
Abstract
Purpose
The objective of this study was to assess the accuracy of FreeStyle Libre Pro (FSL-Pro) flash continuous glucose monitoring (CGM) in patients with type 2 diabetes mellitus (T2DM) and acute myocardial infarction (AMI).
Methods
A single-arm, single-center prospective study was conducted in the cardiac care unit from January 2021 to September 2023. Patients underwent finger-prick blood glucose (FPBG) testing before breakfast (6:00 am) and after meals (at 9:00, 13:00, 19:00 pm), along with CGM during their hospitalization. Statistical analyses included mean differences (MDs), mean absolute relative difference (MARDs) of blood glucose levels, and hypoglycemia occurrences. A Bland–Altman plot analysis and Pearson correlation were performed.
Results
Ninety-seven T2DM and AMI patients underwent CGM for up to 72 h (1142 monitoring point). Mean daily BG, Fasting plasma glucose (FPG) and mean postprandial plasma glucose (PPG) were significantly lower by CGM than by FPBG with an estimated MD of −0.89 mmol/L in BG, −0.88 mmol/L in FPG, and −0.90 mmol/L in PPG, respectively. The maximum effect was mainly in the first day and then the difference was gradually declined (falling range, Day1, −1.24; Day 2, −0.70; Day 3, −0.68, mmol/L, respectively). The incidence rates of hypoglycemia and potential hypoglycemia was 1.57% and 8.5% higher, respectively, in CGM than in FBPG. A Bland–Altman Plot revealed some variability and bias between the two methods of measurement of glucose monitoring (p < .001). Pearson's correlation coefficient demonstrated a significant correlation between the mean BG, FPG, and PPG of CGM and FBPG (Pearson's coefficient: 0.92, 0.87, 0.92, respectively, p < .001).
Conclusion
Compared with FPBG, FSL Pro-CGM showed lower mean glucose and higher hypoglycemia detection in T2DM and AMI patients, especially in the first 24 h.
Keywords
Introduction
Acute myocardial infarction (AMI) continues to be a serious medical emergency linked to substantial morbidity and mortality. 1 Dysglycemia, encompassing stress hyperglycemia, hypoglycemia, and glycemic fluctuations, plays a crucial role in determining the clinical outcomes of patients with AMI. 2 For the majority of critically ill patients in the coronary care unit (CCU) with persistent blood glucose concentrations exceeding 10·0 mmol/L (>180 mg/dL), it is recommended to initiate insulin therapy with a target range of 7·8–10·0 mmol/L (140–180 mg/dL) to prevent complications associated with hypoglycemia and hyperglycemia. 3 Continuous intravenous insulin (CII) therapy is generally recommended for critically ill patients as it enables rapid adjustment of insulin doses to maintain blood glucose levels within a narrow target range. 4 While this approach is effective, it places a significant burden on nurses, as it typically involves hourly testing of point-of-care glucose values for treatment adjustments. 5 Additionally, during the patient management process, we observed that hourly fingertip blood glucose monitoring led to low patient tolerance. 6 Our previous experiences with a multidisciplinary blood glucose management team, comprising physicians, pharmacists, nurses, and other medical staff, have been beneficial in reducing glucose fluctuations and achieving glucose targets in patients with diabetes and AMI.6–8 Noninvasive health monitoring, including continuous glucose monitoring (CGM) using biocompatible conjugated polymers, offers convenient, real-time, and reliable blood glucose monitoring. 9 CGM devices were first utilized in the intensive care unit for closed-loop control of blood glucose in 2002. 10 Subsequently, they have been validated as a safe tool for detecting trends in glucose levels and predicting impending glucose excursions in ST-segment elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary interventions (p-PCI). 11 The FSL-Pro CGM is a CGM device that can provide real-time blood glucose monitoring. It utilizes a sensor placed on the outer side of the upper arm to continuously collect blood glucose data for a period of 14 days. 12 Previous studies have evaluated the accuracy of flash CGM in hospitalized patients, but a limited number of subjects (13 12 and 89 patients 13 ), and relatively simple disease state (type 2 diabetes mellitus (T2DM) without complicated chronic diseases 14 or stress hyperglycemia without diabetes 13 ) are the main shortcomings of these studies. Although a similar study 11 evaluated the feasibility and safety of CGM in STEMI patients, this study included patients without diabetes and the risks of hypoglycemia and hyperglycemia are relatively lower in patients without diabetes than in those with diabetes. As shown in Figure 1, CGM and FBPG each have their own advantages and disadvantages. The accuracy of CGM in diabetic patients with AMI remains unknown, thus, evaluating the accuracy of CGM in these critically ill patients is crucial. Given these reasons, our study aimed to address these gaps by specifically investigating patients with both STEMI and T2DM, as we know higher blood glucose fluctuations and risks of hypoglycemia may affect the accuracy of CGM. The accurate monitoring of glucose levels in these critically ill patients is crucial for their care. Therefore, we conducted a comparison to evaluate the performance and efficacy of the FSL-Pro CGM relative to FBPG in patients with diabetes and AMI.

The importance of the study and schematic figure.
Materials and methods
Study population
The eligibility criteria for the study were as follows (1) a diagnosis of diabetes, (2) a diagnosis of AMI, including both STEMI and non-STEMI (NSTEMI), (3) treatment with oral or intravenous antihypoglycemic drugs, (4) CGM and finger-prick blood glucose (FPBG) monitoring was needed, (5) a minimum length of stay of 3 days, (6) age 18 years or older. Patients were excluded if they refused blood glucose monitoring. The study was approved by the ethics committees of Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine (KY2019-076). Written consent was obtained from all subjects or their legally authorized representatives (in case of minors) prior to study initiation. Since our studies did not include minors, it was not necessary to obtain written consent from minors. All informed consent forms have been provided to the journal office.
Study procedures
As for CGM monitoring, sensors of FSL-Pro flash were placed by the study team in the posterior upper arm following manufacturer recommendation and under an aseptic technique. The study team checks each sensor daily to make sure the placement and functional status for up to 14 days or until they were discharged. All CGM sensor data was downloaded after hospital discharge. All glucose values were exported into standard Excel data files for further statistical analysis by the study team. FPBG monitoring was conducted at four monitor sites, including before breakfast (6:00 am) and after meals (9:00, 13:00, 19:00 pm). Diabetes management was conducted by the research team, targeting glucose levels between 70 and 180 mg/dL.15,16
Outcomes measures
Our primary end point was the comparison between FPBG and CGM on glycemic control metrics among hospitalized patients, including mean daily glucose (mean BG, mean FPG, breakfast PPG, lunch PPG, dinner PPG, and mean PPG), the first day, second day and third day mean glucose, hypoglycemia (defined as blood glucose less than 3.9 mmol/L), potential hypoglycemia (defined as blood glucose less than 7.8 mmol/L, for patients with T2DM and AMI). 8
Principles of Freestyle Libre Pro flash CGM
The principles of FreeStyle Libre Pro flash CGM are mainly based on Radio Frequency Identification (RFID) technology. The sensor communicates with the reader through RFID, allowing the information stored in the sensor to be read when in proximity to the reader. It mainly consists of a glucose electrode, an RFID chip, and a waterproof casing. Its electrode uses a technology involving a wired enzyme, which is a special enzyme that can continuously measure glucose in tissue fluid. This dynamic technology automatically measures blood glucose once per minute and records it every 5 min, resulting in 288 data points per day, effectively monitoring both high and low blood glucose levels. In this study, patients with T2DM complicated with AMI were included, many of whom experienced stress-induced hyperglycemia and required hourly blood glucose monitoring. Therefore, this technology was employed for blood glucose monitoring in these critically ill patients.
So far, there are three CGM technologies widely used in clinical practice, including FreeStyle Libre, Dexcom, and Guardian Connect. A comparison of key parameters of these devices is presented in Supplemental Table S1. We primarily used the FreeStyle Libre in this study due to its early approval date in 2016, longest service life of up to 14 days, high sensitivity, and compact product size. We are currently utilizing the hospital version of the FreeStyle Libre, which still acquires data through scanning. When the second and third generations are launched in the future, we will upgrade to the latest versions.
Data analyses
Continuous variables were described in terms of mean with standard deviation (SD) and compared by unpaired Student's t tests or Mann-Whitney U tests. Categorical variables were described as number and percentage and compared by chi-square test or Fisher's exact tests. Baseline data analysis was performed using the SPSS software, version 22.0 (SPSS Inc., Chicago, Illinois, USA), and p < .05 was considered significant. The Pearson correlation coefficient and Bland–Altman analysis were conducted by MedCalc. This method provides mean bias, SD, and 95% confidence intervals (CIs) based on the differences between CGM and FBPG. The mean difference (MD) represents the discrepancy between the average values obtained from the tests conducted to assess the difference between CGM and FBPG. Mean absolute relative difference (MARD) is a statistical metric used to quantify the discrepancy between two sets of data, serves as a measure of the accuracy of blood glucose monitoring systems. The formula for calculating MARD is listed as follows:

Results and discussion
Patients’ characteristics
The baseline characteristics of patients are presented in Table 1. A total of 97 hospitalized cases with diabetes and AMI were included in the study, 1142 monitoring events were completed and matched. Among the cases, 78.4% of the patients were male, 81.4% (79/97) of the patients were hospitalized for STEMI, 18.6% (18/97) of the patients for Non-STEMI. The mean age, BMI, HbA1c%, admission insulin, duration of diabetes, length of CCU stay were 63.5 years, 25.3 kg/m2, 7.9%, 10.7 uIU/ml, 7.4 years, 10.1 days, respectively.
Study participant characteristics.
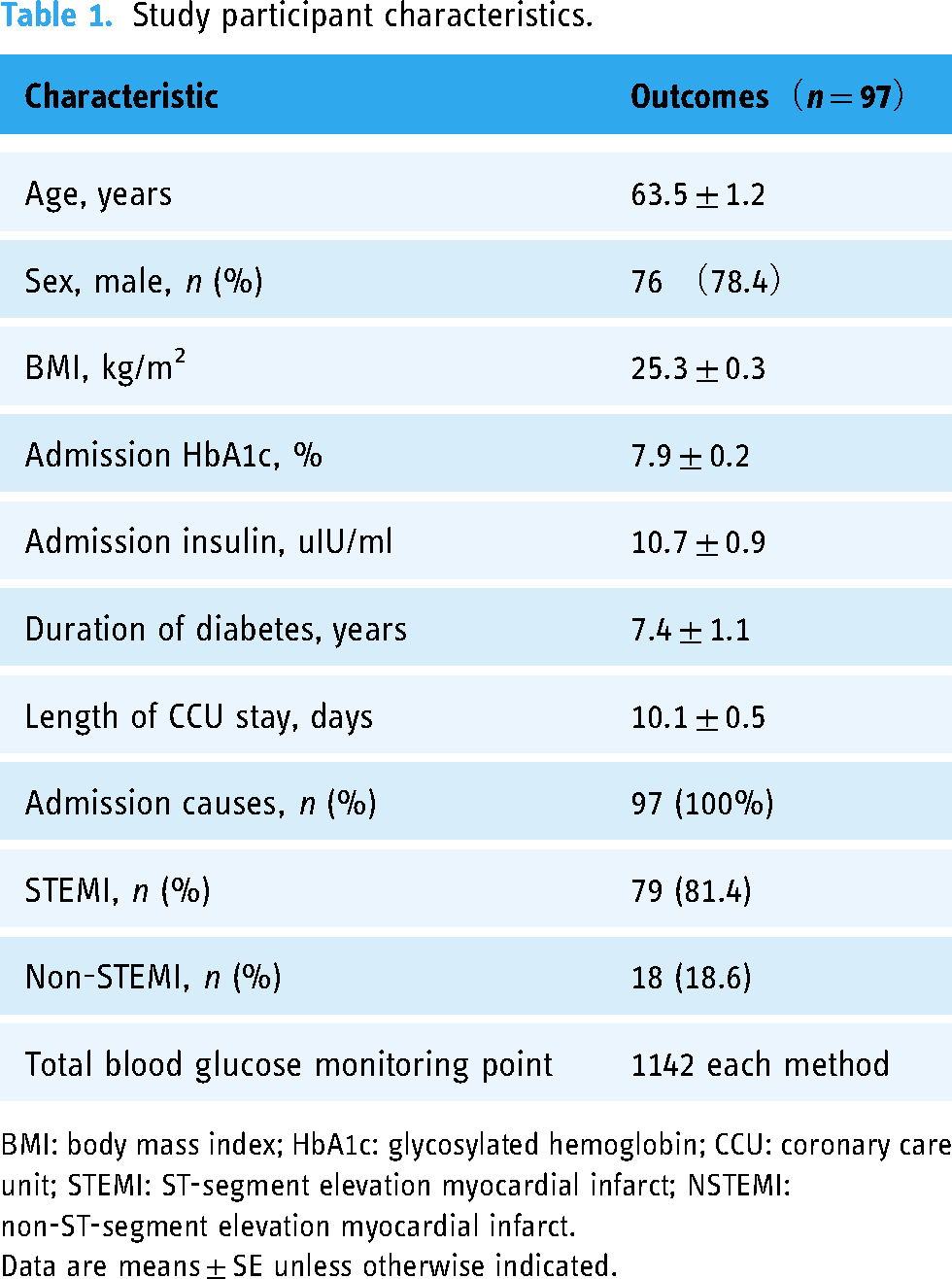
BMI: body mass index; HbA1c: glycosylated hemoglobin; CCU: coronary care unit; STEMI: ST-segment elevation myocardial infarct; NSTEMI: non-ST-segment elevation myocardial infarct.
Data are means ± SE unless otherwise indicated.
Blood glucose between CGM and FBPG in 72 h of admission
In general, the mean blood glucose in CGM group was lower than in FBPG group. Table 2 provides details of the differences between CGM and FBPG. Specifically, mean BG were 10.4 mmol/L in CGM group and 11.3 mmol/L in FBPG group, indicating a −0.89 mmol/L difference. Similar downward trends have been described for mean FPG and PPG in CGM group as compared to FBPG group (FPG, M ± SE, mmol/L, 7.5 ± 0.2 vs 8.3 ± 0.2; PPG, 11.4 ± 0.3 vs 12.3 ± 0.3, respectively), and there was a significant difference (p < .001). After further analysis, we found the greatest difference in blood glucose only after breakfast, followed by after dinner, and finally after lunch, with differences of 1.03, 0.92, and 0.75 mmol/L (p < .001). It is worth noting that the MARD was similar between 6.6 and 8.2, except for mean FPG, the MARD was 10.6%.
Blood glucose between CGMs and FBPG in 72 h of admission
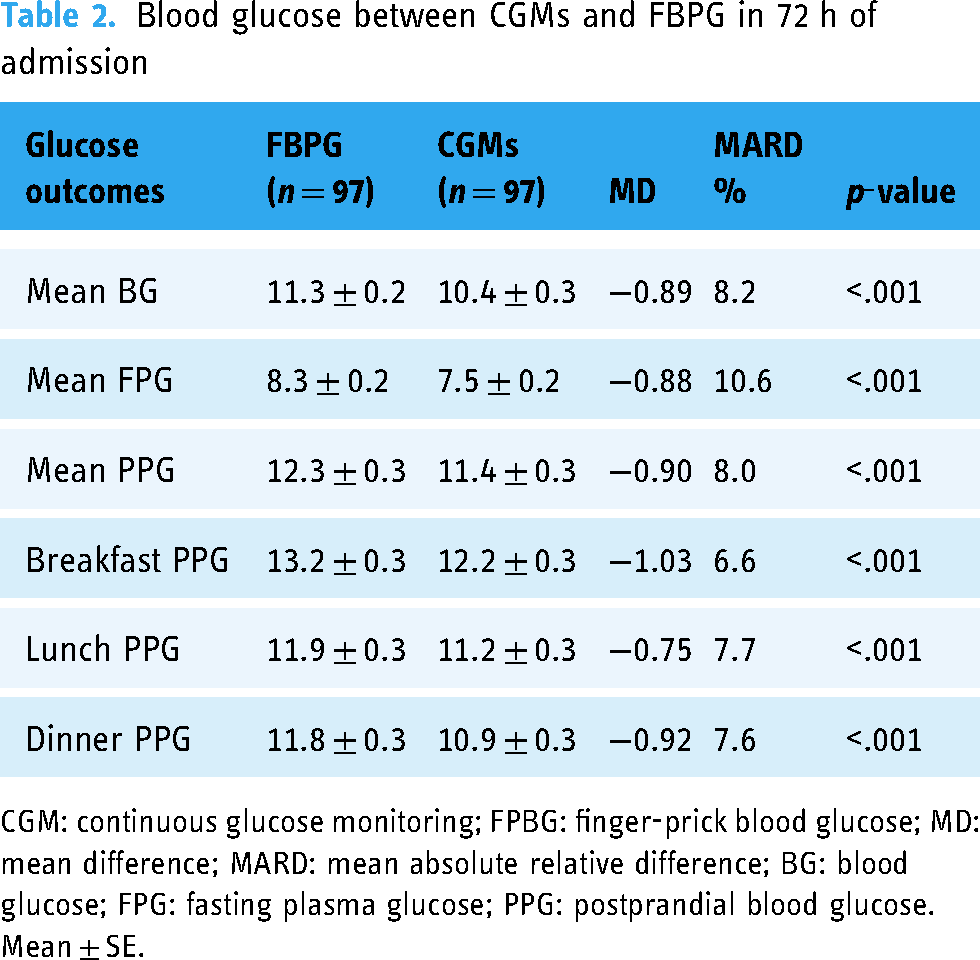
CGM: continuous glucose monitoring; FPBG: finger-prick blood glucose; MD: mean difference; MARD: mean absolute relative difference; BG: blood glucose; FPG: fasting plasma glucose; PPG: postprandial blood glucose.
Mean ± SE.
Blood glucose and hypoglycemia times between CGM and FBPG groups are outlined in Table 3. Following the monitoring in 3 days (72 h), the mean blood glucose in the first day (with 24 h) was much lower in the CGM group than in the FBPG group (Day 1, M ± SE, mmol/L, 10.6 ± 0.3 in CGM group, and 11.8 ± 0.3 in FBPG group, p < .001). As the monitoring time progressed, the differences in blood glucose gradually narrowed (M ± SE, CGM vs FBPG group, mmol/L, 10.4 ± 0.3 vs 11.1 ± 0.3 in the second day, 10.3 ± 0.3 vs 11.0 ± 0.3 in the third day). Additionally, the MARD were consistent with the primary outcomes, the MARD was bigger in the first day (10.9%) than the second and third day (6.2–6.3%). For patients with AMI, the better blood glucose management should aim for a target range of 7.8–10 mmol/L, blood glucose less than 7.8 mmol/L may increase the risk of potential hypoglycemia. The times of hypoglycemia and potential hypoglycemia were higher in the CGM group than in the FBPG group (M ± SE, CGM vs FBPG group, times, hypoglycemia times, 0.21 ± 0.07 vs 0.02 ± 0.01; potential hypoglycemia times, 3.21 ± 0.28 vs 2.21 ± 0.23, p < .01).
Blood glucose and hypoglycemia times between CGMs and FBPG.
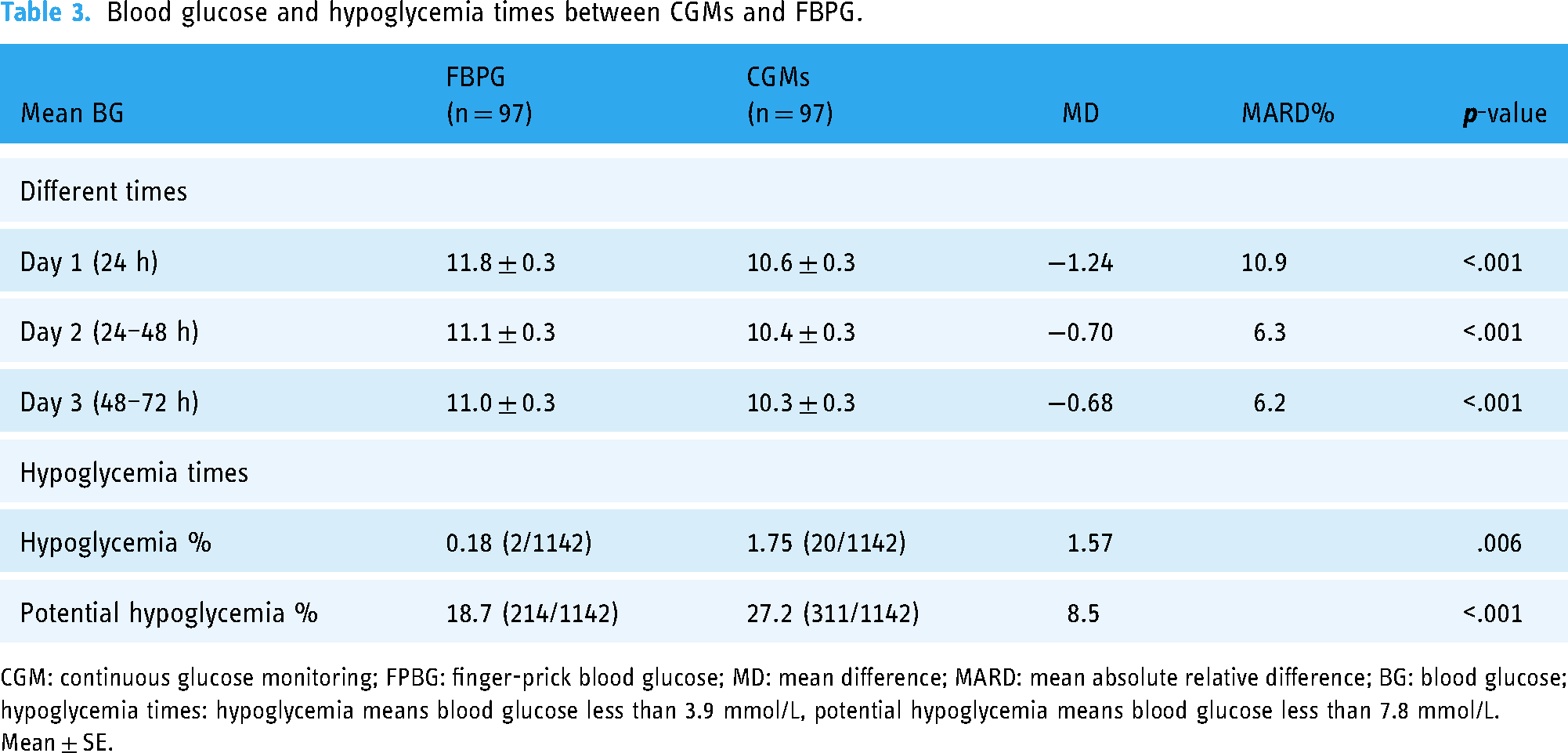
CGM: continuous glucose monitoring; FPBG: finger-prick blood glucose; MD: mean difference; MARD: mean absolute relative difference; BG: blood glucose; hypoglycemia times: hypoglycemia means blood glucose less than 3.9 mmol/L, potential hypoglycemia means blood glucose less than 7.8 mmol/L.
Mean ± SE.
Consistency analysis and correlation analysis between CGM and FBPG
Bland–Altman analysis was performed to investigate the agreement between the CGM and FBPG parameters. Figure 2 shows the Bland–Altman plots. The mean bias and 95% CI for the comparison of mean BG, mean FPG, and mean PPG between CGM and FBPG were −0.89 mmol/L (−1.08 to −0.70), −0.88 mmol/L (−1.08 to −0.68), and −0.90 mmol/L (−1.10 to −0.69), respectively, all p < .001. The mean BG, FPG, and PPG had narrow 95% CIs between CGM and FBPG.
Additionally, we used regression analysis to examine the accuracy of the CGM and FBPG. The regression lines for these three parameters for all participants are illustrated in Figure 2. We also showed y = x lines, which indicated the best scenario where the values obtained from the CGM and FBPG are equal. Specifically, we have formulated the following equations to correlate CGM data (denoted as x-axis) with FBPG values (denoted as y-axis): for mean BG, the equation is: Y = 2.141 + 0.880X, for mean FPG, the equation is: Y = 2.056 + 0.842X, and for mean PPG, the equation is: Y = 2.131 + 0.892X. Besides r2 values were reported, 0.92 for mean BG, 0.87 for mean FPG, and 0.92 for mean PPG, showing the scatter of data around the regression lines. In this analysis, the fitted lines for mean BG, FPG, and PPG were close to the ideal line, and the r2 values were high.

Bland–Altman Plot of mean BG (A), correlations with CGM and FBPG of mean BG (B), mean FPG (C), mean FPG (D), mean PPG (E), mean PPG (F).
Discussions
As of now, this is the first study to evaluate the performance of FSL-Pro CGM in patients with T2DM and AMI using FPBG as the reference. Our findings revealed a decrease of 0.88 to 0.90 mmol/L in the mean blood glucose (BG) levels for daily, fasting (FPG), and postprandial (PPG) measurements. Notably, we discovered that across different glycemic ranges, the maximum effect was primarily observed on the first day, thereafter, it gradually declined (falling range: Day 1, −1.24; Day 2, −0.70; Day 3, −0.68, mmol/L, respectively). Hypoglycemia and potential hypoglycemia were more frequent observed in the CGM group. Bland–Altman analysis highlighted the variability and the bias. We have innovatively introduced three Y = A + BX equations to precisely calculate FBPG data from CGM data, thus empowering clinicians with more accurate blood glucose insights.
The spectrum of glycemic disorders in AMI patients, encompassing conditions such as diabetes, stress hyperglycemia, and impaired glucose tolerance, is not only common but also holds significant prognostic implications. 17 To date, there have been no studies conducting a direct comparison between FSL-Pro CGM and point-of-care capillary glucose testing (POC) in patients with both T2DM and AMI. Previous research has primarily focused on assessing the performance of FSL-Pro CGM in patients with T2DM 14 or during pregnancy. 18
Galindo Rodolfo J. et al. have found compared with POC, FSL-Pro CGM showed a 0.71 mmol/L lower mean daily glucose in 97 patients with T2DM, and a relatively high MARD of 14.8% was reported previously. 14 In this study, our focus was on assessing the precision of FSL-Pro CGM in patients with T2DM and AMI. Our findings revealed that the mean blood glucose levels were approximately 0.89 mmol/L lower compared to POC, aligning closely with the findings of previous research. 14 We observed a relatively low MARD ranging from 6.6% to 8.2% for mean BG, FPG, and PPG. Additionally, we noted low the MARD values of 6.2% to 6.3%, except for FPG (10.6%) and the initial day's blood glucose (10.9%).
Additionally, we have uncovered a novel finding indicating that the disparity in postprandial glucose levels was notably more pronounced during breakfast compared to lunch and dinner (FBPG minus CGM: 1.03 mmol/L for breakfast, 0.75 mmol/L for lunch, and 0.92 mmol/L for dinner). The reasons for the difference in MARD between different meals are still unclear, but some hypotheses can be made: Chinese people often regard rice and noodles as their staple food and consume more carbohydrates for breakfast, resulting in a relatively high blood glucose level. In the study, the average blood glucose level of patients was higher after breakfast than after lunch and dinner (12.2 mmol/L after breakfast, 11.2 mmol/L after lunch, and 10.9 mmol/L after dinner). The relatively high blood glucose level may lead to a greater difference in MARD; therefore, the difference after breakfast is the largest. While Chinese food for lunch is often simpler, with less carbohydrate intake, the difference after lunch is the smallest. As our monitoring progressed, we noticed a gradual reduction in the mean blood glucose difference over time (FBPG minus CGM: 1.24 mmol/L for the initial day, 0.7 mmol/L for the second day, and 0.68 mmol/L for the third day). This trend could be attributed to the time required for sensor stabilization or the initially elevated admission blood glucose levels affecting sensor sensitivity.
In the hypoglycemic range, both the sensors of FSL-Pro CGM and iPro2 have been observed to exhibit inaccuracies during pregnancy. 18 Multiple studies have confirmed that FSL-Pro CGM may overestimate hypoglycemia and improvements in accuracy, suggesting that improvements in accuracy may be necessary.13,14 Since the individuals in our study have both T2DM and AMI, we not only documented instances of hypoglycemia but also highlighted potential occurrences of low blood glucose. For participants experiencing AMI, the criteria for hypoglycemia and potential hypoglycemia should be adjusted based on their specific medical status and the purpose of their hospitalization. Hypoglycemia is classified as blood glucose levels below 3.9 mmol/L, while potential occurrences of low blood glucose is characterized by levels below 7.8 mmol/L. 7
In our current study, we observed that the occurrences of hypoglycemia and potential hypoglycemia were 1.57% and 8.5% more frequent in CGM than in FBPG measurements.
For example, we identified a 66-year-old patient with STEMI who experienced two episodes of hypoglycemia (2.5 and 2.7 mmol/L by CGM) and recorded blood glucose levels of 7.1 and 8.3 mmol/L using FBPG. After further investigation, it was discovered that the patient experienced bleeding at the sensor site, with the inaccuracy potentially resulting from improper sensor placement. While individual patient factors and sensor-related issues may contribute, rectifying the overestimation of hypoglycemic and potential hypoglycemia events represents a pressing imperative for the advancement of CGM technology.
Correlation and Bland–Altman analyses are commonly utilized techniques in studies examining the agreement between two methods within the same sample. 19 A Bland–Altman Plot illustrated certain variability and bias between the two glucose monitoring measurement methods (p < .001). Pearson's chi-square test indicated a significant correlation between the mean BG, mean FPG, and mean PPG levels obtained from CGM and FBPG (Pearson's correlation coefficient: 0.92, 0.87, 0.92, p < .001, respectively). The data exhibited strong correlations between CGM and FBPG, with adjusted linear equations (Y = A + BX) that were consistent for mean BG, FPG, and PPG measurements. In this study, we conducted a direct comparison of the accuracy of FSL-Pro CGM and FBPG in patients with T2DM and AMI. Our analysis revealed that the MD of mean BG, FPG, and PPG ranged from 0.75 to 1.03 mmol/L and MARD from 6.2% to 10.6%, which were deemed acceptable. Notably, we observed that the MARD varied across different meals and decreased over time (from Day 1 to Day 3). Additionally, we introduced adjusted linear equations (Y = A + BX) for enhancing the accuracy of CGM readings. Taking the average blood glucose level as an example, the equation is y = 2.141 + 0.880x. In terms of its application for clinicians, consider two scenarios: if a patient monitors their blood glucose with FreeStyle Libre and gets a reading of 10 mmol/L, but the actual FPBG test reveals a reading of 10.941 mmol/L. Furthermore, if the FreeStyle Libre reading for a patient indicates a hypoglycemic state at 3 mmol/L, the actual FPBG test would yield a result of 4.781 mmol/L. In this hypoglycemic situation, it is reassuring to know that the patient's actual blood glucose level may not be as low as initially indicated, so there is no need for excessive concern. Notably, it is important to note that the use of FSL-Pro CGM was associated with a higher incidence of hypoglycemia and potential hypoglycemia reports, necessitating further validation for clinical acceptance in future studies.
The SWOT analysis of the proposed method is presented in Supplemental Figure S1. The key strength of this method lies in the noninvasive and convenient nature of the FSL-Pro continuous glucose monitor. It alleviates the service pressure on doctors and nurses and enables the detection of nocturnal and occult hypoglycemia. However, some weaknesses are that, to date, no accuracy data have been obtained for patients with T2DM and AMI, and the accuracy is also questionable in the early 24 h and hypoglycemia stages. Therefore, there are opportunities for the proposed method, as it has been stated that hourly monitoring in T2DM and AMI patients is crucial. FSL-Pro CGM, with its more mature technology, is efficacious, and a multidisciplinary team approach involving clinicians, pharmacists, and nurse's benefits patient management. However, the threat cannot be overlooked; the accuracy during hypoglycemia stages and the early 24 h should still be verified using FBPG monitoring, and the accuracy in all scenarios should be further improved.
The strengths of the present study lie in our pioneering demonstration of the accuracy of FSL-Pro CGM in patients with T2DM and AMI. In addition, the utilization of adjusted linear equations (Y = A + BX) that exhibited consistency across mean BG, FPG, and PPG. Notably, the evaluation was conducted by a multidisciplinary team comprising physicians responsible for diagnosis, pharmacists overseeing medication reformulation and monitoring, and nurses tasked with blood glucose monitoring. Nevertheless, our study has some limitations. Firstly, while we observed inaccuracies in some patients during hypoglycemic episodes in the clinical setting, we did not opt to replace the sensors. Secondly, due to variations in individual tolerance levels for FBPG, we restricted our monitoring to four-point finger measurements. Furthermore, given that our study focused on patients with T2DM and AMI, and the sample size was relatively small, and the scope was limited. We are confronted with several challenges: Firstly, given the proliferation of noninvasive blood glucose monitoring devices, determining which one is the most suitable for critically ill patients has become a crucial task. Secondly, we must address the challenge of overcoming the inaccuracies that often arise during hypoglycemic and early-stage monitoring. Finally, for critically ill patients, once we have acquired their blood glucose monitoring data, effectively managing their condition becomes paramount.
Conclusions
This study validates the use of FSL-Pro CGM devices in patients with T2DM and AMI. Our findings show that the MARD in mean BG, FPG, and PPG were deemed acceptable. Notably, the MARD varied across different meals, with the mean FPG MARD being 10.6%, and decreased as time progressed from Day 1 to Day 3. Moreover, we introduced adjusted linear equations (Y = A + BX) to enhance the accuracy of CGM readings. Consistent with previous studies, we also observed that FSL-Pro CGM tends to overestimate hypoglycemia and exhibit inaccuracies during hypoglycemic episodes.
Supplemental Material
sj-jpg-1-dhj-10.1177_20552076241287842 - Supplemental material for Breaking through diabetes management barriers: Assessing the accuracy of Freestyle Libre Pro flash continuous glucose monitoring in diabetes patients with myocardial infarction
Supplemental material, sj-jpg-1-dhj-10.1177_20552076241287842 for Breaking through diabetes management barriers: Assessing the accuracy of Freestyle Libre Pro flash continuous glucose monitoring in diabetes patients with myocardial infarction by Long Shen, Li Xu, Chen Zhang, Wei-Wei Gong, Xiao-Ting Jing, Min-Jia Cao, Fang-Hong Shi and Jun Pu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241287842 - Supplemental material for Breaking through diabetes management barriers: Assessing the accuracy of Freestyle Libre Pro flash continuous glucose monitoring in diabetes patients with myocardial infarction
Supplemental material, sj-docx-2-dhj-10.1177_20552076241287842 for Breaking through diabetes management barriers: Assessing the accuracy of Freestyle Libre Pro flash continuous glucose monitoring in diabetes patients with myocardial infarction by Long Shen, Li Xu, Chen Zhang, Wei-Wei Gong, Xiao-Ting Jing, Min-Jia Cao, Fang-Hong Shi and Jun Pu in DIGITAL HEALTH
Footnotes
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. Shi and Pu are the guarantors of the entire manuscript. Shen, Xu, and Zhang took part in drafting, revising, or critically reviewing the article and gave final approval of the version to be published; Cao contributed to the data acquisition, analysis, and interpretation. All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Availability of data and materials
The raw data supporting the conclusion of this article will be made available by the authors to related qualified researchers.
Competing interests
The authors have declared no conflicts of interest for this article.
Consent for publication
Consent for personal data publication was obtained from the participants and their parents or their grandparents.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study protocol was approved by ethics committees of Renji Hospital, School of Medicine, Shanghai Jiaotong University (KY2019-076).
Funding
This study is supported by Shanghai “Rising Stars of Medical Talent” Youth Development Program—Youth Medical Talents—clinical pharmacist program (SHWRS (2021) _099), the Fundamental Research Funds for the Central Universities (WKCX2022), and Shanghai Jiao Tong University School of Medicine: Nursing Development Program.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.