
Abstract
Background
The clinical adoption of telerehabilitation accelerated rapidly over the last few years, creating opportunities for clinicians and researchers to explore the use of digital technologies and telerehabilitation in the assessment of deficits related to neurological conditions. The objectives of this scoping review were to identify outcome measures used to remotely assess the motor function and participation in people with neurological conditions and report, when available, the psychometric data of these remote outcome measures.
Methods
MEDLINE (Ovid), CINAHL, PubMed, PsychINFO, EMBASE, and Cochrane databases were searched between December 13, 2020, and January 4, 2021, for studies investigating the use of remote assessments to evaluate motor function and participation in people with neurological conditions. An updated search was completed on May 9, 2022, using the same databases and search terms. Two reviewers independently screened each title and abstract, followed by full-text screening. Data extraction was completed using a pre-piloted data extraction sheet where outcome measures were reported as per the International Classification of Functioning, Disability and Health.
Results
Fifty studies were included in this review. Eighteen studies targeted outcomes related to body structures and 32 targeted those related to activity limitation and participation restriction. Seventeen studies reported psychometric data; of these, most included reliability and validity data.
Conclusion
Clinical assessments of motor function of people living with neurological conditions can be completed in a telerehabilitation or remote context using validated and reliable remote assessment measures.
Introduction
Digital health is commonly used as an umbrella term describing the use of telecommunication technology within the healthcare context. 1 In rehabilitation, digital health may involve the use of information and communication technology such as smartphone applications, wearable sensors, activity tracking devices, and telehealth platforms to assess, monitor, or deliver care. Telerehabilitation is defined as the use of communication technology to provide rehabilitation services including clinical assessments, health monitoring, and interventions. 2 Although the adoption of telerehabilitation has increased dramatically over the last few years, rehabilitation professionals still report challenges associated with the uptake of telerehabilitation,3,4 documenting barriers such as remote assessment.
Outcome measures that are valid and reliable when used in remote assessments are necessary when documenting various motor deficits including balance, mobility, and upper extremity function. Currently, research has documented the psychometric properties of musculoskeletal assessments administered remotely (e.g., Oswestry Disability Index, goniometry)5,6; however, the lack of validated remote assessment measures for neurological deficits poses barriers to telerehabilitation implementation in neurological settings by limiting the ability of clinicians to objectively and accurately complete clinical assessment remotely. 7 Authors have reported that remote monitoring and remote assessment are more difficult than in-person assessment due to perceived safety risks, limited space in home settings, or the necessity of caregiver presence.8–10 Although the evidence is growing rapidly for the validity of such remote assessments,7,11,12 additional research is necessary to identify new validated clinical tools.
The objectives of this scoping review were to: i) identify the remote outcome measures being used in the assessment of people with neurological conditions (PwN) including the description of the neurological conditions and the clinician characteristics, ii) describe, as per the International Classification of Functioning, Disability and Health (ICF), how these remote outcome measures were being used, and iii) report the psychometric data (e.g., validity, reliability, normative values) when available.
Methods
Systematic search
The complete scoping review methodology is reported in O’Neil et al. 13 Briefly, following the methodology proposed by Arksey and O’Malley and adapted by Colquhoun et al.,14,15 an initial systematic search of MEDLINE (Ovid), CINAHL, PubMed, PSychINFO, EMBASE, and Cochrane (Appendix 1) was completed between December 13, 2020, and January 4, 2021. The search was updated on May 9, 2022. Specific search criteria were used to identify clinical outcome measures of motor deficits and function limitation of PwN (i.e., gait, balance, mobility, strength) conducted using telerehabilitation platforms including virtual reality, mHealth, videoconferencing, and digital health smart applications. Using Covidence online application (Melbourne, Australia), two reviewers (KB and EMD) independently screened article titles and abstracts to identify those meeting the inclusion criteria; two pairs of reviewers screened each article (KB, EMD, and JO). Full-text reviews were then completed by two reviewers (KB and JO) for articles meeting the review objectives. Conflicts were resolved by a fourth reviewer (LS) before moving to the next step. Interrater reliability between the three reviewers was assessed using Cohen's κ. The reference lists of all reviews and meta-analyses identified during screening were manually searched for additional articles. Since this scoping review did not involve human participants, participant consent was not necessary for this study.
Data extraction
Two reviewers (JO and KB) extracted data from the included articles by categorizing the information into four main domains: i) general information (i.e., study design, sample size, clinician administering the assessment, and neurological condition); ii) outcome measures as per the ICF classifications of body function (i.e., physiological body functions) and activity and participation (i.e., task execution and life involvement); iii) teleplatforms used; and iv) psychometric data (i.e., validity, reliability, and normative data). The level of evidence for included studies was rated, when possible, using the method presented by Butler et al. 16
Results
Included studies
The systematic search identified a total of 687 articles. Two hundred and ninety-three articles were found during the initial search in 2020/2021 and a further 387 in 2022. After hand-searching the reference lists of reviews and meta-analyses identified during screening, an additional 7 articles were added. Of the 687 articles, 364 duplicates were removed, and 323 titles and abstracts were screened. Of the 323 articles screened, 167 were excluded, leaving 156 full articles to be reviewed. A further 106 articles were excluded once the full articles were reviewed, leaving 50 studies on the use of remote assessments for people living with various neurological conditions (Figure 1). Of these 50 studies, seven were among those added following the updated search, which suggested an increased interest in remote assessment since the onset of the COVID-19 pandemic. Interrater reliability for full article selection was very high (k = 0.86) between reviewers KB and EMD and high (k = 0.80) between JO and KB. 17
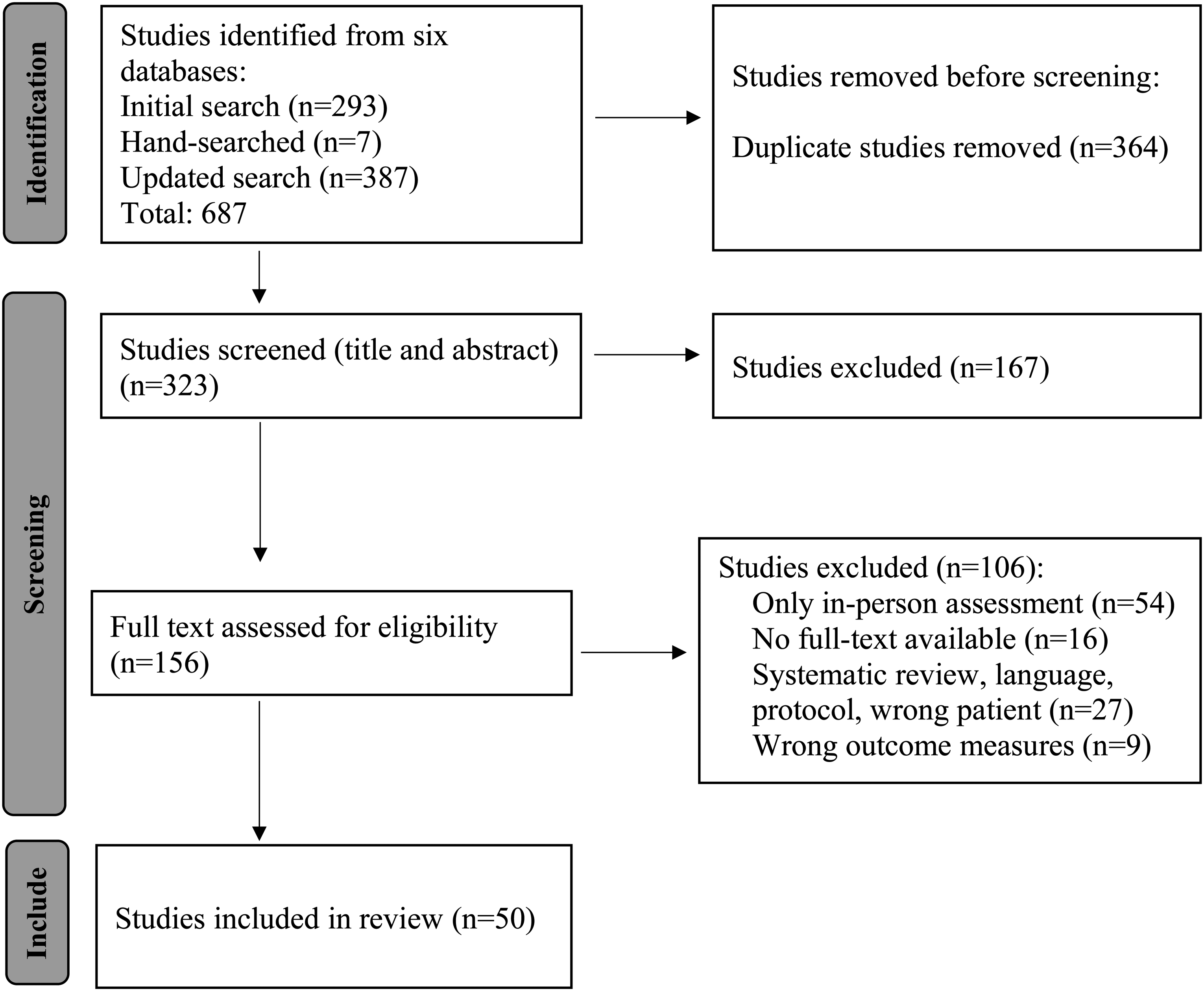
PRISMA flow chart reporting on study identification, screening, inclusion, and exclusion of studies (www.prisma-statment.org).
Objective 1: Identification of the neurological conditions assessed and the characteristics of the clinicians
The studies identified included those investigating remote assessment for people living with stroke (n = 17),11,18–34 Parkinson's disease (n = 16),35–51 traumatic brain injury including concussion (n = 8),52–59 multiple sclerosis (n = 6),60–64 and spinal cord injury (n = 3)65–67 (Table 1).
Description of included studies.

Note: OT: occupational therapist; PT: physiotherapist; SLP: speech language pathologist; RCT: randomized controlled trials.
Half of the studies (n = 25) included in this review were Level V evidence (i.e., case studies) and only eight were Level I evidence (i.e., RCT). Only 37 studies reported on the profession of the clinician completing the remote assessments; these included occupational therapists, nurses, movement disorder specialists, physiotherapists, speech-language pathologists, neurologists, athletic trainers, and exercise physiologists.
Objective 2: Remote outcome measures described using the International Classification of Functioning, Disability and Health
Body structures
Eighteen studies investigated how remote outcome measures were implemented and used to assess deficits specific to body structure impairments. Investigations included the remote assessment of upper extremity motor impairments (n = 5), overall changes in range of motion, strength, or speed of muscle contraction (n = 5), condition-specific neurological impairment assessment (n = 4), lower extremity impairments (n = 2), and postural instability (n = 2). Teleplatforms included were virtual reality coupled with wearable sensors, asynchronous and synchronous telerehabilitation administered via videoconferencing, mobile applications, and home-motion sensors (Table 2A).
Remote assessments used to assess body structure impairments in various neurological conditions, following the International Classification of Functioning, Disability and Health.

Activities and participation
Thirty-two studies reported on outcomes documenting changes in or status of activity limitations. No studies reported on outcomes specific to social participation restriction. Studies remotely assessed functional mobility, gait, and physical activity (n = 12), upper-extremity function including manipulation, grasp-and-release and reaching (n = 10), balance limitations (n = 7), and activities of daily living including communication activities and speech (n = 4). Virtual reality technology with or without wearable sensors or haptic systems was most frequently used, followed by wearable sensors combined or not with mobile applications and synchronous telerehabilitation (Table 2B).
Remote assessments used to assess activity limitation in various neurological conditions as per the International Classification of Functioning, Disability and Health.

Objective 3: Psychometric data
Out of 50 studies, 17 studies provided psychometric data for the remote outcome measures used. These included test–retest reliability of remote assessment, validity, and correlation between remote and in-person or traditional assessment as well as information around usability, acceptance, and satisfaction. A single study provided minimal clinical important difference (MCID) and normative values. Specifically, a cutoff score of steps per day was documented using wearable sensors that enabled the differentiation of ambulatory status in people living with Parkinson's disease 62 (Table 3).
Available psychometric data for remote assessments of neurological conditions.

Discussion
The majority of studies identified for this review are feasibility or pilot studies (level V evidence), reflecting the novelty and preliminary exploration of the use of certain technologies and virtual care systems for remote assessment of PwN.
Remote outcome measures
Studies reported on lab-based or expensive remote technology including haptic systems,18,23 Computer-Assisted Rehabilitation Environment system (CAREN),55,56 Actigraph,40,62 and immersive virtual reality.28,41,42,44,48 Results from this review also revealed that asynchronous technology (i.e., mHealth or wearable sensors using store-and-forward communication) was used more frequently than synchronous technology (i.e., videoconference) when assessing PwN. Importantly, this scoping review demonstrates that there is a significant gap in the determination of needed psychometric characteristics of remote assessment developed for people living with neurological conditions. Telerehabilitation is growing and is quicky being accepted as a way to reduce access barriers for people living with neurological conditions.68–72 The use of sensor technology including wearables, wireless motion sensors, and smart home technology is expanding, in fact, some authors have even identified remote assessment as its own field in telemedicine called “telesemiotic.” 73 For instance, Cubo et al. used motion sensor to capture changes in motor symptoms for people living with Parkinson's 39 while others have studied the use of home sensors to assess safety and night-time wandering with people living with dementia. 74 Usability of a device is critical for self-monitoring, autonomous use, and self-efficacy.75,76 Emerging smart home technologies have the potential to improve independence, quality of life, and remote monitoring for people with disability.77,78 Access, cost, portability, and availability of teleplatforms must be considered as laboratory-grade devices or expensive remote assessments may pose a challenge for clinical adoption and implementation.
Types of assessment as per the International Classification of Functioning, Disability and Health
Studies incorporating remote assessments of body impairments were mostly completed with people living with impairments from stroke, multiple sclerosis, and Parkinson's disease. Mobile applications and wearable sensors were most frequently used and were reported as easy to use. Specifically, people living with Parkinson's disease reported that mHealth applications were easy to use. 40 The use of remote supervision to monitor changes in symptoms and inform prognosis is increasingly reported when monitoring symptoms of Parkinson's disease36,39,46,47 and could well be suited for other neurodegenerative conditions such as multiple sclerosis, amyotrophic lateral sclerosis, and muscular dystrophy.
Studies of activity and participation used wearable technologies to detect changes in activities such as mobility, gait, and upper extremity functional tasks. This supports findings from recent systematic reviews reporting on the use of mobile devices to assess gait in people with Parkinson's disease, 79 to assess physical activity and mobility in PwN, 7 and on the feasibility of using remote assessments for hand function in PwN. 80 To date, a limited number of studies have targeted the use of remote assessment for social participation or community reintegration outcomes for PwN.81,82 Community integration and societal participation are crucial components of life satisfaction for PwN. 83 Future research should, therefore, focus on the development of remote assessments targeting social participation for PwN. Defining the ICF construct being assessed in terms of body impairments, activity limitation, or participation restriction may facilitate the development and clinical use of remote assessment.
Psychometric data
Only one-third (n = 17) of the studies documented the psychometric properties of the remote outcome measures used. Importantly, these psychometric properties were mostly established in a controlled and standardized environment such as a laboratory setting. Therefore, it is critical to determine similar properties in clinical and home-based environments. No studies reported the standard error of measurement, the data around floor and ceiling effects as well as measure responsiveness is lacking and only one study documented the MCID and clinical normative data, making it harder for clinicians to rely on remote assessments for treatment planning.
Moderate to strong correlations between in-person and remote assessment measures were reported in a small number of the studies. However, a lack of congruence between the assessments performed in-person and remotely was also frequently documented. For example, Tobler-Ammann et al. 23 documented high test–retest reliability for the virtual version of the Nine Hole Peg Test (NHPT) but when they compared it to an in-person assessment with a similar construct such as the Box & Block Test (BBT), correlations were low for the number of transported cubes (p = −0.23) and dropped cubes (p = −0.12). It is unclear if this difference was observed due to a lack of correlation between the in-person BBT and the virtual NHPT or because one test was administered in-person and one was administered virtually. Similarly, Wang et al. reported that people living with Parkinson's disease reached less far when measured using a wearable sensor in a virtual environment compared to the in-person environment while completing the same task. 49 Although the same measure could be administered in a virtual and in-person context, they may be measuring different constructs as described by the ICF. For example, the in-person BBT could be measuring an activity-related task, while the virtual reality version could be measuring body impairments such as the velocity of finger movements. Since psychometric properties may differ depending on the context within which the assessment is being administered, validity, reliability, diagnostic accuracy, and normative values associated with a clinical measure should be established independently for both in-person and remote assessments 84 and within the context that it is being used. 85 Identifying comparative psychometric norms between in-person and remote assessments is key to the successful and effective hybrid use of telerehabilitation. It is also critical that validated remote assessments specific to other neurological injuries not included in this review be made available.
Limitations and opportunities
The terminology used as search terms, as well as by authors to describe remote assessment, is an important limitation to note as it might have limited the number of studies identified and may have excluded potentially eligible studies for this scoping review. For example, overarching terms for telehealth, mHealth and telemedicine were used as search terms in this review, which may have led to missing key studies which used specific terms or devices for telehealth assessments such as smartphone applications. Future studies should expand search terms to include specific technologies used in telehealth. Our initial search was completed in 2020 near the beginning of the COVID-19 pandemic and an updated search was performed in May 2022 (2 years into the pandemic). Due to the rapidly growing body of literature on this topic, future updates will be necessary.
Conclusion
It is critical for healthcare providers to consider the neurological condition, the outcome being assessed as per the ICF, the type of remote monitoring, as well as teleplatform used when using remote assessment clinically. Results from our review demonstrated that the identification and reporting of psychometric data for remote clinical outcome measures is still novel and psychometric properties may differ when being assessed in clinical or home environments, and laboratory spaces. When possible, clinicians should use remote assessments which have been validated in a clinical or home space before adopting them within their clinical practice. It is necessary to establish the reliability and validity of remote assessments for each neurological condition to improve adoption and clinical implementation of assessment measures within various clinical contexts.
Footnotes
Authors’ note
International Registered Report Identifier (IRRID): PRR1-10.2196/27186.
Acknowledgments
The authors acknowledge the valuable assistance from the UOttawa librarian in the development of the search strategy.
Contributorship
Each author has made substantial contribution to the development of the methodology, data collection and analysis, and interpretation of the findings. Each author contributed to the redaction, and revision of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable for this scoping review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KB is supported by an admission scholarship from the University of Ottawa and by a grant provided by the Workplace Safety and Insurance Board (Ontario). The provision of grant support by WSIB does not in any way infer or imply endorsement of the content by the WSIB.
Guarantor
Not applicable