
Abstract
Objective
Osteoarthritis (OA), particularly knee OA, is a leading cause of disability and poses significant challenges in healthcare management. Mobile applications (apps) have emerged as potential tools to support therapeutic exercise by providing tailored programs, instructional content, and progress tracking. This systematic review evaluates the efficacy of mobile apps in enhancing therapeutic exercise for knee OA management.
Methods
A systematic review was conducted, analyzing randomized controlled trials (RCTs) to assess the impact of mobile apps on pain and knee function in patients with OA. The review followed the Cochrane Handbook guidelines and was registered with PROSPERO. Inclusion criteria focused on RCTs involving adults aged 40 and above with knee OA, and outcomes were measured based on pain intensity and knee function.
Results
Five RCTs met the inclusion criteria. The results varied: while some studies demonstrated minor improvements in pain and function with app-based interventions, others showed comparable effectiveness to traditional methods. The review highlights the potential of mobile apps to offer benefits in managing knee OA, though outcomes were inconsistent due to intervention and population heterogeneity.
Conclusion
Despite the low certainty of evidence, mobile app-based interventions appear to have a positive impact on reducing pain and improving physical function in patients with knee OA. Continued research is essential to better understand the effectiveness and long-term impact of mobile technology in OA management, underscoring the value of digital health interventions in enhancing patient care.
Introduction
Osteoarthritis (OA) represents the main cause of disability in the Western world and the main cause of days lived with disabilities in the European population. This trend is constantly growing also in consideration of population ageing. 1
Therapeutic exercise stands as a cornerstone in the management of knee OA, aiming to ameliorate symptoms, enhance joint function, and improve overall quality of life. However, adherence to exercise regimens often presents a formidable challenge, necessitating innovative approaches to optimize engagement and outcomes. 2
Opportunities presented by digital technologies in modern health and healthcare scenarios have been receiving incredible attention both from regulatory authorities and the clinical and scientific world. 3
In recent years, the proliferation of mobile technology has spurred interest in leveraging mobile applications (apps) as adjunctive tools in knee OA management. 4 These apps offer the promise of delivering tailored exercise programs, providing instructional multimedia content, facilitating progress tracking, and fostering peer support networks, all accessible at the fingertips of patients. Such advancements hold the potential to address barriers to traditional exercise therapy, including accessibility, convenience, and patient motivation. 4
While smartphone applications can provide convenient access to exercise programs and may enhance patient engagement and adherence, 5 the effectiveness compared to traditional methods may vary depending on the specific application and the individual patient.
Despite the burgeoning interest, the efficacy and utility of mobile apps in supporting therapeutic exercise for knee OA remain a subject of inquiry. While initial studies suggest promising outcomes, a comprehensive appraisal of existing evidence is warranted to elucidate the landscape of app-based interventions in knee OA management. Therefore, this systematic review, by synthesizing current literature and identifying research gaps, aims to provide insights into the role of mobile technology in augmenting knee OA management paradigms, such as pain reduction and improved function.
Materials and methods
This systematic review analyzed the effect of mobile apps on the management of therapeutic exercise in patients with knee OA in terms of pain and functioning. The “Cochrane Handbook for Systematic Reviews’ of Interventions” was used to develop, implement, and conduct the systematic review. 6 Its protocol was registered in the PROSPERO database (reference: CRD42024516781) and reported following the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P).7,8
Inclusion criteria
Types of study
We included in this systematic review only randomized controlled trials (RCT) evaluating the effect of mobile apps on the management of therapeutic exercise in patients with knee OA. We included only RCTs on humans in English without any date restrictions.
Participants
We included studies on adult people (≥40 years old) with knee OA diagnosis. Inclusion criteria were age 40 years or older, a clinical diagnosis of knee OA (defined as knee pain for > 3 months, early morning stiffness <30 minutes, crepitus, bony tenderness, and no palpable warmth), 9 as well as radiographically established knee OA (determined by Kellgren and Lawrence grade > 1 on the 1–4 scale).10,11 Exclusion criteria were as follows: system lupus erythematosus, rheumatoid arthritis, spondyloarthropathies, Sjögren syndrome, gout, scleroderma, and infectious arthritis; history of metabolic, hormonal, orthopedic, and cardiovascular disease; spinal deformities; flat feet; and previous surgery of knee/s of any cause or injection of knee/s for the past 6 months.
Interventions
We included RCTs wherein at least one group of participants utilized smartphone apps to support therapeutic exercise. Our decision to focus specifically on smartphone apps, rather than broader categories of digitally delivered interventions (e.g. web-based applications), stems from the unique features of smartphone apps, such as portability, accessibility, and enhanced user engagement through mobile devices. These characteristics can lead to different user interaction patterns and potentially more effective health-related behavior changes compared to web-based applications. Any other studies employing different intervention methods (e.g. traditional exercise programs, manual therapy, etc.) without the use of smartphone apps were deemed ineligible. We considered various types of nonsurgical treatments (e.g. traditional exercise programs, manual therapy, electrotherapies, psychological interventions, etc.) as control or comparison groups. Additionally, we included studies incorporating smartphone apps as additional interventions in the intervention group if both groups received the same baseline intervention characterized by any of the treatments.
Outcomes
We identified the intensity of pain, assessed using the numeric rating scale 12 or the relevant sections of comprehensive scales such as the Knee Injury and OA Outcome Score 13 or The Western Ontario and McMaster Universities OA Index, 14 as our primary outcome. Knee function, evaluated through the pertinent sections of these scales focusing on the knee, was considered as a secondary outcome.
Information sources
We created the search string with the research question built upon the Population Intervention Comparison Outcome (PICO) acronym. Then, we adapted it for the Cochrane Controlled Trial Register (CENTRAL), MEDLINE (via PubMed), EMBASE, and PEDro. We adopted the Cochrane Handbook for Systematic Reviews for Interventions recommendations. 6 In their book, the Cochrane group suggested using MEDLINE via PubMed, Scopus, and CENTRAL as the bare minimum requirement and other sources based on the specific topic of the review (rehabilitation). Therefore, we also adopted PEDro. Databases were searched from their inception until March 2024. After completing the study, we conducted follow-up research in May 2024 to check for any additional relevant papers that might have been published during that time. Our search did not yield any new or pertinent research findings. The complete search terms are listed in Supplemental File 1 (Research Terms). Additional records (cross-references) were searched through a manual search using references from systematic reviews and clinical practice guidelines on the use of mobile applications for therapeutic exercise in knee OA management, but no studies were found to meet the inclusion criteria.
Selection process
Articles retrieved were uploaded onto the Rayyan website (https://rayyan.qcri.org) after duplicate removal with EndNote 20. 15 Afterward, two researchers (LP and GB) independently, blindly, and systematically, applying the inclusion and exclusion criteria, reviewed titles, and abstracts to determine eligibility and to retrieve articles. In case of disagreement between the two reviewers, a third author (TP) was consulted to reach a consensus. No authors or experts were contacted to get additional studies. Afterward, the full texts of the selected papers were further screened against the inclusion criteria following the same process.
Data extraction
Two reviewers (LP and GB) extracted the following data from each selected study: authors, title, study design, setting, participants characteristics (number, age, and gender), symptoms characteristics (duration, localization, and intensity), main treatment characteristics (duration, frequency, and type of technique), control treatment characteristics, and outcomes (tools used to record each outcome, mean, and standard deviations). Disagreements in the data collection were resolved by either a consensus process or consultation with a third author (TP).
Risk of bias assessment
Two authors (LP and GB) independently assessed the risk of bias using the “Revised Cochrane risk-of-bias tool for randomized trials” (RoB 2). 16 This tool evaluates the risk of bias in five domains: randomization process, deviation from intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result. All domains are then rated as “low risk,” “high risk,” or “some concern.” If necessary, disagreements between the two investigators were resolved by discussion with a third author (TP).
Data synthesis and assessing certainty in the findings
A meta-analysis was unfeasible because of the heterogeneity of the population, comparison, and intervention. The overall quality of evidence was evaluated through the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) framework. 17 This framework allows for assessing and developing a summary of evidence in a systematic approach. For each outcome, the five GRADE domains were considered: risk of bias, imprecision, inconsistency, indirectness, and publication bias. Using the GRADE approach, the overall quality of evidence was selected between four possible levels: high, moderate, low, and very low.
Results
Study selection
A total of 2169 records were identified through database searching. After removing the duplicates (n = 282), we assessed the remaining records by titles and abstracts. Eventually, 76 studies were eligible for full-text reading. Among these 76 studies, only 3 studies met the inclusion criteria and were included in this systematic review. Two additional records (cross-references) were found through a manual search using references from a systematic review 18 about the use of mobile applications for therapeutic exercise in knee OA management and were included in this review. The screening and selection process is shown in Figure 1.

PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers, and other sources.
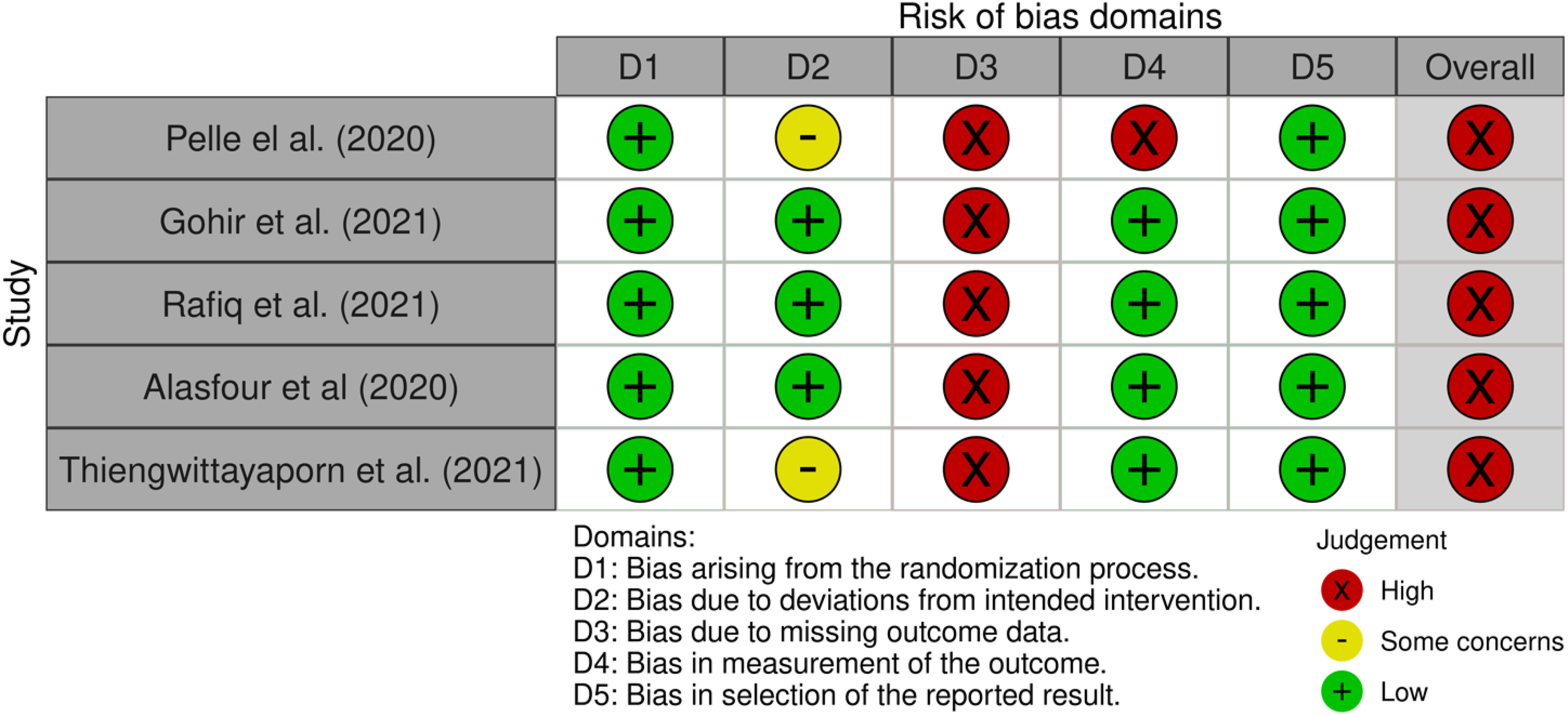
Cochrane risk-of-bias tool for randomized trials version 2 (RoB 2). In this color-coded ranking, green color represents low risk of bias, yellow some concerns, and red high risk of bias.
Study characteristics
The included articles were published between February 2020 and October 2021. Across the 6 studies, the number of participants in each study ranged from 40 to 427 (total N = 775).
In addition, all studies used a RCT design,19–22 and two were single-blind RCT.20,23 Studies were conducted in the Netherlands, 19 Malaysia, 20 the United Kingdom, 21 Saudi Arabia, 22 and Thailand. 23
The mean age of patients with knee OA ranged from 52.92 (SD 4.58) years to 66.7 (SD 9.2) years, and all studies included both men and women except for the study by Alasfour and Almarwani, 22 which included only women.
The duration of the interventions ranged from 4 weeks to 6 months and the duration of follow up ranged from 3 weeks to 6 months. None of the studies specified whether the apps or other elements of interventions such as fitness trackers, were taken away from participants at the end of the monitored intervention or left with them to be used until follow up (Table 1).
mHealth applications description
In the five studies reviewed, various mHealth applications were used to support therapeutic exercises. Pelle et al. 19 incorporated a weight management mobile application to promote healthy behaviors, including features like dietary intake tracking, physical activity monitoring, and motivational feedback. Rafiq et al. 20 used a mobile health application tailored for managing knee pain, mobility, and function in overweight and obese patients, offering exercise routines, progress tracking, and educational content to support self-management. In Gohir et al., 21 a self-management platform for pain management was employed, featuring functionalities such as pain logging, personalized advice, and symptom monitoring. Alasfour and Almarwani 22 focused on a home exercise program delivered through a mobile app, aimed at enhancing adherence to home-based physical activities and improving pain, physical function, and lower-limb strength. Thiengwittayaporn et al. 23 utilized a mobile application designed to improve exercise accuracy, providing guidance and monitoring to ensure adherence to proper techniques and protocols.
Effects of the interventions
Table 2 presents the outcomes of the included studies. Pelle et al. 19 aimed to evaluate the impact of the Dr. Bart application on the frequency of secondary healthcare consultations compared to standard care in individuals with knee/hip OA. Although the application did not result in a reduction in secondary healthcare consultations, it demonstrated minor positive effects on pain, symptoms, and activities of daily living, albeit not clinically significant.
Study characteristics.
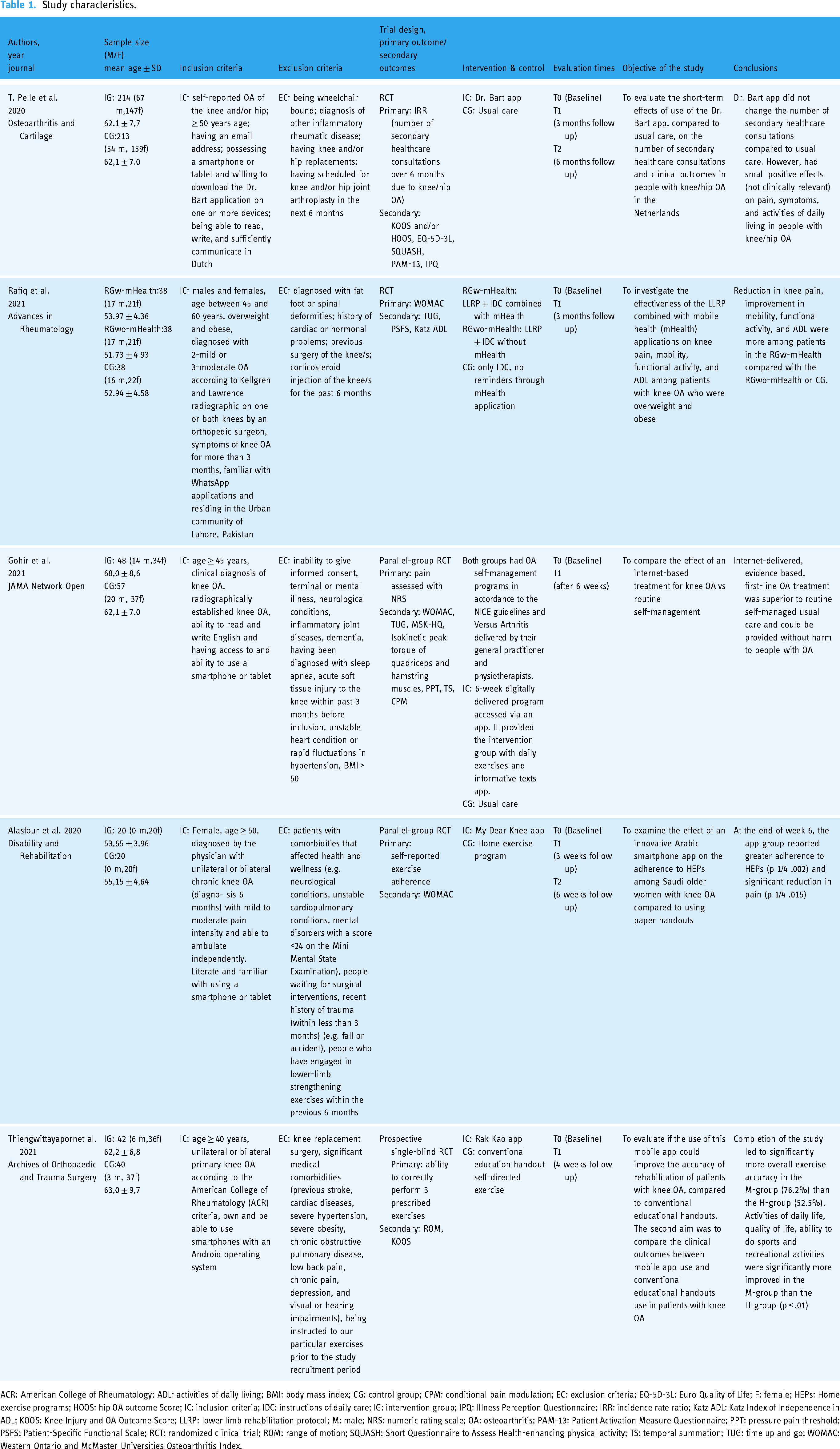
ACR: American College of Rheumatology; ADL: activities of daily living; BMI: body mass index; CG: control group; CPM: conditional pain modulation; EC: exclusion criteria; EQ-5D-3L: Euro Quality of Life; F: female; HEPs: Home exercise programs; HOOS: hip OA outcome Score; IC: inclusion criteria; IDC: instructions of daily care; IG: intervention group; IPQ: Illness Perception Questionnaire; IRR: incidence rate ratio; Katz ADL: Katz Index of Independence in ADL; KOOS: Knee Injury and OA Outcome Score; LLRP: lower limb rehabilitation protocol; M: male; NRS: numeric rating scale; OA: osteoarthritis; PAM-13: Patient Activation Measure Questionnaire; PPT: pressure pain threshold; PSFS: Patient-Specific Functional Scale; RCT: randomized clinical trial; ROM: range of motion; SQUASH: Short Questionnaire to Assess Health-enhancing physical activity; TS: temporal summation; TUG: time up and go; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Study outcomes.

ANPRS: Arabic Numeric Pain Rating Scale; CI: confidence interval; Cont.: control; Int: intervention; KOOS: Knee Injury and OA Outcome Score; NRS: Numeric Rating Scale; SD: standard deviation; TUG: time up and go; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Rafiq et al. 20 investigated the additional benefits of mHealth usage alongside standard care in patients with OA. Their study revealed that patients utilizing mHealth experienced greater reductions in knee pain, improved mobility, and functional activity, as well as enhanced activities of daily living compared to those who did not use mHealth, along with a control group.
Furthermore, Gohir et al. 21 demonstrated the superiority of evidence-based first-line treatment for OA delivered via the Internet over self-administered treatment in the short term. Importantly, this intervention was shown to be safe for individuals with OA.
Alasfour et al. 22 conducted a RCT to assess the impact of the “My Dear Knee” smartphone application on adherence to home-based exercise programs for older women with knee OA in Saudi Arabia. Results showed that the app group had significantly greater adherence to the exercise program and experienced a notable reduction in pain compared to the control group. The study concluded that smartphone applications with motivational features can effectively enhance adherence to home exercise programs among this population.
Thiengwittayaporn et al. 23 developed a mobile application called “Rak Kao” aimed at improving exercise accuracy and quality of life in patients with knee OA. Their RCT compared the app's effectiveness with conventional educational handouts. Results indicated that patients using the app showed significantly better exercise accuracy and improvements in daily activities, quality of life, and recreational activities. Satisfaction with the rehabilitation process was also higher in the mobile app group, suggesting that the app is a superior alternative for delivering exercise guidance and disease education to patients with knee OA.
These findings underscore the potential of digital interventions, including mobile applications and online platforms, as adjunctive tools in managing OA. They provide valuable insights into the effectiveness and safety of various digital health interventions, highlighting their role in improving outcomes and enhancing patient care in OA management.
Quality assessment
All studies included in this systematic review were found to be at high risk of bias. Despite the authors’ diligent efforts to minimize the potential bias effects, all included studies exhibit a high dropout rate (consistently exceeding 5%). This phenomenon results in a high risk of bias across all studies (Figure 2).
Certainty of the evidence
The certainty of evidence following GRADE criteria was very low for both outcomes (pain and recovery of function), as reported in Table 3.
Certainty of evidence.

GRADE: Grading of Recommendation, Assessment, Development, and Evaluation; RCT: randomized controlled trial.
Discussion
This review provides a summary of the available evidence on the effectiveness of mobile technology in managing knee OA. The results indicate that the use of mobile app-based instructions can significantly reduce pain and improve physical function and overall condition among patients with knee OA. Additionally, the intervention group showed improvements in various aspects of quality of life, including fatigue/energy and increased autonomy in activities of daily livings. Notably, no studies suggested the ineffectiveness of mobile apps in enhancing the physical performance of patients with OA. Furthermore, mobile apps provide diverse exercise resources, demonstrating potential benefits in reducing knee pain.
Clinical guidelines highlight that patient education is crucial in the management of knee OA. 2
However, it is important to acknowledge that, despite the evident benefits of mHealth technologies, there are still individuals who do not have access to these technologies.24,25 This issue is not limited to developing countries but also affects certain segments of the population in developed countries, such as older adults or those living in less-served areas.26–28
For these individuals, limited access to mobile technology can present a significant barrier. Therefore, it is essential to adopt an integrated approach that combines digital interventions with traditional options, such as face-to-face education and rehabilitation sessions, to ensure that even those without access to modern technologies can receive adequate support.
It is also important to address the issue of health literacy and the factors influencing the adoption of mHealth technologies among older adults. Although there is growing interest among older adults in using mHealth technologies, healthcare providers often exhibit reluctance to adopt these tools.29,30 This reluctance is influenced by factors such as time constraints and ageist beliefs about the abilities of older adults to use modern technology.30–32 Several studies have highlighted that while older adults are increasingly open to using digital health tools, the adoption by healthcare providers can be hindered by misconceptions and a lack of confidence in these technologies’ effectiveness. 31 For example, some providers may underestimate older patients’ capacity to learn and use these technologies, leading to missed opportunities for integrating mHealth solutions into their care plans. Addressing these barriers through education and training for both healthcare providers and patients is crucial for improving the adoption and effectiveness of mHealth interventions.
Another avenue for improvement lies in enhancing program usability. While a feature may be easily navigable for young adults, it may pose challenges for older individuals due to age-related factors or reduced physical function. 33 However, it is essential to ensure that program usability is enhanced to cater to the target population effectively, including cognitive, physical, and behavioral factors.34–36
This finding highlights that digitally delivered exercise interventions have the potential to enhance the effects of education alone for individuals with knee OA. The choice of exercise delivery, whether it be face-to-face or digital, should be a shared decision between the patient and the clinician. Although the evidence is of low to very low certainty, the review of Fan et al. 18 revealed no clinical advantage for pain, physical function, and QoL outcomes of one mode of delivery over the other.
It is worth noting that OA is not only a condition affecting the elderly but also younger individuals in their working years. 37 In such cases, digitally delivered exercise interventions offer a solution by providing the flexibility to seamlessly integrate into a patient's unique lifestyle circumstances. This adaptability makes digital delivery an attractive option for some patients compared to traditional face-to-face exercise programs. 38
Mobile health technology presents a more accessible and flexible mode of healthcare provision compared to traditional methods. For instance, the widespread use of telephones, being user-friendly and cost-effective, particularly benefits individuals less familiar with modern technologies, such as older adults or those with low information technology literacy. 18 It is essential not to overlook the potential of mHealth applications in this demographic, considering that a significant proportion of older adults now possess smartphones. Therefore, seizing the opportunity to harness mHealth app interventions for older adults is paramount. 39
Overall, the risk of bias was high for all studies. All studies had an RCT design and described random sequence generation, allocation sequence generation, and blinded outcome assessment. All studies were judged at high risk of performance bias as it was not possible to blind participants to a mHealth app intervention. Generally, the study attrition rates were high.
Some factors contribute to heterogeneity. These include variations in comparator groups (active and nonactive), variations in the intervention package, the length of follow up, and variations in the outcome measurements.
The scope of mHealth interventions across the included studies was found to be heterogeneous due to the absence of a detailed definition of mHealth as a medical intervention. To ensure consistency and clarity in the application and evaluation of mHealth interventions, it is imperative to establish a more rigorous delineation of these interventions. This would lead to a better understanding and a more accurate assessment of the impact of mHealth interventions on healthcare outcomes.
Our review shows that mHealth interventions can be as effective as traditional therapies in improving knee OA patients’ pain, and physical function. Although mHealth does not offer significantly greater clinical benefits than standard rehabilitation, it highlights the cost-effectiveness of mHealth solutions, which can achieve similar outcomes without constant medical supervision. It is important to continue incorporating cost-effectiveness analyses into future study evaluations and recognize mHealth's potential as a valuable tool in treating knee OA.
Conclusion
Mobile applications offer a potentially effective means of supporting therapeutic exercise and improving pain management and functionality in patients with knee OA. However, the findings of this systematic review should be interpreted cautiously. While the included studies suggest potential benefits of mobile apps in alleviating symptoms and enhancing quality of life, all studies exhibited a high risk of bias, and the overall certainty of the evidence was low to very low.
The limited number of studies and the heterogeneity of interventions and outcome measures reduce the ability to draw definitive conclusions regarding the effectiveness of mobile apps compared to traditional rehabilitation methods. Therefore, it is premature to assert that mobile apps can replace or surpass conventional therapies for knee OA management.
Further high-quality research, including larger and better-designed trials, is necessary to confirm the efficacy of these technologies. In the meantime, mobile apps may be considered as a supplementary option for some patients, particularly those with limited access to traditional care, but should not be regarded as a definitive solution.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241297296 - Supplemental material for Exploring ways to improve knee osteoarthritis care: The role of mobile apps in enhancing therapeutic exercise—a systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241297296 for Exploring ways to improve knee osteoarthritis care: The role of mobile apps in enhancing therapeutic exercise—a systematic review by Teresa Paolucci, Letizia Pezzi, Federica Bressi, Raffaele La Russa, Bruno Beomonte Zobel, Gianluca Bertoni, Giacomo Farì and Andrea Bernetti in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241297296 - Supplemental material for Exploring ways to improve knee osteoarthritis care: The role of mobile apps in enhancing therapeutic exercise—a systematic review
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241297296 for Exploring ways to improve knee osteoarthritis care: The role of mobile apps in enhancing therapeutic exercise—a systematic review by Teresa Paolucci, Letizia Pezzi, Federica Bressi, Raffaele La Russa, Bruno Beomonte Zobel, Gianluca Bertoni, Giacomo Farì and Andrea Bernetti in DIGITAL HEALTH
Footnotes
Contributorship
TP, AB, FB, and RLR were involved in study conceptualization; LP and GB in data collection, analysis and interpretation of results data curation, investigation and methodology, and draft manuscript preparation; and TP, FB, GF, BBZ, and AB in editing of the manuscript. All authors revised it critically for intellectual content and have approved the final version of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is a part of Grant PRIN, number 2022CCFXEX—titled “SyDiDOa—Symptomatic Digital Drugs for Osteoarthritis”.
Guarantor
LP.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.