
Abstract
Background
Despite its potential to improve patient access, streamline administration, and enhance healthcare efficiency, systematic data on online appointment scheduling (OAS) in medical practices is lacking.
Method
Prospective, single center study conducted at an ophthalmology practice. Over a period of 12 weeks, all booked appointments, both online made via the OAS system, and offline made by practice staff via phone, email, or in-person, were recorded across four doctor consultations. Patient demographics, booking type (new appointment/rescheduled/cancelled), date and time of the booking, and the next available appointment slot were documented.
Results
1080 interactions (new booking 76.8%, rescheduling 13.1%, cancellation 10.1%) were made by 880 patients via OAS and 2427 appointments offline by 1902 patients. Patients booking offline were older than those booking online (mean 50.3 ± 28.1 years vs. 41.7 ± 22.2, p < 0.0001). No difference between the groups was found regarding sex distribution (both, female around 59%, male around 41%, p = 0.81). New patients showed a preference for booking online (p < 0.0001). 63.1% of online bookings occurred on weekdays during practice hours. 36.8% of cancellations/reschedulings were made one to two days before the appointment. These vacant slots were promptly filled again, as OAS was primarily used for near-term bookings (booking time to appointment ≤7 days in 47.7%; selection of the earliest available appointment in 44.1%). Compared to appointments made offline the no-show rate was reduced by OAS (6.8%, n = 164, vs. 1.6%, n = 13, p < 0.0001).
Conclusion
OAS contributes to patient-centered and efficient resource utilization in healthcare by reducing no-show rates and promptly filling vacant slots.
Introduction
The advancing digitization not only alters people's daily lives but also profoundly impacts healthcare. Within this context, online appointment scheduling (OAS) is increasingly gaining significance in medical practices as it optimizes workflows, enhances patient satisfaction, and improves resource utilization in the healthcare sector. 1
A decade ago, physicians were hesitant and ill equipped to offer OAS. According to a German study “Physicians in the Future Healthcare Market 2010”, 2 although 55.8% of the 461 surveyed physicians, dentists, and psychotherapists acknowledged OAS as a service for patients and a relief for practice staff, only 14% offered OAS themselves. This reluctance was attributed to concerns about an inefficient cost-benefit ratio (30% of respondents) and clashes between online and offline scheduled appointments (32.7% of respondents). Only 7.5% of respondents saw OAS as an opportunity to increase revenue and thereby influence the future of appointment scheduling in office-based patient care (22.4% of respondents).
From the patient's perspective, the attitude towards OAS is a different one nowadays. A representative German Bitkom survey of 1144 people conducted in November 2022 found that 33% of patients use OAS, with 34% considering it. 66% believe that all medical facilities should offer OAS. 22% even choose practices based on whether they offer OAS. 3
Traditional appointment scheduling mechanisms, characterized by manual coordination and telephone communication, are becoming increasingly inefficient in light of rising demands on healthcare. Challenges such as a lack of temporal flexibility, long waiting times, and potential communication issues between patients and practice staff could be effectively addressed through OAS. Furthermore, online appointment systems could provide patients with the opportunity to schedule appointments autonomously at any time, potentially enhancing patient satisfaction, reducing the telephone workload for practice staff, and minimizing the sources of error associated with manual appointment entry.
Despite the opportunities OAS presents, there is a lack of systematic data on this topic. 1 Our pilot study, based on ongoing OAS implementation in a German ophthalmology practice, investigates how OAS can contribute to contemporary, efficient, and patient-centered healthcare delivery.
Methods
Study design
This is a prospective, single center study, conducted in a German ophthalmology practice. Following a written request to the Ethics Committee of the responsible State Medical Association of Hessen, Germany, prior to the study initiation, the committee informed us that, in accordance with § 15 Abs. 1 BO, an ethics vote and written informed consent from participating subjects or their legally authorized representatives are not required for this study (ethical approval number: 2024-3837-AF).
Study population
The study cohort included all existing and new patients of the German ophthalmology practice who scheduled appointments, both online and offline, during the observation period and, to provide an additional control period, during a historical period of three months preceding the implementation of the OAS system in the practice.
Inclusion and exclusion criteria
The focus of the data collection was to record all appointments booked online and offline during the observation period to provide a complete representative picture of the use of the OAS system within a representative quarterly billing period for public health insurance. Therefore, all interactions with the OAS system during the observation period were included in the study from all existing and new patients without exception.
Online appointment scheduling
OAS was conducted through a commercially available program accessible via a mobile app and a web browser. For competitive reasons, the company name is omitted. The OAS program used includes a calendar through which the practice manages all appointments and is connected to the patient record software of the practice via a data protection-compliant interface.
All appointments, including those made by practice staff by phone, email, or in person (offline booking), are processed in real-time through the OAS program's calendar. This prevents appointment overlaps. Patients insured via public healthcare system can only book an appointment with a specialist through OAS once per quarter. All further bookings must be coordinated directly with the practice staff. The same applies to children <2 years old, as in the practice where the study was conducted, they may require evaluations by multiple physicians depending on the reason for their presentation. Consequently, they necessitate individualized scheduling, which cannot be implemented on a patient-specific basis using the OAS.
The practice decided to make the following distinctions for online-available appointments: 1. Patient age: > 13 years for adult consultations, < 13 years for pediatric consultations. 2. New or existing patient (new patient = first visit to the practice, existing patient = previously had one or more visits to the practice), 3. Public or private insurance. The above distinctions can be revised dynamically by the practice itself at any time through the OAS program.
The practice has organized the appointment calendar according to the above-mentioned categories and adapted it to the specific needs of each consultation. For example, a longer time slot per appointment has been allocated for patients in the pediatric consultation, as this patient group generally requires more time.
OAS was implemented in the practice ten months before the start of the study. The practice staff informs patients on site about the option of using OAS. Furthermore, a link to OAS is provided on the practice's homepage and Google Business profile. The OAS system used is commercially available in Germany and is used nowadays by many different medical specialists. Apart from the points mentioned above, it remains indeterminate to what extent the study cohort had prior familiarity with the OAS system before the commencement of the study.
Data collection
Observation period
The data collection period was set from Tuesday, January 2, 2024, to Monday, March 25, 2024 (12 weeks). This corresponds to a representative quarterly billing period for public health insurance without public holidays. Each weekday is equally covered. All four consultations recorded (three adult and one pediatric consultation) were available during the data collection period and were not significantly restricted by vacation or days of illness.
The period from November 2022 to January 2023 was selected as the historical control period, preceding the implementation of the OAS system in the practice in March 2023.
Data collection of the online appointment booking
Data collection took place on the same day as the online appointment booking. Documented were the date and hour of the online booking, the date of the booked appointment, and the date of the next available appointment. It was distinguished whether it was a new appointment, or a rescheduling or cancellation of an existing appointment. The age (in years) and sex of the patients were recorded, as well as whether they were a new or already existing patient.
Data collection of the offline appointment booking
All appointments booked offline during the observation and historical periods were identified. For the observation period, data on patient age (in years) and sex were recorded, along with the status of the patient as either new or existing. Since the historical period involved the same study cohort (same consultations of the same doctors), demographic data were not recollected for this period.
No-Show rates for online booked appointments
A separate part of this study compared no-show rates between appointments booked online and those booked offline. A “no-show” was defined as an appointment where a patient did not appear without informing the practice beforehand. Data for all appointments during the observation period for the three adult and one pediatric consultations were collected, differentiated between appointments booked online and offline, and the presence or absence of patients.
For the historical control period, only data from the three adult consultations conducted by the same doctors were recorded, as the pediatric consultation was still in its start-up phase at that time and was therefore not representative. Consequently, only data of the adult consultations were included in the statistical comparison with the historical control period.
Statistical analysis
GraphPad PRISM (GraphPad Software, Version 8, San Diego, US) was used for data analysis. Descriptive data such as mean ± standard deviation, median, interquartile range (IQR) from Q1 to Q3, or minimum, and maximum were calculated. The time span between data points (in days) was calculated from the booking timepoint data (booking date / booked appointment date / next available appointment date). The Mann-Whitney U test was used to compare the age of patients using online or offline appointment scheduling and booking behavior between groups (existing vs. new patients, females vs. males, minors vs. adults). Significance was assumed at p < 0.05. Due to the commercially sensitive nature of the data, no distinction was made between publicly and privately insured patients. The chi-square test was used to compare the proportions of sex, new or existing patients and no-show rates for all online and offline booked appointments.
Results
Demographic data of the study cohort
A total of 880 patients used the OAS during the twelve-week observation period. The median age of the patients was 45.0 years (IQR 24.3 to 58.8 years, mean 41.7 ± 22.2 years). 145 patients (16.5%) were under 13 years of age, and accordingly, they were scheduled for pediatric consultations. 532 (60.5%) were existing patients, and 348 (39.5%) were new patients.
A total of 1902 patients booked their appointments offline during the observation period. The median age of these patients was 58.0 years (IQR 19.8 to 74.0 years, mean 50.3 ± 28.1 years). Of these, 342 patients (18.0%) were under 13 years of age and were scheduled for pediatric consultations. A total of 1582 (83.2%) were existing patients, while 320 (16.8%) were new patients.
During the study period, 101 patients utilized both online and offline appointment scheduling methods.
The age and sex distribution of patients using online or offline appointment scheduling systems are illustrated in Figure 1A and 1B, or Figure 1C and 1D, respectively. The 101 patients who utilized both, online and offline appointment scheduling methods, were included in both groups. Patients who booked their appointments offline were significantly older than those booking online (p < 0.0001). No significant difference was found regarding sex distribution (p = 0.81). New patients showed a preference for booking online (p < 0.0001).

Demographic data of the study cohort. A Age and B Sex distribution of all 880 patients who utilized the online appointment scheduling during the observation period. C Age and D Sex distribution of all 1902 patients who utilized the offline appointment scheduling during the observation period. 101 patients used both, online and offline appointment scheduling, and therefore are listed with both, the patients who utilized the online appointment and those who utilized the offline appointment scheduling.
Online booking behavior of patients
During the observation period, there were 1080 interactions via OAS. Of these, 830 (76.8%) were new appointments, 141 (13.1%) were reschedulings, and 109 (10.1%) were cancellations of existing appointments. On average, there were 1.2 ± 0.6 interactions per patient (median 1, range 1–5) and 12.9 ± 6.4 interactions per day (median 12.5, range 1–33).
Time of online booking on a weekly and daily basis
The timing of online bookings over the course of the week is shown in Figure 2A. When aggregating online bookings by day of the week and time of day, the distribution pattern shown in Figure 2B and 2C emerges. Most online bookings (63.1%), including new bookings, rescheduling and cancellations, occurred on weekdays during practice opening hours from Monday to Thursday from 8 am to 5 pm and Fridays from 8 am to 1 pm.
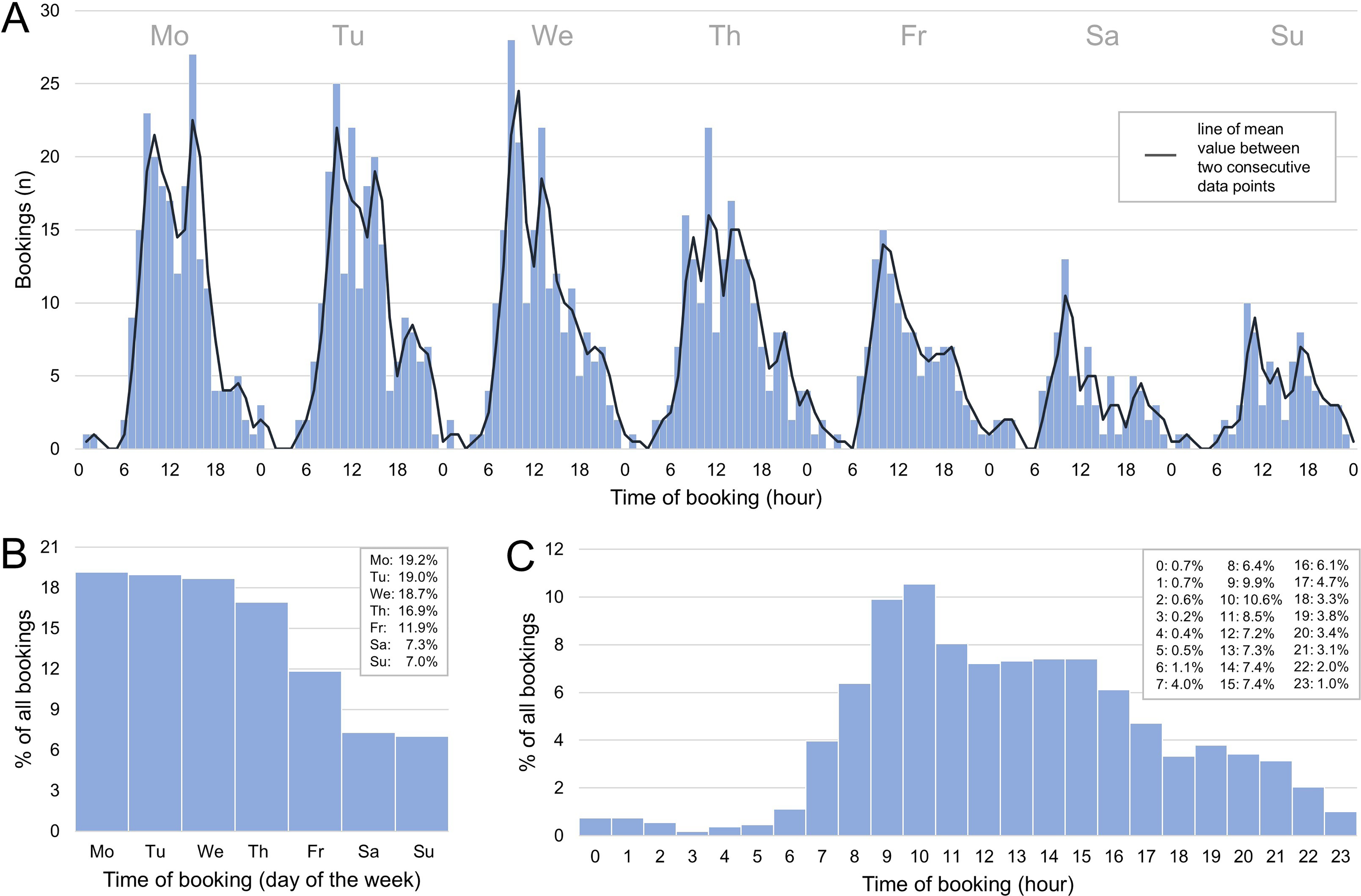
Timing of online booking by week and time of day. Distribution patterns of interactions (booking of a new appointment, rescheduling or cancellation of an already existing appointment) with the online appointment scheduling system concerning the timing within A the overall weekly chart, B the day of the week, and C the time of day within a day.
Time of online booking in relation to the booked appointment
Figures 3A and 3B demonstrate that OAS was primarily used to book appointments as soon as possible. The time between the day of booking time and the booked appointment of ≤7 days was observed in 47.7% of all booked appointments, and ≤14 days in 62.4% (Figure 3A). Such near-term booking behavior was significantly more pronounced in new patients compared to existing patients (p < 0.0001, Figure 3A). No different booking behavior was observed between groups based on sex or age (females vs. males, p = 0.72; minors vs. adults, p = 0.94). This preference for near-term booking behavior is further illustrated by the time between the next available appointment and the booked appointment (Figure 3B). In 44.1% of cases, the next available appointment was chosen, and in 67.0% an appointment within 7 days after the next available appointment.

Timing of online booking in relation to the booked appointment. A Distribution patterns of booked appointments via the online scheduling system in relation to the time between the day of booking and the booked appointment for all newly booked and rescheduled appointments (n = 971, time span 0 to max. 180 days). The cut-off was set at day 60, as subsequently only a few bookings were made until day 180 (n = 143). Mann-Whitney U test was used for comparison between groups (existing patients n = 612, new patients n = 359, females n = 566, males n = 405, minors n = 193, adults n = 778). Compared to existing patients, new patients showed a significantly near-term booking behavior (p < 0.0001). B Distribution patterns of booked appointments via the online scheduling system in relation to the time between the booked appointment and the next available appointment. The cut-off was set at day 60, as subsequently only a few bookings were made until day 180 (n = 85).
Timing of appointment cancellations (cancellation or rescheduling) via the online appointment scheduling system
Appointment cancellation (Figure 4A) or rescheduling (Figure 4B) mainly occurred one to two days before the originally booked appointment (cancellation: 44.0%, n = 48; rescheduling: 31.2%, n = 44, cancellation + rescheduling: 36.8% of all 250 cancellations + reschedulings). Only a small proportion of appointment cancellations or reschedulings occurred on the same day as the originally booked appointment (2.8%, n = 3, and 4.3%, n = 6, respectively). Regarding appointment reschedulings, 22.7% of appointments (n = 32) were moved to an earlier date and 73.0% (n = 103) to a later date. 4.3% of appointments (n = 6) were rescheduled to a different time within the same day (Figure 4C). In 42.7% of appointments rescheduled to a later date, an appointment within 7 days after the next available appointment was chosen (55.3% within 14 days).

Timing of appointment cancellations (cancellation or rescheduling). Distribution patterns of appointment cancellations concerning the time between the interaction in the online appointment scheduling system and the originally booked appointment in A appointment cancellations and B appointment reschedulings. The cut-off was set at day 30 for A and B, as subsequently only a few cancellations (n = 14) or reschedulings (n = 24) occurred until day 180. C Distribution patterns of the time between the day of the originally booked appointment (dashed line) and the newly booked appointment in case of appointment reschedulings via the online appointment scheduling system. Not depicted: n = 10 reschedulings with < -30 days and n = 8 reschedulings with >60 days.
No-Show rates compared between online and offline booked appointments before and after implementation of online appointment scheduling
The percentage distribution of excused and unexcused no-shows for online and offline booked appointments relative to all available appointments during the observation period is shown in Table 1. About 804 (24.9%) of the 3231 appointments taking place during the observation period was made via the OAS system. Compared to offline booked appointments (n = 2427), the no-show rate for online booked appointments (n = 804) was significantly reduced to less than one-fourth (6.8%, n = 164, vs. 1.6%, n = 13, p < 0.0001). No significant influence of age on the no-show rate was observed; however, younger patients appeared to have a higher tendency to miss their appointments without prior notice (no-show group: 49.1 ± 27.8 years vs. attended/cancelled appointments: 51.9 ± 27.8 years, p = 0.20). No significant effect of gender was identified, although male patients demonstrated a non-significant trend toward a higher no-show rate (p = 0.18).
No-Show rate of online versus offline scheduled appointments.

* p < 0.0001
Shown is the percentage of all missed appointments, appointments that were excusably missed (excused cancellations), and appointments that were unexcusably missed (No-Show), in relation to all corresponding scheduled appointments during the observation period.
The percentage of all missed appointments, including those canceled with an excuse (excused absence) and those unexcused (no-show), in relation to all scheduled appointments during the observation period is presented. Offline booked appointments = appointments made by practice staff via phone, email, or by personal contact in the practice. Online booked appointments = appointments made via the online appointment scheduling system.
A comparison of offline-booked appointments for three adult consultations from January to March 2024 with the same consultations from November 2022 to January 2023, before OAS implementation, showed no significant difference in no-show rates (6.6%, n = 1683 shows, n = 134 no-shows vs. 6.9%, n = 1859 shows, n = 163 no-shows, p = 0.43). Consequently, the no-show rate for online-booked appointments during the study period was also significantly lower than that of the historical period (p < 0.0001).
Discussion
In recent years, OAS in healthcare has undergone significant development and has become an integral part of patient care.1,4 The present study demonstrates that OAS contributes to efficient and patient-centered resource utilization in the healthcare sector.
Potential advantages associated with online appointment scheduling
From the patient's perspective
OAS offers numerous benefits to patients, including improved accessibility, reduced waiting times 5 and flexibility in appointment scheduling. Figure 2 illustrates that while the majority of online bookings occurred during regular practice hours, 36.9% of interactions with OAS occurred outside of this time frame. Comparable studies also found that 34% to 46% of all interactions with OAS occurred outside of practice hours.6,7 The OAS used in our study allows patients to react more flexibly to their healthcare needs by placing themselves on a waitlist for an earlier appointment. If an earlier appointment becomes available, the patient receives an email/SMS and can reschedule their appointment. This improves communication between patients and medical practices and contributes to higher patient satisfaction8,9 by reducing bottlenecks and shortening appointment wait times. The waitlist system also explains the significantly more last-minute booking behavior of new patients compared to existing patients, since at the time of data collection, the practice was only gradually accepting new adult patients with public health insurance. Therefore, a waiting list existed for these patients. Appointments for public insured, adult new patients were sometimes made available a maximum of five days before the appointment (see peak of the chart for new patients at 5 days, Figure 3A).
From the perspective of the medical practice
An advantage of OAS from the perspective of practices lies in optimizing resource utilization. Not only can spontaneously vacated appointments be quickly and easily filled again through OAS (Figure 3), but the automation of the appointment scheduling process reduces administrative costs and the administrative burden of the limited capacity of telephone lines and appointment schedulers. 10 Accordingly, efficiency in practices can be increased. 11 Comparable results are already provided by industries outside of healthcare. For example, it has been shown in the transportation and hospitality sectors that the use of consumer-based online reservation systems contributes to improvements in operation, 12 profitability, 13 customer loyalty, 14 and wait times. 15 The concern expressed by some physicians about a potential imbalance in the cost-benefit ratio of OAS2,16 cannot be justified based on the data of the present study. While appointment cancellations / reschedulings mainly occurred one to two days before the originally booked appointment (Figure 4), these vacated appointments could be directly refilled by OAS since OAS was primarily used to book appointments as soon as possible (Figure 3).
Also, as shown in other studies,5,7,16–19 the no-show rate for appointments booked via OAS was significantly reduced to more than one-fourth (Table 1). The reduction in missed appointments and thus the full utilization of resources increases the efficiency of healthcare facilities. 20 The reduction in the no-show rate may be due to reminder emails/SMS sent seven and two days before the appointment via OAS to those patients who already used the OAS once before, or because patients feel more responsible for their appointment when they have booked it themselves. 21 Nevertheless, it should be noted that the literature contains data indicating no difference in the no-show rate between online-booked and traditionally-booked appointments, 22 and data showing an even higher no-show rate for appointments booked online. 23 Therefore, the causality between OAS and a potential reduction in the no-show rate remains not clear, especially since the no-show rate can also depend on many other factors like for example the interval between scheduling and the appointment and demographics like for example age.24,25 Nevertheless, no clear influence of age or sex on the now-show rate could be detected in our study, however, younger patients appeared to have a higher tendency to miss their appointments without prior notice (p = 0.20). Patients who book their appointments online were younger than patients who book their appointments offline (Figure 1A and 1C, p < 0.0001). Accordingly, the lower no-show rate for online-booked appointments cannot be attributed to age. Similarly, with no difference in sex distribution between online and offline bookers (Figure 1B and 1D, p = 0.81), sex does not explain the reduced no-show rate for online appointments. As the no-show rate for offline bookings during the study period was unchanged from the historical control period (p = 0.43), other factors possibly changing over time in the practice are also unlikely to account for the reduced no-show rate of online bookings.
Potential disadvantages associated with online appointment scheduling
Despite the mentioned advantages, several challenges related to OAS must be considered. Data protection and data security remain important concerns, especially given the sensitive nature of health data. Legal regulations may vary depending on the country and region and must be carefully observed to minimize legal risks and ensure the quality of care. 26 It is crucial to implement robust security measures to ensure the confidentiality and integrity of patient data. Compliance with data protection policies is crucial to strengthen patient and public trust in OAS.
Furthermore, technical barriers can limit the use of OAS, especially for older patients27,28 or those with limited access to digital technologies. 28 Such patients may be disadvantaged by OAS, as it becomes more difficult for them to obtain a timely appointment. 29 Figure 1A and 1C illustrates, that patients older age prefer offline appointment scheduling (p < 0.0001). Although Figure 1A shows that 23.7% of all patients who used OAS were aged over 60 years, the collected data do not provide information on whether this patient group booked their appointments themselves or whether this was done by another person for the patient. A recently published study by Atherton H et al. 27 revealed that working patients prefer using OAS, whereas older patients prefer to book appointments via telephone. Additionally, the study identified a deprivation gradient concerning the awareness and utilization of OAS, with a significant decrease in both awareness and usage of OAS among patients aged over 75 years.
Another issue to consider concerns the potential impact of OAS on the doctor-patient relationship. While online communication can improve efficiency, there is a risk that personal contact between patients and practice staff will be neglected. It is important to find a balanced approach that harnesses the benefits of technology without neglecting the importance of comprehensive, personal care.16,30
Excessive healthcare utilization may also be attributed to the OAS system. Patients insured via public healthcare system can only book an appointment with a specialist through OAS once per quarter. However, patients can schedule a new appointment via the OAS in the subsequent quarter, even if it is deemed unnecessary from the physician's perspective.
Limitations of the study
The present study examines how a cohort of patients in an ophthalmology practice managed the OAS. Patient cohorts from other medical specialties may have different demographic compositions and, consequently, may handle the OAS differently. Therefore, full comparability with other medical disciplines may not be given.
Another limitation is, that a sample size analysis was not performed, since the focus of the data collection was to record all appointments booked online during the observation period to provide a complete representative picture of the use of the OAS system within a representative quarterly billing period for public health insurance.
Furthermore, given that these are economically critical business data which could reveal the practice's generated revenue, it was decided not to differentiate between publicly and privately insured patients.
Beside age and sex, no further demographic patient data could be collected in this study. It was therefore not possible to compare the groups of patients who booked appointments online and those who booked appointments offline in more detail. Consequently, the present study cannot clarify whether other factors, such as for example social status of the patients, could also explain the difference between the no-show rates of online and offline booked appointments.
Conclusion
Overall, OAS in healthcare offers a variety of benefits, including improved accessibility, efficiency gains in practice processes, and optimized resource utilization. However, challenges such as data protection, technical barriers, and the preservation of the doctor-patient relationship must be addressed to fully exploit the potential of this technology. Through a holistic approach that considers both patient needs and healthcare system requirements, OAS can contribute to improve patient care.
Outlook
A follow-up project focuses on the implementation of OAS in various medical facilities - both in practices and university hospitals - and how this can increase the efficiency of the facility.
Footnotes
Acknowledgments
No third-party submissions or writing assistance were used. We thank all patients and all employees of the ophthalmologists’ practice “Augenärzte am Städel”.
Author contributions
PKB made substantial contributions to the conception and interpretation of data and was involved in drafting the final manuscript. JJ and DB made substantial contributions to the conception and interpretation of data. CL, ML, MCK, TR made substantial contributions to the interpretation of data. MR made substantial contributions to the conception and design, acquisition, analysis, and interpretation of data and was involved in drafting the final manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Guarantor
MR
Research ethics and patient consent
According to a written communication from the Ethics Committee of the responsible State Medical Association of Hesse, an ethics vote is not necessary for the present study in accordance with § 15 Abs. 1 BO (ethical approval number: 2024-3837-AF).