
Abstract
Telemedicine (TM) is a new medical service model in which computer, communication, and medical technologies and equipment are used to provide “face-to-face” communication between medical personnel and patients through the integrated transmission of data, voice, images, and video. This model has been increasingly applied to the management of patients with sleep disorders, including those with obstructive sleep apnea syndrome (OSAS). TM technology plays an important role in condition monitoring, treatment compliance, and management of OSAS cases. Herein, we review the concept of TM, its application to OSAS, and the related effects and present relevant application suggestions and strategies, which may provide concepts and references for OSAS-related TM development and application.
Introduction
With the rapid development of communication technology, informatization has become a prominent feature of the modern society. Telemedicine (TM), a novel medical model using the network communication technology for remote diagnosis, treatment, and management services to promote patient health, is becoming increasingly popular. Through two-way video, wearable devices, smartphones, wireless tools, and other forms of telecommunication technology, TM aids in providing emergency medical decision-making and chronic disease management and improving access to health care for patients in remote areas.1,2 The core pathophysiological mechanism of obstructive sleep apnea syndrome (OSAS) is obstructive sleep apnea (OSA). OSA, defined as apnea, hypopnea, or respiratory effort-related microawakening events at least 5 times/hour, is a chronic condition in which the upper airway is obstructed due to soft tissue relaxation of the pharynx during sleep, throat contraction, and reclining of the base of the tongue. 3 Common clinical symptoms of OSAS include daytime sleepiness, nighttime snoring, headache, and difficulty breathing after waking,4–6 significantly affecting the patient's daily life. The main risk factors for OSAS include obesity, age, sex, and large neck circumference,7–9 and the condition is often associated with diseases such as hypertension, stroke, and diabetes mellitus.10–12 Epidemiologic studies have shown that 10% of 30- to 49-year-old men and 3% of 30- to 49-year-old women have moderate or higher sleep-disordered breathing; moreover, this prevalence is 17% in 50- to 79-year-old men and 9% in 50- to 79-year-old women.13–15 According to the 2012 American Academy of Sleep Medicine (AASM) judgment criteria, 16 globally, the number of 30- to 69-year-old individuals with OSA increased from 9.8 billion in 2015 to 1.05 billion in 2019; this number is expected to increase to approximately 1.147 billion by 2024 (Figure 1). Moreover, many patients with OSAS demonstrated an urgent need for effective diagnosis and treatment and refined chronic disease management. 17 Because of the prevalence and indiscernibility of OSAS symptoms and the limitations related to conventional OSAS management modalities (e.g. poor therapeutic efficacy, poor adherence, high cost, and low equipment portability), many patients do not receive timely treatment and management. 18 The AASM guidelines for the clinical application of TM in patients with sleep disorders 19 also advocate the development of OSAS home diagnosis, treatment, and remote management through TM technology, as well as the construction of a TM management model, so as to improve the quality of life of patients with OSAS. The AASM's recent research advancements have demonstrated that TM is effective in OSAS diagnosis and management, particularly in improving the effectiveness of positive pressure ventilation therapy.20,21

Projected trends in OSA population.
Herein, we review the application of TM to OSAS and the related effects and provide relevant strategies and suggestions, with an aim to inform clinical and community medical workers and provide references for future comprehensive applications of TM to OSAS.
TM overview
TM is a new patient-centered health care system integrating remote monitoring, diagnosis, treatment, and remote management through the online transmission of data, voice, images, and other information from a patient's home via electronic devices, sensors, the Internet, and other technological modes 22 (Figure 2). The aim of TM is to improve medical standards and promote patients’ self-management of diseases. TM allows patients with OSAS to complete the examination process at home without being hospitalized for overnight sleep apnea monitoring; as such, OSAS patients who are located far from health care centers, nonambulatory, and of low economic status can obtain medical service resources to fulfill their diversified and multilevel needs in a timely manner. 23 In addition, real-time TM can reduce or prevent various difficulties encountered by patients with OSAS in the long-term use of noninvasive positive pressure ventilation therapy at home, enhance the patients’ adherence to long-term treatment at home, and ease the provision of professional guidance, publicity, and education. Currently, TM for the treatment and management of chronic diseases such as stroke 24 and diabetes mellitus 25 is relatively well-developed. For OSAS treatment and management, however, continuous positive airway pressure (CPAP) is currently the preferred treatment, while for remote data monitoring of patients, remote video consultation, wireless wearable devices are relatively few applications. Therefore, the application of TM technology to OSAS can reduce bias in medical resource distribution, increase access to medical services in remote areas, and fulfill patient health care needs. 26
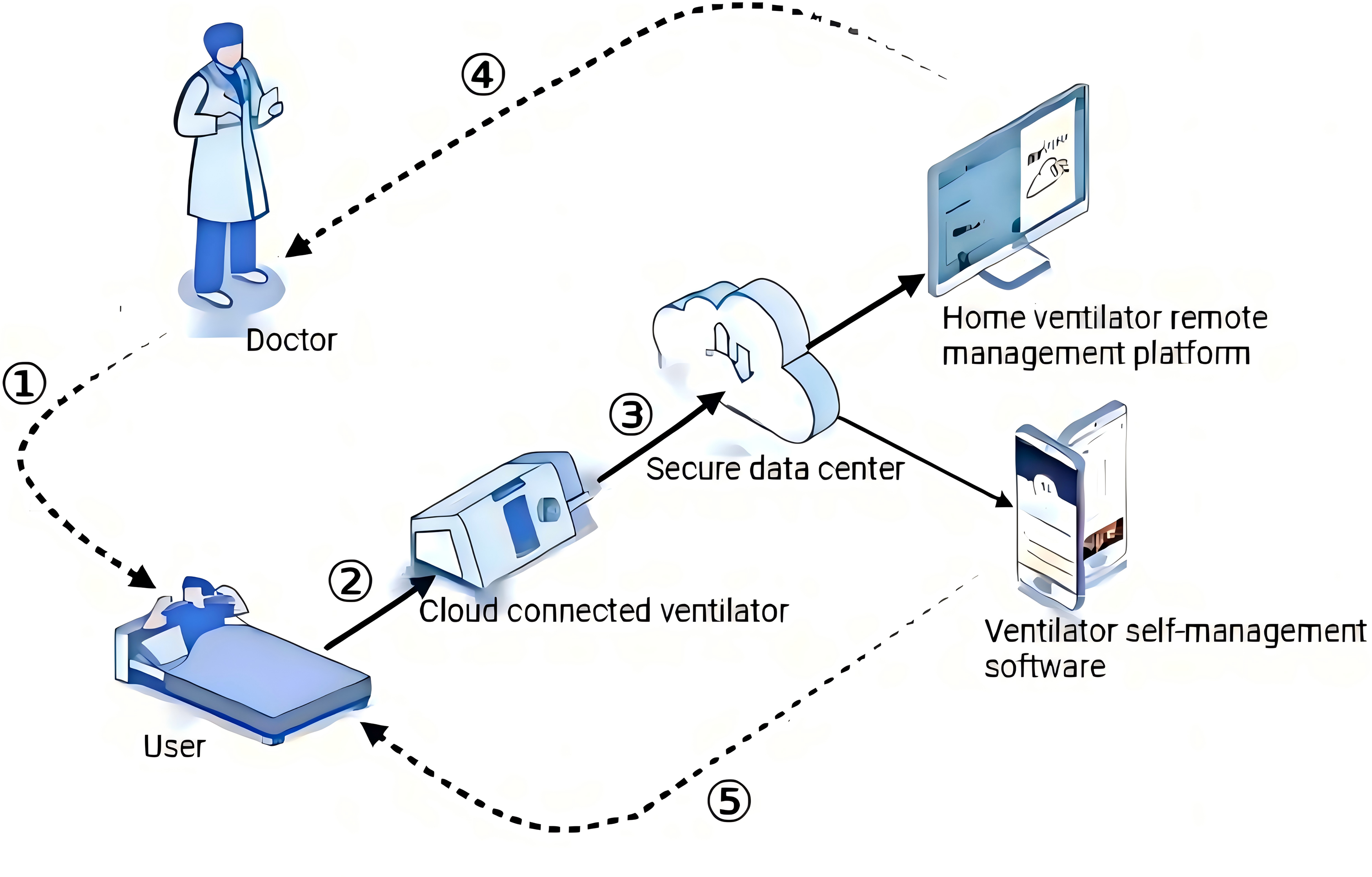
TM cloud management flow, with sleep apnea management as an example: 1 = remote monitoring and management by a physician, 2 = ventilator use by a patient, 3 = upload of data to the cloud, 4 = review of treatment and usage data by the physician, and 5 = understanding of the daily treatment results and usage issues by the patient through cell phone.
Importance of TM for OSAS
Conventional polysomnography (PSG) is performed all through the night in a sleep laboratory with professional assistance. However, because the number of sleep medical resources is limited, meeting the needs of many patients can be difficult, making OSAS diagnosis and treatment inconvenient. 27 In recent years, with the development of home sleep apnea monitoring (i.e. home sleep apnea test (HSAT)), 28 wireless wearable devices, 29 and wireless transmission devices, the conventional diagnosis and treatment modes have become sophisticated to a large extent (Figure 3). Patients undergoing HSAT at home and subsequently followed up at outpatient clinics have demonstrated considerable improvements in patient consultation rates. Since the COVID-19 pandemic, the use of wearable devices and Internet technology for OSAS has gained further popularity.30,31 Through TM, patients can consult with their sleep physician remotely via video and undergo HSAT at home. The treatment data can be synchronized to a web-based interactive platform via a wireless, modem-based positive pressure ventilation device, allowing sleep physicians to follow up with their patients directly via a remote management platform. 32 Therefore, TM can effectively enhance OSAS diagnosis, treatment, and management.

Clinical roadmap for OSAS diagnosis and management.
OSAS TM applications
Clinical video telehealth
Clinical video telehealth (CVT) is the most widely used TM technology for remote consultation and follow-up of patients with OSAS. In CVT, health care professionals and patients communicate remotely via two-way video. In this novel paradigm, medical consultations and exchanges, as well as physical examinations using remote stethoscopes and mobile cameras, can be conducted via video even when the participating parties are far apart; moreover, the diagnostic and therapeutic contents can be transmitted during physician–patient communication. 33 In a study on the reliability of two-way videoconferencing in CPAP-based treatment, 34 patients with CPAP were divided into face-to-face consultation and teleconsultation groups; the teleconsultation group patients underwent remote PSG (outside of a sleep center). The between-group difference in terms of CPAP treatment adherence over 6 months was found to be significant. In their study, Kosky et al. 35 found that patients trained for CPAP therapy via videoconferencing were 2% more knowledgeable about OSAS and CPAP therapy than those trained via face-to-face consultation; their results demonstrated the effectiveness of televideo education in improving patient knowledge. In a recent study, Isetta et al. 36 enrolled 50 patients with OSA from a sleep laboratory; they were followed up via teleconsultation and then asked to anonymously evaluate the effects of teleconsultation. Their results demonstrated that >95% of the patients surveyed were satisfied with teleconsultation and that 66% of the patients felt that teleconsultation could replace their offline follow-up. Recently, Fields et al. 37 prospectively compared remote video consultation with traditional face-to-face consultation model on the basis of the feasibility of OSAS management pathway in TM. Their authors noted that all patients indicated that teleconsultations and in-person visitations were comparable in terms of quality and content; moreover, teleconsultations demonstrated more positive effects. TM can improve satisfaction, lifestyle behaviors, social support, and family education in patients with OSAS. Moreover, remote, mobility-impaired patients with OSAS and their caregivers are more likely to use TM for consultation and follow-up.
Remote sleep-monitoring devices
Remote PSG monitoring devices.
Remote PSG, or tele-PSG, is operated using mobile devices and sensors with remote data transmission over the Internet. This type of monitoring is processed and analyzed while obtaining data such as sleep apnea index, breathing patency, and heart rate and remotely diagnose and treat OSAS. Gagnadoux et al. 38 evaluated, for the first time, the effects of real-time teletransmission on unattended PSG in a prospective randomized crossover trial in which 99 patients underwent inpatient PSG on two consecutive nights and an inpatient unattended but tele-PSG treatment. The patients undergoing tele-PSG treatment were controlled intermittently, in real-time, and remotely by a sleep technician in a centralized sleep laboratory. Their results demonstrated that the effectiveness of tele-PSG was much higher than that of control treatment.
New types of wearable devices.
Wearable devices are portable electronic health devices worn directly on the body during clinical and daily health activities. 39 By wearing a sleep-monitoring device, a patient can monitor their sleep status in real-time, including indicators such as sleep time, sleep depth, and number of apneas.40,41 These data can aid health care professionals in assessing a patient's condition more accurately and developing a more effective treatment plan. Ishida et al. 42 proposed a new wearable respiratory monitoring system developed for noninvasive detection of sleep apnea syndrome. The system was attached to a shirt in close contact with a patient's chest, and time-frequency analysis was used to detect whether the patient was breathing during this period. When the patient demonstrated 10-second apnea, a microcontroller sent the recorded respiratory waveforms during and a minute before and after the apnea directly to a hospital server computer via a cell phone. The server computer then automatically created an apnea profile for each patient. Erdenebayar et al. 43 also proposed a new method for OSAS detection by using a wearable piezoelectric sensor. The device was attached to a patient's neck and detected heartbeats via pulse waves originating from the carotid artery, providing data related to not only snoring but also movement and heartbeat during sleep. The results demonstrated the feasibility of piezoelectric sensors for OSAS detection, as well as their reliability for sleep monitoring and OSAS diagnosis. In a clinical trial comparing finger-ring oximetry with laboratory PSG, 44 207 Chinese individuals were subjected to both PSG and finger-ring testing at a sleep laboratory; the results demonstrated that finger-ring testing had high specificity for accurate identification of patients with moderate-to-severe OSAS, facilitating high-risk patient stratification. A finger-ring blood saturation meter monitors the oxygen, oxygen desaturation index, body motion, and heart rate variability; its main advantages are that it is comfortable, convenient, and easy to wear. In a European clinical trial on the accuracy of wearable devices, 45 data from 101 patients diagnosed as having OSA were analyzed using laboratory PSG and the NightOwl wearable device, and their results were compared with those of the Michele Sleep Scoring System (manual combined with automated). The results demonstrated that the NightOwl wearable device was extremely sensitive and specific. However, there has not been sufficient clinical validation of NightOwl, and clinical researchers can further carry out sufficient empirical studies. The reliability and effectiveness, sensitivity and specificity of the new long-range radar monitoring device were analyzed in a study of overnight PSG and simultaneous sleep monitoring of the subjects. 46 The results show that the new radar monitoring device, as a portable instrument, can calculate the sleep cycle by relying on the breathing rate, and its accuracy, size, and volume are more advantages than PSG. Many studies47–49 have revealed that both the NightOwl and finger-ring wearable devices are more accurate than the laboratory PSG (Table 1).
Accuracy of various wearable devices for sleep monitoring.

Telehealth management platforms
According to the 2016 European Respiratory Society's statement on remote monitoring of patients relying on ventilators, 6.6 in 100,000 individuals need long-term ventilator treatment in Europe; moreover, the number of relevant patients and the related costs are increasing, and the existing health care institutions are largely unable to meet their needs. 50 A sleep respiratory monitoring management platform for OSAS treatment, involving a two-way information exchange between physicians and patients with OSAS, can resolve issues associated with timely self-use of ventilators and significantly improve machine-wearing adherence and treatment effects among the patients. It can also provide convenient data support for sleep medicine center standardization to the patients, thus promoting appropriate follow-up management and affording high clinical value. 51 Deng et al. 52 prospectively enrolled 48 severe OSAS patients receiving CPAP treatment and randomized and equally divided into two groups: Group A in which guided treatment was administered using the conventional ventilator card-reading mode and Group B in which guided treatment was administered the cloud platform of sleep apnea monitoring and management. In general, compared with Group A, Group B demonstrated better outcomes, including adherence, mean oxygen saturation, titration pressure, and Epworth Sleepiness Scale counting score; moreover, Group B patients demonstrated higher confidence in treatment. In a study, 53 investigators uploaded HSAT data, as well as CPAP data transmitted from the patient's residence for remote monitoring, to the Remote Veterans Apnea Management Platform (REVAMP) for sleep practitioners to review and take action on. Veterans under CPAP treatment were asked to complete an initial standardized questionnaire, collecting data such as their sleep habits, quality, and concerns, in the REVAMP. Moreover, the veterans registered their devices in the REVAMP, and their device data were displayed to both the veterans and clinicians. Through the REVAMP, the veterans could access their CPAP data, communicate with their clinicians via email, self-administer their CPAP therapy by using available video tutorials and support materials on the platform, and complete regular follow-up questionnaires facilitating assessment of changes in the veterans’ symptoms and sleep quality.
A remote health management platform can be used as a continuity management tool with personalized features. Through relevant platforms on specific websites or cell phone applications, patients can participate in their disease self-management process, which may include obtaining disease knowledge and tracking monitoring indicators such as ventilator use, daily exercise, diet, and CPAP data. These platforms are conducive for health education and psychological guidance of patients with OSAS.
Effectiveness of TM in patients with OSAS
Improvement in CPAP treatment compliance and promotion of disease recovery
Treatment adherence is defined as a patient's self-management or treatment in accordance with recommendations and prescriptions from medical personnel. 54 Currently, CPAP ventilation is a treatment methodology commonly used for patients with OSAS; however, it is the most effective when patient adherence is high. TM allows patients with OSAS to be educated and managed through real-time interventions provided by mobile applications. In their prospective study, Garmendia et al. 55 administered participants with teleeducation; the intervention comprised (i) use of a smartphone application where a nurse provided patients with treatment information and (ii) daily transmission and analysis of signals from a CPAP device, along with potential changes in nasal pressure, if necessary. At the end of the intervention, CPAP adherence time increased, along with a significant decrease in the number of patients with low adherence. Aardoom et al. 56 conducted a meta-analysis on the effectiveness of a wide range of e-health interventions in improving CPAP treatment adherence. The results demonstrated that in adults with OSAS, the e-health interventions gradually improved CPAP adherence at 3 weeks after treatment initiation, increasing the average time spent using it per night by approximately 30 minutes. These results significantly improved adherence to treatment in adults with OSAS through distance education. In two recent studies,57,58 researchers analyzed the effects of TM after 3 months of conventional treatment through the development of individualized treatment plans, regular follow-up, and monitoring of patients with OSAS. The results demonstrated that after 6 months of follow-up, adherence improved in both TM studies.
In patients with OSAS, CPAP treatment adherence, a complex behavioral issue, is influenced by many factors. In addition to objective factors, a positive initial experience and supportive health care services are essential for long-term CPAP treatment adherence. The aforementioned findings clarify that TM and related technological interventions play an important role in increasing CPAP adherence and that targeted and individualized interventions are relatively effective in improving CPAP treatment adherence.
Improvement in self-management skills for disease recurrence prevention
Self-management behavior refers to the behavior of patients to maintain and promote their health; to reduce the impact of their diseases on their social functioning, emotions, and interpersonal relationships; and to persistently treat their diseases. 59 A self-management model combined with personalized health education and health interventions on the mobile application WeChat demonstrated favorable results. 60 In patients with OSAS, personalized behavioral interventions, which prompt active lifestyle adjustments and improve self-management, have been noted to alleviate OSAS symptoms and improve health.61,62 In their study, DeMolles et al. 63 randomly divided patients with OSAS into remote and control groups; in the remote group, a computer-based telephone-linked communication system was used by patients to ask questions and by physicians to monitor the patients’ self-reported behaviors and provide education and behavioral reinforcement for health-related behavioral goals. The results demonstrated that after 2 months of follow-up, the rates of improvement in the patients’ quality of life and sleep-related symptoms were significantly higher in the remote group than in the control group. Moreover, personalized education combined with interventions on a remote web-based platform has been demonstrated to effectively improve self-management in patients with OSAS. Suzanne et al. 64 designed a self-management intervention to improve CPAP treatment adherence in patients with OSAS; the intervention included health education, self-management tools, and cognitive restructuring. Communication with the provider for guidance and effectiveness of same-disease case guidance has been observed to improve patient motivation and self-efficacy in problem-solving. Hood et al. 65 applied interventions such as daily dietary self-monitoring and cognitive–behavioral weight loss manuals to promote self-management in patients with OSAS over 6 months through remote supervision on WeChat. The results demonstrated that among the patients with OSAS, supervising diets through WeChat effectively facilitated weight loss and improved self-management.
Reduction in psychological pressure and improvement in patient satisfaction
TM technology can save time and energy through the elimination of the need for patients to make frequent trips to health care facilities. Patients can be monitored and treated at home, improving access and flexibility and increasing patient satisfaction considerably. 66 TM allows patients with OSAS to be remotely contacted via telephone or video, affording convenient health care access for satisfactory OSAS management. Younger (<65-year-old) patients with OSAS are more inclined to recommend teleconsultation to others than patients from other age groups.58,67 Valentina et al. 68 reported that at a sleep clinic, the participation rate was 82% among 163 patients. After 12 weeks of monitoring, the patients responded to an online satisfaction survey; the highest level of agreement was observed for the statement “I am satisfied with the web service,” confirming their interest in participating in long-term web monitoring. In another study, 69 80% of the individuals felt satisfied with having an appointment for their sleep medicine issues through TM; they were also satisfied with TM appointments for OSAS evaluation and found making these appointments convenient. In summary, TM can improve access to OSAS evaluation without reducing patient satisfaction, particularly if these appointments are financially comparable with offline visits.
Increase in health care access and reduction in care cost
TM can be used as a strategic approach to address the public health challenges related to chronic diseases, providing a relatively cost-effective management option. 70 For patients with OSAS, physical disability, distance to the clinic, economic effect of family, and lack of health care professionals can negatively affect health care coverage. In their study, Isetta et al. 71 applied a web-based TM strategy to follow-up patients at home through an established website; the strategy afforded savings in transportation costs and reduction in lost productivity (i.e. indirect cost), thereby reducing the total cost and saving time and financial resources effectively. Contal et al. 72 assessed reductions in costs associated with remote management in 120 patients diagnosed as having OSAS, who were randomized into usual-care and telemonitoring groups. The telemonitoring group was managed using the AirView platform. Over the following months, two follow-up visits were scheduled for the usual-care group. Similarly, for the telemonitoring group, two teleconsultations were scheduled along with adjustments in remote CPAP parameters. After 12 months, the total cost per patient was significantly lower in the telemonitoring group than in the usual-care group.
In summary, there is a greater need for a convenient, effective, and low-cost OSAS treatment program. Therefore, TM services should be developed to benefit patients with chronic diseases and facilitate public health emergency responses effectively.
Recommendations and strategies for TM in patients with OSAS
Policy environment optimization
We suggest that the integration of health care and information technology should be accelerated. Moreover, the health care model should be broadened by deeply combining new-generation information technologies, such as cloud computing, big data, Internet of Things, blockchain, and fifth-generation mobile communication, with health and health services. In addition, the government should increase its TM investment and support and formulate more advanced regulations, such as tax incentives and health insurance reimbursement, according to the actual situation. Countries with improved health insurance policies and disease management models, 73 such as the United States, have incorporated home sleep monitoring for OSAS into their health insurance programs. This type of integration can alleviate the imbalance between health care resource development and human resource shortage to a certain extent. As such, the service cost related to OSAS patients receiving TM can be reduced. In addition, the government should increase public awareness and acceptance of TM through appropriate publicity and education.
Individualized treatment plan development
Considering the development of the TM technology thus far, future studies should focus on the development of personalized treatment plans. A personalized OSAS treatment plan should involve a remote assessment–diagnosis–education–support–follow-up system.
Assessment: A comprehensive assessment of the patient condition should include sleep apnea index, oxygen saturation, sleep quality, and quality of life. Oral appliances may be considered for patients with mild or moderate OSAS, whereas surgical treatment or positive pressure ventilation may be recommended for patients with severe OSAS. Health education and self-management: Health education may be provided to patients, including basic knowledge, treatment methods, and self-management skills related to OSAS. Patients may also be encouraged to adopt a reasonable diet and lifestyle and reduce harmful habits such as alcohol consumption and cigarette smoking. Psychological support: Patients with OSAS often encounter psychological issues such as insomnia, anxiety, and depression; therefore, they may be provided with psychological support and treatment. Regular follow-up: Patients are regularly followed up and evaluated to adjust the treatment program in time.
On the basis of different sleep-monitoring data, conditions, and lifestyles of patients with OSAS, health care professionals can accurately adjust treatment strategies, establish personalized health records, formulate personalized treatment plans, and provide home care and community rehabilitation services. This type of personalized treatment may aid in achieving and further optimizing personalized OSAS management comprehensively, improving quality of life and treatment effectiveness, and reducing complications in patients.
Joint family–community–hospital management model construction
In three-tier health care systems, collaborations should be strengthened to construct Internet + health and service information platforms, connecting and providing feedback via a closed-loop model. 74 With the government's policy support, hospitals, community health centers, and families can achieve tripartite information interoperability through a liaison officer. Via a negative feedback mechanism, a family's health care needs are reported to a group of tertiary and community hospitals. These needs are assessed by these tertiary and community hospitals; next, they make the required adjustments and finally provide services and supplemental supplies to the family at one of the tertiary and community hospitals. Figure 4 illustrates this evaluation and feedback mechanism.

Schematic of OSAS hospital–community–family tertiary linkage.
Joint interdisciplinary cooperation and technological innovation
First, cross-sectoral TM service platforms connecting hospitals, sleep centers, and other medical institutions should be established as follows.
Sleep medicine experts should work closely with TM technology providers to develop highly effective remote diagnostic and treatment tools. Hospital respiratory specialists should participate in remote diagnosis and treatment processes to provide professional diagnosis and treatment advice. Medical information technology experts should develop more advanced TM platforms to provide technical support and training. Nursing health management experts should participate in remote diagnosis and treatment processes to provide health management advice and guidance. Artificial intelligence and machine learning technologies may be used to develop highly effective remote diagnostic tools with considerable diagnostic accuracy and efficiency. Advanced remote monitoring equipment should be developed to realize real-time monitoring and recording of patient conditions. Medical big data analysis technology should be employed to provide health care professionals with highly accurate condition analysis and treatment recommendations.
Moreover, research institutions and enterprises should conduct research related to innovation in OSAS TM technology, as well as promote the development and application of the related technologies (e.g. sleep-monitoring equipment and intelligent ventilators), as follows.
Limitations of TM in patient applications
With the rapid development of the TM technology, its application in OSAS patient management has gradually attracted attention. However, when promoting TM services in the elderly population, we often face a series of potential difficulties.
Technical barriers and digital divide. The issue of technological adaptability is key, as older groups are often less receptive to new technologies and unfamiliar with the operation of the Internet and mobile devices, leading them to face technical barriers when using TM services. A survey of the use of smartphones and health apps in Germany found that the use of mobile health apps was correlated with the age of the user, i.e. older people had lower usage than average.
75
Therefore, hospitals and community personnel can provide specialized technical training and support services for elderly patients and their family members through lectures, one-on-one counseling, etc., to help them get familiar with the operation of TM equipment and the use of the Internet, and improve the popularity of TM. Acceptance and trust problems of elderly patients. Some elderly patients are skeptical about the security and effectiveness of TM services, worried about data leakage, misdiagnosis, and other problems, so they are not willing to accept such services. Relevant studies have shown
76
that TM has played a practical role in the field of geriatric health care, but information security problems have gradually emerged, and the personal information of the elderly is stored in the cloud through the network, which is vulnerable to hacker attacks. Therefore, through publicity, education, case sharing and other ways to improve the elderly patients’ awareness and trust in TM services. At the same time, update the privacy security protocol of mobile medical devices; Build more secure direct communication between medical devices and cloud databases to ensure data authenticity, accuracy and integrity; Develop more accurate risk identification procedures to predict unexpected security attacks and ensure that patients’ personal information is not compromised. Legal and regulatory restrictions. Different countries and regions have different laws and regulations on TM services, which limits the development of TM services to a certain extent. Especially in the elderly group, the relevant medical insurance payment system and policy support are not perfect. Therefore, international cooperation and exchanges can be strengthened to promote the formulation and improvement of laws and regulations related to TM services. At the same time, the governments of all countries should increase the investment of funds, strengthen the publicity, improve the medical security system, and expand the TM service from the city to the grass-roots medical service center, so that more elderly patients can get medical services in time.
Conclusion
Traditional medical model requires face-to-face doctor–patient communication, but most patients, especially those in remote areas, often have difficulties in obtaining expert treatment. On the one hand, the lack of medical resources, on the other hand, the traditional medical treatment model is time-consuming and laborious. With the continuous development of information technology and the reformation of medical models, TM technology plays an increasingly crucial role in OSAS diagnosis, treatment, and management. TM enables medical resource integration and optimization, affords patient guidance in home self-management, facilitates optimization of medical continuity service quality, and improves patient treatment compliance and satisfaction. However, TM for OSAS is associated with several limitations, such as data security, privacy protection, health insurance, and conventional concepts of medical care. Future studies focused on resolving the aforementioned issues to improve TM safety and reliability, as well as treatment outcomes and quality of life, among patients are warranted.
Footnotes
Acknowledgments
The authors would first like to sincerely thank the participants of this study. The authors also thank Dr Koda Chen for his help in preparing the figures and tables in this paper and Dr Ke Yang for his help with the arithmetic analysis in this study.
Contributorship
ZRC and PL: conceptualization. ZRC and LJX: writing—original draft preparation. ZRC, LJX, and JXY: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The manuscript has no associated data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
An ethics statement is not applicable because this study is based exclusively on published literature.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Open Fund of Modern Service Industry Research Center of Zhejiang Province, China [grant number SXFJY202202].