
Abstract
Objective
The timely identification of deterioration on general wards is crucial to patient care with each hour of delay independently associated with increased risk of death. The introduction of continuous monitoring of patient vital signs on general wards, currently not standard care, may improve patient outcomes. Our aim was to investigate whether patients on general wards receiving continuous vital signs monitoring have better outcomes than patients receiving usual care.
Methods
Meta-analysis of randomised controlled trials comparing non-critical care patients receiving continuous monitoring of vital signs to usual care. We searched Medline, Embase, and Web of Science, and assessed risk of bias with version 2 of the Cochrane risk-of-bias tool for randomised trials. In addition to measures related to the early detection of deterioration, we planned to present all patient outcomes reported by the clinical trials included.
Results
We included seven trials involving 1284 participants. There were no statistically significant differences in the four outcomes pooled. Comparing continuously monitored to normal care, the pooled odds for hospital mortality, major event/complication, and HDU/ICU admission was 0.95 (95% CI 0.59–1.53, p = 0.84; 660 participants, 3 studies), 0.71 (95% CI 0.38–1.31, p = 0.27; 948 participants, 4 studies) and 0.82 (95% CI 0.25–2.67, p = 0.74; 655 participants, 4 studies), respectively. The mean difference for length of stay was 2.12 days lower (95% CI −5.56 to 1.32, p = 0.23; 1034 participants, 6 studies).
Conclusion
We found no significant improvements in outcomes for patients continuously monitored compared to usual care. Further research is needed to understand what modalities of continuous monitoring may influence outcomes and investigate the implications of a telepresence service and multi-parameter scoring system.
Registration
PROSPERO CRD42023458656.
Introduction
Rationale
The measurement of patient vital signs was gradually introduced into medical practice in the mid to late 19th century. Today it is common to measure heart rate, respiratory rate, blood pressure, oxygen saturation and temperature in clinical settings. Clinicians measure vital signs to provide patients the best possible care, with vital signs used to detect abnormalities, monitor response to interventions and flag early signs of potential deterioration. Highlighting the considerable potential for patient care, research demonstrates patient deterioration is frequently preceded by abnormal vital sign measures. 1
As technology advanced electronic devices to continuously monitor patient vital signs started to appear by the mid-20th century. 2 Today it is standard for critical care patients to have their vital signs continuously monitored, while for patients on general wards, standard care remains the manual periodic measurement every 4 to 6 hours. This can be a problem as patients may experience harmful physiological changes and deteriorate between manual readings.3,4 The timely identification of and response to potential deterioration is critical with one study estimating each hour of delay in admitting a deteriorating patient to intensive care unit (ICU) is independently associated with a 1.5% increased risk of ICU death. 5 It is known that continuous monitoring detects physiological abnormalities that are missed by periodic observations, however, it is not known whether detecting these abnormalities alters outcomes.
Introducing continuous monitoring of patient vital signs on general wards is a potential solution. Patients see the importance of having their vital signs continuously monitored, particularly after-hours, however there are several barriers to implementation. 6 For example, while staff generally appreciate continuous monitoring's potential to enhance patient safety, common issues include perceived increased workload and concerns with ease of technology use. 7 Other barriers include increased false alarms leading to alarm fatigue, patient discomfort with devices, and data capture and storage issues. 3
Researchers from around the world have conducted useful investigations into the application of continuous vital sign monitoring on general hospital wards.3,8–10 A previous systematic review and meta-analysis of observational and experimental evidence found patients continuously monitored experienced some improved outcomes when compared to patients receiving normal care with physiological observations being recorded and documented at fixed intervals. However, the authors concluded there was insufficient evidence of effectiveness to recommend routine use of continuous vital sign monitoring in general wards. 11 Their review included studies published up to June 2014 and since then, significant advancements have been made to wireless monitoring technology and techniques to analyse high-frequency patient data. A more recent systematic review and meta-analysis pooled data from observational and experimental studies published up to August 2020 and specifically focused on the impact of wearable devices for the continuous monitoring of vital signs. 12 This study also concluded there was insufficient evidence of improved outcomes in patients whose vital signs were continuously monitored with wearable devices. However, as this review was limited to studies investigating wearable devices only two randomised controlled trials (RCTs) were included in the meta-analysis.
Objectives
There continues to be rapid advancements in healthcare technology and care delivery to detect, escalate and respond to acute deterioration. As such, the effectiveness of continuous monitoring of vital signs on general wards remains unclear. The purpose of this systematic review and meta-analysis was to address this evidence gap by synthesising the results of RCTs using wearable or traditional devices to continuously monitor vital signs in patients on general wards. Our aim was to systematically search the medical literature for the highest and most recent available evidence, comparing outcomes of patients receiving continuously monitored vital signs to patients receiving normal care. Specifically, we sought to answer the question: What are the patient outcomes reported and associated with continuous vital sign monitoring on general wards?
Methods
We registered our protocol on PROSPERO (CRD42023458656) before commencing our review. We based our study methodology on recommendations from the Cochrane Handbook and reported our results in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Given our systematic review and meta-analysis included data already available in the published literature we did not seek formal ethics approval.
Eligibility criteria
RCTs were eligible for inclusion if they studied inpatients having their vital signs continuously monitored. The comparator group was patients receiving normal care, with intermittent measurement of vital signs. The studies identified needed to be in settings where the continuous monitoring of vital signs is not standard care, that is non-critical care units or recovery wards. To meet inclusion criteria the studies also needed to measure at least one patient outcome. We excluded studies not published in the English language. Our study group of interest was participants receiving continuous vital signs monitoring. We defined this as patients having at least two vital signs (heart rate, respiratory rate, oxygen saturation or temperature) automatically measured in a continuous manner.
Information sources
Searches were conducted in Medline and Embase (both on the OVID platform) and the Web of Science Core Collection on 5 October 2023. All databases were searched from inception to October 3, 2023. Forward citation chasing of a set of 12 gold standard papers was undertaken using Citation Chaser. 13 Table S1, Supplementary Material lists the publications to which citation searching was applied.
Search strategy
Two experienced health librarians (GJ, SH) developed the search strategies using a combination of free-text (keyword) and thesaurus terms, and this process underwent internal peer review by a third senior librarian. The initial search was developed for Medline and tested against an identified set of 12 gold standard papers (Table S1, Supplementary Material) and subsequently transposed to Embase and Web of Science. The searches were constructed around the concepts of continuous monitoring, vital signs, and general ward inpatients. The searches prioritised sensitivity to maximise retrieval of relevant records with regards the first two concepts; and were adjusted to balance sensitivity and precision with regards to retrieving studies pertaining to inpatients on general hospital wards.
Searches were limited to RCTs. For the Medline search this was done by applying the Cochrane Highly Sensitive Search Strategy for identifying randomised trials in MEDLINE: sensitivity maximising version (2008 revision). 14 For the Embase search the ISSG Embase RCT filter was applied. 15 The full search strategies for all databases are available in Table S2, Supplementary Material.
Selection and data collection process
Two of the study authors (KT, LT) independently screened the 5108 titles and abstracts returned by the literature search. A third author (TB) independently reviewed a random sample of 700 titles and abstracts. Studies that did not meet inclusion based on the pre-defined eligibility criteria were excluded. Details on the reason for exclusion are available in Table S3, Supplementary Material. Disagreements were first resolved through discussion, followed by resolution with a third independent party. Two authors (KT, LT) performed the data collection process, independently extracting data from eligible RCTs and entering these on standardised data extraction forms. All disagreements arising from the data extraction were resolved by discussion.
Data items
The main outcome initially chosen was any measure related to the early detection of deterioration. In addition, we planned to report all additional patient outcomes which we expected to include mortality, morbidity, ICU transfer, length of hospital stay and length of ICU stay. We used a pre-defined electronic form to extract data on study author details, year of publication, intervention group details, comparison group details, inclusion and exclusion criteria, clinical setting, total number of participants randomised, vital signs measured, subgroups reported and information needed to assess the risk of bias.
Study risk of bias assessment
Two authors (KT, LT) independently assessed the risk of bias in the included studies using Version 2 of the Cochrane risk-of-bias tool for randomised trials (RoB 2). This assessment was done using the RoB 2 electronic tool. 16 In this tool, bias is assessed for each outcome in five distinct domains (randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result), with bias judged as ‘low risk of bias’, ‘some concerns’ or ‘high risk of bias’. These domain level judgements lead to an overall risk-of-bias judgement for each study outcome.
Effect measures and synthesis methods
We reported dichotomous outcomes as odds ratios (95% confidence intervals [CIs]), and continuous outcomes as mean differences (95% CIs). We planned to synthesise results through meta-analysis where at least three studies reported the same outcome. This decision was consistent with a previously published systematic review and meta-analysis. 11 Where studies did not present standard deviations for continuous outcomes, we planned to obtain them from standard errors or CIs for group means. Where studies presented continuous outcomes as median, minimum, maximum or interquartile range values we estimated the mean and standard deviation of the sample applying techniques described in the literature.17,18
Statistical analyses were performed using Review Manager Web (RevMan Web, Version 4.12.0, The Cochrane Collaboration). For our meta-analysis we chose to apply a random-effect meta-analysis model as we expected some heterogeneity between study populations and definitions of outcomes. For binary outcomes we chose the Mantel–Haenszel method to calculate pooled odds ratios (95% CI), and for continuous outcomes we applied the inverse-variance method and reported the pooled mean difference (95% CI). We examined heterogeneity among pooled studies using the I2 statistic and the Chi2 test, and as a rough guide considered Chi2 test p-value above 0.10 and an I2 statistic under 30% to suggest heterogeneity may not be important. As we identified fewer than 10 studies for inclusion, we did not visually assess the risk of reporting bias using a funnel plot.
Results
Study selection
Figure S1, Supplementary Material summarises the number of studies identified, screened for eligibility and included in our systematic review. After duplicates were removed, our literature search returned 5108 article titles and abstracts, of which 5064 were excluded. Following this, 44 full-text articles9,19–58 were retrieved and assessed for eligibility and 37 excluded for not meeting our inclusion criteria. More details on exclusion reason are available from Table S3, Supplementary Material. This left 7 RCTs meeting the criteria for inclusion in our review.36,37,48,54,55
Study characteristics
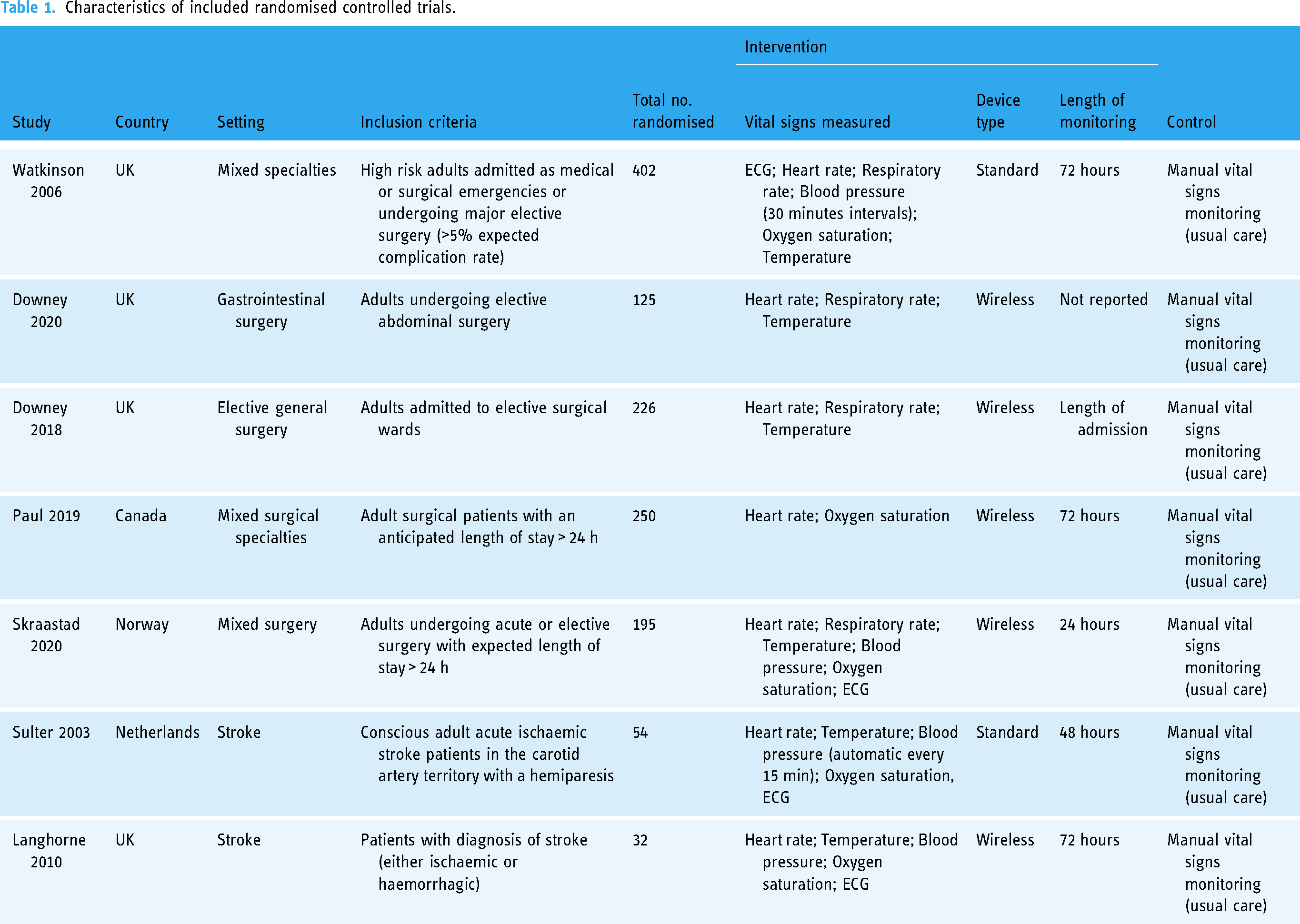
Overall, the seven RCTs included in our review randomised a total of 1284 patients in general wards across the UK, Canada, Norway and The Netherlands. Of these 664 were randomised to continuous vital sign monitoring and 620 were allocated to usual care. The characteristics of included studies are presented in Table 1. Four of the studies were conducted in surgical patients,36,37,48,54 one was conducted in a mixed medical/surgical population 55 and two were in the stroke setting.59,60 The vital signs continuously measured differed between studies. Two studies54,55 measured ECG, heart rate, respiratory rate, blood pressure and oxygen saturation, two studies36,37 measured heart rate, respiratory rate and temperature, two studies59,60 measured ECG, heart rate, temperature, blood pressure, oxygen saturation and one study 48 measured heart rate and oxygen saturation. The control arm in all studies was normal care, with intermittent measurement of vital signs. The length of continuous monitoring ranged from 24 hours, 54 to the length of patient admission. 36 One study did not report the length of time patients were monitored. 37 Five of the seven trials randomised patients to receive continuous monitoring from wireless devices.36,37,48,54,59
Characteristics of included randomised controlled trials.
A total of 38 patient outcome measures were reported by the included studies. Table S4, Supplementary Material lists all the patient outcomes along with their definitions. The most common patient outcomes were length of stay (n = 6),36,37,54,55,59,60 major events/complications (n = 4) as defined by the study authors,36,37,54,55 HDU/ICU admissions (n = 4)36,37,48,60 and in-hospital mortality (n = 3).36,55,59 The definition of major complications/events varied from Clavien-Dindo score >2 in two studies36,37; unconsciousness, seizure, or stroke in one study 54 ; and urgent staff calls, a change to a higher care level, cardiac arrest or death in 96 hours following randomisation in one study. 55
Risk of bias in studies
We assessed the risk of bias for the 38 individual outcomes included in the seven studies reporting patient outcomes included in this review. The risk of bias assessment for each outcome within each study is available in Figure S2, Supplementary Appendix. In general, we assessed the overall risk of bias to be either ‘some concerns’ (n = 33, 86.8%) or ‘low’ (n = 5, 13.2%). No outcomes were assessed as ‘high risk’ of bias (Figure 1). The risk of bias assessment for outcomes synthesised by meta-analysis are included in the forest plots and are represented using the traffic light system.

Risk of bias 2 assessments for 38 outcomes reported by 7 randomised controlled trials. Assessed using version 2 of the Cochrane risk-of-bias tool for randomised trials (RoB 2).
In-hospital mortality
Data on in-hospital mortality were provided in three of the seven studies included in our review.36,55,59 Overall, these three studies reported 42/357 (11.8%) events in the continuously monitored group and 43/303 events (14.2%) in normal care group. The pooled odds ratio for in-hospital mortality was 0.95 (95% CI 0.59–1.53, p = 0.84) times lower in the group receiving continuous monitoring to the group receiving normal care (Figure 2).

In-hospital mortality in patients receiving continuous monitoring for vital signs versus normal care.
Major events/complications
Data on major events/complications were provided in four out of the seven studies included in our review.36,37,54,55 One study reported significantly fewer major events/complications in the continuously monitored group, 37 the remaining three reported no statistically significant differences between groups.36,54,55 Overall, these four studies reported 125/497 (25.2%) events in the continuously monitored group and 136/451 events (30.1%) in the normal care group. The pooled odds ratio for a major event/complication was 0.71 (95% CI 0.38–1.31, p = 0.27) times lower in the group receiving continuous monitoring to the group receiving normal care (Figure 3).

Major events/complications (as defined by the included studies) in patients receiving continuous monitoring for vital signs versus normal care.
Length of stay
Six studies presented data on hospital length of stay.36,37,54,55,59,60 One study reported significantly shorter length of stay in the continuously monitored group. 60 Of the remaining studies, three reported shorter mean length of stay in the continuously monitored group when compared to normal care,36,37,54 while two reported longer mean length of stay,55,59 however, none of these were statistically significant. The pooled mean difference for length of stay was shorter in the continuously monitored group (mean difference −2.12 days, 95% CI −5.56 to 1.32, p = 0.23) (Figure 4).

Length of hospital stay in patients receiving continuous monitoring for vital signs versus normal care.
HDU/ICU admissions
Data on HDU/ICU admissions were available from four studies.36,37,48,60 These four studies each reported no statistically significant differences in HDU/ICU admissions between groups. The pooled odds ratio for HDU/ICU admission was 0.82 (95% CI 0.25–2.67, p = 0.74) times lower in the group receiving continuous vital sign monitoring when compared to the group receiving normal care (Figure 5).
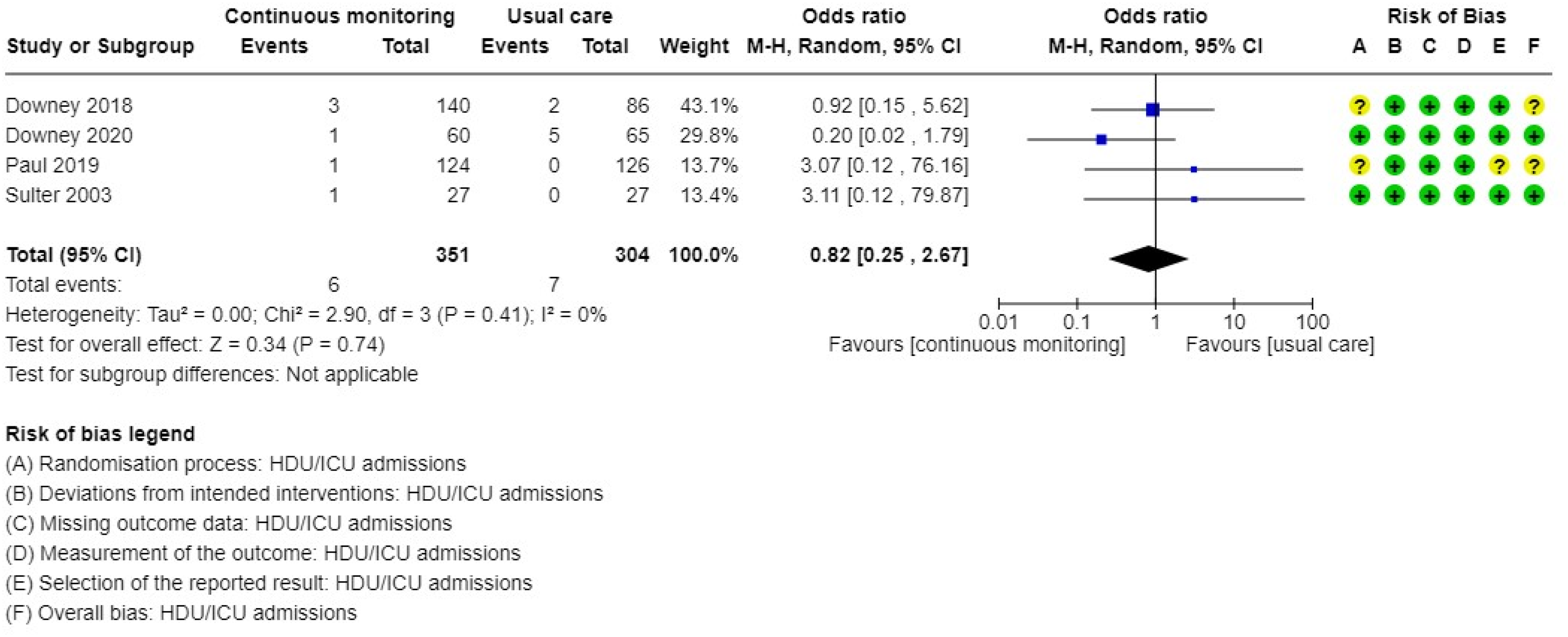
HDU/ICU admission in patients receiving continuous monitoring for vital signs versus normal care.
Other patient outcomes
We did not pool the results for any other patient outcomes reported in the included studies. Complications (as defined by the study authors) and 30-day readmissions were available in two studies each and therefore did not meet our minimum criteria for data synthesis.36,37,59
For the outcome of any complications (as defined by the study authors) 111/156 had an event in the continuous monitoring group and 63/102 had an event in the intermittent group,36,59 30-day readmissions were 22/200 versus 23/151.36,37 Other outcomes extracted including sepsis, time to antibiotics for sepsis, cardiac arrest team activation, mortality (96 hours and 30-day), supplementary oxygen, time to mobilisation, minor complications, Barthel Index (5-day and 90-day), and respiratory events were only available in one study and therefore could not be pooled. These results are available in Table S4, Supplementary Material.
Subgroup analysis – continuous monitoring using wireless devices
There were no statistically significant differences in patient outcome between the continuous monitoring of vital signs using wireless devices and traditional devices. Occurrences of major events/complications was reported in three studies using wireless continuous monitoring technology.36,37,54,59 The pooled odds ratio for a major event/complication was 0.49 (95% CI 0.19–1.26, p = 0.14) times lower in the group receiving continuous monitoring, to the group receiving normal care (Figure S3, Supplementary Appendix; test for subgroup differences: Chi2 = 1.55, df = 1, p = 0.21). Four studies using wireless continuous monitoring presented data on hospital length of stay.36,37,54,59 The pooled mean difference for length of stay was 0.53 days (95% CI −1.99 to 0.93, p = 0.48) shorter in the continuously monitored group (Figure S4, Supplementary Appendix; Test for subgroup differences: Chi2 = 0.47, df = 1, p = 0.49). Three studies with wireless continuous monitoring presented data on HDU/ICU admission. The pooled odds ratio for HDU/ICU admission was 0.67 (95% CI 0.18–2.53, p = 0.55) times lower in the group receiving continuous monitoring to the group receiving normal care (Figure S5, Supplementary Appendix; test for subgroup differences: Chi2 = 0.74, df = 1, p = 0.39).
Discussion
Our systematic review and meta-analysis included seven clinical trials randomising 1284 inpatients to continuous vital sign monitoring or usual care on general wards. The pooled results from our meta-analyses suggest that inpatients receiving continuous monitoring were not less likely to experience in-hospital mortality, have major complications, shorter length of hospital stay or fewer HDU/ICU admissions. However, this conclusion is limited by the low number of studies, relatively low event rate and variability in outcomes reported.
Our results are consistent with previous systematic reviews. A meta-analysis by Areia et al. pooled the results of seven studies and 4127 participants, and reported no statistically significant reductions in mortality (RR 0.48, 95% CI 0.18–1.29), major complications (RR 0.55, 95% CI 0.24–1.30), ICU admission (RR 0.87, 95% CI 0.66–1.15), or mean length of stay (mean difference, −0.09, 95% CI −0.43 to 0.44) with continuous monitoring. 12 Like our results however, these non-statistically significant results favoured continuous monitoring. The main difference between Areia et al. and our study is that they restricted their analysis to wireless monitoring devices and included non-randomised trial designs. A further previous study by Sun et al. pooled nine studies and 12,721 participants and looked at a wide range of devices to continuously monitor vital signs including wired and wireless. They reported a statistically significant reduction in mortality (RR 0.61, 95% CI 0.39–0.95), and non-statistically significant reductions in ICU admission (RR 0.86, 95% CI 0.67–1.11) and mean length of stay (mean difference −3.32, 95% CI −8.82 to 2.19). Their study however did include studies with a higher risk of bias. 61
Limitations of the evidence
Significant questions nonetheless remain regarding the outcomes from continuous monitoring. The best patient outcome to measure remains unclear and was variable among the studies identified. The trial providing the largest number of outcome events 55 used a composite outcome, which included urgent escalation calls, as well as cardiac arrests, unplanned ICU transfer or death. The authors conducted a post-hoc analysis separating potentially beneficial events (such as unscheduled escalation to senior medical staff or critical care outreach), from adverse events such as cardiac arrest, with no significant difference identified between the monitoring and standard care groups. When excluding this RCT from our subgroup analysis, the point estimate for major complications favoured the continuously monitored group, though this was not statistically significant. This may be due to the very low number of events remaining after excluding the potentially beneficial ones and therefore benefit from continuously monitoring patients in non-critical care wards cannot be ruled out.
The RCTs included in our review used different combinations of continuous monitoring modalities, and it is possible that different modalities may have different outcomes. There is also uncertainty around the optimal duration of monitoring. One study used a monitoring period of 24 hours, and although two studies48,55 aimed to apply the monitoring for 72 hours, in one of those trials only 16% of patients were able to be monitored for this whole duration and 39% were monitored for 24 hours or less. 55 It is possible that this short monitoring period, out of an average hospital length of stay of 3 to 22 days in the various studies, is not adequate to detect a high enough proportion of adverse events to meaningfully alter outcomes.
Another limitation is that the RCTs identified used different inclusion criteria. The largest trial included patients with a calculated risk of death greater than 5%, where the other trials did not specify high risk. The theoretical benefit of continuous monitoring is that early deterioration can be detected and acted upon. It is possible that this benefit is reduced in patients who are already identified as high risk, as they will already be receiving enhanced care. In addition to risk of death, the trials varied in the patient cohort, from elective surgical to stroke to mixed populations.
Monitoring is widely used and generally regarded as safe. The devices used are validated and generally accurate. One study 46 described statistically significant increases in the rate of detection of adverse physiology, including hypotension and hypoxia, without significant changes in the rate of interventions. Alterations in physiology are known to predict patient deterioration. It is therefore unclear why continuous monitoring would not improve outcomes. There are several possible explanations, some of which were addressed in the identified studies.
The monitoring of physiological observations occurs as part of a chain of response, in which as a first step the abnormality must be recognised as such. Unfortunately, the application of continuous monitors to patients who are mobile can create significant volumes of false alarms. This can occur due to interference from movement, or transient physiological changes associated with patient activity such as movement or coughing. It is possible that the resulting alarm fatigue would result in failure of recognition of true abnormalities. A solution to this proposed in one study was the use of a multi-parameter track and trigger system. 55 The National Early Warning Score (NEWS) was used in three of the studies published since 2006, without a significant difference in outcomes observed.
The included RCTs focused on abnormalities detected through continuous monitoring of vital signs, however in addition to the detection of a change in physiology, a robust response to this change must occur. No studies investigated the impact the presence of a medical emergency team (MET) could have had on outcomes. None of the included studies explicitly discussed the effector arm of the monitoring system- who was informed of the monitoring abnormality, and whether there were set responses to abnormalities. The implementation of MET services is now widespread, however, the effect of a MET service on outcomes from continuous monitoring is still unclear. It could act to reduce the effect of the intervention by improving the reliability of response in the control group, or it could enhance the intervention by clear escalation of abnormalities.
A variant of the ‘eICU’ model was proposed as a solution in one study. 55 This would consist of a remote presence that can act to minimise the number of false alarms by filtering the noise and informing bedside staff of true, actionable alerts. With recent improvements in technology, telehealth systems with a remote presence can act directly on physiological changes to treat developing problems or escalate concerns as appropriate to ward teams. This would therefore act to improve the ability of the continuous monitoring to detect true abnormalities, and to respond appropriately to those abnormalities.
Implications for practice, policy and future research
Our meta-analysis is novel in that it restricted analysis to RCTs, which are considered the gold standard in clinical research. Furthermore, as a recently conducted systematic review, it provides an important update of the current literature incorporating the most recent technological advancements in continuous vital signs measurements. When interpreted with other research, the findings from of our systematic review and meta-analysis are important. Our investigation addresses a gap in current clinical practice as continuous monitoring of vital signs is not routinely performed outside critical care settings. This is a significant issue for inpatient care as high-risk patients on general wards can deteriorate unexpectedly between periodic vital sign recordings, and therefore has implications for safety and quality standards and clinical guidelines. 62
Current guidelines do not recommend the continuous monitoring of vital signs outside critical care settings and our results do not provide evidence to warrant a change in clinical practice. However, the point estimates for patient outcomes consistently favour continuous monitoring (albeit not statistically significant), and the continuous monitoring technology is improving rapidly. Therefore, it is possible that as more clinical trials are published, and meta-analyses with larger sample sizes are conducted, the results may favour continuously monitoring high-risk patients on general wards over manual intermittent monitoring. In this context our findings may encourage policymakers to consider reviewing and updating guidelines at frequent intervals as new evidence emerges to ensure they are up to date and reflect recent technological developments.
Our meta- analysis has not demonstrated overall benefit to clinical outcomes from continuous monitoring. However, the CIs include benefit, and there remains significant heterogeneity in patient populations who may benefit. Significant research questions remain, including:
What modalities of continuous monitoring have most beneficial effect on outcomes? Which patient groups are most likely to benefit from continuous monitoring? Does the addition of a telepresence service to maintain and filter the continuous monitoring, and action the results, alter the benefits of continuous monitoring? Does the development of multi-parameter scoring systems utilising the continuous monitoring, where false alarms are filtered, improve the outcomes associated with continuous monitoring? Where multi-parameter models are used, which is most effective, and which elements are most important? Current multi-parameter models look at multiple parameters at a single time point. How does the use of time averaged or time-trend data alter the performance of multi-parameter models? What are the health economic implications of implementation of continuous monitoring systems, and are they cost effective in improving patient-orientated or health service orientated outcomes?
A fundamental problem with studying any monitoring modality is that the monitoring in isolation forms only part of a clinical process, which extends from alteration in patient state, detection of that alteration, activation of a response, to confirmation of resolution of alteration or escalation of care if needed. Changes to one element- the monitoring, is unlikely to be effective unless matched by an appropriate response. We would recommend future research includes a response system, as well as detection. In this context, future trials of the intervention are unlikely to be feasible at individual patient level and will likely require ward or hospital level randomisation.
Conclusion
We found no significant improvements in outcomes for patients continuously monitored compared to normal care. However, this conclusion is limited by the low number of studies, relatively low event rate, and variability in outcomes reported. As vital sign monitoring technologies continue to advance, and more clinical trials and meta-analyses are conducted there may be some patient groups where continuous monitoring is proved beneficial. More research is needed to understand what modalities of continuous monitoring may influence outcomes and investigate the implications of a telepresence service and multi-parameter scoring system.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241288826 - Supplemental material for Outcomes in patients receiving continuous monitoring of vital signs on general wards: A systematic review and meta-analysis of randomised controlled trials
Supplemental material, sj-docx-1-dhj-10.1177_20552076241288826 for Outcomes in patients receiving continuous monitoring of vital signs on general wards: A systematic review and meta-analysis of randomised controlled trials by Tim Bowles, Kevin M. Trentino, Adam Lloyd, Laura Trentino, Glynis Jones, Kevin Murray, Aleesha Thompson, Sarah Halpin and Grant Waterer in DIGITAL HEALTH
Footnotes
Acknowledgments
The review authors would like to acknowledge the contributions of the senior staff of the Library & Information Service for the South and East Metropolitan Health Services for the peer review of the primary search strategy.
Contributorship
TB and KT designed, developed and refined the study protocol with contributions from AL, GW. TB, KT, GJ, SH developed the search strategy and conducted the literature search. KT and LT screened titles and abstracts and undertook the data extraction. TB, KT, AL, LT, AT, KM, GW interpreted the data for the work; TB, KT drafted the manuscript. All authors were involved in critically revising the draft; All authors approved the final version to be published.
Declaration of conflicting interests
Ethical approval
Ethics approval and patient consent for publication was not required as all data retrieved and analysed was publicly available and sourced from previous published studies in which informed consent was already obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
TB is the manuscript guarantor and is willing to take full responsibility for the article, including for the accuracy and appropriateness of the reference list.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.