
Abstract
Objective
The current study explores the formation of an intention to use wearable fitness devices (WFDs) with wearable fitness attributes and health consciousness (HCS). Moreover, the research examines the use of WFDs with the health motivation (HMT) and intention to use WFDs. The study also exposes the moderating effect of HMT between the intention to use WFDs and the use of WFDs.
Methods
Five hundred and twenty-five adults participated in the current study, and data were collected from January 2021 to March 2021 through the online survey of Malaysian respondents. The cross-sectional data was analyzed using the second-generation statistical method of partial least square structural equation modeling.
Results
HCS is insignificantly associated with the intention to use WFDs. Perceived compatibility, perceived product value, perceived usefulness, and perceived technology accuracy significantly influence the intention to use WFDs. HMT significantly impacts the adoption of WFDs; however, the intention to use WFDs negatively but significantly influences the use of WFDs. Lastly, the association between the intention to use WFDs and the adoption of WFDs is significantly moderated by HMT.
Conclusions
Our study findings illuminate the significant impact of technology-level attributes of WFDs on the intention to use WFDs. However, an insignificant impact of HCS on the intention to use WFDs was reported. Our result confirms that HMT plays a significant role in the use of WFDs. Such as the moderating role of HMT is vital to transform the intention to use WFDs into the adoption of WFDs.
Introduction
The aging population and obesity rates are rising in most developed and emerging countries. 1 Wearable healthcare technologies can substantially empower users and enhance the preventive healthcare system. 2 Additionally, due to advancements in healthcare technology and growing health consciousness (HCS), healthcare devices for fitness are principally employed to track users’ health conditions besides exercise habits. 3 Fitness trackers are becoming increasingly popular, which is projected to continue in the years to come. 4 Healthcare monitoring is an emerging market; future market demand epitomizes significant business potential. 5
Currently, many people's lifestyle depends on their health, and personal fitness and health monitoring have become part of their lifestyle.6,7 Users can now track, save, and send information about their fitness activities due to the widespread use of wearable devices. 8 Wearable fitness devices (WFDs) have arisen as an innovative technology that tracks one's health in real-time. 9 WFDs can be employed to track physiological characteristics, including heartbeat rate, blood pressure, temperature, burned calories, personal mobility, and regular actions.10,11 Furthermore, WFDs can display a visual dashboard of users’ actions and can be combined with other health routine apps like nutrition tracking and health monitoring. 11 The benefits of wearable healthcare technology are not restricted to cost savings in healthcare; WFDs can also help manage healthcare instantly. 10 Fitness trackers, electronic movement monitors, smart wristbands, Fitbit, Jawbone, and smartwatches are some WFDs.2,12 WFDs are becoming more robust and offering suitable medical services platforms. 13 This is especially valuable with the growing attention on health, well-being, preventing illness, and fitness, in addition to the massive change towards individual-controlled healthcare. 14
Fitness devices track physiological indicators and everyday activities in real-time, motivating people to adopt a better lifestyle and save money on health care. 15 Individual and societal factors influence the adoption of WFDs. 15 WFDs have received much interest due to their ability to collect and analyze ambient data, raising enthusiasm among users. 13 Fitness trackers provide a solution for individuals seeking to enhance their health by offering them more efficient motivation through personal data-driven information. 16
The COVID-19 plague emergency worldwide has instigated a surge of attention on healthcare wearables, 14 and healthcare apps have become a primary priority during this pandemic. 2 Given these difficulties and uncertainties during COVID-19, it is probable that interest in healthcare devices and apps will continue to grow in the future. 17 More individuals have become interested in their health and physical and psychological well-being due to the COVID-19 pandemic; they desire to deliver exercises and fitness content to their homes via WFDs. 5
Although adopting wearable fitness trackers has benefited society, 18 limited scholars have examined the factors influencing users’ consciousness and their acceptance and adoption of fitness devices. 19 Health habits, consciousness, and motivation, are a few factors not utilized in literature to examine the instigation of intention and behavior towards using technological healthcare devices.13,15 Most studies inspect the formation of an intention to use wearable healthcare devices with technological attributes. 14 Identifying the fundamental determinants that affect consumers’ or users’ behavioral intention to adopt WHDs is crucial because it will help wearable device suppliers to develop a marketing strategy that will result in a greater level of adoption of fitness devices. 20 Besides, understanding customer intent and adoption of WFDs is critical for the wearable health technology industry's future success. Numerous investigations on WFDs have concentrated on “technology-driven” rather than “consumer-driven” over the last few years. 15 The global market for wearable healthcare devices will reach USD 16.2 billion in 2021 and reach USD 30.1 billion by the end of 2026. 21 Malaysian are more inclined towards wearable technologies than other South East Asian residents, and among Malaysian consumers, 65% are using wearable technologies for fitness and healthcare purposes. 22
Malaysia is regarded as a low HCS nation facing high obesity among adults. 23 The 12th Malaysia Plan intends to change the countrywide healthcare scene digitally. 24 The mounting healthcare charges reduce people's capacity to pay for healthcare expenses and take personal actions to manage their health issues. 5 Besides affordability, healthcare technologies must build on quality and convenience. 25 Malaysian users are suffering a 13.5% increase in the cost of medicinal facilities since the quantity of qualified doctors and nurses for 1000 individuals is 1.5 and 3.5, correspondingly. 23 Therefore, WFDs help users to attain well-being and offer personal convenience to accomplish a healthy life. 25 The number of wearable healthcare users in Malaysia touched 1.6 million at the end of 2022, and USD 29.5 million in market volume. 26
Wearable devices are still in their beginning stage of market dissemination. There is a nuanced understanding of current consumer demands, particularly in Malaysia; consequently, it is necessary to categorize the features that move Malaysian users’ behavioral intention and adoption of WFDs. Additionally, while consumers view wearable technologies as novel, their social acceptance and health-related issues must be examined. Only a few studies have attempted to inspect the role of health motivation (HMT) in the connection among consumer intention and the use of WFDs. As such, the present study introduces HMT as a moderator in the relationship between the use intention and WFDs adoption.
Literature assessment
Theoretical underpinning
Health behaviors develop from multiple social, technological, and psychological factors.2,14 Technology Acceptance Model (TAM) is a renowned model used to assess the acceptance of new technology among users based on technology factors like ease of use and usefulness. 27 Besides technological attributes, personal inclination is vital in evolving the technology use intention. Another aspect is perceived value, a significant predictor of technology use, in which the product or technology is viable. 20 The usefulness of technology also positively explains the intention to use novel technology. 16 Meanwhile, technology accuracy helps form a positive attitude toward using technology. 28
Personal health inclination also influences the intention to use health-linked technologies. 19 HCS, or awareness of any health concerns, promotes an individual's efforts to achieve good health and well-being. As a personal trait, HCS instigates a healthy lifestyle and the use of healthcare technology. On the other hand, HMT plays a substantial part in transforming intention into a healthcare behavior. The current work theoretically adds to the literature that HMT is vital to activating healthcare behavior. The study model is provided in Figure 1.
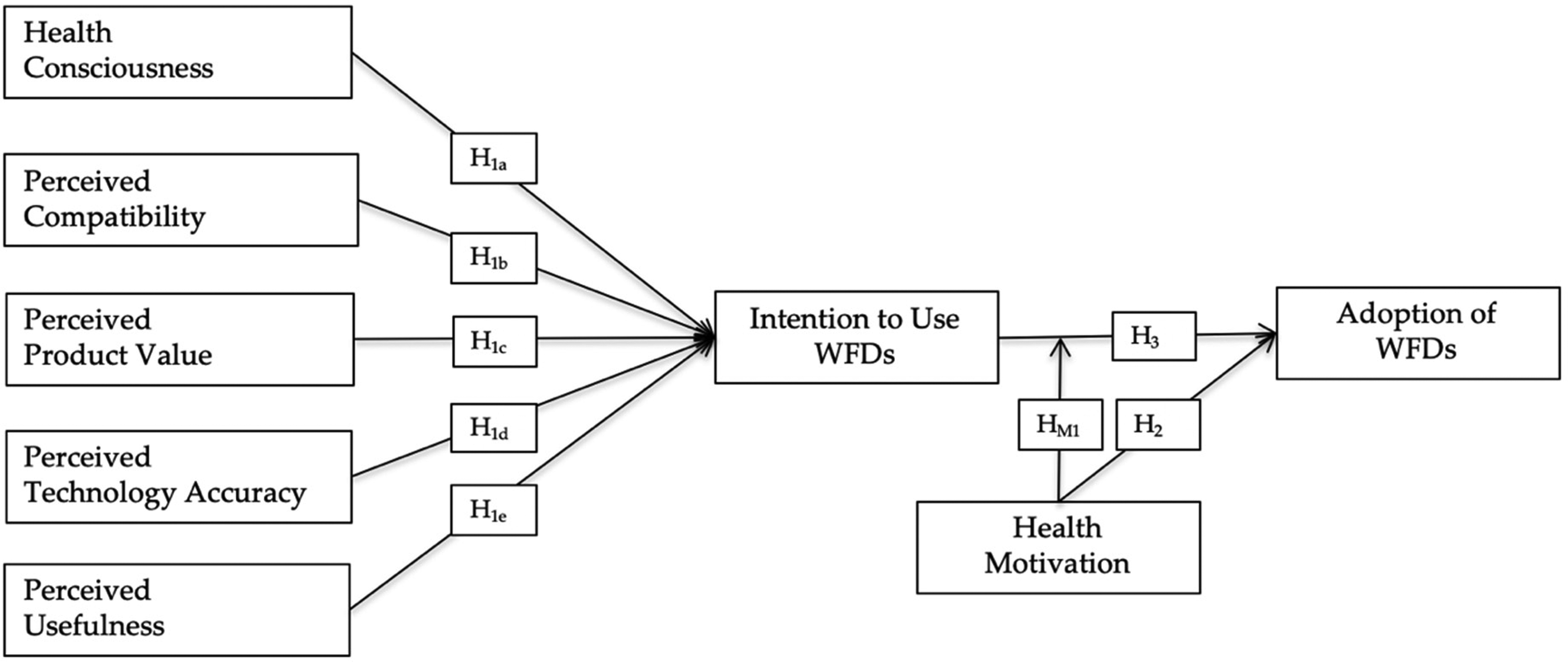
Research framework.
Hypotheses development
Health consciousness
HCS is the level to which medical issues are merged into a person's normal doings.
2
Health-conscious people are aware of potential health risks, responsible for their health, worried about their physical fitness, and interested in stress and nutritional management.
29
Additionally, health-conscious individuals are concerned about their well-being and attempt to improve and preserve it by establishing healthy behaviors such as eating healthy foods and intending to acquire health-related products, for example, fitness trackers.
30
If an individual is health-conscious, he or she is more inclined to use fitness equipment.
9
According to Chang,
2
health-conscious people are cognizant of and worried about their well-being, which leads to increased enthusiasm to improve or preserve their health. Users or individuals with a healthy lifestyle and who are health-conscious are highly expected to practice preventive health behaviors, for instance, regularly monitoring their health indicators and using healthcare services in fitness devices.
31
Individuals with a higher level of HCS are more attentive and responsive to a healthy diet and lifestyle. Therefore, they are more inclined to adopt and use WFDs.
30
The study proposes the following hypothesis:
Perceived compatibility
Perceived compatibility (PCM) discusses the personal perception of which innovative technology is compatible with prevailing ideals and habits, needs, and experiences of potential adopters.
12
Customers are more inclined to accept a fitness device that is deemed compatible. In contrast, those considered incompatible require extensive adjustments and significant learning about how to use the product.
4
Apart from that, if fitness devices are more compatible with the user's experience and lifestyle, it will be easier to comprehend how to use them.14,32 Users may deem fitness devices more compatible if they see the advantages of utilizing them for specific activities. Higher compatibility signifies a connection between the fitness devices and users’ behavioral-cognitive skills, reinforcing the longing to benefit from fitness gadgets.6,11 Hence, the subsequent hypothesis is projected:
Perceived product value
Perceived value is a vital element in envisioned behavior and is regarded as a critical marketing approach.
33
It is a user's overall valuation of a product's efficacy grounded on insights into what is received and what is given.
34
In healthcare, the overall perception of fitness equipment based on its benefits and costs is described as the perceived value.
33
Furthermore, perceived product value (PPV) refers to the difference between what is received in terms of advantage, worth, and efficacy and what is paid in terms of costs and price.1,34 Consumers are expected to possess information before they can understand the benefits and values acquired from using a product or service, which might then influence their behavioral intention.
17
Users are enticed to buy fitness equipment because of the health information and benefits they can attain from the equipment.1,19 A user will be satisfied if the wearable technology device, which includes a fitness tracker, surpasses the desirable health improvement. However, he or she will be dissatisfied if the outcomes are unexpected.
14
Consumers’ attitudes, comfort, and usage intention are all influenced by perceived value.
35
Hence, the study puts forth the succeeding hypothesis:
Perceived technology accuracy
In the digital and healthcare industries, the accuracy of the technological product is a crucial factor in the intention to adopt.
36
The perceived accuracy of wearable healthcare technologies is critical in determining their perceived credibility and adoption.
31
Furthermore, the accuracy of technology-based information helps assess users’ health management.
34
Health information accuracy refers to how accurate and adequate the evidence provided by wearable healthcare technology regarding users’ health conditions.
31
Raising the legitimacy and accuracy of a product's quality is crucial for customers, who can be influenced to become potential technological healthcare consumers.
14
The evidence's authenticity, precision, and reliability are termed accuracy.
33
The exactness of health information influences users’ willingness to involve in health-related knowledgeable choices.
36
Perceived technology accuracy (PTA) is expected to influence WFDs, per se, the subsequent is proposed: H1d: PTA effects the WFDs use intention.
Perceived usefulness
Perceived usefulness (PUS) states users’ belief that utilizing innovative technology would improve their performance.
34
PUS influences users’ intention to adopt digital technology in the TAM model.
10
In healthcare, PUS is an individual's belief that using a fitness device would enhance his or her health condition.
32
Wearable fitness trackers can make the users’ activities more comfortable, simple, and practical, thereby meeting the users’ needs more quickly and consequently playing a substantial part in improving their health.
18
Users tend to adopt fitness devices to continually monitor their body conditions if they believe this innovative device can help them better monitor their health and enhance their health and quality of life.
37
The easier people perceive the fitness tracker is to use, the more likely they are to utilize it.
6
Users’ behavioral intentions are influenced by the awareness of how easy to use and valuable fitness tracking equipment.
4
Accordingly, the succeeding hypothesis is expressed:
Health motivation
HMT is defined as an individual internal attribute of a person, whereas HCS relates to the outward aspects of how a person's health is taken good care.
25
Dehghani
12
describes HMT as the intersection of medical problems, health information acquisition behavior, and technology to deliver novel techniques to meet unique healthcare demands. Individuals interested in their health condition are more prospective to employ and embrace fitness devices.
20
Fitness trackers provide safer and better preventive treatment and more patient-centered practice and enable the transition from a traditional hub-based healthcare system to more individualized solutions.
12
Users with a developed HTM who are actively driven to investigate habits to augment their health condition are expected to learn about the advantages of fitness devices, increasing their intention to use and adopt fitness devices.
36
Consequently, the current study suggests the next hypothesis:
Intention to use WFDs
Behavioral intention, the strongest indicator of use,
38
is distinct as an individual's mental plan to undertake a specific behavior.
12
“Usage behavior” is crucial for building predictive approaches to understanding why individuals adopt or utilize a specific technology.
18
A widespread consensus is that a positive association exists between behavioral intention and the adoption of healthcare-based technology.
38
Higher intention to use WFDs is significantly related to higher levels of adoption of fitness devices.
8
Users more willing to adopt a fitness wearable technology are inclined to convert adopters and recommend it to others.
31
Hence, the resulting proposition is put forth:
Moderation effect of HMT
HMT reflects a person's involvement in preventative health behaviors such as health information acquisition activities and comprehensive health behaviors.
25
Motivation to utilize WFDs relates to a motivating force that can encourage users to take action to satisfy their essential health conditions.
29
Users who might be more inspired and involved in healthcare are more persuaded to utilize wearable healthcare technology.
14
Besides, users interested in improving health conditions are more likely to use and adopt WFDs to monitor their health conditions instantly and often a day.
20
Based on the study aim, we suggest that the HMT moderates the use intention and adoption of WFDs. The subsequent hypothesis is therefore projected:
All of the abovementioned associations are depicted in Figure 1.
Research methodology
Sample size calculation and data gathering
The present work assumed a confirmatory research design taking the quantitative method. The survey-based data was collected through the cross-sectional procedure using social media. The Google forms were prepared and circulated on social media to collect data from January 2021 to March 2021. The sample size calculation was accomplished using the G-Power 3.1, with a power of 0.95, an effect size of 0.15 with seven input variables, and a total of 153 samples necessary to realize the current study. 39 Hair et al. 40 endorse performing the partial least square structural equation modeling (PLS-SEM) analysis with a minimum of 200 samples. Data analysis was executed with 525 valid replies.
The local ethics team ruled that no prescribed ethics consent was mandatory in the particular study because (a) the data is entirely unidentified as no individual information is being collected; (b) the data is not considered to be sensitive or confidential in nature; (c) the issues being researched are not likely to upset or disturb participants; (d) vulnerable or dependent groups are not included; and (e) there is no risk of conceivable exposes or reporting responsibilities. The current study has been performed in accordance with the Declaration of Helsinki. Informed written consent for partaking was attained from the study participants, and the participation is voluntary. All the study participants were above 18 years old. The inclusion criteria were that the samples were aware of the wearable fitness healthcare devices resident of Malaysia and above 18 years of age. The exclusion criteria were people under the age of 18, not aware of the wearable fitness healthcare devices, not accepting the written consent form, and residing outside of Malaysia.
Measurement scales
The study's measurement scales were derived from known and effective scales. First, HCS was judged using four items taken from Dutta-Bergman 29 ; the reported Cronbach's alpha for the scale was 0.72. Second, HMT was assessed with four items taken from Li et al. 25 with the reported Cronbach's Alpha of 0.91. Next, PCM was evaluated using the four items from Yang et al., 32 having Cronbach's alpha for the scale was 0.96. PUF was assessed with four items taken from Kim et al., 5 with Cronbach's alpha of 0.93. In the meantime, the perception of technology accuracy was judged using four statements from Alam et al. 31 with Cronbach's alpha of 0.88.
The perception of product value was appraised using four statements taken from Kim et al. 5 and with a Cronbach's alpha of 0.91. On the other hand, the intention to use WFDs was evaluated using four items from Alam et al. 31 and Gao et al. 38 having Cronbach's alpha 0.85 and 0.82, respectively. Lastly, the use of WFDs was gauged with a single-question item. All the questionnaire items relating to exogenous variables were marked using a 5-point Likert scale, whereas endogenous variables were graded based on a 7-point Likert scale. In the research design stage, employing discrete Likert gauges for input and outcome variables can solve the matter of common method variance (CMV). 41
Common method variance
Using single-source data collection techniques is popular among social science researchers, and it builds the CMV. 41 Harman's one-factor assessment is anticipated as an approach to evaluate the CMV issue in the current research. 41 The outcome of single-factor Harman's assessment supports the idea that the CMV was not a grave issue in the current work; the one-factor account for 31.5% change and less than the recommended 40% edge. 41 Additionally, the study evaluated CMV by testing the complete collinearity, as suggested by Kock. 42 The variance inflation factor (VIF) values were determined: 2.618 (HCS), 2.695 (HMT), 2.488 (PCM), 2.169 (PPV), 2.670 (PUF), 2.188 (PTA), 2.950 (intention to use WFDs), and 2.520 (adoption of WFDs). Since all the VIF values were below 3.3, it indicated the nonappearance of bias from the data collected in unisourced. 41
Multivariate normality
PLS-SEM is a nonparametric analysis device, and nonnormal data can be evaluated in the SmartPLS. 43 Consequently, multivariate data normality examination is accomplished with the online tool of web power (https://webpower.psychstat.org/wiki/tools/index). 32 The outcome settles that the present data were nonnormal, as Mardia's multivariate coefficient p-values were below .05. 44
Analysis of reliability and validity
Relied on Hair et al., 43 the reliability scores for the study's variables were evaluated using three measurements, i.e. CA, rho, and CR. The CA score must be above 0.650 to depict the reliability of the variables. The outcomes in Table 1 confirmed that all the CA scores were above 0.650, and HCS attained the lowest score with a CA score of 0.656. Meanwhile, the rho scores for all the variables were above 0.70; the lowest score was achieved by PUF, with 0.70. Likewise, the CR values for all the constructs were above 0.70, suggesting that the constructs accomplished reliability. HCS attained the lowest score, and the score was 0.798. Succeeding, the AVE for all the study variables surpassed 0.50, henceforward, suggesting suitable convergent validity. 43 Furthermore, the VIF must be less than 3.3 to represent no subject of multicollinearity. 43 All the study's constructs showed no multicollinearity issue, as the VIF scores were less than 3.3. 42
Reliability and validity.
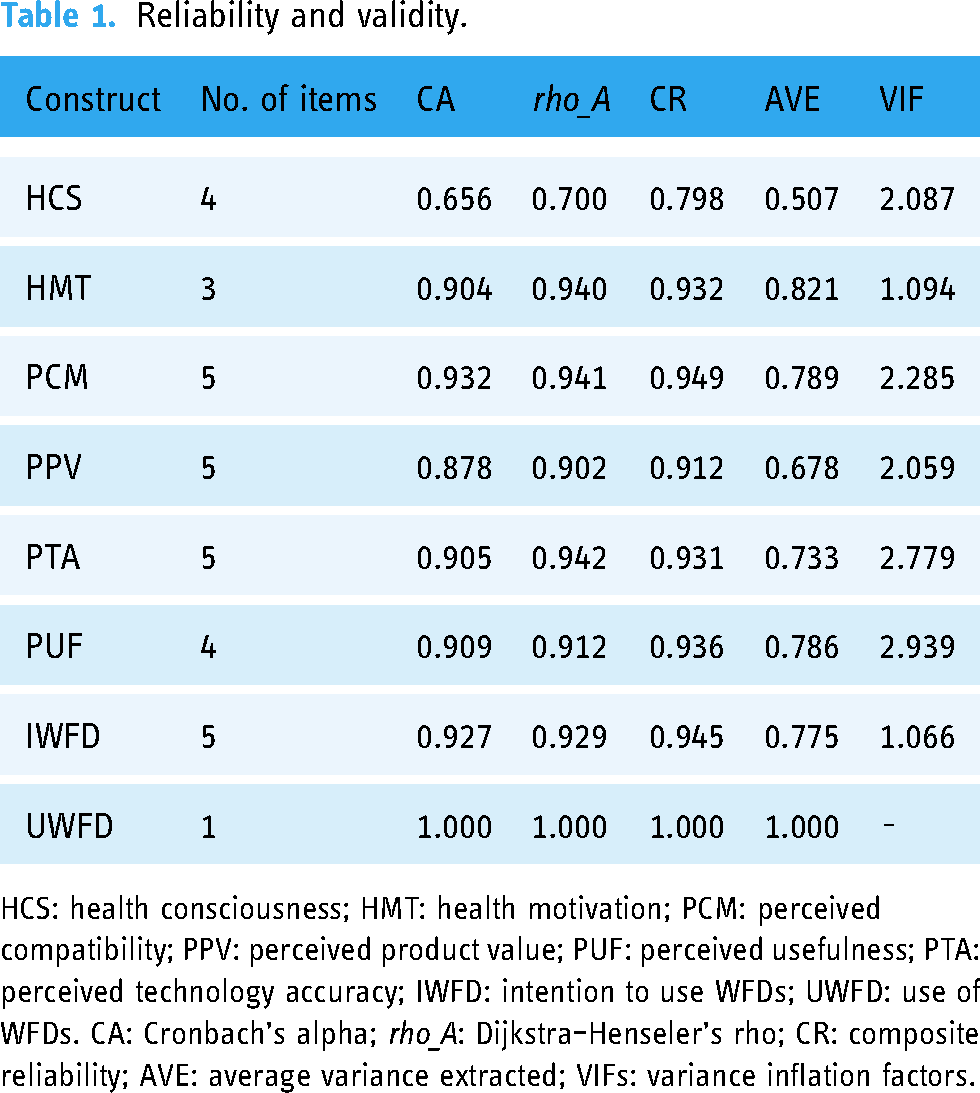
HCS: health consciousness; HMT: health motivation; PCM: perceived compatibility; PPV: perceived product value; PUF: perceived usefulness; PTA: perceived technology accuracy; IWFD: intention to use WFDs; UWFD: use of WFDs. CA: Cronbach's alpha; rho_A: Dijkstra–Henseler's rho; CR: composite reliability; AVE: average variance extracted; VIFs: variance inflation factors.
The discriminant validity was evaluated using the Fornell–Larcker criterion, HTMT, and cross-loading scores. The Fornell–Larcker criterion was appraised using the square root of the AVE score of particular constructs and compared with the correlation score. The square root of AVE must be higher than the correlation between the other constructs. The outcomes revealed that the study's model achieved discriminant validity. Next, the HTMT ratio was utilized to assess the discriminant validity, and it needs to be below 0.900 to depict the discriminant validity accomplished by the study's constructs. All the HTMT ratio scores were below 0.900; thus, discriminant validity was attained. Lastly, the cross-loading table was employed and evaluated to establish the discriminant validity of the current study's model. Appendix 1 lists the discriminant validity score.
Data analysis method
PLS-SEM is a multivariate analysis technique that empowers the assessment of study models having latent variables. Smart-PLS software 3.3 was utilized to assess the study model and hypotheses. 43 PLS-SEM works well with small data sets, nonnormal data, and intricate-based models. 40 Additionally, the evaluation of goodness-of-fit for a model is not a condition. 43 The first phase of analysis evaluates the variables’ reliability, convergent, and discriminant validity. 43 The second-stage analysis appraises the model and path association.
Results
Respondent profile
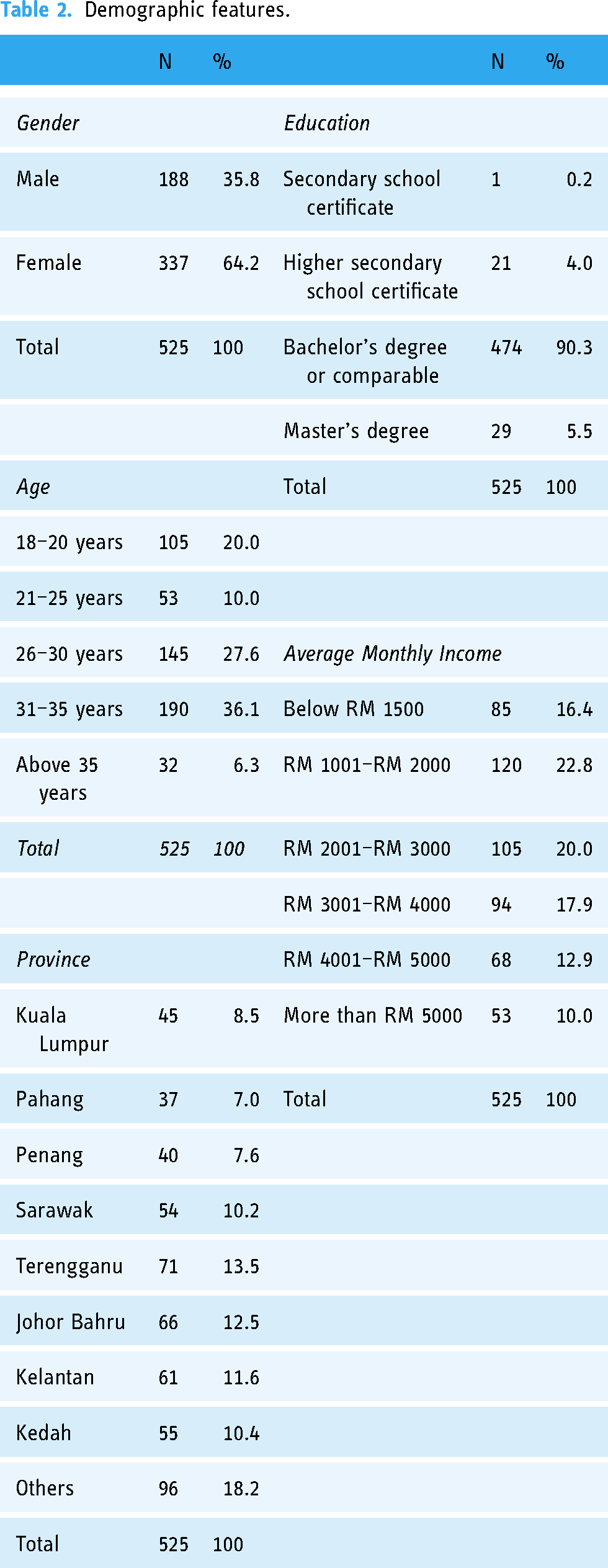
As indicated in Table 2, 64.2% of the respondents were females. The respondents’ age ranges were: 18–20 years (20.0%), 21–25 years (10.0%), 26–30 years (27.6%), 31–35 years (36.1%), and 35 years old and above (6.3%). On the other hand, the respondent's level of education varied, i.e. secondary school certificate (0.2%), diploma (higher secondary school certificate) (4.0%), bachelor's degree (90.3%), and master's degree (5.5%). Concerning their average monthly income, 16.4% earned below RM 1,500, 22.8% between RM 1001 and RM 2,000, 20.0% between RM 2001 and RM 3,000, 17.9% between RM 3001 and RM 4,000, 12.9% between RM 4001 and RM 5,000, and 10% earned more than RM 5000. The respondents’ lived in Kuala Lumpur (8.5%), Pahang (7%), Pulau Pinang (7.6%), Sarawak (10.2%), Terengganu (13.5%), Johor Bahru (12.5%), Kelantan (11.6%), Kedah (10.4%), and others (18.2%).
Demographic features.
PLS-SEM analysis
Results of path analysis
The adjusted R2 score for intention to use WFDs (IWFD) with the five input variables (i.e., HCS, PCM, PPV, PTA, and PUS) indicated that these five variables explained 68.5% of the change in the IWFD. Meanwhile, the Q2 score for the portion of the study model was 0.526%, displaying high predictive relevance. 45
The path among HCS and IWFD exposed that HCS had a positive but insignificant impact on the intention to use WFDs, thus, subsisting no provision to accept H1a. The effect size (f2 = 0.004) for the path depicted the small effect of HCS on IWFD. Next, the path value between PCM and IWFD displayed that PCM had a positive and significant effect on the intention to use WFDs. This result offered evidence to accept H1b; the effect size for the path was medium (f2 = 0.004). The path coefficients between PPV and IWFD suggested a positive and significant effect, while the effect size (f2 = 0.016) for the path showed a medium effect size, supporting the acceptance of H1c. On the other hand, the path score for PTA and IWFD demonstrated that PTA had a positive and significant effect on the intention to use WFDs. The outcome offered support to accept H1d; the effect size for the path was medium (f2 = 0.050). Lastly, the path value between PUF and IWFD showed that PUS positively and significantly impacted the intention to use WFDs. This finding meant that H1e was accepted; the effect size for the path was medium (f2 = 0.205). All the consequences are accessible in Table 3.
Path coefficients.

HCS: health consciousness; HMT: health motivation; PCM: perceived compatibility; PPV: perceived product value; PUF: perceived usefulness; PTA: perceived technology accuracy; IWFD: intention to use WFDs; UWFD: use of WFDs.
The adjusted R2 value for the use of WFDs with the two input concepts (i.e. HMT and intention to use the WFD) proved that HMT and IWFD clarified 10.7% of the disparity in UWFD. The Q2 score of the model was 0.093, displaying a low predictive relevance. 45 Next, the path between HMT and UWFD revealed the significant positive effect of HMT on the adoption of WFDs. This result offered empirical support for accepting H2. On the other hand, the path between IWFD and UWFD demonstrated a negative but significant effect of the intention to use on the adoption of WFDs, consequently indicating no sustenance to admit H3. Table 3 offered the path analysis.
Moderation investigation
The moderation analysis revealed that HMT significantly moderated the association between IWFD and UWFD, offering sustenance to admit HM1. The outcomes are offered in Table 4.
Moderating effects.

HCS: health consciousness; HMT: health motivation; PCM: perceived compatibility; PPV: perceived product value; PUF: perceived usefulness; PTA: perceived technology accuracy; IWFD: intention to use WFDs; UWFD: use of WFDs.
Discussion
The current study intended to discover the development of the intention to use WFDs with HCS and four WFDs attributes (i.e. compatibility, product value, usefulness, and technology accuracy) and whether HMT and intention to use WFDs influenced the adoption of WFDs. The analysis showed that HCS exhibited a positive but insignificant outcome on the intention to use WFDs. The outcome does not concur with the outcome in Chang2 that health concern builds a healthy attitude and uses healthcare instruments to achieve a healthy lifestyle. Furthermore, the Malaysian respondents showed a low HCS, which did not enable the use of healthcare devices to gain better health. The result accords with the results of Abdullah et al. 46 that 50% of Malaysians are experiencing obesity, and people are practising unhealthy lifestyles in ASEAN countries. A low level of awareness and the lack of a healthy lifestyle promotes a low HCS and quality of life.
Next, the perception of WFDs’ compatibility significantly promoted the intention to use WFDs. The outcome approves the verdict reported by Talukder et al. 11 that fitness devices’ compatibility positively impacts the intention to use the fitness devices. Technology compatibility facilitates the users by offering the advantage of the ease of using healthcare technology. Besides, compatibility activates the perceived appropriateness to gain the advantage of using healthcare technology. 4 This study also evaluated the association between PPV and the intention to use WFDs. The finding revealed the significant positive effect of PPV on the intention to use WFDs. This outcome matches the result in Sripoothon et al. 17 that the perception of value drives the attention of the prospective users and instigates the intention to use the WFDs. Consumers estimate the expected gains and costs related to technology use, and the expected higher gains promote the likelihood of using healthcare technology. 34
The perception of WFDs’ technology accuracy significantly impacted the intention to use the WFDs. This finding concurs with the outcome of Alam et al. 31 that technical accuracy is related to the intention to use healthcare devices. A technology's accuracy builds user confidence, and adequate, accurate information empowers users to manage their health reliably. Moreover, accurate technology empowers users to maintain a healthy lifestyle. 19 The study also inspected the link among PUS and the intention to use WFDs. The result exposed the significant positive consequence of WFDs’ usefulness on the intention to use WFDs. This outcome agrees with that reported by Yang et al., 6 whereby a technology's usefulness affects the intention of WFDs, empowering the users to accomplish their health and achieve a good value of life. Technology usefulness offers users an effective way to monitor and manage their health via WFDs frequently.
On the other hand, personal HMT effect the adoption of WFDs. The study's conclusion agrees with the verdict of Dehghani 12 that users utilize smart technologies with the right motivation. The fitness technologies facilitate the users and satisfy their health enthusiasm. Only people with precise HMT can use healthcare technologies. Besides, the influence of the intention to use WFDs on the use of WFDs was evaluated, and the outcome showed a significant negative effect of the intention to use on the use of WFDs. The verdict disagrees with the result of Alam et al. 31 that the intention to use healthcare technology promotes the use behavior of the healthcare technology. However, the HMT significantly moderates the relationship between the intention to use and the use of WFDs. Our study outcome achieves acceptance from Lee and Lee 14 that HMT facilitates the use of technological healthcare devices. Our study confirms that individual HMT instigates the use of WFDs.
Theoretical inferences
The existing research augments the theoretical posture towards adopting healthcare technology with HCS and technology attributes. Wearable healthcare devices are unique as these significantly facilitate and empower users to shape the intention for WFDs use. Second, healthcare technology adoption requires users to have HMT, and HMT moderates the connection between the intention to use and adoption of WFDs. Theoretically, the present effort is among the limited studies that have explained the part of HMT in promoting healthcare technology. The WFDs are practical tools for personal healthcare management and promoting healthy lifestyles among Malaysian adults.
Practical and managerial inferences
The present study's verdicts bid practical suggestions for the healthcare business to promote HCS and HMT. The healthcare industry management can improve the consumer product mix and work closely with them to achieve sustainable health management. Marketing and advertisement campaigns can help promote the healthcare culture and influence attitudes toward wearable healthcare gadgets. 11 The development of personal healthcare concerns facilitates an individual to manage his or her health and the global healthcare system.
Furthermore, public awareness is crucial for promoting personal health concerns. Public spending promotes HMT and attaining a healthy lifestyle, and promoting a healthy lifestyle nurtures a healthy nation and reduces public spending in the healthcare system. Additionally, promoting HCS and HMT can transform the Malaysian national health landscape and promote the individual level of health care besides reducing the obesity rate and unhealthy lifestyles in Malaysia.
Conclusion and future directions
The present work revealed that the WFDs features meaningfully influence the formation of an intention to use the WFDs, and HMT suggestively influences the use of WFDs. The HMT for the study sample significantly moderated the relationship between the intention to use and the use of WFDs. However, the current study has empirically contributed to the existing literature and practice. Nevertheless, three pertinent limitations in the current work pave the way for future research directions. First, only a limited number of variables that affected the adoption of wearable healthcare devices were employed. Hence, future studies must incorporate other technological attributes such as sustenance arrangement, social norms, mass adoption, and facilitating conditions that influence the adoption of WFDs. Next, the study assumed the quantitative design associated with restricted generalization. Future studies need to integrate mixed methods with a qualitative research design to determine the adoption of WFDs. Lastly, technology adoption is complex, and consumers’ personal and social factors play a significant role in technology adoption. Furthermore, technology adoption may undergo different stages and might not be simple. Thus, future studies must explore the continuous intention to adopt, partial adoption, or rejection of products after adoption. Consumers’ perception of product value varies, and future studies must explore the personal health conditions in adopting healthcare technologies such as WFDs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180728 - Supplemental material for Exploring the mass adoption potential of wearable fitness devices in Malaysia
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180728 for Exploring the mass adoption potential of wearable fitness devices in Malaysia by Naeem Hayat, Anas A Salameh, Abdullah Al Mamun, Syed Shah Alam and Noor Raihani Zainol in DIGITAL HEALTH
Footnotes
Contributorship
Naeem Hayat, Anas A. Salameh, and Noor Raihani Zainol: conceptualization, methodology, and writing—original draft. Abdullah Al Mamun and Syed Shah Alam: conceptualization, methodology, and writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Prince Satam bin Abdulaziz University (PSAU/2023/R/1444).
Ethical approval
The local ethics committee ruled that no formal ethics approval was required in this particular case because (a) the data is completely anonymous with no personal information being collected; (b) the data is not considered to be sensitive or confidential in nature; (c) the issues being researched are not likely to upset or disturb participants; (d) vulnerable or dependent groups are not included; and (e) there is no risk of possible disclosures or reporting obligations. This study has been performed in accordance with the Declaration of Helsinki. Written informed consent for participation was obtained from respondents who participated in the survey. For the respondents who participated in the survey were asked to read the ethical statement posted at the top of the form and proceed only if they agree. No data was collected from anyone under 18 years old.
Guarantor
Abdullah Al Mamun.
Supplemental material
Supplemental material for this article is available online.
Appendix 1. Discriminant validity

| HCS | 1PCM | PPV | PTA | PUF | HMT | IWFD | UWFD | |
| Fornell–Larcker criterion | ||||||||
| HCS | 0.712 | |||||||
| PCM | 0.648 | 0.888 | ||||||
| PPV | 0.526 | 0.580 | 0.823 | |||||
| PTA | 0.560 | 0.644 | 0.676 | 0.856 | ||||
| PUF | 0.662 | 0.662 | 0.630 | 0.741 | 0.886 | |||
| HMT | 0.346 | 0.246 | 0.468 | 0.187 | 0.242 | 0.906 | ||
| IWFD | 0.606 | 0.661 | 0.629 | 0.723 | 0.785 | 0.162 | 0.880 | |
| UWFD | −0.176 | −0.177 | 0.032 | −0.081 | −0.208 | 0.128 | −0.243 | 1.000 |
| HTMT ratio | ||||||||
| HCS | - | |||||||
| PCM | 0.865 | |||||||
| PPV | 0.704 | 0.633 | ||||||
| PTA | 0.721 | 0.671 | 0.775 | |||||
| PUF | 0.853 | 0.713 | 0.696 | 0.803 | - | |||
| HMT | 0.485 | 0.278 | 0.542 | 0.259 | 0.261 | - | ||
| IWFD | 0.776 | 0.707 | 0.688 | 0.769 | 0.853 | 0.187 | - | |
| UWFD | 0.217 | 0.178 | 0.052 | 0.130 | 0.219 | 0.112 | 0.252 | - |
| Cross loading table | ||||||||
| HCS1 |
|
0.414 | 0.399 | 0.478 | 0.542 | 0.133 | 0.436 | −0.093 |
| HCS2 | 0.518 | 0.362 | 0.427 | 0.572 | 0.229 | 0.501 | −0.139 | |
| HCS3 | 0.412 | 0.388 | 0.349 | 0.427 | 0.249 | 0.465 | −0.168 | |
| HCS4 | 0.558 | 0.372 | 0.350 | 0.312 | 0.463 | 0.297 | −0.093 | |
| PCM1 | 0.561 | 0.478 | 0.571 | 0.552 | 0.239 | 0.538 | −0.104 | |
| PCM2 | 0.567 | 0.522 | 0.573 | 0.589 | 0.218 | 0.592 | −0.165 | |
| PCM3 | 0.614 | 0.531 | 0.623 | 0.644 | 0.221 | 0.647 | −0.239 | |
| PCM4 | 0.495 | 0.508 | 0.477 | 0.465 | 0.178 | 0.491 | −0.080 | |
| PCM5 | 0.627 | 0.535 | 0.602 | 0.664 | 0.233 | 0.646 | −0.174 | |
| PPV1 | 0.262 | 0.306 | 0.412 | 0.360 | 0.269 | 0.353 | 0.080 | |
| PPV2 | 0.426 | 0.484 | 0.571 | 0.488 | 0.430 | 0.480 | 0.050 | |
| PPV3 | 0.493 | 0.577 | 0.640 | 0.626 | 0.430 | 0.586 | −0.021 | |
| PPV4 | 0.486 | 0.487 | 0.595 | 0.520 | 0.379 | 0.523 | 0.020 | |
| PPV5 | 0.458 | 0.493 | 0.546 | 0.557 | 0.401 | 0.600 | 0.028 | |
| PTA1 | 0.228 | 0.223 | 0.579 | 0.374 | 0.521 | 0.309 | 0.145 | |
| PTA2 | 0.517 | 0.562 | 0.550 | 0.662 | 0.126 | 0.629 | −0.078 | |
| PTA3 | 0.578 | 0.661 | 0.675 | 0.742 | 0.128 | 0.736 | −0.112 | |
| PTA4 | 0.496 | 0.614 | 0.566 | 0.684 | 0.113 | 0.644 | −0.081 | |
| PTA5 | 0.488 | 0.572 | 0.576 | 0.632 | 0.124 | 0.668 | −0.110 | |
| PUF1 | 0.591 | 0.532 | 0.527 | 0.658 | 0.231 | 0.712 | −0.147 | |
| PUF2 | 0.592 | 0.682 | 0.599 | 0.687 | 0.246 | 0.666 | −0.181 | |
| PUF3 | 0.629 | 0.612 | 0.582 | 0.631 | 0.193 | 0.750 | −0.206 | |
| PUF4 | 0.528 | 0.522 | 0.523 | 0.655 | 0.188 | 0.648 | −0.205 | |
| HMT1 | 0.257 | 0.238 | 0.454 | 0.138 | 0.187 | 0.166 | 0.040 | |
| HMT2 | 0.311 | 0.178 | 0.350 | 0.130 | 0.210 | 0.109 | 0.147 | |
| HMT3 | 0.351 | 0.288 | 0.531 | 0.242 | 0.251 | 0.107 | ||
| IWFD1 | 0.504 | 0.517 | 0.520 | 0.545 | 0.660 | 0.136 | −0.283 | |
| IWFD2 | 0.588 | 0.578 | 0.560 | 0.619 | 0.750 | 0.184 | −0.220 | |
| IWFD3 | 0.548 | 0.553 | 0.528 | 0.637 | 0.720 | 0.151 | −0.238 | |
| IWFD4 | 0.453 | 0.580 | 0.533 | 0.724 | 0.620 | 0.095 | −0.115 | |
| IWFD5 | 0.568 | 0.679 | 0.623 | 0.663 | 0.701 | 0.144 | −0.211 | |
| UWFD | −0.176 | −0.177 | 0.032 | −0.081 | −0.208 | 0.128 | −0.243 | |
HCS: health consciousness; HMT: health motivation; PCM: perceived compatibility; PPV: perceived product value; PUF: perceived usefulness; PTA: perceived technology accuracy; IWFD: intention to use WFDs; UWFD: use of WFDs.
Source: Author's data analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.