
Abstract
We previously demonstrated the non-inferiority of a synchronous (real-time) telemedicine model (compared to gold standard in-person examination) for pediatric ophthalmology consultations using a Polycom conferencing system, smart glasses, digital slit lamp, and digital indirect ophthalmoscope. Although we acknowledge there is a learning curve associated with becoming proficient with this system, we believe implementation of a synchronous telemedicine model is advantageous to both patient and provider in the right care setting. In conducting 348 such examinations over the course of our study and dozens of subsequent examinations after the implementation of our model in the community, we have gleaned many insights into optimizing the experience and efficiency. We wish to share these insights to help guide those interested in adopting such a model to expand access to specialists for underserved patients or improve efficiencies in their practice.
Keywords
Introduction
Serving a large, socioeconomically disadvantaged population experiencing long waits and other barriers to care, The Vision Center at Children’s Hospital Los Angeles (CHLA) implemented telemedicine in partnership with community-based clinics to increase access to care and undertook a pilot study to validate the reliability of the platform for pediatric ophthalmology consultations. 1 Here, we share best practices learned over the course of 348 study examinations and dozens more that have followed since community implementation.
We previously demonstrated the non-inferiority of synchronous (real-time) telemedicine, relative to in-person examinations, in diagnosing and managing pediatric eye conditions with a high degree of patient and provider satisfaction. 1 Although our studies1–5 were conducted in children, our model is certainly usable for the adult population. In this collaborative model, an on-site optometrist on the patient’s end conducts the examination using smart glasses for external and sensorimotor (eye alignment) examination, a digital slit lamp, and digital indirect ophthalmoscope, while an off-site pediatric ophthalmologist views over a Polycom® video conferencing system (Polycom, San Jose, California, USA). 1 All devices connect to a local computer with a monitor mounted on a mobile cart. In our model, the video is streamed via a Polycom codec from the local computer to the off-site consulting ophthalmologist, who has a Polycom camera and codec on their end as well. However, we believe a completely software-based streaming system will be viable soon, reducing the cost of the video conferencing system. For examinations conducted at external community clinics, both providers must have access to the same electronic medical record for shared documentation. Importantly, this model is intended for virtual ophthalmic consultations involving an on-site advanced care provider (e.g. optometrist) consulting an off-site ophthalmologist, not for delivering care directly to patients at home.
Best use cases
This model of synchronous telemedicine is ideal for consultation examinations that address a specific concern of the referring provider rather than general follow-up examinations. In our program, this is a pediatric optometrist from our own practice working in remote primary care clinics; however, this could also be a technician, orthoptist, or even another physician. In our current model, the pediatric optometrist will have previously conducted at least one dilated exam on the patient prior to the telemedicine consultation. Our telemedicine examinations are rarely performed on-demand; rather, patients return to their optometric clinic later for the telemedicine consultation. This is done for a few reasons. First, in cases of strabismus, we must know the refractive error to determine whether glasses may help prior to considering surgery. Second, planned telemedicine appointments are easier to accommodate in the ophthalmologist’s schedule than on-demand consults. In our model, ophthalmologists block time for telemedicine consults, which are most often surgical cases pre-screened by the optometrist
Telemedicine has thus far proven to be a useful screening modality for a variety of ophthalmological diseases with benefits to both patient and provider.6–12 In general, telemedicine is optimal for evaluating nonurgent ophthalmologic conditions that are safe to wait 1–4 weeks for consultation. In our experience, even some urgent conditions such as staphylococcal keratoconjunctivitis may be evaluated same-day via telemedicine. Emergent conditions like retinal detachment, retinoblastoma, or globe rupture, however, should always be evaluated in person by the ophthalmologist. If same-day in-person consultation cannot be coordinated, the patient should be sent to the emergency department, due to the likely need for hospital admission and/or emergent surgical intervention.
In our studies,1–5 we moved beyond screening to accurately diagnose and formulate management plans for conditions affecting all parts of the eye. External eye disease (most commonly strabismus) and conditions affecting the anterior segment were relatively easily diagnosed. However, posterior segment conditions requiring the use of indirect ophthalmoscopy generally required more time to diagnose. In our experience, this is mostly due to technical challenges related to the digital indirect ophthalmoscope itself, such as working distance discrepancies between what the person using the digital ophthalmoscope sees and what is streamed. Such issues, though, are usually easily solved with communication between the on-site provider and the off-site consulting ophthalmologist
It should be noted that using telemedicine with pediatric patients provides its own unique challenges. Children who are not able to sit still long enough for a good video to be taken may not be good candidates for this type of telemedicine consultation. An attempt at telemedicine consultation may be worthwhile, however, as we have successfully completed strabismus examinations in hundreds of pediatric patients, even infants.
When an established patient is a good candidate for a telemedicine consultation, the on-site provider should begin by notifying the patient of the option to use telemedicine to see the off-site ophthalmologist. We view this initial education as the beginning of the consent conversation. The purpose, nature, risks, benefits, and alternatives of telemedicine should be discussed and an informational brochure provided. The on-site provider then ensures the patient is comfortable proceeding with the telemedicine consult and documents all of this in the medical record. At the outset of the telemedicine encounter, the off-site ophthalmologist must confirm and document that the patient consents to the use of telemedicine.
Provider etiquette
On the day of the visit, just prior to the telemedicine examination, the on-site provider reviews history, checks vision, and gathers other information. Once the telemedicine call has begun, they relay the patient history and reason for consultation to the off-site ophthalmologist. The ophthalmologist then introduces themselves to the patient and family and asks them any pertinent questions directly. The on-site provider must make sure the monitor on the cart is facing the family, ideally positioned close to eye level so that the off-site ophthalmologist and family are face to face, so to speak.
To begin the examination, the on-site provider switches the feed to the monitor from the Polycom camera to the local computer’s desktop. The smart glasses, slit lamp, and digital indirect ophthalmoscope each stream video via their respective applications on the local computer, which is then transmitted live to the ophthalmologist by sharing the screen over the Polycom system.
In demonstrating the pertinent features of the examination, the on-site provider should refrain from interpreting the findings. Rather, they should make sure that the off-site ophthalmologist is able to see the features of concern. While the video is being captured, it is being simultaneously streamed to a local computer in the room as well as streamed to the viewing ophthalmologist. With young children, it is helpful to position the cart with the monitor away from the child, who may get distracted by viewing themselves on the monitor. The child should be looking toward the on-site provider in order for the necessary eye examination elements to be captured by the digital equipment. When possible, the monitor should be visible to the parents, who may be interested in watching the streamed video to better understand the examination findings.
The off-site consulting ophthalmologist should verbally guide the examination to obtain whatever additional elements are needed. With their attention on the patient, the on-site provider does not watch the monitor; therefore, the ophthalmologist may occasionally need to alert the on-site provider when the patient is out of frame on the smart glasses. Once the consulting ophthalmologist feels enough examination information has been gathered, they can ask the on-site provider to switch back from the desktop to the Polycom camera feed (we call this “consultation mode”). There, the ophthalmologist can speak directly to the patient and/or their family to relay the findings and provide recommendations.
When speaking to the patient or the patient’s family over telemedicine, the ophthalmologist should look at the camera instead of their monitor to simulate eye contact. In addition, the ophthalmologist should wear neutral colors, keep the background uncluttered and professional, and ensure adequate lighting on their own face for best visibility.
Clinical pearls of wisdom for equipment
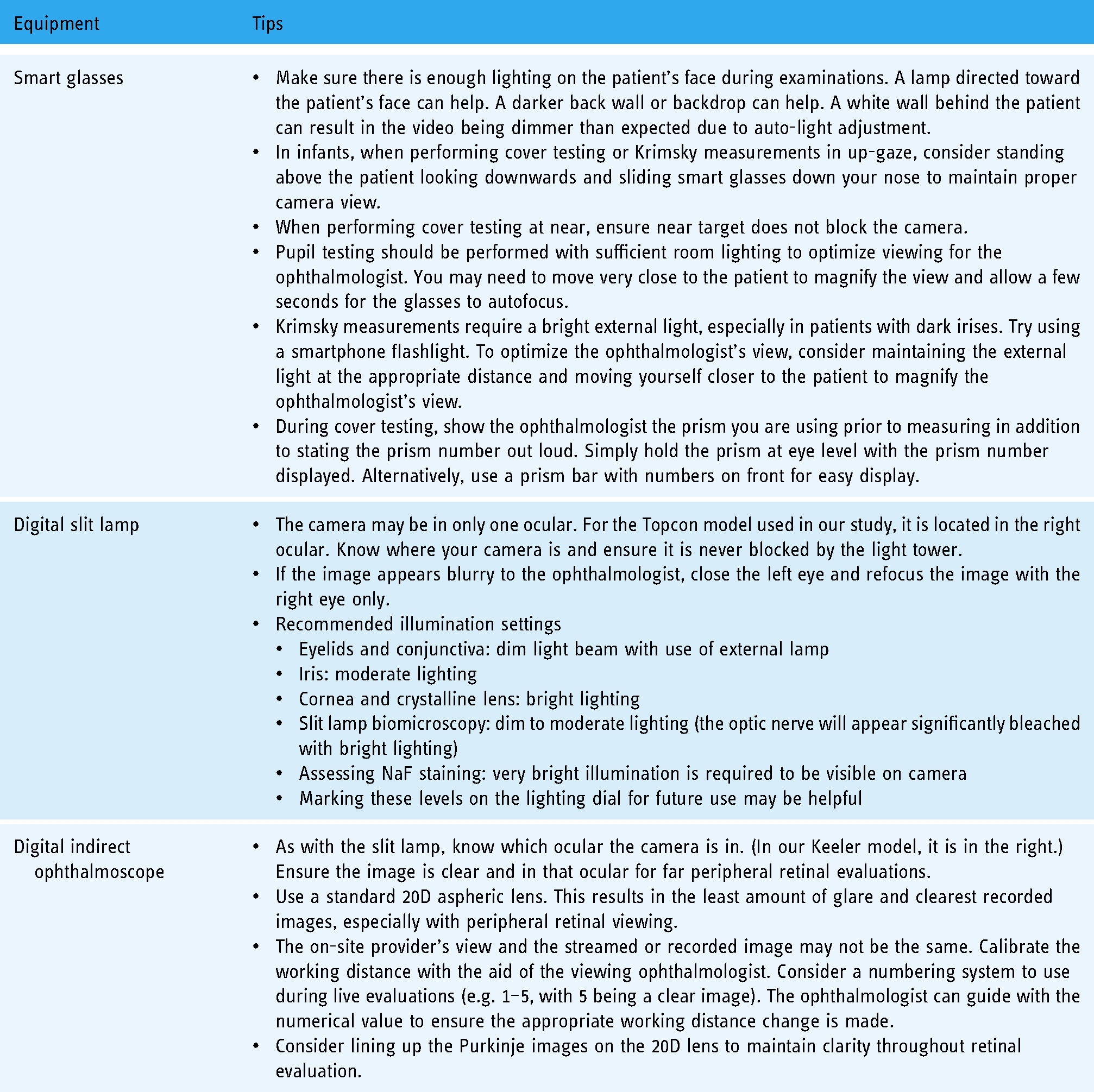
In conducting hundreds of examinations using our telemedicine model, we have numerous equipment-related recommendations we believe would be useful to those looking to incorporate a similar model into their practice (Table 1). Videos of the equipment in use are available in the supplemental materials of our previous paper 1 : https://drive.google.com/file/d/1QBCs8i2HH9prxOGXHNGgNWJszGQmJxTZ/view.
Recommendations for equipment usage.
Conclusions
The use of telemedicine has expanded significantly over the past few decades and will most likely continue to expand in the years to come. Adoption of telemedicine is sometimes viewed as a moral imperative; 13 however, it can be complex and requires time and resources to appropriately implement. For the successful implementation of our telemedicine model for synchronous ophthalmology consultations, one must overcome an initial learning curve. We hope that the pearls of wisdom shared here will be helpful to those wishing to adopt such a system and ultimately help to expand access to care and improve efficiencies in the delivery of ophthalmic care.
Footnotes
Contributorship
CS, JC-S, and SN conceived most of the advice given in this manuscript. All authors researched the literature. All authors participated in drafting, reviewing, and editing the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The advice provided in this paper is based on studies conducted at CHLA and approved by the CHLA Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Margot and Robert E. Petersen Foundation.
Guarantor
SN.