
Abstract
Background
To facilitate disease management, understanding the attitude of healthcare professionals regarding the use of this tool can help mobile health (mHealth) program developers develop appropriate interventions.
Aims
To assess the perspective of healthcare professionals regarding the contribution of mobile-based interventions in the prevention, diagnosis, self-care, and treatment (PDST) of COVID-19.
Methods
This is a survey study conducted in 2020 in Iran with 81 questions. In this study mHealth functionalities were categorized into four dimensions including innovative, monitoring and screening, remote services, and education and decision-making. The data were analyzed using descriptive statistics, ANOVA, and the Kruskal–Wallis test to compare the attitudes of the different job groups.
Results
In total, 123 providers participated, and 87.4% of them reported that mHealth technology is moderate to most helpful for the management of COVID-19. Healthcare professionals believed that mHealth technology could be most helpful in self-care and least helpful in the diagnosis of COVID-19. Regarding the functionalities of the mobile application, the results showed that the use of patient decision aids can be most helpful in self-care and the use of computer games can be least helpful in treatment. The participants believed that mHealth is more effective in monitoring and screening dimensions and less effective in providing remote services.
Conclusions
This study showed that healthcare professionals believed that mHealth technology could have a better contribution to self-care for patients with COVID-19. Therefore, it is better to plan and invest more in the field of self-care to help patients to combat COVID-19. The results of this study revealed which mhealth functionalities work better in four domains of prevention, treatment, self-care, and diagnosis of COVID-19. This can help healthcare authorities to implement appropriate IT-based interventions to combat COVID-19.
Introduction
COVID-19, which can cause serious respiratory illnesses such as pneumonia and lung failure, was first reported in Wuhan, China in December 2019. 1 This disease spreads fast throughout China and other parts of the world.2,3 COVID-19 is somewhat similar to severe acute respiratory syndrome (SARS-CoV) in pathogenicity, clinical status, and epidemiology. 4 Fever, cough, shortness of breath, pneumonia, and fatigue are the common symptoms of this disease.5–9 On February 11, 2020, the World Health Organization (WHO) named this disease COVID-19. 3 Currently, no effective antiviral treatment is available, and due to its high prevalence and mortality, the WHO announced that this disease is an international public health concern.10,11 Until August 9, 2021, more than 204 million people have been infected, and more than 4 million deaths have been confirmed by WHO. 12 In Iran, until May 6, 2021, more than 2.5 million people have been infected, and more than 74,000 deaths have been confirmed. 13
Due to the epidemic of this disease and the importance of social distancing, information and communications technology (ICT) has become more important in improving public awareness and prevention, monitoring, diagnosis, and treatment of this disease. Various ICT-based methods have been used around the world to combat this disease. A review study by Zaman et al. found that ICT interventions such as websites and dashboards, mobile apps, robots and drones, artificial intelligence and machine learning, data analytics, wearable technologies or sensors, social media, and interactive voice response had primarily been used to combat the outbreak of COVID-19 and to provide medical services in this vulnerable period. 14
The samples of the activities done using ICT interventions include sensors embedded in smartphones for disease prediction, 15 vital sign monitoring and remote care coordination, 16 remote patient counseling and screening, 17 and the use of geographic information system to determine how the virus spreads and spatial modeling of its incidence.18,19 Moreover, some studies have used artificial intelligence and machine learning techniques for medical image processing to diagnose COVID-19.20–23
Various studies have shown the views of healthcare professionals regarding the use of mobile health (mHealth) for the management of diseases such as asthma, 24 COPD, 25 malaria, 26 tuberculosis, and HIV. 27 Such studies have been also done regarding burn injury counseling 28 and providing appropriate services to pregnant mothers. 29 The results of these studies showed that despite some problems such as low health literacy among individuals and lack of accessibility to smartphones for some individuals, this technology is useful and acceptable for disease prevention, control, and self-management.
During the COVID-19 pandemic, Miner et al. in his study assessed physicians’ views on the use of telemedicine and showed that physicians who were more flexible and understood the value of technology were more inclined to use this technology. 30 A study by Park et al. in Korea assessed the satisfaction of patients and healthcare professionals with the use of telephones for counseling and prescription during the COVID-19 epidemic. The results of his study showed that physicians and nurses were less satisfied than patients. Patients’ higher satisfaction with telemedicine might be associated with the emergent situation due to COVID-19. Patients’ great appreciation and satisfaction were due to improved efficiency and cost-effectiveness without the risk of direct person-to-person transmission. In Korea, negative views on the safety and inconveniences of using technology have led to dissatisfaction among health providers (doctors and nurses). 31
One of the goals of using technology during a global epidemic is to reduce the risk of transmission to healthcare professionals. Using technology has the potential to reduce transmission by minimizing face-to-face contact between physicians and patients. 32 On the other hand, one of the important factors in the acceptance of technology by physicians is the understanding of the usefulness of that technology. 33
Therefore, by assessing the views of healthcare professionals and evaluating the readiness of healthcare professionals to use mHealth technology in Iran and other countries,34–37 it is possible to identify important and practical areas that mHealth technology can be used in the COVID-19 crisis. Considering providers’ views could increase the acceptance of the technology among healthcare professionals and take advantage of the potential effects of technology on COVID-19 diseases.
Given the availability of smartphones and the importance of using technology in the prevention, diagnosis, self-care, and treatment (PDST) of COVID-19, to facilitate disease management, understanding the attitudes of healthcare professionals regarding the use of this technology can help mHealth developers to design appropriate interventions. Various studies applied IT-based interventions to combat COVID-19, but the question is what healthcare professionals actually need and expect to respond to IT-based interventions. Therefore, in this study, it is tried to identify mHealth interventions and their functional capabilities that can help providers in the PDST of COVID-19 from the perspectives of healthcare professionals.
Although various mHealth interventions can be developed to manage COVID-19 due to limited resources and also to increase the acceptance of technology among healthcare professionals, assessing the views of healthcare professionals can make planning in this direction more effective.
mHealth services of Iran Ministry of Health
The Ministry of Health and Medical Education of Iran combat the COVID-19 pandemic through public media and the use of communication systems such as call centers 4030 and 190, screening using various systems and sending educational text messages on the prevention of new coronavirus, launched a website and shared information and guidelines related to COVID-19 disease.
According to published studies, the number of Iranian mobile phone users is over 53 million 38 and 69% of them have a smartphone. 39 Therefore, due to a large number of mobile users and the extension of Iran, a number of health services can be provided through mobile.
Methods
Design and sample size
This is a survey study conducted in 2020 in Iran. The study population included all healthcare professionals including physicians, nurses, allied medicines (including radiology experts, laboratory experts, operating room personnel, etc.), and personnel with indirect contact with patients (including personnel working at admission discharge, IT departments, etc.). Those providers who were members of social networks such as WhatsApp and LinkedIn were included in this study. The sample size was calculated based on the sample size estimation formula and the results of previous studies which measure the ratio,40,41 in which, the ratio of knowledge concerning mHealth technology was around 60%. With a power level of 1 – β = .70 and a significance level of α = .05, the sample size was estimated with 100 participants. In order to increase the precision of the study, 20% was added to the estimated sample size.
Study instrument
The data collection instrument in this study was a questionnaire developed by researchers in which some questions were taken from other studies in the field of mHealth interventions.42–50 General questions regarding the application of mHealth were extracted from other studies and in consultation with the research team, these questions were generalized to the four domains of the study. A consensus method was used to adjust the structure of the questionnaire and develop questions that were relevant to the aim of this study. 51 To complete the questionnaire, we were looking for people who work in the healthcare system, so our sampling was purposeful. Therefore, we distributed the questionnaire in social networks whose users are working in the healthcare system.
In order to collect data, an electronic version of the questionnaire was developed by porsline Web-based survey instrument and the URL link of this online questionnaire was distributed to participants through three social networks; WhatsApp, Telegram and LinkedIn. Data collection was continued until reaching the desired sample size, which long about 3 months.
The face validity of the questionnaire was confirmed by five medical informatics specialists. Face validity is the appropriateness, sensibility, or relevance of the test and its items as they appear to the persons answering the test. 52 The questionnaire was sent to these specialists through E-mail. They had some comments that were resolved through discussion and the final version of the questionnaire was approved by researcher consensus. Cronbach’s alpha coefficient was used to evaluate the reliability of the questionnaire (α = .96). This questionnaire consisted of six sections with 81 questions. The first section included demographic information of the participants with five questions, the second section included questions regarding familiarity with mHealth technology, the third to sixth sections contained questions regarding the identification of mHealth functionalities and the extent of their contribution in the prevention (19 questions), diagnosis (18 questions), treatment (22 questions), and self-care (16 questions) of COVID-19. The meaning of prevention in this study is the measures and training needed to prevent the disease, diagnosis is the process of determining the disease, self-care is actions patients take to manage the disease, and treatment is steps taken to deal with the disease by providers.
The questions of the third to the sixth sections were in the form of a 5-point Likert scale. These options ranged from very high to very low. The answer to each question was scored from 5 (strongly agree) to 1 (strongly disagree) in this questionnaire. To reduce the possible ambiguity regarding the questions a short explanation is provided in parentheses in front of questions that might be ambiguous. Based on the minimum and maximum attainable mean scores in this questionnaire (2.26 and 4.72), we classified the overall perspective of the participants on mHealth technology into three categories: least helpful (2.26–3.08), moderately helpful (3.09–3.9), and most helpful (3.91–4.27).
In this study, the mHealth functionalities and capabilities were categorized into four dimensions including Innovative functionalities (such as image processing and wearable devices), monitoring and screening (such as monitoring of patients within/out of and triage application), remote services (such as tele-visit and tele-consultation), and education and decision-making (such as educational health nutrition programs and decision support systems for the general public) in a bottom-up method by agreement. By using this approach, the questions with similar features were categorized into a category. The categorization was continued till no more questions and no overlap category remained.
Statistical analysis
Data were analyzed by IBM SPSS Statistics version 24 (IBM Inc., Armonk, NY, USA). In order to analyze the data descriptively frequency, mean median, IQR, and standard deviation were used. Kolmogorov–Smirnov test was used to measure the normality of the data distribution. ANOVA test (normal distributions) and Kruskal–Wallis test (non-normal distributions) were used to compare the average responses of different job groups regarding the extent by which mHealth technology can be helpful concerning PDST and also to compare the average responses of different job groups regarding mHealth functionalities in four dimensions of Innovative functionalities, monitoring and screening, remote services and education and decision-making.
We used linear regression for examining the relationship between independent variables (gender, education, job, age, and the level of mHealth familiarity) and response variables (the role of mHealth in PDST). Gender, education and job were nominal and age was ordinal.
Ethical considerations
This research was approved by the research ethics committee of Kerman University of Medical Sciences with ethics code IR.KMU.REC.1399.247. Before completing the questionnaire, in order to comply with ethical rules, the research objectives were explained to the participants in the first part of the questionnaire and informed. Written consent was obtained from the participants at the beginning of the questionnaire. After completing the informed consent form, the participants had access to the questionnaire questions and could complete the research questionnaire.
Results
A total of 123 questionnaires were completed, of which three were not included in the study due to incomplete information. According to Table 1, among the participants, 60% (n = 67) were women. About half of the participants in this study (n = 48, 49.2%) were under 30 years old, and only 4% (n = 5) of the participants aged over 50 years old. More than 44% of the participants had bachelor's degrees (n = 51). The occupation of 44% of the participants (n = 52) in this study was nurse. More than 73% of the participants (n = 76) reported their level of familiarity with mHealth technology as moderate and higher. Among the participants with age under 30 years old 70% also reported their familiarities with mHealth technology as moderate and higher. Only 11% (n = 13) of the participants had no familiarity with health technology.
Demographic information of the participants.

In total, 37% (n = 44) of the participants reported that mHealth is very helpful, and 12.6% (n = 15) stated that it is the least helpful for managing COVID-19. 87.4% of participants believed that mHealth technology is moderate to most beneficial. The results of ANOVA test showed that the level of familiarity of the healthcare professionals with mHealth technology had no effect on the providers’ attitudes towards the role of mHealth technology in prevention (P = .67), treatment (P = .26), self-care (P = .67) and diagnosis (P = .058) of COVID-19. The results of ANOVA test also showed that the level of familiarity of the healthcare professionals with mHealth technology had no effect on the providers’ attitude towards the mHealth functionalities (remote services (P = .93), innovation functionalities (P = .22), monitoring and screening (P = .91), education and decision (P = .92)).
The results of Kolmogorov–Smirnov test to measure the normality of the data distribution showed that the attitudes of the healthcare professionals regarding the role of mHealth in prevention (P = .08) treatment (P = .20) and diagnosis (P = .20) have a normal distribution and regarding the self-care (P = .01) has an non-normal distribution.
The mean scores of the responses of the providers regarding their attitudes towards the role of mHealth in four domains of PDST showed that the highest score was assigned to the role of mHealth in self-care (mean = 3.96, SD = 0.51). The next scores assigned to prevention (mean = 3.88, SD = 0.48), treatment (mean = 3.58, SD = 0.63) and diagnosis (mean = 3.57, SD = 0.60), respectively.
The results of this study regarding the role of mHealth functionalities in the PDST of COVID-19 showed that the lowest score was assigned to COVID-19 treatment using computer games (providing indirect training) (mean = 3.06, SD = 1.067) and the highest score was assigned to the self-care using the patient decision aids (providing reminders about timely use of medication, hand washing, etc.) (mean = 4.17, SD = 0.7) (Figure 1).

Mean scores given by the participants to mHealth functionalities in terms of different health domains.
The results of ANOVA in Table 2 show a significant difference between the scores that various groups of the providers assigned to the three domains of treatment, diagnosis and prevention. This means that there is a significant correlation between the participants’ jobs and their attitudes towards the use of mHealth technology in these three domains. Nurses compared to other job groups gave higher scores to the role of mHealth technology in the prevention, treatment, and diagnosis of COVID-19, but physicians assigned lower scores to the role of mHealth in these domains
Comparison of the participants’ scores assigned to the role of mHealth technology in the four domains of prevention, treatment, self-care and diagnosis.

The results of Kruskal–Wallis tests in Table 2 show that there is no significant difference between the attitudes of the providers in the field of self-care. All of the healthcare professionals believed that the role of mHealth technology in self-care was greater than in other domains.
Figure 2 shows the mean and standard deviation scores that participants gave to mHealth functionalities categorized into the four dimensions of innovative functionalities, monitoring and screening, remote services, education, and decision-making to assist PDST. The highest score was assigned to the functionalities of the monitoring and screening category and the lowest score to the functionalities of the remote services category.
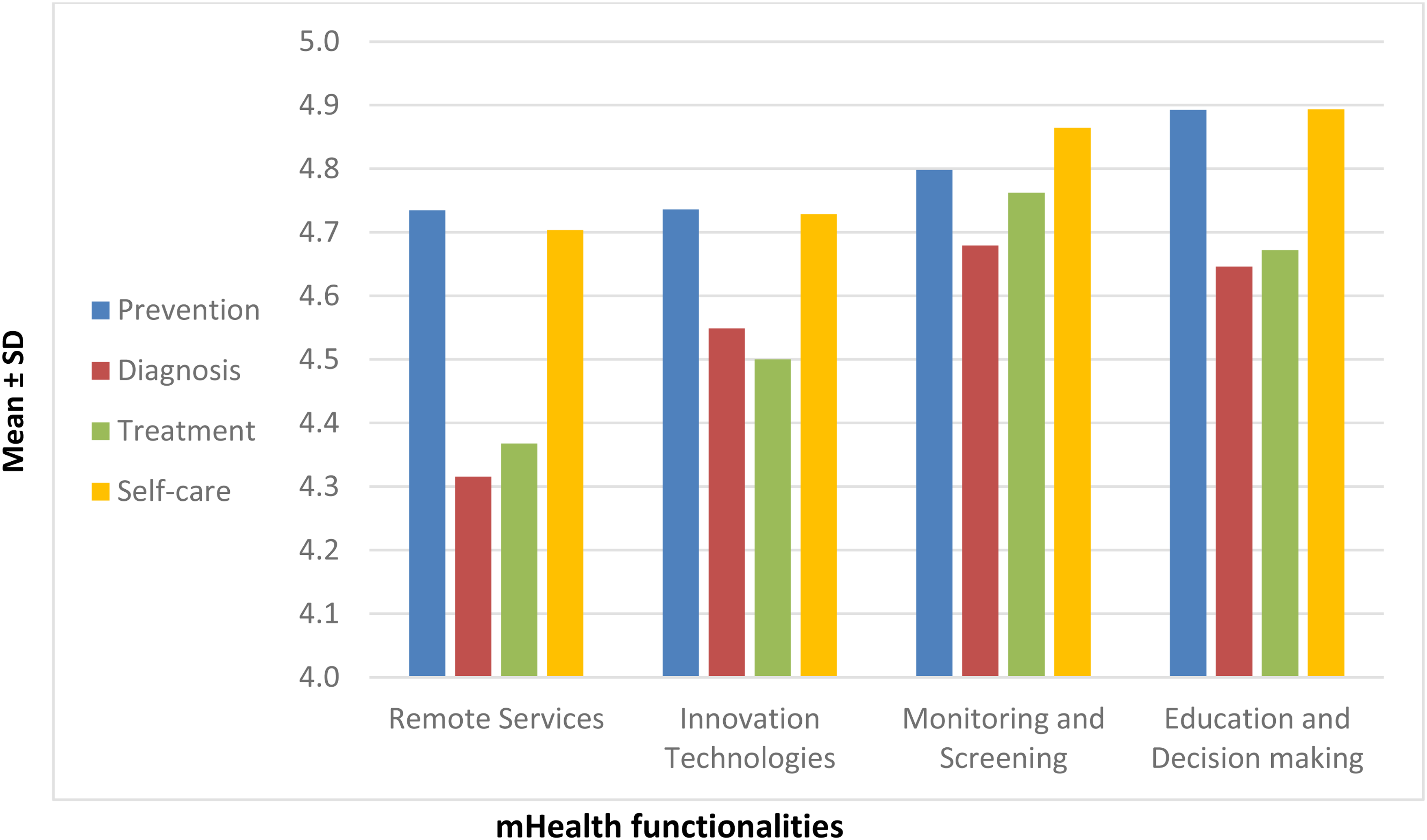
Mean and standard deviation of scores given by the participants to mHealth functionalities.
According to Table 3, the results of ANOVA test showed that there were significant differences between the scores assigned by the four groups of the participants to the remote services (P = .007), innovative functionalities (P = .02) and monitoring and screening (P = .03) functionalities. There was no significant difference between the scores assigned by the participants to functionalities related to education and decision-making (P = .36).
Comparing the scores assigned by four groups of the participants to four dimensions of mHealth functionalities

Overall, according to the results of this table, nurses compared to other participants had positive attitudes towards the functionalities such as innovative functionalities, monitoring and screening, and remote services.
The following five variables were entered into the linear regression model: gender, education, age, job, and familiarity with mHealth. Of these variables, only job remained a significant independent variable. Gender (P = .53), education (P = .41), age (P = .20), and familiarity with mHealth (P = .13) did not affect the providers’ attitudes towards the role of mHealth technology in prevention, treatment, self-care, and diagnosis of COVID-19.
Discussion
The results of this study showed that most healthcare professionals believed that mHealth technology could contribute to the prevention and self-care of COVID-19. But in the field of self-care, it could be can be more effective. Nurses reported after self-care, the highest contribution of mHealth technology was in the monitoring and screening of community members. Also, they further believed that the use of mHealth technology could be helpful in the prevention, treatment, and diagnosis of COVID-19. However, physicians reported lower agreement regarding the role of mHealth technology compared to other healthcare professionals. Moreover, the present study also showed that the use of mHealth in education during the disease epidemic can be helpful.
One study in Iran showed that mHealth technology was effective in prevention. 53 This was due to the low rate of disease prevention in Iran.54,55 In consistence with the results of our study, Parizad et al. 56 in their study showed that using mHealth had important effects on promoting self-care activities among patients with type 2 diabetes in Iran. Also, another study showed that more than 93% of the patients with chronic diseases preferred to use mHealth services. 50 Garabedian et al., 57 in their study, showed the use of mHealth technology increased self-care in patients with diabetes and thus improved their disease (improved HbA1c).
A study by Alwashmi 32 has shown that digital technologies provide a unique opportunity to enhance the diagnosis and management of infectious diseases and can be used in the management of various stages of COVID-19 disease, including monitoring and screening. Ting et al., 58 in their study, also stated that digital technologies can be used to monitor, diagnose and prevent COVID-19. Moazzami et al. 59 also concluded that the use of telemedicine allows physicians to screen patients with early signs of COVID-19 before referral to hospitals.
Taylor et al. 60 also, in a study conducted on the nursing community, stated that having reliable and flexible technology and allocating sufficient resources for providing remote health services, delivering proper staff training, and developing a participatory intervention can help to overcome the initial barriers of technology acceptance and provide essential remote monitoring. Judson et al., 61 in their study, concluded that patient self-assessment instruments integrated with the electronic health record system have the potential to greatly improve triage efficiency and avoid unnecessary referrals during the COVID-19 pandemic.
Arneson et al. 62 showed in her study that the nurses’ attitude towards using Tele-ICU in the treatment process of COVID-19 patients was positive, and this technology helped less experienced nurses could benefit from this technology when working in the ICU and overcome the challenges of low human resources. A study done by Weissman et al. 63 showed that the use of mHealth technology had improved eating disorders in patients with COVID-19, so the use of this technology can replace hospitalization in some cases. In another study done by Vidal-Alaball et al., 64 it is concluded that the use of telemedicine in the face of COVID-19 has many benefits, including remote evaluation of laboratory results, a shorter waiting list for specialists, and monitoring patients at their homes.
The reason for less agreement among doctors regarding the role of mHealth technology in Iran could be the way physicians are paid in the reimbursement system in Iran. Physicians in Iran receive money for each patient service, and the more services a physician provides, the higher the income. 65 Therefore, physicians may believe that mHealth technology will affect their reimbursement. Moreover, physicians may also be concerned that the use of mHealth technology in diagnosing the disease will replace them. 66
Another reason for this result is that healthcare practitioners seek to achieve maximum efficiency, save money, ensure the highest quality and avoid mistakes simultaneously. 67 Therefore, rely less on technology in cases such as diagnosis and treatment. One factor that makes for a better experience is the proper design of the systems. Studies have shown that mobile applications have beneficial effects on managing chronic diseases, reducing mortality and hospitalization, 68 and reducing medication errors. 69 Proper and principled design reduces design-based errors and improves the quality and safety of systems. 70 However, errors in design can endanger patient safety.71,72
The results of our study also showed that there is a significant correlation between the participants’ jobs and their attitudes toward the use of mHealth technology in the prevention, treatment, and diagnosis of COVID-19. The demographic information of the participants had no effect on their attitudes toward the use of mHealth technology in the prevention, treatment, and diagnosis of COVID-19.
In a study conducted by Gallagher et al., 73 age and education were important influences on technology use. Younger and more educated patients were more likely to use mobile technology and to do so for health reasons, as well as to use apps, especially, if they were employed. Tadayon et al., 74 in their study, reported a reverse relation between the age of the participating physicians and their willingness to use mHealth technology. Younger physicians were more willing to use mHealth technology. The results of Hoque and Sorwar’s study 75 showed matters such as performance expectancy, effort expectancy, social influence, facilitating conditions, technology anxiety, and resistance to change had a significant impact on the acceptance of mHealth technology.
Various studies76,77 have shown that people accept technology if they are sure that the technology has a positive effect on their performance and the type of job has an impact on the acceptance of the technology. Due to the fact that using smartphones has become popular among different ages and genders and the vast penetration of this technology, the demographic information of the participants had no effect on their attitudes toward the use of mHealth technology.
The results of this study showed that most healthcare professionals were familiar with mHealth technology, and they use it for getting information and for education. The result of our study also showed that the use of mHealth in education during the disease epidemic can be helpful. Zamberg et al. 78 described the use of mHealth as an effective communication channel for disseminating coronavirus-related information to all hospital medical staff, which can also save time for sharing the information. Hussein, in his study, showed that physicians use mobile phone interventions more than other IT-based interventions, which can be attributed to their availability and ease of use in any place and time. Moreover, they use more social networks such as Facebook and WhatsApp to obtain information about COVID-19 and share this information.79,80 Nevertheless, Zarocostas and Li H.O. in their studies,81,82 showed that not all the information that providers receive from social networks is necessarily accurate.
Although different researchers may propose and implement various IT-based interventions from the perspective of healthcare professionals, some of them could contribute in disease management. Our study identified that from the perspective of healthcare professionals in which domains and which interventions, mHealth can be effective. This makes the investment more effective and can help to implement appropriate intervention to combat COVID-19. Considering the limited resources of health services in Iran, if we know which IT-based intervention is effective, it can help us to save resources. Moreover, by identifying helpful interventions, it is possible to make the training of healthcare professionals conditional on these interventions and save financial resources in the field of health.
Although the power level in this study was not high enough, the differences were so great that even with this power, the differences were detectable and the results became meaningful.
Limitations
We had five limitations in this study. First, data collection was done through an online questionnaire, so this may result to miss the attitudes of professionals who do not prefer to complete the online questionnaires. The questionnaire was distributed through online social media and we could not evaluate whether respondents were comfortable with the parameters and/or terms and conditions of the questionnaire itself. Second, a low number of physicians participated in this study, thus it is suggested that further studies be conducted with a greater sample size. Third, the issue of readiness to use mHealth technology was not included in this study. However, there are other studies that had addressed the readiness of healthcare professionals to use mHealth technology.34–37 Fourth, We only evaluated the face validity of the questionnaire and did not calculate validity indicest. Fifth, the questionnaire was completely structured and no open-ended questions were considered. To gain a complete insight into the attitude and desires of healthcare professionals, in future studies, it is suggested to perform qualitative studies so in-depth interviews.
Conclusion
This study showed that healthcare professionals believed that mHealth technology could be most helpful in self-care. Therefore, it is better to plan and invest, more in the field of self-care to better manage the COVID-19 disease. According to the attitudes of the healthcare professionals, applying decision aid to help patients regarding their self-care can help them to have better control over the disease. According to the positive attitudes of healthcare professionals toward the use of mHealth technology in the prevention, treatment, self-care, and diagnosis of COVID-19, healthcare authorities can implement appropriate interventions to combat COVID-19.
Since this technology can help improve and manage the health status of patients, healthcare professionals should be aware of the benefits of this technology in monitoring and managing the COVID-19 disease and make benefit of its capacity on a large scale to manage and control the disease. Health policymakers and planners also need to develop rules and regulations to address legal and ethical barriers to the use of this technology to manage the health crisis.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231171969 - Supplemental material for The role of mobile health in prevention, diagnosis, treatment and self-care of COVID-19 from the healthcare professionals’ perspectives
Supplemental material, sj-docx-1-dhj-10.1177_20552076231171969 for The role of mobile health in prevention, diagnosis, treatment and self-care of COVID-19 from the healthcare professionals’ perspectives by Mahdieh Montazeri, Zahra Galavi and Leila Ahmadian in DIGITAL HEALTH
Footnotes
Contributorship
MM and ZG were the major contributors in writing the manuscript. LA was the research supervisor and final editor. All authors agreed on the design of the study and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethical committee of the Kerman University of Medical Sciences (Code: IR.KMU.REC.1399.247).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Mahdieh Montazeri.
Informed Consent
All participants gave written informed consent. All procedures performed in the present study were in accordance with the ethical standards of the institutional and national research committee of the Kerman University of Medical Sciences and the 1964 Helsinki declaration and its further updates.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.