned to the same eHealth website and also received tailored email messages from their PCP; or (3) Enhanced Usual Care (EUC) comparison condition, which received a 15-page booklet from the National Heart, Lung, and Blood Institute. Both intervention groups were more effective than EUC such that 12-month weight losses were −0.9 kg for EUC, −3.7 kg for IWL, and −3.6 kg for IWL + PCP. The IWL and IWL + PCP feedback lost significantly more weight than EUC but were not significantly different from each other on any study variables. 32 The primary paper includes a description of the intervention. 32
Website-based intervention
The intervention included a comprehensive behavioral weight loss website with individualized goals for diet and physical activity that promoted 1–2 pounds weight loss per week. 32 Daily calorie goals were based on participant baseline weight and ranged from 1200 to 1800 kcals/day. Physical activity goals were updated weekly. Upon the first login each day, participants were prompted to enter their weight from that morning or to indicate that they had not weighed themselves, which encouraged frequent weighing and allowed participants to closely track their weight. Participants were recommended to weigh themselves at least weekly. Other website components included a self-monitoring diary to track dietary intake and physical activity, computer-tailored feedback, instructional lessons, a summary plan page and problem-solving tool, a goal-setting tool, message board, progress page, and resource page. Additionally, automated emails tailored to participants’ progress were sent out monthly and a live webinar was offered biannually across groups. The participants in IWL + PCP also received a biweekly, semiautomated, tailored email from their PCP regarding their adherence and weight loss; the email text was predefined, but the PCP could choose to edit it prior to sending it to individual participants. Participants received an automated email prompt each week alerting them to new content and reminding them to check-in to the website to report their weight, calorie intake and physical activity. To maximize flexibility during the intervention, participants could choose from several Eating Plan monitoring options to customize how they monitored calories and change their monitoring plan if desired.
Participation rates were not different between the IWL and IWL + PCP interventions on measures of average use (median) nor the proportion of users logging in at least once per month over time. 32 Therefore, data for the current study included participants who were randomized to either intervention group (N = 363).
Ethical statement
The parent study was approved by institutional review boards at both study sites. All participants provided written informed consent prior to enrollment and randomization into the parent study. This secondary data analysis was exempt from IRB approval.
Measures
Self-monitoring engagement. Number of days tracking weight, diet, and physical activity were calculated across 4 timepoints: 0–3 months (Time 1), 4–6 months (Time 2), 7–9 months (Time 3), and 10–12 months (Time 4). Three-month increments were used to allow for at least 4 timepoints to examine heterogeneity in growth trajectories of self-monitoring behaviors. Weight, diet, and physical activity entries on the intervention website were time-stamped. Total tracking days for weight, diet, and physical activity were calculated by summing the number of days any tracking data were entered for each participant across the 4 timepoints. If a participant had no objective tracking data, number of tracking days was equated to 0 for that timepoint.
Demographics. Participants completed a baseline demographic questionnaire assessing sex, age, race, and type II diabetes status.
Percent weight loss. Body weight was measured by research staff at the physician's office at baseline, 3 months, 6 months, and 12 months using a calibrated standard digital scale (Tanita Health Equipment, Arlington Heights, Illinois, USA). Percent weight loss was calculated at 3, 6, and 12 months. Height was also measured in the office and used to calculate BMI.
Statistical analyses
The current study used latent class growth modeling (LCGM) with another mixture layer to identify groups of participants based on trajectories of engagement with self-monitoring of weight, diet, and physical activity. This statistical approach is one way of approximating unknown trajectories across members of a population and enables other analyses to better characterize these groups, which could be meaningful for future research on engagement in DBCIs for weight loss.
This analysis was conducted in three stages: (1) Identifying latent trajectories for each behavior; (2) Distinguishing trajectory classes across behaviors; and (3) Regressing trajectory classes onto demographic predictors and weight loss. The conceptual model guiding this analysis is displayed in Figure 1.
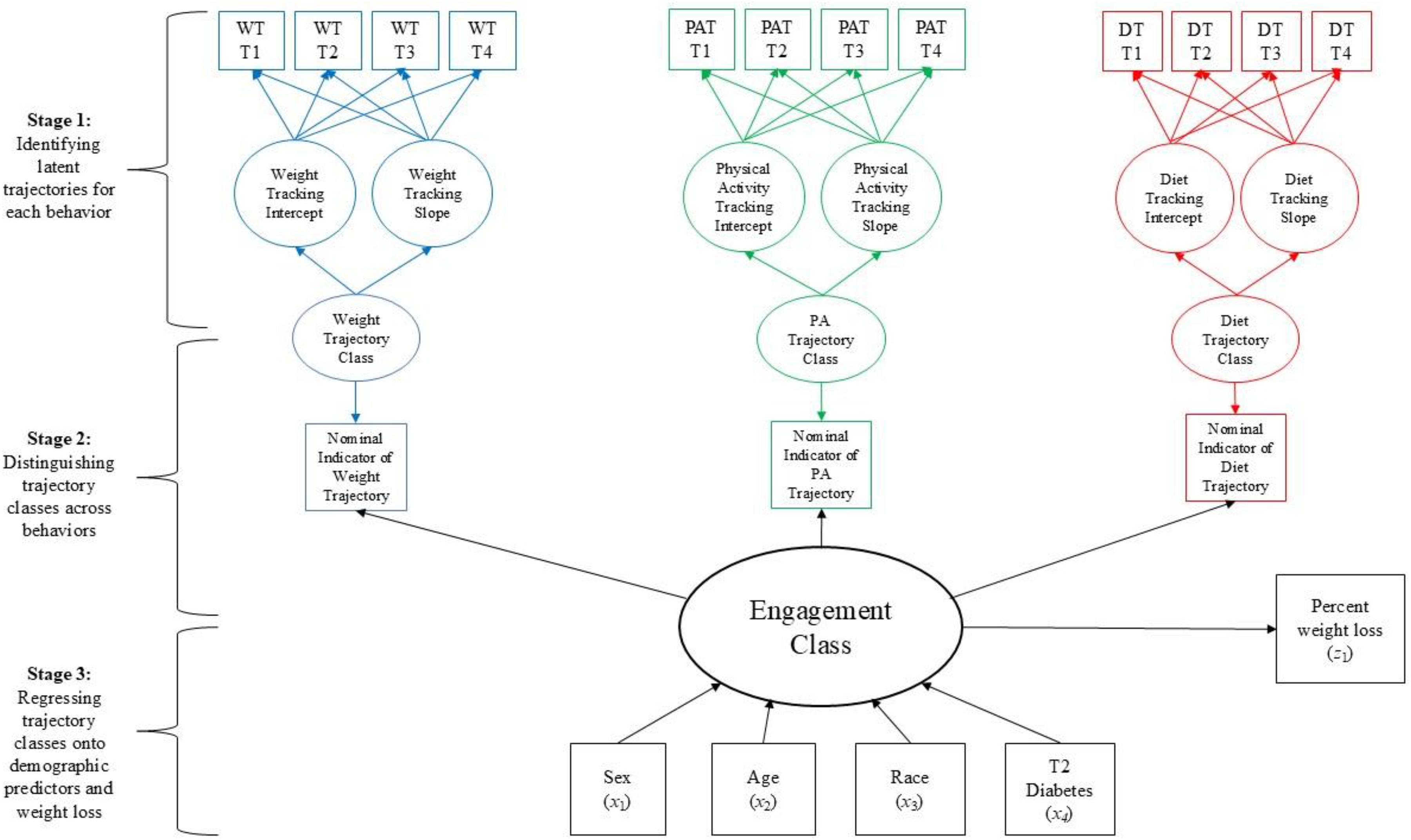
Conceptual model for analysis.
Stage 1: Identifying latent trajectories for each behavior
The LCGMs generate a discrete set of prototypical trajectories which provide a semiparametric summary of sample heterogeneity across individual trajectories. These models constrain within-class growth parameter (co)variances to zero, permitting selection of the most parsimonious latent class solution sufficient to recover most of the sample heterogeneity through between-class mean differences in growth parameters. 33
An excess of zeros in the data initially prevented the models from converging using the full dataset since LCGM requires at least two timepoints of data to estimate trajectories. Therefore, decision rules were made in conjunction with a statistician to manually reassign eligible participants for each behavior (i.e., diet, physical activity, weight) as follows: If participants showed 0 engagement across all timepoints, they were reclassified into a nonengagement trajectory class since these participants did not have data at enough timepoints to estimate trajectories using LCGM and were qualitatively distinct from participants with any engagement. If participants showed 0 engagement for at least one timepoint, they were reclassified into an intermittent-engagement trajectory class. Approximately half of participants manually assigned to this trajectory class for each behavior did not have data at enough timepoints to estimate trajectories. We decided to combine all possible patterns of intermittent engagement into one trajectory class with the commonality that engagement was missing for at least one timepoint. Only participants with values greater than 0 tracking days at each timepoint for weight (n = 172), diet (n = 85), and physical activity (n = 101) were included in the analyses to allow for model estimation of trajectories and detect heterogeneity amongst engagers. Polynomial order of time (i.e., linear, quadratic) was tested for each LCGM and applied as appropriate to improve fit. All variables were treated as continuous.
Models were constructed ranging from two to four trajectory classes and fit was evaluated using Akaike's Information Criterion (AIC), Bayesian Information Criteria (BIC), and Sample Size Adjusted BIC (SSBIC), where lower values indicate greater model parsimony. 34 Due to the modest sample size, we did not enumerate more than four trajectory classes. The entropy index was also used to describe the class solution, where values approaching 1 indicate clearer delineation of classes. Parametric bootstrapped likelihood ratio tests (LRTs) were used to compare nested models, where a significant p-value indicates better fit of the model with more classes. The optimal class solution at this step was selected based on the best-fitting model, interpretability of the class solution, and class sizes.
Stage 2: Distinguishing trajectory classes across behaviors
Once these classes were identified, second-layer mixture modeling was applied to estimate codeveloping patterns of weight, diet, and physical activity tracking over the 12-month intervention. Participants with 0 tracking days at any time point were added back in at this layer. This second-layer mixture model enabled detection of latent classes (i.e., groups of individuals following similar development of self-monitoring behaviors over time) through finite mixture modeling. Models ranging from three to five classes were created and assessed for model fit using the criteria previously described to determine the best fitting number of classes for our sample of participants. The resulting predicted group membership was used as a grouping variable to analyze demographic predictors and examine associations with intervention outcomes (see Figure 1).
Stage 3: Regressing trajectory classes onto demographic predictors and weight loss
Multinomial regression was used to examine associations between demographic categorical predictors of sex, race, and type II diabetes status, as well as continuous predictors of age and BMI, and predicted group membership, with one group as the reference category. Predicted group membership was dummy-coded and linear regression was used to examine associations between predicted group membership and predicted percent weight loss at 12 months. Four models were constructed with each level of predicted group membership as the reference category to make all possible comparisons for predicted percent weight loss between groups. Full information maximum likelihood estimation was used to account for missing data, assumed missing at random. All analyses were conducted using Mplus version 8. 35
Results
Participant characteristics
Intervention participants (N = 363) were a majority female (73.3%), with an average age of 51.9 (SD = 10.9) years and BMI of 35.4 (SD = 5.5) kg/m2. Most participants identified as white (86.9%), with 17.6% identifying as either Black (12.4%) or another race (5.2%). Twelve percent of participants reported having type 2 diabetes at baseline. Average percent weight loss at 12 months was 3.34% (SD = 7.19) among completers (n = 318). There were no associations between participant characteristics and loss to follow-up at 12 months.
Stage 1: Latent class growth models
Three-trajectory models with linear functions of time emerged as the best fitting models among participants who engaged at each timepoint for weight (n = 169, 46.6%), diet (n = 82, 22.6%), and physical activity (n = 98, 27.0%) tracking based on fit statistics and parametric bootstrapped LRTs (Supplementary Table 1). Trajectory classes were similar across all three behaviors. For each behavior, one trajectory class had the lowest intercept and a slight decline over time, indicating a consistently low level of engagement with weight (n = 83), diet (n = 21), and activity (n = 39) tracking. Another trajectory class had the highest intercept and a slight decline over time, indicating a consistently high level of engagement with weight (n = 51), diet (n = 42), and activity (n = 29) tracking. The third trajectory class had a high intercept and a large negative slope, indicating a high starting level of engagement with tracking that was not sustained over time for weight (n = 35), diet (n = 19), and activity (n = 30). For each behavior, participants who did not engage at each timepoint were manually assigned to either a nonengagement or intermittent-engagement trajectory class. Participants assigned to the nonengagement trajectory class had 0 tracking days at all timepoints for weight (n = 28, 7.7%), diet (n = 90, 24.8%), and activity (n = 106, 29.2%). Participants assigned to the intermittent-engagement trajectory class had 0 tracking days for at least one timepoint for weight (n = 166, 45.7%), diet (n = 191, 52.6%), and activity (n = 159, 43.8%).
Stage 2: Second-layer mixture model
Engagement trajectories were similar across behaviors within the same class, shown in Figure 2. A four-group model characterizing self-monitoring behavior codevelopment emerged as the best fitting model since AIC, BIC, and SSBIC improved, and entropy was the same as the three-group model. Additionally, the parametric bootstrapped LRT indicated that a four-group model was a significantly better fit than a three-group model (p < 0.001), but the five-group model was not a significantly better fit than the four-group model (p = 0.24), as shown in Table 1.

Average tracking days for weight, diet, and physical activity by group.
Fit statistics for second-layer mixture model (N = 363).

AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; LRT: Likelihood Ratio Test.
The largest subgroup (n = 176, 48.5%) was labeled low/declining-engagers because they were characterized by relatively low average tracking days at Time 1 that declined to near-zero average tracking days by Time 4 across all three behaviors. One subgroup (n = 82, 22.6%) was labeled never-engagers owing to their near-zero or zero average tracking days at each timepoint across all three behaviors. A smaller subgroup (n = 47, 12.9%) was labeled early-engagers because of their relatively high average tracking days at Time 1 that moderately declined by Time 4 but never reached zero average tracking days at any timepoint across all three behaviors.
Finally, another subgroup (n = 58, 16.0%) was labeled sustained-engagers because they were characterized by consistently high average tracking days that only slightly declined over time across all three behaviors (Figure 2).
Stage 3: Associations between trajectory classes, demographic predictors, and weight loss
The low/declining-engager group was used as the reference category because almost half of participants (48.5%) fell into this group. The odds of being in the sustained-engager group relative to the low/declining-engager group increased by a factor of 1.06 for every year increase in age, controlling for sex, race, type II diabetes status, and BMI (p < 0.001). Controlling for all other covariates, the odds of being in the never-engager group relative to the low/declining-engager group increased by a factor of 3.91 for participants who identified as a race other than white or Black (p = 0.01). The odds of being in the early-engager group relative to the low/declining-engager group decreased by a factor of 0.88 for every 1 unit increase in BMI at baseline, controlling for all other covariates (OR = 0.88, p = 0.001). There were no other significant associations.
The model explained 31% of variance in percent weight loss at 12 months (R2 = 0.32), which was statistically significant (p < 0.001). Controlling for sex, age, race, type II diabetes status, and BMI, sustained-engagers had significantly greater percent weight loss at 12 months compared with all other groups. These differences were also significant at 3 and 6 months. Early-engagers had significantly greater percent weight loss at 12 months than low/declining-engagers and never-engagers. These differences were also significant at 3 and 6 months. Percent weight loss at 12 months was not significantly different between low/declining-engagers and never-engagers. However, at 3 and 6 months low/declining-engagers had significantly greater percent weight loss than never-engagers. All results are summarized in Table 2.
Differences in predicted percent weight loss at 12 months, controlling for sociodemographic covariates.

*p < 0.05; sociodemographic control covariates = sex, age, race, type 2 diabetes status, baseline body mass index (BMI).
SE: standard error.
Controlling for covariates, average predicted percent weight loss at 12 months was 10.4% (SE = 1.05) for sustained-engagers and 5.1% (SE = 0.96) for early-engagers. Average predicted percent weight loss at 12 months was less than 2% for both low/declining-engagers and never-engagers at 1.30% (SE = 0.42) and 0.48% (SE = 0.76), respectively, as shown in Figure 3.

Predicted percent weight loss (PWL) at 3, 6, and 12 months by group and controlling for covariates (N = 363).
Discussion
Results from this exploratory trajectory analysis provide evidence that individual engagement patterns for self-monitoring are similar across weighing, activity, and dietary tracking behaviors and can predict treatment response in an online weight management intervention. Continued research on patterns of engagement over time with other intervention components, such as lesson page views, visits to the problem-solving tool, or posts to the message board could provide a more comprehensive view of individual engagement patterns across intervention features that can predict weight loss. In addition to these behavioral dimensions of engagement, future research could also consider cognitive and affective dimensions of engagement, which may help researchers better understand how to measure this complex construct. 36
Similar patterns of engagement over time have been identified in other digitally delivered interventions for weight management.37–39 Demment and colleagues used latent class analysis to identify engagement trajectories in an online intervention to prevent excessive gestational weight gain during pregnancy, including “super-users” (i.e., high and consistent use of all intervention features), “medium-users” (i.e., almost consistent use of weight tracker and high use of other intervention features), and “nonusers” (i.e., never engaged with intervention features). 37 Goh and colleagues used latent-class growth modeling to identify engagement trajectories in an 8-week diabetes self-management intervention delivered via a smartphone app, including “consistent users” (i.e., weekly use throughout the 8 weeks), “intermittent-waning users” (i.e., occasional weekly use in the first 4 weeks), and “minimal users” (i.e., no app use or use only in the first 2 weeks). 38 Lavikainen and colleagues used latent class growth models to identify engagement trajectories over 12 months with an app designed to prevent type 2 diabetes, including “daily usage,” “twice weekly usage,” “weekly usage,” and “terminated usage” (i.e., few usage days in the first months dropping close to zero after 6–7 months). 39 To ease comparison across studies, future research could synthesize engagement patterns identified in the literature. 40
The proportion of participants categorized into these engagement patterns is also similar across studies. For example, a small group of “consistent” users characterized by high and consistent engagement emerged. In the current study, sustained-engagers accounted for 16% of the sample, compared to 13% (“super-users”), 37 9.5% (“consistent users”), 38 and 15.1% (“twice weekly” and “daily usage”). 39 A similar group of “nonusers” characterized by no use or minimal engagement also emerged. In the current study, never-engagers accounted for 22% of the sample, compared to 20% (“nonusers”). 37 In the literature, most participants are categorized into a “minimal” engagement category characterized by overall low or occasional engagement in the first few weeks of the intervention. Demment and colleagues found that 38% of their sample were categorized as “almost consistent” and “inconsistent” weight trackers. 37 In the current study, low/declining-engagers accounted for 48.5% of the sample, compared to 46.9% (“terminated usage”) 39 and 78.6% (“minimal users”). 38 Given the high proportion of participants categorized into the “minimal” engagement category across studies, future research could explore possible heterogeneity within this group, such as participant characteristics and outcomes on intervention targets.
Greater engagement with self-monitoring was associated with more favorable weight loss outcomes over 12 months, which aligns with findings from other DBCIs for weight loss.7,8,23,41–43 In the current study, low/declining-engagers (48.5% of the sample) did not achieve 5% weight loss at 12 months, whereas early-engagers (13% of the sample) did achieve clinically significant weight loss. In both groups, engagement decreased over time. However, on average, early-engagers engaged at each timepoint whereas low/declining-engagers did not, especially by months 6–12, which may account for the significant difference in weight loss between the groups at 1 year. Alternatively, Lehmann and colleagues found that within the first 3 months of a blended-care weight loss intervention, greater engagement with the mobile app component was predictive of percent weight loss, while there was no significant association between engagement and weight loss at 6 months. 44 This finding suggests that early engagement, rather than sustained engagement, may be critical for achieving desired weight loss outcomes. In a systematic review to conceptualize engagement in digital interventions, Perski and colleagues suggest that there may be a predetermined level of engagement at which an intervention is effective (i.e., “optimal dose”). 15 It is possible that participants who engage early in digital weight loss interventions achieve an “optimal dose” of engagement that can result in significant weight loss.
An unmeasured third variable could also explain the observed relationship between increased engagement and favorable intervention outcomes. 15 In the current study, participants with higher BMI were significantly less likely to be in the early-engager class relative to the low/declining-engager class. Therefore, it is possible that individuals with higher BMI may need more support to sustain engagement with self-monitoring. Alternatively, psychosocial variables associated with BMI may have contributed to the observed relationship between increased engagement and favorable intervention outcomes. Although the current study did not examine associations between psychosocial constructs and engagement, other studies have found associations between engagement and baseline motivation levels, 45 baseline self-efficacy scores, 45 exercise motivation scores, 38 and baseline diet quality. 39 Other studies have noted likely relationships between depression and lower engagement in DBCIs, though this relationship has not been explored in-depth in the literature.15,46,47 Future studies could investigate the extent that different psychological characteristics may be related to these latent engagement patterns, or test adaptive components for lapses in engagement, such as arranging meetings with a counselor, to improve outcomes among groups that may be less likely to engage long term.
Age and race were also associated with likelihood of engagement class membership. Relative to the low/declining-engager class, older participants were more likely to be in the sustained-engager class. Similarly, Glasgow et al. and Lavikainen et al. found that older participants were more likely to demonstrate ongoing engagement in digital interventions for weight loss and type 2 diabetes prevention,39,45 respectively, and other studies have shown young adults to be at risk for low engagement. 48 Self-identified Black and Indigenous People of Color (BIPOC) participants have also been observed to have lower engagement in these types of interventions. Glasgow and colleagues found that African Americans were less likely to demonstrate ongoing engagement in an IWL program. 45 Blackman Carr and colleagues also found that African American women had significantly fewer website log-ins compared with non-Hispanic white women in a 4-month randomized controlled trial based on the Diabetes Prevention Program. 49 Interestingly, the current study found that participants that identified as a race other than white or Black were more likely to be in the never-engager class relative to the low/declining-engager class. Social determinants of health factors may drive disparities in engagement rather than reported race, which may explain why the current study did not observe the same trend among participants who identified as Black. It is important to consider intervention characteristics which may be contributing to reduced engagement among BIPOC participants to ensure the field does not fall into the trap of creating recommendations which are primarily derived by- and for- white demographics. 50
Strengths of this study include a powerful data-driven analysis that identified true usage patterns based on multiple trajectories of objectively measured engagement with self-monitoring website components over 12 months. Additionally, self-monitoring data was captured automatically from the website interface. Limitations include a modest sample size (N = 363), especially for participants with engagement data at each timepoint for weight (n = 169, 46.6%), diet (n = 82, 22.6%), and activity (n = 98, 27.0%), which yielded small class sizes in the LCGMs. Additionally, the proportion of participants who identified as a race other than white or Black was relatively small at 5.2% (n = 19). Given that study participants were majority white female, the generalizability of this study is limited. Participants who engaged at some but not all timepoints were manually assigned to an intermittent-engagement trajectory class for weight (45.7% of participants), diet (52.6% of participants), and activity (43.8% of participants) tracking. Although approximately half of participants manually assigned to this trajectory class for each behavior did not have data at enough timepoints to estimate a trajectory using LCGM, a smaller proportion of participants manually assigned to this class did have data for at least two timepoints. Hence, the LCGMs did not distinguish potential heterogeneity in engagement patterns among these participants (23% of participants for diet, 24% of participants for weight, and 17% of participants for physical activity). This analysis did not account for the different ways participants could track their diet during the intervention. Although all participants had to directly engage with diet tracking, participants using different Eating Plans may have engaged differently. For example, one dietary format had users log all calories they consumed manually, while another was assigned to a ‘meal plan’ format that recorded preset menu items with calories automatically and requested users note any changes from that plan. Regardless of which dietary monitoring option participants selected, this study quantified dietary self-monitoring engagement as the total number of days any dietary tracking data were entered into the website across the 4 timepoints. Finally, the mode of self-monitoring was the same across all three behaviors (i.e., participants entered their information on the intervention website), which may explain why individual engagement patterns for self-monitoring were similar across behaviors. Future studies could examine whether varying engagement patterns emerge across behaviors using different modes of self-monitoring, such as a digital scale for weight tracking, an app-based food log for diet tracking, and a wearable device for activity tracking. Research recommendations include exploring usage patterns based on multiple trajectories of engagement with other intervention features, synthesis of engagement patterns over time across studies, and further examination of heterogeneity in engagement patterns within the “minimal” or “intermittent” engagement category.
Clinical implications
On average, participants in the low/declining-engager class adhered to weight and dietary tracking for less than 30 days and engaged in physical activity tracking for less than 20 days during the first 3 months of the intervention. Therefore, promoting increased engagement among intervention participants with low adherence to self-monitoring in the first month of an intervention (approximately 2–3 days or less per week), especially those with a higher BMI and those who are younger and/or identify as BIPOC, is critical to keeping more participants engaged for longer in the intervention, which in turn may improve weight loss outcomes for more participants.
Conclusions
This study identified four classes of engagement trajectories among participants in a 12-month DBCI for weight loss and determined that sustained and early-engagement patterns were associated with improved weight loss at 12 months. Engagement patterns were similar across self-monitoring behaviors within the same class, which may have resulted from participants using the same platform for self-monitoring across all three behaviors. Age, race, and baseline BMI were associated with engagement class membership such that older participants were more likely to exhibit the sustained engagement pattern, participants that identified as a race other than white or Black were more likely to never engage, and participants with a higher BMI were less likely to exhibit the early engagement pattern, compared to participants with low engagement. Given that participants with low engagement did not achieve clinically significant weight losses, future research should explore how to identify these participants early in an intervention to promote increased engagement with self-monitoring.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261434062 - Supplemental material for Examining latent trajectories of participant engagement in a 12-month eHealth weight management intervention
Supplemental material, sj-docx-1-dhj-10.1177_20552076261434062 for Examining latent trajectories of participant engagement in a 12-month eHealth weight management intervention by Julianne M Power, Lex Hurley, Nisha Gottfredson O’Shea, Brooke T Nezami, Christopher Sciamanna and Deborah F Tate in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Karen Hatley, Molly Diamond, and Kristen Polzien for their invaluable assistance with the primary LNPA intervention. The authors would also like to thank Cathy Zimmer and Chris Wiesen for their important contributions to this secondary data analysis.
ORCID iDs
Ethical approval
The parent study was a clinically registered trial with identifier NCT01606813, approved by the Institutional Review Boards at both study sites. This secondary analysis was exempt from ethical approval as all data were de-identified such that the identities of human subjects could not be readily ascertained directly or through identifiers linked to the subjects.
Consent to participate
Within the parent study, primary care providers and patients completed and returned informed consent forms prior to randomization and data collection.
Consent for publication
Not applicable.
Contributorship
JMP authored the first draft of the manuscript and implemented coauthors’ feedback, conceived the secondary study design. LH, NG, BTN, CS, and DFT: supervision, manuscript review, and methodology. CS and DFT: main trial design, funding, and data acquisition. All authors have read and approved the final version of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases (R01-DK095078).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
De-identified data and Mplus code from this analysis may be made available by request to the corresponding author.
Guarantor
JMP.
Supplemental material
Supplemental material for this article is available online.