
Abstract
Objective
Anxiety is prevalent in childhood but often remains undiagnosed due to its physical manifestations and significant comorbidity. Despite the availability of effective treatments, including medication and psychotherapy, research indicates that physicians struggle to identify childhood anxiety, particularly in complex and challenging cases. This study aims to explore the potential effectiveness of artificial intelligence (AI) language models in diagnosing childhood anxiety compared to general practitioners (GPs).
Methods
During February 2024, we evaluated the ability of several large language models (LLMs; ChatGPT-3.5 and ChatGPT-4, Claude.AI, Gemini) to identify cases childhood anxiety disorder, compared with reports of GPs.
Results
AI tools exhibited significantly higher rates of identifying anxiety than GPs. Each AI tool accurately identified anxiety in at least one case: Claude.AI and Gemini identified at least four cases, ChatGPT-3 identified three cases, and ChatGPT-4 identified one or two cases. Additionally, 40% of GPs preferred to manage the cases within their practice, often with the help of a practice nurse, whereas AI tools generally recommended referral to specialized mental or somatic health services.
Conclusion
Preliminary findings indicate that LLMs, specifically Claude.AI and Gemini, exhibit notable diagnostic capabilities in identifying child anxiety, demonstrating a comparative advantage over GPs.
Introduction
Among the rapid advancements in the domain of artificial intelligence (AI) is the emergence of large language models (LLMs), such as Bard by Google, Claude.AI 2 by Anthropic, and ChatGPT versions 3.5 and 4 by OpenAI. LLMs have demonstrated significant potential within the realm of mental healthcare.1–4 These technological innovations have the potential to transform the mental healthcare landscape by expediting research processes, augmenting clinical practice by providing valuable assistance to healthcare professionals, and extending support mechanisms to patients.5,6 Nevertheless, the efficacy and practicality of directly employing LLMs to enhance mental health outcomes, particularly in the case of anxiety disorders (ADs), warrant further investigation. This study evaluates the ability of advanced AI models, specifically LLMs, to diagnose childhood anxiety in complex cases or those with comorbidities, compared to general practitioners (GPs) and mental health experts. It is noteworthy as one of the first studies to focus on the mental health of children, particularly in the area of childhood anxiety, using AI technology, addressing the significant gap in research in this field.
Undiagnosed ADs have a profound impact on human development and well-being.7,8 With prevalence rates as high as 25%. ADs represent the most widespread mental health challenge across the lifespan. 9 Indeed, only about 10% of children with ADs, including those exhibiting subthreshold severity, are expected to be free of any mental health issues in adulthood.10,11 The effectiveness of treatment in mitigating the risks and adversities associated with ADs is well-established.12,13 Given the pivotal role and accessibility of GPs and their ongoing relationships with families, they are uniquely positioned to identify ADs, which are often characterized by early onset, a chronic or episodic course, physical manifestations, and comorbidities.14,15
The challenge of detection is compounded in cases of early onset, lower severity, and less overt manifestations. 16 This difficulty is inherent to the nature of anxiety itself, which is characterized by concealment of core symptoms, a gradual and fluctuating course, and a wide array of accompanying symptoms that are not typically associated with anxiety. 17 These symptoms, which range from temper tantrums and a need for control to social withdrawal, interpersonal difficulties, concentration problems, and somatic complaints, may not be immediately recognized as interconnected or indicative of an underlying AD.18,19 Detection is further complicated by the overlap of these symptoms with other mental health disorders. 20 The constrained timeframe of GP consultations necessitates swift and accurate interpretation of presented problems, making the initial diagnostic impression critical for effective identification of anxiety in children. 21 Despite the widespread prevalence of ADs, GPs already seem to overlook anxiety in their early diagnostic opinion.22,23
This study examined the following research questions:
How do various AI tools (ChatGPT-3, ChatGPT-4, Claude.AI, and Gemini) compare to human professionals (MHPs and GPs) in accurately recognizing anxiety, as measured by their performance in total recognition, first identification, and second identification questions?
How often do various AI tools (ChatGPT-3, ChatGPT-4, Claude.AI, and Gemini) identify anxiety compared to human professionals (MHPs and GPs)?
What is the ideal placement for a child diagnosed with anxiety disorder according to the various AI tools (ChatGPT-3, ChatGPT-4, Claude.AI, and Gemini) compared to human professionals (MHPs and GPs)?
How do treatment recommendations for mental and behavioral disorders differ between AI tools and GPs?
Method
AI procedure
The findings were collected during February 2024. The transfer of the vignettes took one month and was conducted using the interfaces of the language models ChatGPT, Claude, and Gemini to identify childhood ADs. These evaluations were compared with the results reported by Dutch mental health professionals (MHPs) and GPs as described by Aydin et al. 23
Input source: vignettes
To investigate the extent to which LLMs are sensitive to ADs in children, we utilized a series of clinical vignettes developed by Aydin et al. 23 These vignettes were designed to depict the varied symptom presentations commonly seen in pediatric ADs. The original researchers constructed the vignettes to portray a probable underlying AD, while also including symptoms that overlap with other common mental health issues. The vignette development process employed by Aydin et al. 23 began with a review of clinical handbooks and questionnaires to identify relevant symptoms and characteristics. The researchers also analyzed actual referral letters written by GPs for children who were later diagnosed with ADs. These letters provided natural language descriptions of presenting complaints and enabled the researchers to map the correspondence between GPs’ stated reasons for referral and the eventual diagnoses. According to Aydin's 23 research, the sample of GPs had varying levels of experience, with 54.1% having over 20 years of practice, indicating a predominantly highly experienced group.
The researchers categorized the extracted descriptions into five domains of symptoms that commonly co-occur with anxiety: somatic complaints, difficult behaviors, depressed mood, developmental problems, and school attendance issues. They then developed vignettes representing each domain. Each vignette depicted a 10- to 12-year-old child with anxiety symptoms as well as attributes suggesting other potential problems. Contextual details were included to enhance realism. The original authors undertook an iterative process of drafting, review, and refinement, in consultation with MHPs and GPs. The vignettes were adjusted to achieve a consistent length of 165 to 172 words each. Audio recordings of the vignettes were created, with the text also included as subtitles, to replicate the verbal nature of clinical encounters while ensuring consistent presentation to participants. This multistep process resulted in a final set of five vignettes, each centered around one key problem area while incorporating a greater number of anxiety cues than other mental health symptoms. The vignettes aimed at authentically capturing the ambiguity of real-world clinical presentations in general practice. The vignettes are described in Appendix 1.
Measures
The LLMs were asked to respond to a series of questions designed to assess their interpretation of the presenting problems and their decision-making with respect to patient referral and management. The survey items were divided into two main sections:
Typical development (Option one if it is probably an example of typical development)
Behavioral problems (Option two for difficult behavior: examples include aggressive behavior or antisocial behavior)
Complaints regarding establishing contact (If problems likely indicate an autism spectrum disorder, you can choose option three)
Mood problems (Mood problems and problems that could be related to depressive disorders)
Somatic complaints (For physical symptoms choose option five, also if a problem might be psychosomatic in nature)
Eating problems (Option six for eating problems and probable eating disorders)
Anxiety-related complaints (Option seven for problems related to anxiety and anxiety disorders)
Complaints regarding attention and activity (Option eight for attention-related complaints that might indicate attention deficit hyperactivity disorder or attention deficit disorder)
Complaints related to experience of a traumatic event (Option nine for problems related to experience of a traumatic event). What profile would you ascribe this vignette?
No second complaint group (Please choose option 10 if you do not see another complaint.)
Nurse practitioner
Local youth teams
Generalized mental healthcare
Specialized mental healthcare
Somatic healthcare/hospital
Where do you think that children with this type of complaint can best be helped? (The eight mental health groups are shown. For each group, please indicate how you would tend to refer children when you suspect these complaints.)
Answer questions B1–B8 by indicating the number of the option you would choose for each question among the options provided.
B1–B8. Where do you think children with (B1) Behavioral problems/(B2) Complaints regarding establishing contact/(B3) Mood problems/(B4) Somatic complaints/(B5) Eating problems/(B6) Anxiety-related complaints/(B7) Attention and activity/(B8) Complaints related to experiencing a traumatic event can best be helped?
Watchful waiting
Nurse practitioner
Local youth teams
General mental healthcare
Specialized mental healthcare.
Testing the large language models
Each of the five vignettes and the three questions (A1–A3) were input ten times into each of the four AI language models: Claude, ChatGPT 3.5, ChatGPT 4, and Gemini. Each of the ten measurements was conducted in a new tab to avoid the influence of previous information. Questions B1–B8 were asked ten times together in the same tab, with each of the ten measurements conducted in a new tab. Table 1 describes the number of iterations for the different vignettes and questions.
Number of iterations for the different vignettes and questions.

Statistical analysis
The statistical methodology used in this study was designed to provide a rigorous assessment of the effectiveness of various AI tools and human professionals in recognizing anxiety. We calculated three types of recognition rates for anxiety: (1) First Recognition Rate: The percentage of cases where anxiety was identified as the primary concern. (2) Second Recognition Rate: The percentage of cases where anxiety was identified as a secondary concern. (3) Total Recognition Rate: The percentage of cases where anxiety was identified in either the first or second instance. This rate represents the overall ability to recognize anxiety, regardless of whether it was identified as the primary or secondary concern. The first RQ was examined using Chi-squared test of independence to assess whether the differences in total recognition, first identification, and second identification rates across these entities were statistically significant. Due to the multiple comparisons involved in comparing each pair of entities, Bonferroni correction method was used. The second RQ was explored using a Chi-squared test of independence to determine whether the likelihood of recognizing anxiety varied among the different evaluators, taking the multiple vignettes into account as repeated measures. The third RQ was analyzed descriptively by comparing the percentage of referrals to different healthcare services by each entity, highlighting differences in their approach to managing anxiety. The fourth RQ was analyzed descriptively by comparing the treatment recommendations for mental and behavioral disorders across AI tools and GPs. This approach quantified the differences in recommendation patterns, highlighting the potential for integrating AI into clinical decision-making.
Results
Comparison of effectiveness of AI tools (ChatGPT-3, ChatGPT-4, Claude.AI, and Gemini) and human professionals (MHPs and GPs) in recognizing anxiety
To evaluate the differences in performance across these entities, Chi-squared tests of independence were conducted to assess the statistical significance of the observed frequencies in each category. Given the multiple comparisons across entities, post-hoc pairwise Chi-squared tests with Bonferroni correction were employed to identify which specific pairs of entities exhibited significantly different recognition rates.
Chi-squared tests of independence revealed significant differences in total recognition rates across the entities (χ2(5, N = 600) = 34.38, p < .001). Similarly, significant differences were found for the first identification (χ2(5, N = 600) = 37.41, p < .001) and second identification (χ2(5, N = 600) = 25.31, p < .001) questions. These results suggest that not all entities performed equally well in recognizing anxiety.
Post-hoc pairwise comparisons with Bonferroni correction revealed significant differences between ChatGPT-4 and both Claude.AI and Gemini for first identification and between ChatGPT-3 and GPs for second identification. Claude.AI and Gemini also exhibited significantly better recognition rates compared to GPs on both identification questions. These findings suggest that specific AI tools (Claude.AI and Gemini) outperformed others as well as human professionals in recognizing anxiety. Table 2 and Figure 1 show the anxiety recognition rates across the different entities.

Comparison of anxiety recognition rates across different entities.
Comparison of anxiety recognition rates across different entities.
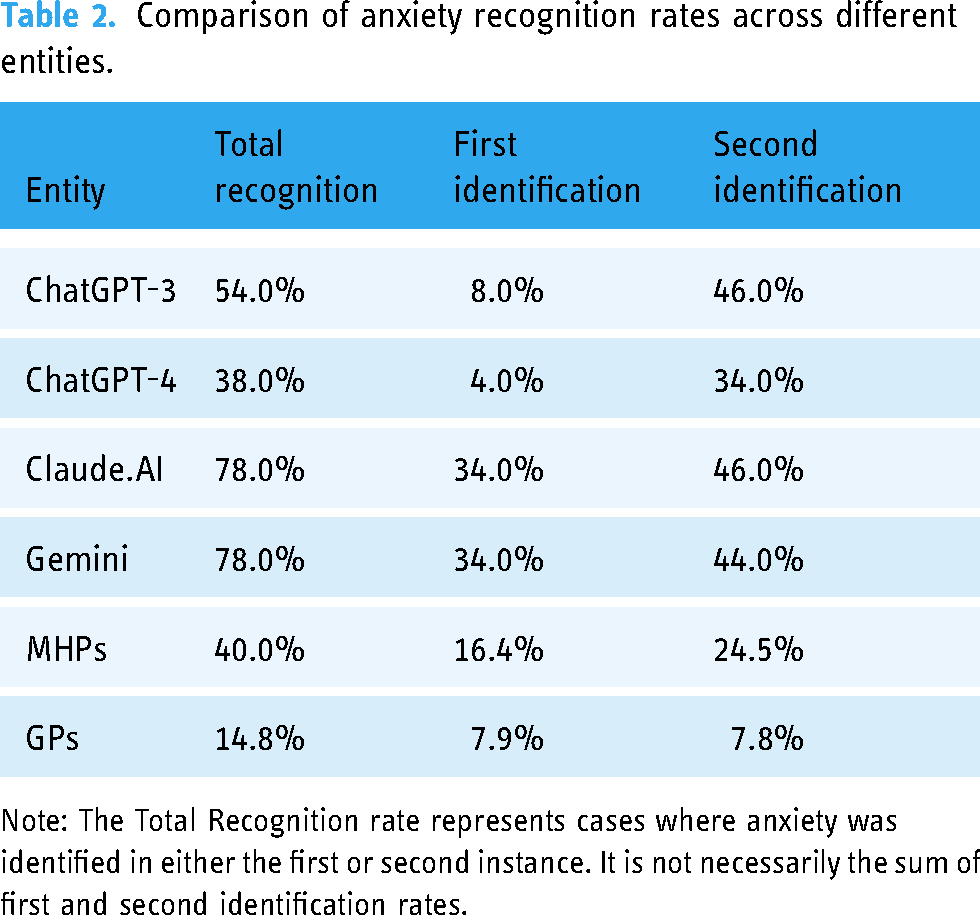
Note: The Total Recognition rate represents cases where anxiety was identified in either the first or second instance. It is not necessarily the sum of first and second identification rates.
Comparison of number of times anxiety was recognized over five vignettes by various AI entities and medical professionals
A Chi-squared test of independence was conducted to explore the relationship between type of evaluator (ChatGPT-3, ChatGPT-4, Claude.AI, Gemini, MHPs, and GPs) and frequency of anxiety recognition across the five vignettes. The analysis revealed a significant effect of type of evaluator on recognition of anxiety (χ2(25) = 931.66, p < .001), suggesting that the probability of recognizing anxiety varied among the different evaluators. Due to the low number of observations, a post-hoc analysis was not conducted.
As can be seen in Table 3 and Figure 2, all the AI tools recognized at least one vignette as anxiety, similar to the MHPs and contrary to the GPs. Claude.AI and Gemini identified at least four of the vignettes as anxiety. The comparison between ChatGPT-3 and ChatGPT-4 shows that ChatGPT-3 identified three vignettes as anxiety in 80% of the cases, whereas ChatGPT-4 identified only 1 or 2 cases of anxiety in 80% of the cases.

Percentage of times anxiety was selected by different AI tools and medical professionals, over five vignettes.
Comparison of referral recommendations among different LLMs and GPs.
Percentage of times anxiety was identified by different AI tools and medical professionals, over five vignettes.

Comparison of referral recommendations among different LLMs and GPs.

Ideal referral for child
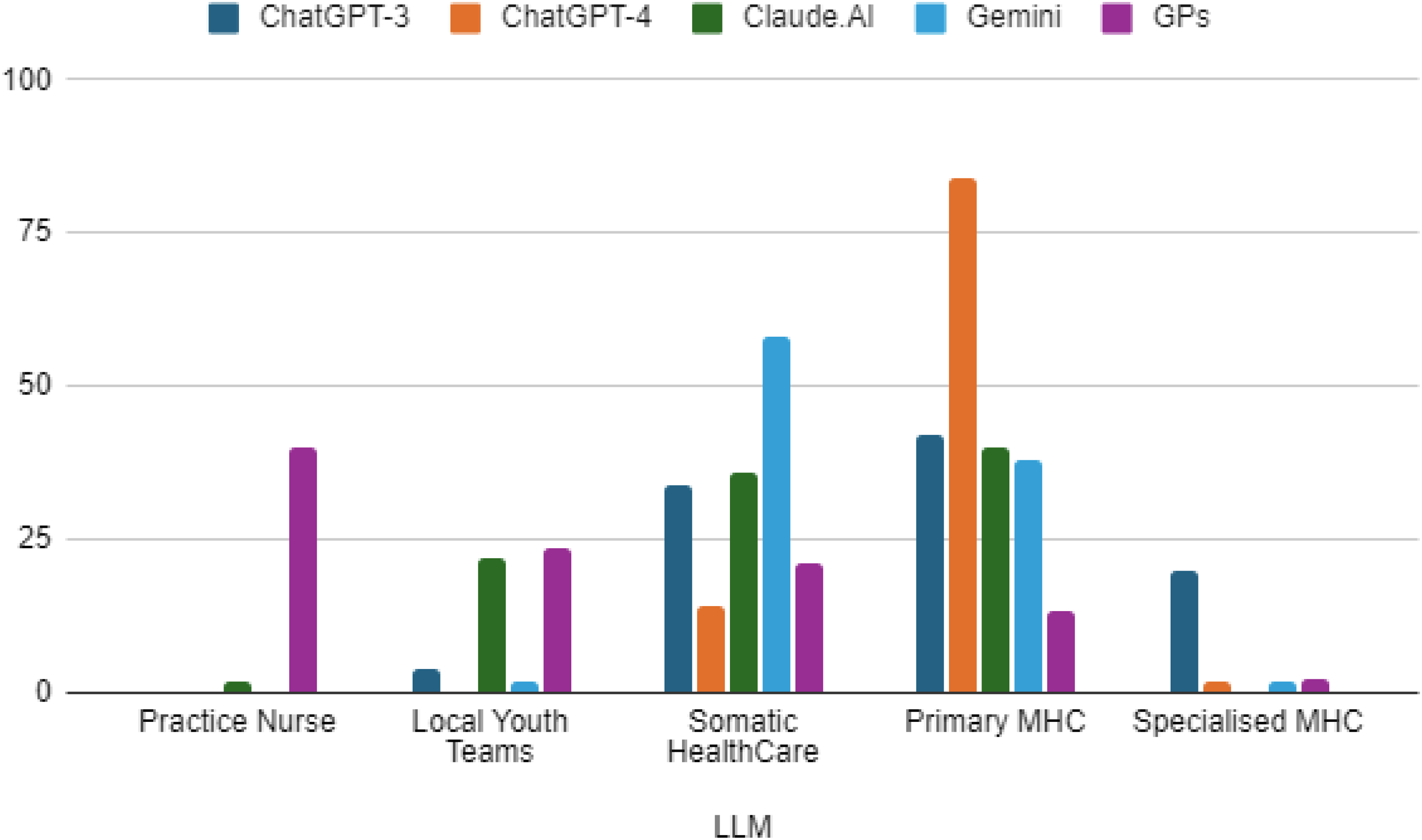
The comparison between the four AI tools and the GPs regarding where they would refer a child with a profile similar to the one in the vignette elicited interesting observations (Figure 3). The majority of the GPs responded that they would recommend treating the child in general practice (nurse practitioner = 40%). The AI tools, in contrast, did not recommend treating the child in general practice, except for Claude.AI in one case. Instead, the AI tools recommended referring the child to primary MHC or somatic healthcare. Claude.AI. recommended referring the child to local youth teams more frequently than the other AI tools, whereas ChatGPT-3 recommended referring the child to specialized MHCs more frequently than the other AI tools (Table 4).
Referral preferences for different types of disorders
The last stage of this research compared the recommendations of the four AI tools—ChatGPT-3, ChatGPT-4, Claude AI, Gemini—and of the GPs for eight distinct mental and behavioral disorders: anxiety, trauma, mood disorders, physical symptoms with psychological basis, eating problems, autism spectrum disorders, attention deficit hyperactivity disorder (ADHD), and difficult behavior. The treatment options ranged from less intensive approaches such as watchful waiting to more specialized interventions such as specialized mental healthcare. Table 5 compares the percentage of treatment recommendations for mental and behavioral disorders of AI tools and GPs.
Comparative analysis of percentage of treatment recommendations for disorders by AI tools and GPs.

Note: 1. The numbers in the table represent the percentage of responses for suggested treatment. 2. Empty cells signify that this option was not suggested as a response.
Anxiety
For ADs, GPs exhibited a balanced approach, recommending a variety of treatment levels, with a notable preference for general mental healthcare (53.6%) and nurse practitioner interventions (25.9%). In contrast, AI tools tended toward more extreme recommendations, with ChatGPT-4 and Claude AI favoring general mental healthcare and ChatGPT-3 and Gemini recommending specialized mental healthcare in all responses.
Trauma
In the case of trauma, the AI tools again showed a propensity for more intensive treatments, with ChatGPT-4, Claude AI, and Gemini predominantly recommending specialized mental healthcare. The GPs demonstrated a more distributed approach, albeit with a tendency toward recommending specialized mental healthcare (37.3%) and general mental healthcare (42.9%).
Mood disorders
For mood disorders the AI responses differed, with ChatGPT-4 and Claude AI significantly recommending general mental healthcare, diverging from ChatGPT-3's sole recommendation of specialized mental healthcare. GPs favored general mental healthcare (52.3%) but also considered nurse practitioner involvement (27.7%).
Physical symptoms
In addressing physical symptoms with psychological underpinnings, AI tools and GPs both recommended a range of treatments. GPs exhibited a notable preference for specialized mental healthcare (25.5%) and nurse practitioner interventions (33.5%). ChatGPT-4 uniquely recommended a balance of general mental healthcare and nurse practitioner interventions, while Gemini leaned toward less intensive options.
Eating problems
Eating problems elicited strong recommendations for specialized mental healthcare from all AI tools, with Claude AI equally endorsing general mental healthcare. In contrast, GPs predominantly recommended specialized mental healthcare (61.2%) but also considered less intensive options to a lesser extent.
Autism spectrum disorders
For autism spectrum disorders, the AI tools favored more intensive interventions, with ChatGPT-4 and Gemini primarily recommending specialized mental healthcare. GPs also preferred specialized mental healthcare (23%) but exhibited significant consideration of nurse practitioner (24.9%) and general mental healthcare (24.9%) interventions.
Attention deficit hyperactivity disorder
In the treatment of ADHD, ChatGPT-4 and Gemini showed a strong inclination toward specialized mental healthcare, whereas Claude AI recommended general mental healthcare. GPs displayed a balanced approach, with no clear preference among the treatment options, suggesting a case-by-case evaluation.
Difficult behavior
For difficult behavior, AI responses varied, with ChatGPT-4 and Gemini recommending specialized mental healthcare, while Claude AI favored general mental healthcare. GPs preferred general mental healthcare (44.4%) and nurse practitioner intervention (32.9%), indicating a preference for a step-up approach based on severity.
In summary, the AI tools tended to recommend more intensive treatment options across most disorders, particularly specialized mental healthcare. GPs, in contrast, displayed a more nuanced approach, considered a wider range of treatments and showed a tendency to prefer general mental healthcare and nurse practitioner interventions, potentially reflecting a more holistic and staged approach to treatment. This comparison highlights the potential differences in treatment recommendation patterns between AI tools and human practitioners, underscoring the importance of integrating AI recommendations with clinical judgment in healthcare decision-making.
Discussion
This study sought to compare AI tools and human professionals in recognizing anxiety among children. Our first research question asked how various AI tools compare to human professionals in accurately recognizing anxiety. Our findings directly answer this question, revealing that Claude.AI and Gemini demonstrated better detection rates than GPs in both identification instances. The research findings reinforce the existing body of literature by highlighting that unnoticed ADs are prevalent among children. 9 Even though children typically visit their pediatricians more than twice a year, over two-thirds of anxiety cases remain undiagnosed.10,11 GPs may fail to recognize ADs, suggesting that unfamiliarity with early symptom presentation may be a key factor. GPs adequately recognized anxiety in vignettes that explicitly mentioned ‘fears,’ but struggled with less overt presentations. Some GPs focused heavily on school and home functioning while overlooking other relevant domains, such as social relationships. 23 This underscores the potential use of AI to assist healthcare professionals as a supportive tool in detecting ADs. Investigations into the application of AI within the domain of mental health care (MHC) have yielded promising outcomes, with research examining its effectiveness across various dimensions, such as assessment, ongoing observation, and provision of therapeutic measures. Tools employing natural language processing have attracted significant interest due to their proficiency in mimicking human-like discourse and facilitating interactive dialogues. These instruments, often referred to as AI tools, offer potential for administering empirically supported mental health interventions. 4 Such interventions have shown initial success in diminishing symptomatology and enhancing overall mental well-being, with some investigations indicating considerable user satisfaction. 24 For instance, relative to the provision of assistance by human personnel, applications of AI-based tools have demonstrated efficacy in managing patient mental health.25,26 Furthermore, a recent comprehensive review of these applications revealed that mental health-oriented chatbots are characterized by their user-friendliness, appealing design, prompt responsiveness, reliability, and overall user satisfaction. 27
The second research question inquired about the frequency of anxiety identification by AI tools compared to human professionals. Our study revealed that each AI instrument successfully identified at least one case study as indicative of anxiety, mirroring MHPs and contrasting with GPs’ assessments. Claude.AI and Gemini identified a minimum of four vignettes as instances of anxiety. A comparison of the performances of ChatGPT-3 and ChatGPT-4 revealed that ChatGPT-3 recognized anxiety in three vignettes, whereas ChatGPT-4 recognized anxiety in only one or two vignettes. Even though no studies were found that directly compare Claude.AI and Gemini with medical teams, the current study also highlights the potential use of AI in mental health. The results of this study are in contrast to previous research that examined suicide, depression, and schizophrenia, in which superior capabilities were attributed to the ChatGPT-4 language model over other AI languages.2,3,5,28 For example, a comparative analysis of different LLMs, such as ChatGPT-3.5, ChatGPT-4, Claude, and Bard, that included mental health professionals (GPs, psychiatrists, clinical psychologists, and mental health nurses) revealed variations in AI assessments regarding recovery outcomes. Specifically, ChatGPT-3.5 tended to exhibit a consistently pessimistic viewpoint, whereas the assessments of ChatGPT-4, Claude, and Bard were more in line with the perspectives of mental health professionals and the general populace. 3
Our third research question explored the ideal placement recommendations for children with anxiety according to AI tools versus human professionals. The findings revealed, that on the question of the optimal referral for the child, a significant proportion of GPs indicated a preference to retain the child within the general practice setting, with 40% opting for nurse practitioner. In contrast, the AI tools for the most part did not advocate retaining the child in general practice, with the exception of a solitary instance involving Claude.AI. Instead, the AI tools displayed a tendency to recommend referring the child to primary MHC or somatic health care services. Aydin et al. 23 observed a notable discrepancy in GPs’ responses. While a majority of GPs indicated they would consider referring patients when they suspected ADs, in the presented case vignettes for the most part they opted for management within primary healthcare settings rather than referral to MHC. Conversely, AI systems showed a preference for referring cases to mental health services. This discrepancy may suggest that AI is capable of identifying a broader spectrum of symptoms without the influence of factors such as consultation pressure that a GP might experience. 29 Additionally, it may imply that doctors, while occasionally suspecting ADs, only refer to the most severe cases for specialized treatment, possibly due to constraints within their practice environment. 30
The final research question asked how treatment recommendations for mental and behavioral disorders differ between AI tools and GPs. The current study compared treatment recommendations for eight different mental and behavioral disorders, drawing upon the insights from four AI tools—ChatGPT-3, ChatGPT-4, Claude AI, Gemini—and the responses of GPs. The treatment options under consideration ranged from less intensive approaches such as watchful waiting to more specialized interventions such as specialized mental healthcare. The AI tools exhibited a notable inclination toward recommending more intensive treatments, particularly specialized mental healthcare, across the majority of the disorders. This tendency was most pronounced in the responses for anxiety, trauma, and eating problems, where the AIs almost uniformly suggested the highest level of care. In contrast, GPs demonstrated a more balanced and diversified approach in their treatment recommendations. For most disorders, they considered a range of treatment options, with a tendency to prefer general mental healthcare and nurse practitioner interventions. This suggests a more graduated approach to care, potentially taking into account the individual patient's circumstances and the severity of the disorder. In the field of medicine, preliminary studies have found a good predictive capacity for adapting drug treatment to AI.31,32 Research in mental health presents conflicting evidence about the predictive capabilities of AI compared to professionals. A review study highlights a shortfall in the diversity of treatment options provided by AI relative to therapists, undermining its reliability and utility for clinicians. 33 In another study, ChatGPT-3.5 and ChatGPT-4 mainly advised psychotherapy for mild depression (95% and 97.5%), unlike primary care physicians who rarely recommended psychotherapy (4.3%). In severe cases, ChatGPT favored psychotherapy, while physicians preferred combined treatments. 2
The current study found the most significant divergence between AI tools and GPs in the case of trauma and eating problems, with AIs predominantly recommending specialized mental healthcare, whereas GPs exhibited a broader distribution of recommendations. The literature review reveals multiple ways in which AI could enhance MHC, including support in self-management, diagnostic precision, and treatment monitoring. 34 Nevertheless, a recurring concern expressed by family doctors is the impact of AI on therapeutic relationships. Substituting AI for human contact could undermine the therapeutic alliance due to diminished empathy and misinterpretations. 35 Given the low remission rates and the complexity of these disorders, it remains uncertain whether AI can fully grasp and address them. Consequently, skilled clinicians who understand the individual's complexity and background and the nature of the disorder are still needed.
In addition, the category of physical symptoms was unique in that both AIs and GPs suggested a variety of treatment options, indicating no clear consensus regarding the most appropriate level of care. Adolescents frequently mask mental health issues with physical symptoms in primary care, yet over 50% remain unscreened for such concerns. Reviews of 11 studies suggest that pre-consultation electronic screening is effective in fostering open discussions and greater youth disclosure. 36
In this study, the AI tools’ preference for more intensive treatments raises questions about their risk-version or potential for overestimating the need for specialized care. This preference may reflect the algorithms’ prioritization of caution in the absence of nuanced clinical judgment. AI should augment rather than replace human decision-makers. Decision-making transcends algorithmic analysis by incorporating distinctly human traits such as creativity, intuition, and ethical judgments, highlighting the need for an integrated approach that combines AI with human insight. 37
The deployment of AI in the identification of anxiety disorders holds considerable promise, yet it is accompanied by an array of challenges. The precision of AI predictions is contingent upon the caliber and demographic inclusiveness of the datasets utilized for algorithm training. Data that are biased or lack adequate representation can lead to erroneous forecasts or exacerbate existing healthcare disparities. Moreover, AI algorithms frequently function as opaque entities, obscuring the logic underpinning their predictions. This opacity can hinder the development of trust and acceptance among end-users. Moreover, the application of AI in the diagnosis of anxiety disorders raises several ethical concerns. Paramount among these is the issue of safeguarding data privacy and security, given the particularly sensitive nature of mental health information. It is imperative that users receive clear and thorough information regarding how their data will be used and protected. Additionally, AI should not supplant the clinical acumen of healthcare professionals in diagnosing anxiety disorders. Rather, it should serve as an auxiliary tool that enhances the capability of practitioners to make informed clinical judgments.
Clinical implications
The findings of our research contribute to the discourse on overcoming obstacles in the provision of mental health services, in light of the inadequacy of current resources and intervention strategies to meet the extant and burgeoning demands. A report by the World Health Organization indicates that in excess of 400 million individuals worldwide are afflicted by mental health conditions. While psychotherapeutic interventions and social support mechanisms have demonstrated efficacy, there exists a significant barrier in terms of accessibility to such therapeutic and counseling services for numerous at-risk populations. For example, the psychiatrist-to-population ratio in most nations is less than 1 per 100,000 people, highlighting a critical shortfall in professional workforce and a dearth of available face-to-face treatment modalities.
The contrast between AI and GP recommendations underscores the potential for a synergistic approach in which AI can offer a preliminary assessment that GPs can refine, balancing the efficiency and breadth of AI with the nuanced, patient-centered approach of human practitioners. The varied treatment recommendations by GPs highlight the importance of human judgment in healthcare, which considers the patient's broader context, including factors that AI may not yet adequately account for.
Limitations
The current study highlights AI's potential in identifying anxiety disorders in children, yet certain limitations must be considered. The reliance on standardized vignettes may not fully encompass the complexity inherent in real-life assessments of anxiety disorders, indicating a need for further research that includes more detailed and personalized cases. Additionally, future studies must extend their scope to include a broader spectrum of factors, such as socioeconomic status, cultural backgrounds, and individuals’ previous mental health records, to achieve a more comprehensive evaluation. The cross-sectional nature of this research limits the ability to track the evolution of diagnostic precision over time. The inherent opacity of AI algorithms poses a challenge to the interpretation of their decisions. Developing innovative techniques that can demystify and illustrate the logic behind AI judgments would enhance transparency and insight. Moreover, the experimental setting of this study may not adequately reflect the intricate realities of implementing AI in actual clinical environments. Future research should investigate the practical aspects and ramifications of utilizing such AI models in genuine MHC settings, taking into account the interaction between human clinicians and AI technologies and the practicality of their integration.
To enhance the diagnostic accuracy of AI models in identifying childhood anxiety disorders, it is essential to incorporate a comprehensive range of information. This should include detailed symptom profiles encompassing both physical and psychological symptoms, as well as developmental and contextual data, such as the child's age, family history, and environmental influences. Longitudinal data on symptom progression, comorbidity information, and assessments of functional impact across various domains are also critical. Additionally, standardized scores from validated anxiety screening tools, treatment history, and cultural and socioeconomic factors should be integrated. Reports from schools and teachers, along with parental observations of home behavior and family dynamics, further contribute to a holistic understanding of each case. By incorporating this diverse array of data points, AI models can develop a more nuanced and accurate diagnostic capability. However, it is crucial to emphasize that, while AI can efficiently process and analyze complex information, the interpretation and application of AI-generated insights should always be guided by clinical expertise. This approach ensures ethical and patient-centered care, aligning AI's capabilities with the nuanced understanding provided by healthcare professionals.
Conclusion
This study explored the efficacy of AI tools compared to human professionals in identifying anxiety among children. The findings indicate a significant difference in recognition capabilities, with AI tools such as Claude.AI and Gemini demonstrating superior performance over GPs in the initial identification phases. This discrepancy highlights the potential of AI to enhance diagnostic processes in mental health. However, it is essential to consider AI as a supportive adjunct to healthcare professionals, rather than as a standalone diagnostic method. AI has the potential to complement traditional approaches by providing an additional layer of analysis, thereby improving the accuracy and efficiency of anxiety detection. Nonetheless, the integration of AI-generated insights should be balanced with the clinical judgment, expertise, and nuanced understanding that healthcare professionals bring to patient care.
The study also examined treatment recommendations, revealing differences between AI tools and GPs. AI tools tended to recommend more intensive treatments and specialized mental healthcare, especially for conditions like anxiety, trauma, and eating disorders. In contrast, GPs often preferred less intensive options, such as general mental healthcare or the involvement of a nurse practitioner. This divergence underscores the need for a collaborative approach that leverages both AI and human expertise. While AI can offer valuable insights and help identify cases that may otherwise be overlooked, healthcare professionals play a critical role in contextualizing these insights within the broader framework of the patient's life, preferences, and available resources.
Integrating AI into mental health diagnostics and treatment planning holds significant promise, but it should be implemented within a holistic framework that emphasizes the irreplaceable role of healthcare professionals. Future research and clinical practice should focus on developing methodologies that effectively combine AI capabilities with human expertise to optimize patient outcomes in MHC.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241294182 - Supplemental material for Large language models outperform general practitioners in identifying complex cases of childhood anxiety
Supplemental material, sj-docx-1-dhj-10.1177_20552076241294182 for Large language models outperform general practitioners in identifying complex cases of childhood anxiety by Inbar Levkovich, Eyal Rabin, Michal Brann and Zohar Elyoseph in DIGITAL HEALTH
Footnotes
Abbreviations
Availability of data and materials
The authors have the research data, which is available upon request.
Contributorship
IL contributed to the research design, wrote the study protocol, organized the study, coordinated the data collection, drafted the initial manuscript, and approved the final submitted manuscript. ZE contributed to the study design and organization, participated in the data collection, reviewed the manuscript, and approved the final submitted manuscript. MB contributed to the data collection. ER carried out the analysis. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure instructions
During the preparation of this work the authors used SPSS, Google sheets and ChatGPT to analyze and visualize the data. After using these tools/services, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical approval
The study was approved by the Ethics Committee of Oranim College (Authorization No. 1852024) and was conducted in accordance with the Declaration of Helsinki. No patients were involved, and there was no need for informed consent from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient and public involvement
No patients were involved.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.