
Abstract
Objective
In response to COVID-19, the fall prevention program (FPP) at Sunnybrook Health Sciences Centre was modified to be delivered virtually. We compared patient populations assessed for the FPP virtually versus in-person to explore equitable accessibility.
Methods
A retrospective chart review was performed. All patients assessed virtually from the beginning of the COVID-19 pandemic until the end of abstraction (April 25, 2022) were compared to a historic sample of patients assessed in-person beginning in January 2019. Demographics, measures of frailty, co-morbidity, and cognition were abstracted. Wilcoxon Rank Sum tests and Fisher's Exact tests were used for continuous and categorical variables, respectively.
Results
Thirty patients were assessed virtually and compared to 30 in-person historic controls. Median age was 80 years (interquartile range 75–85), 82% were female, 70% were university educated, the median Clinical Frailty Score was 5 out of 9, and 87% used >5 medications. Once normalized, frailty scores showed no difference (p = 0.446). The virtual cohort showed significantly higher outdoor walking aid use (p = 0.015), reduced accuracy with clock drawing (p = 0.020), and nonsignificant trends toward using >10 medications, requiring assistance with >3 instrumental activities of daily living (IADLs), and higher treatment attendance. No significant differences were seen for time-to-treat (p = 0.423).
Conclusion
Patients assessed virtually were similarly frail as the in-person controls but had increased use of walking aids, medications, IADL assistance, and cognitive impairment. In a Canadian context, frail and high socioeconomic status older adults continued to access treatment through virtual FPP assessments during the COVID-19 pandemic highlighting both the benefits of virtual care and potential inequity.
Keywords
Introduction
The majority of older adults over the age of 65 in Canada are community dwelling, meaning they reside independently at home outside of hospitals and long-term care facilities. 1 It is important to prevent falls in community-dwelling older adults as they are associated with increased morbidity and mortality. 2 Prevention may include participation in programs that focus on improving balance and strength.3,4 The COVID-19-related isolation increased the risk of developing sedentary lifestyles and loneliness, which can worsen health, increasing frailty and falls.2,5–9 This highlights the importance of continued fall prevention efforts during a time when access to in-person programs was limited.
Before the pandemic, Sunnybrook Hospital's fall prevention program (FPP) was an 8-week group-exercise program designed to prevent falls by helping community-dwelling older adults build strength and balance.
10
The weekly one-hour-group sessions, instructed primarily by physiotherapists, taught various strength and balance exercises that patients could continue daily at home for long-lasting fall prevention. The exercises were taught in circuits and were tailored to the individual based on an initial assessment. Some examples of circuit exercises include:
Balance building—Stand facing the counter and hold lightly with both hands. Push up onto your toes and hold for 5 s. Repeat 10 to 15 times, now rock back onto your heels, lifting your toes up. Repeat 10 to 15 times. Strength building—Punch forward with one arm while the other arm pulls back. Alternate one arm and then the other with a light weight or can of soup.
Participants would also use the Nu-Step machine, the arm ergometer, and would walk the hallway for 5 minutes each. Additionally, a multidisciplinary team contributed to education sessions on three of the days covering nutrition, medications, and home safety. The program's ability to safely assess and treat patients was impacted during the pandemic and resulted in the implementation of a virtual format which had to be tailored according to each individual patient and public health restrictions at the time of referral. Changes that were made include the shift to virtual assessments, the reduction in the number of sessions from eight to four, and a variety of platforms for exercise classes including video calls, pre-recorded videos, and a hybrid model that included these virtual methods with complementary in-person sessions. While program changes were carefully planned, the impact on accessibility, feasibility, and effectiveness is unknown. Virtual care may introduce barriers due to the need to access and navigate online platforms.
11
The accuracy, safety, and intimacy of an in-person program may also be impacted.
11
It is critical to examine the demographics including socioeconomic status (SES), frailty, and cognition of the population seeking the FPP virtually. This will help inform quality improvement and our understanding of the utility of a virtual FPP beyond the pandemic.
This retrospective chart review compares the patient population who were assessed for the Sunnybrook FPP virtually versus in-person and explores impact on equitable accessibility.
Methods
Study design
This was a retrospective single-centre cross-sectional study. We followed the STROBE statement in the preparation of this manuscript (Supplemental material: Table 2). 12 This study did not require patient consent. The Research Ethics Board approved this study (REB ID: 5029).
Participants and setting
The population consisted of community-dwelling older adults referred to the Sunnybrook FPP. This program required primary practitioner referral. Criteria to guide referral includes anyone 65 years or older who is at risk of falling, able to walk 25 m, and who is considered able to safely participate in the supervised exercise program. 10 Prior to the pandemic, the FPP assessment and treatment was entirely in-person (Figure 1). In response to the COVID-19 pandemic, telephone screening was implemented to screen for red flags requiring the assessment to be done in-person; red flags included no access to a computer or smart phone, a visit to the emergency room in the past 6 months, or a Fatigue, Resistance, Ambulation, Illnesses, & Loss of Weight (FRAIL) scale score ≥ 2 out of 5. Patients suitable for a virtual assessment joined through video platforms such as Zoom or Microsoft teams. A falls risk assessment was conducted, and the clinical judgment of the geriatrician and physiotherapists was used to determine if the patient should participate in the virtual FPP or a hybrid program with select in-person components. The fall risk assessment included a comprehensive falls history assessing frailty and fall risk factors. The assessment also required participants to perform a set of tasks assessing strength and balance. In-person, these tasks included Berg balance scale test, Timed Up & Go test, 2-minute walk test, and 6-minute walk test. Virtually, the physical performance battery test was used. Values included in the assessment are outlined in Supplemental material: Table 3. At the time of data abstraction, only 30 patients had participated in the FPP since the onset of the pandemic. To create the largest sample possible, we included the first 30 patients who received a virtual assessment for the FPP, which spanned a period from the beginning of the COVID-19 pandemic to April 25, 2022. As a historic control group, we included the first 30 patients assessed in-person beginning January 1, 2019.

Modifications of Sunnybrook Health Sciences Centre's fall prevention program due to COVID-19.
Data collection and variables
The following were abstracted from patient charts: demographics, care delivery variables, measures of cognition, measures of frailty and fall risk factors, and measures of balance. A full list is included in Supplemental material: Table 3. Median household income was determined based on the postal code forward sortation areas using National Household Survey data from 2011. 13 Date of assessment and treatment were used to calculate the number of unattended treatments in each cohort as well as time between assessment and treatment (time-to-treat). Age, time-to-treat, and frailty measures were treated as continuous variables. The remaining were treated as categorical.
Analysis
Based on the method of assessment, participants were categorized into a virtual cohort (VC) or an in-person cohort (IPC) and compared using Wilcoxon Rank Sum tests for continuous variables and Fisher's Exact tests for categorical variables. Due to limitations in virtual assessment, the program changed the administered frailty measure from the Clinical Frailty Scale to the FRAIL questionnaire beginning in July 2020. These tools assess frailty via different methods and are scored from 1 to 9 and 0 to 5, respectively.14,15 We first compared the Clinical Frailty Scale directly between patients with available data. This resulted in uneven comparison as 29 IPC participants were compared to 11 VC participants. To solve this discrepancy, we used min–max normalization to allow for comparisons between the two scales. 16 Missing data were managed using pairwise deletion. 17 The analysis for this paper was generated using R (R Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, and a p-value of ≤ 0.05 was considered statistically significant.
Results
Demographics
Among all 60 patients, the median age was 80 years (interquartile range (IQR) 75–85), 82% were female, 70% were university educated, the median household income was CAD$83,019, and 97% spoke English as their primary language (Table 1). The IPC had a higher proportion of females compared to the VC (56% VC, 83% IPC; p = 0.047), and the other demographic factors were not significantly different between cohorts.
Patient characteristics.

ADLs: activities of daily living; IADLs: instrumental activities of daily living; ED: emergency department; IQR: interquartile range; NA: not applicable.
Frailty
Clinical Frailty Scale scores were measured in 29 IPC and 11 VC participants. There was a significant difference in median scores (5 of 9 VC [IQR 5–5], 5 of 9 IPC [IQR 4–5]; p = 0.041), with higher frailty among VC patients with available data. When using min–max normalization to additionally include 17 VC participants scored with the FRAIL questionnaire, there was no significant difference found (p = 0.531) (Figure 2).
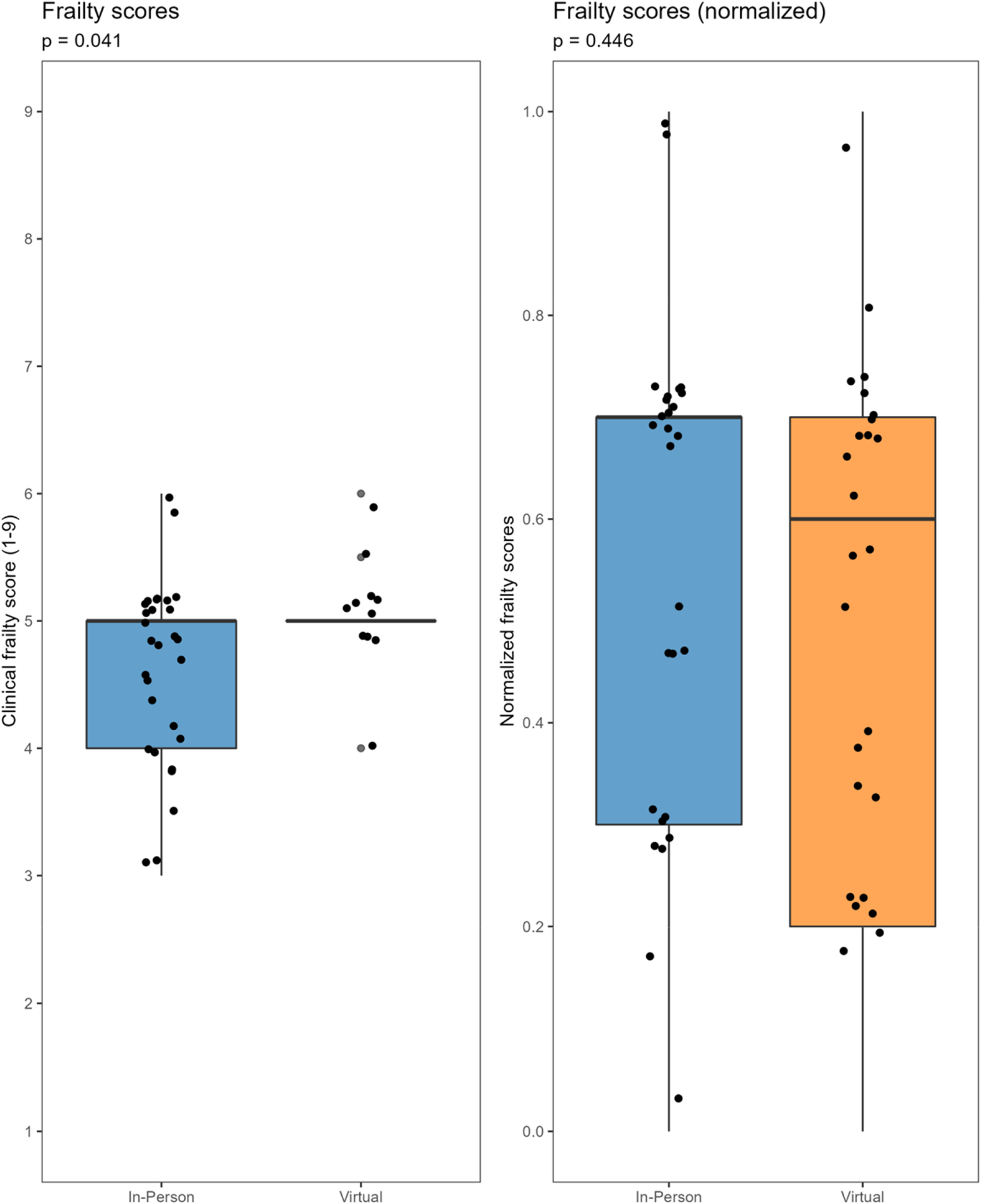
Frailty in the virtual and in-person cohorts of patients assessed for the fall prevention program.
Other measures of functional and cognitive impairment
The VC showed significantly higher use of outdoor walking aids (80% VC, 47% IPC; p = 0.015) and poorer performance on the clock drawing portion of the Mini-Cog test with less participants scoring 3 out of 3 (25% VC, 77% IPC; p = 0.020). Nonsignificant trends included a larger proportion of the VC using >10 medications (37% VC, 13% IPC; p = 0.127), and requiring assistance with >3 IADLs (50% VC, 30% IPC; p = 0.367) (Figure 3). Additional variables are reported in the Supplemental material section and were either not significant or had too many missing values to make notable comparisons.

Selected measures of functional decline, cognitive decline, and program accessibility in the virtual and in-person cohorts of patients assessed for the falls prevention program.
Attendance and time-to-treat
Attendance and time-to-treat were compared between cohorts. Seventeen patients were assessed but did not attend treatment (28%). Of these, 10 were in the in-person cohort and 7 were in the virtual cohort. The VC had a nonsignificant higher treatment attendance (77% VC, 67% IPC; p = 0.567). Reasons for missed treatment are reported in Supplemental material: Table 3. There was no significant difference in time-to-treat (50 days VC, 53 days IPC; p = 0.423) (Figure 3).
Discussion
This study characterizes the patient population assessed for the Sunnybrook FPP virtually versus in-person. The demographics remained similar between cohorts and characterize the population as predominantly university educated and high-income earning suggestive of high SES. Markers of high SES have been found to improve older adults’ ability to access and navigate virtual care despite frailty. 18 One noticeable difference between the cohort demographics was a greater number of female participants. Females have a longer life expectancy than males, and high-SES females tend to seek care more often than males.19,20 This may explain the predominantly female sample. A significantly lower proportion of females attended the virtual FPP compared to in-person FPP. Men and women who received their education in the 1960s and 1970s were entering the workforce at the same time; however, women from this generation were more likely to discontinue working once having children and computer literacy may have declined as a result. 21 The reason for a lower female attendance in the virtual program is not fully understood; however, societal norms from this generation of seniors may influence computer literacy and thus accessibility of virtual care. Our data abstraction reveals similar frailty between cohorts; however, there were some indications of a frailer VC. This was reflected in a VC with increased walking aid use, a greater number of medications, more assisted IADLs, and poorer Mini-Cog test performance; the clock drawing test requires patients to apply their visual-spatial functioning to draw the correct arrangement of numbers inside a circle followed by the executive functioning to appropriately add clock hands in the position of “half-past-ten.” The difference in cognition between groups in this case was significant and demonstrates the program reaching a frailer population with reduced cognitive functioning. More specifically, patients with decreased visual-spatial and executive functioning were able to access the assessments and program when delivered virtually. The number of missed treatments and the time-to-treat were similar between cohorts suggesting that virtual assessment did not delay access to care. This is critical as delayed access to care in geriatric patient populations is associated with functional decline and premature death. 22 The unimpaired accessibility suggests that technology is less of a barrier to this frail geriatric population characterized as high SES. Virtual care could be alleviating barriers to in-person programs thus increasing access. For example, a larger proportion of the VC required assistance with > 3 IADLs and had more cognitive impairment suggestive of the inability to independently drive to in-person programs, 23 yet virtual appointments remained accessible to these patients. Previously, age has been associated with decreased accessibility to virtual care 18 ; however, our findings reveal high-SES frail older adults are able to continue accessing FPP treatment following virtual assessments. This demonstrates the existing equity within the virtual FPP as a population both frail and elderly continued to access supportive care. Our study also demonstrates existing inequity within the virtual FPP as access may depend on high SES. These findings help to inform equitable quality improvement as resources should be made available to less affluent populations to help alleviate this inequity and facilitate virtual FPP accessibility. A separate study is currently underway that will provide a qualitative lens through patient interviews to gain a deeper understanding on barriers, alleviators, and overall experiences with the virtual program to further inform quality improvement.
To date, there is no literature on the outcomes of virtually delivered FPPs. Relevant literature includes a study by Aubert et al. 24 that examined a virtual diabetes management program for older United States veterans. Their results revealed increased virtual physician–patient visits overcompensating for the loss of in-person visits. Furthermore, diabetes control was not impacted suggesting maintenance of accessible and effective care. This supports our findings by suggesting that virtual programs can remain accessible to certain geriatric populations. In contrast, Mañago et al. 25 examined the impact of virtual exercise classes for geriatric patients with Parkinson's disease noting reduced exercise quantity and intensity and identifying that technology and lack of socialization were barriers to the virtual format. These findings suggest limitations to accessibility and effectiveness of virtual programs depending on the programs purpose and its intended patient population. Existing literature has explored various forms of virtual care for older adults and suggests patient preference for telephone calls over video calls.26–28 These studies have also identified successful virtual care depends on SES and eHealth literacy—higher income and educated geriatric populations are better equipped for the technological requirements of video-based programs.26–28 This supports our findings as the virtual FPP remained accessible to a frail high-SES patient population.
Limitations include the study population of patients assessed for the FPP at Sunnybrook, which tends to service a high-SES population. Income estimates were calculated using data from 2011 which likely underestimated income. This may limit generalizability to other centers, particularly those in rural areas who could benefit from specialized geriatric care delivered virtually to reduce travel time and improve access. Regarding methodology, the convenience sampling created the opportunity for selection bias; however, the approach was used to maximize the available virtual cohort sample size. The small sample size also did not allow for sample matching, thus not controlling for possible confounders. Furthermore, direct comparison of some measures was not possible as some assessment measures used in-person were not done virtually, resulting in a high proportion of missing data (Supplemental material: Figure 4). Missing data may not be missing at random and thus pairwise deletion could result in biased estimates potentially impacting generalizability. This work is exploratory and hypothesis-generating and further studies may build upon our findings.
Notwithstanding these limitations, these findings suggest utility of virtual assessment beyond the pandemic and serves as a foundation for further investigation into the specific benefits and barriers of the virtual FPP to inform equitable quality improvement.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231178410 - Supplemental material for Virtual fall program assessment for frail Canadian community-dwelling older adults: Examining equitable accessibility
Supplemental material, sj-docx-1-dhj-10.1177_20552076231178410 for Virtual fall program assessment for frail Canadian community-dwelling older adults: Examining equitable accessibility by Sophie M. Weiss, Matthew Castelo, Barbara Liu and Mireille Norris in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to acknowledge the pivotal role of Martha Ta who provided administrative support for the study and who's role in launching the virtual fall prevention clinic was key.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The appropriate permission was obtained from the research ethics board (REB ID: 5029).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Sunnybrook Program to Access Research Knowledge for Black and Indigenous Medical Students.
Patient consent
Patient consent was not obtained for this study as it was a retrospective data abstraction using existing hospital records and was approved by the research ethics board.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.