
Abstract
Objective
Health programs for Indigenous people are most effective, acceptable, and sustainable when Indigenous perspectives are prioritized. Codesign builds on Indigenous people's creativity and propensity to experiment with new technologies and ensures research is designed and implemented in a culturally safe and respectful manner. Limited research has focused on older Indigenous people as partners in digital health. No research has focused on the acceptability and feasibility of older Indigenous people using wearables for heart health monitoring. This study provides insights into the acceptability and feasibility for ≥55-year-old Indigenous people living in remote locations to use wearables (watches and patches) to detect atrial fibrillation (AF) and high blood pressure.
Methods
This mixed methods study was codesigned and coimplemented with the local Aboriginal Controlled Health Service in a remote area of New South Wales, Australia. It included active involvement and codesign with the participants. The devices used in this study included a Withings Scan watch and a Biobeat patch.
Results
Despite challenging conditions (>36°C) and variable internet connectivity, 11 Indigenous older adults participated in a five-day wearables program in a remote location. Participants indicated that using digital health devices was acceptable and feasible for older Indigenous users. They described high levels of comfort, safety and convenience when using wearables (patches and watches) to detect AF. They were active participants in codesigning the program.
Conclusion
Older Indigenous Australians are motivated to use wearable health devices. They are keen to participate in codesign innovative health tech programs to ensure new health technologies are acceptable to Indigenous people and feasible for remote locations.
Keywords
Introduction
Healthcare is being transformed by digital health technologies that are capable of accomplishing previously inconceivable tasks.1–3 Artificial intelligence and materials science have spurred the proliferation of comfortable and convenient wearable devices that provide real-time, user-friendly, accurate biomedical data. These devices are advancing user-centered health care and contributing to greater personal autonomy and accountability for health and well-being.4–6 It is crucial that the opportunities and benefits of digital health are distributed equitably.
In Australia, as in other high-income countries, Indigenous people experience significant health gaps compared to the broader population, resulting in an avoidable death rate three times that of other Australians. 7 Likewise, people living in rural and remote locations experience poorer health outcomes, including higher rates of hospitalizations, deaths, and injury than people living in urban areas. 8 Cardiovascular diseases are one of the most significant causes of mortality for Indigenous people.9,10 Atrial fibrillation (AF) is often asymptomatic, intermittent and frequently associated with debilitating stroke and heart failure. 11 Indigenous Australians are more likely to have undetected and untreated AF and an increased risk of AF-related stroke. A recent multisite screening study in Australia found that AF prevalence for Indigenous Australians was higher in those aged ≥55 years than in the general population (7.2% compared with 5.4%).12,13
Digital health technologies can help bridge gaps in access for people living in nonurban areas and offer a new path to address health disparities experienced by Indigenous people.7,14,15 mHealth, including handheld devices, watches, and patches, are increasingly used to detect AF. These commercially available devices are more convenient for users and reporting in the popular press associated with AF detection using watches and trackers suggests a greater awareness and interest in self-detection of AF and other silent symptoms. 16 Moreover, a recent systematic review concluded that smartphone-connected EGC devices resulted in a higher detection rate than standard care. 17
Despite evidence that Indigenous people are prolific social media users, including for help-seeking related to health,18–21 and evidence that older Indigenous people have strong interests in using wearables, 22 only one study has explored Indigenous adult perspectives and health experiences with wearable devices. This study, which included eight women university students, found that using wearable devices enhanced self-efficacy and self-health knowledge. 4 In tandem with facilitating equity in access, it is essential to learn how to implement culturally safe programs in remote locations in Australia, where conditions such as internet connectivity and extreme heat may impact access, acceptability, and efficacy of wearables. Likewise, it is necessary to explore further how screening, including wearable programs, could be implemented within the existing healthcare system, particularly in rural and remote locations, where services are often stretched. 23
Objective
This mixed methods codesigned translational study aimed to assess the acceptability and feasibility for Indigenous people aged ≥55 years living in a remote location to use wearables (watches and patches) to detect AF and high blood pressure.
Methods
Ethics
This study was approved by The Aboriginal Health and Medical Research Council of NSW; AHMRC HREC Reference Number: 1135/15. The AHMRC ethics committee and the Djurali Aboriginal Governance Panel reviewed and approved the manuscript.
All participants provided written consent to participate in the study.
All devices used in this study were purchased commercially, and no copyrighted material was used.
Aboriginal governance
The Djurali Aboriginal Governance Panel provided governance for this research. A senior Aboriginal research team member, a Bundjalung Elder and Associate Professor (BR) oversaw the research. The study was codesigned and implemented in a collaboration between the Djurali Centre for Aboriginal and Torres Strait Islander Health Research and Education at Macquarie University (Djurali) and an Aboriginal Community Controlled Medical Service (AMS) serving patients in a remote location in New South Wales (NSW). The Djurali team has a long-standing, trusted relationship with the AMS, and the Chief Operations Manager (COM) is an investigator in this study.
Codesign
Historically research methodology has marginalized and often excluded Indigenous people from leadership and governance roles. Also, many research methodologies have objectified and disempowered Indigenous people, failing to consider Indigenous ways of thinking, learning, and doing science. Moreover, research has demonstrated the critical importance of Indigenous leadership and governance to ensure a culturally safe and effective research design and program implementation.24,25 Likewise, health and education programs achieving sustainable outcomes are consistently associated with community engagement and incorporating Indigenous ways of thinking, learning, and doing. 26
This study is part of a multiyear, multicomponent, codesigned research program to identify and implement innovative methods to foster earlier detection and better management of AF in Aboriginal people aged ≥55 years. The long-term programmatic nature of this codesign research contributes to a strong “backbone support” (Figure 1) for individual projects. The Rambaldini model 27 informed our approach to codesign. It emphasizes the collective, ensures the people that the research will impact are engaged in all aspects of the research and aligns well with respectful engagement and decision-making with Indigenous Elders, Aboriginal Community Control Health organizations and communities. The Rambaldini model has been validated for health research with Indigenous communities. Moreover, it aligns with Indigenous ways of knowing, being and doing. The Rambaldini model also privileges the voice and perspectives and knowledges of Indigenous people and recognizes community contributions in ways that communities experience as meaningful, including coauthorship.

Rambaldini Model. 27
In keeping with the “shared measurement” and “continuous communication” components of the Rambaldini model, the Djurali research team worked closely with the COM and other key members of the AMS, including the head nurse and Aboriginal Health Workers, to iteratively codesign the study flow. This allowed the process to work most effectively and efficiently within the AMS, provide the most comfort and generate interest for the participants. The flow included recruiting, consenting, and onboarding participants. It also involved assisting participants in downloading the necessary phone apps, registering their devices, applying patches and “admitting” each participant into the online dashboard (required to collect data from the patches). The participants were active in the codesign process, contributing to the “common agenda,” “shared measurement and continuous communication” by providing feedback and recommendations throughout the study.
ECG care pathway
The pathway for care when a device detected AF (shown in Figure 2) was established as culturally safe and feasible in a previous study for in-clinic AF screening. The care pathway was reviewed with the AMS clinical team before commencing this study. Participants who received a possible AF result were scheduled for a follow-up 12-lead ECG within 24 h. The ECG is read by the General Practitioner (GP) for assessment and potential referral to cardiology. 12
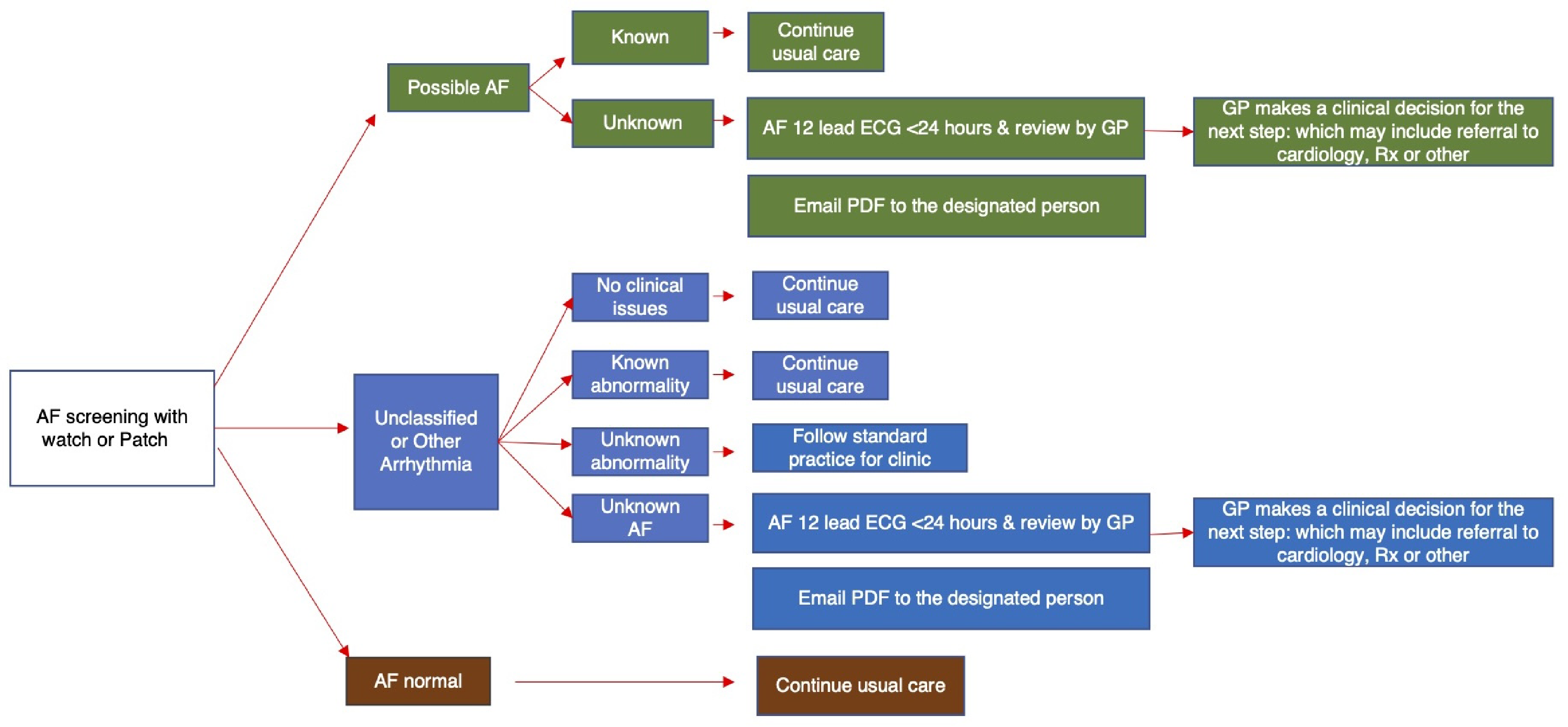
Care pathway for AF and other arrhythmia detection.
Participants
This study recruited Indigenous people at higher risk for developing AF. Aboriginal Health Workers and nursing staff from the AMS shared general information about the purpose and requirements for participation in the study with patients who met the eligibility criteria (see Table 1). Patients who expressed interest in the study were provided verbal and written details about the study, including the requirements to attend the clinic once a day for the duration of the study, to have regular access to either a smartphone running iOS 12 or later or Android 8 or later and be willing to download the Health Mate and Biobeat apps.
Inclusion and exclusion criteria.

Participants received a $25 voucher as an incentive for daily attendance to use the clinic's Wi-Fi to upload data from their phone apps to the Biobeat dashboard, meet with the researcher to review the data from their watches and patches and discuss their experiences using the devices in the preceding 24 h. This small recognition of their time is an effective recruitment strategy and is required for AHMRC ethics approval.
Context
The context of this study is critical to the aim. AMS partners on this study knew that many participants would not have 24/7 internet due to technical connectivity (due to remote location) and financial constraints. The patches and watches transmitted data to the phone apps via Bluetooth, and participants came into the clinic daily for five consecutive days to use the Wi-Fi to upload data from their phones and meet with the research team. Another critical aspect of the context is the weather. The study was completed during the summer in a remote town in NSW, to determine the acceptability of using wearables in hot conditions.
Devices
The devices used in this study included a Withings Scan watch and a Biobeat patch. See the supplemental file for device selection criteria and selection process. Data from the Biobeat dashboard and the HealthMate app were reviewed with participants each day. Participants were encouraged to ask questions about the functions of the devices and to follow up with their GP for any specific queries related to their health.
Privacy
Australia's colonial history has resulted in Indigenous people being subjected to various wrongs at the hands of researchers, including disregarding privacy and unauthorized use of personal data. All participants were assigned a research number on day 1. Data collected via survey and yarns only included the participant's research number. Only participant research numbers were used for registration to the Biobeat dashboard. Participants downloaded and registered the HealthMate app using their email addresses and were made aware of the privacy policy for the application. Health reports from the HealthMate app were downloaded to the researcher's computer, and the identifying information was immediately redacted and replaced with a research number. Upon completion of the study, the list of participants and their corresponding research numbers were destroyed in accordance with our ethics approval.
Data collection
We used Indigenous and non-Indigenous methodologies. We administered surveys on days 1 and 5 via an in-person semistructured interview. On day 5, we incorporated the survey into a one-on-one yarning28,29 session (Box 1). To explore the acceptability and feasibility of using patches and watches, we used a blended quantitative (rating on a 5-point Likert scale) and qualitative method (yarning) to investigate four predetermined issues contributing to acceptability for participants (comfort, cultural safety, convenience, and concerns). This blended data collection method facilitated consistency in collecting data that covered the full range of issues of interest while ensuring that participants could express their perspectives in a culturally safe and comfortable way. The questions and prompts were similar to questions in our previous acceptability/feasibility studies for other devices and were considered culturally safe and understandable for Indigenous people aged 55 and older.
Yarning.
Yarning is an Indigenous research tool and a key technique to co-create knowledge, including data collection, analysis and interpretation of research data. Yarning was also applied as a codesign technique for this project. Yarning is a recognized and validated Indigenous research method for qualitative research.28,29 Research yarning involves a discussion (group or one-to-one), whereby the facilitator poses questions and invites the participant/s to use the questions as a catalyst for discussion. Participants are also encouraged to reinterpret the questions and add additional information that they consider relevant. Yarns in this study invited participants to reflect on their experiences and perspectives and included plenty of time for nonstructured discussion.
Day 1 (prestudy): Questions related to previous use of smartphone health apps and wearable devices, the participant's expectations of comfort/discomfort in using a patch and a watch to screen for AF and other heart health indicators, hours of expected use and any concerns about using either device. Participants also provided basic demographic information.
Day 2—Four participants met with the researcher each day. During these sessions, we showed the participant their data on the dashboard for the patch, reviewed watch data on the HealthMate app and facilitated a yarning session about their experiences in the last 24 h.
On day 5 (poststudy): Questions and prompts were related to participants’ experience using the watch and patch. We specifically asked about feelings, including their comfort/discomfort levels, cultural safety/unsafety, convenience, confidence in using the devices, and how long they were worn. We also asked about the families’ reactions. Participants were queried about any concerns, and we specifically prompted participants to discuss any concerns about data privacy and confidence in the technology. Likewise, we included time for general reactions and requested feedback and recommendations for improving the program to make it maximally acceptable and appealing to ≥55 years old Indigenous people.
Six-weeks poststudy: The participants were invited to attend a videoconferencing yarning session to review the study's findings and provide any additional reactions or feedback.
Data analysis
Survey data were downloaded and summarized. Yarns were recorded and transcribed. We intuitively analyzed the qualitative data, creating composite descriptions of participants’ experiences and perspectives related to each area of interest: comfort, cultural safety, convenience, confidence, family reactions, and concerns. We also derived additional themes from the yarning, including issues related to context and recommendations. Data from the devices were reviewed with the participants but were not analyzed as part of this user experience study. The themes were presented to the participants six weeks poststudy, and participants yarned about the findings and provided additional data, which is included in the final analysis.
Results
A total of 11 people participated in the study. The demographics are listed in Table 2. The daytime temperature ranged between 32.2°C and 36.8°C across the five days of the study.
Demographic information.

Eleven participants used the patches. Two were unable to use the watches. One participant's phone could not load the HealthMate app, and the watch band was not the correct size for one participant. Participants attended the clinic each day. One person did not attend on day 3, and one did not attend on days 4 and 5 but completed the surveys online and spoke with the researcher by phone to provide additional input. One other person did not attend the appointment on day 5 but dropped off their watch and patch with reception (indicating that they had been called into work and could not take time for a final meeting). They were not reachable by telephone.
Baseline data: Day 1
Only two participants had ever used a phone or wearable device to track health (exercise and steps). However, all participants were interested in using wearables (patches and watches) for tracking AF and blood pressure. Many also indicated an interest in using the watch to track steps and other exercise.
On day 1, after the patches were applied and activated and participants put on the watch, they described the initial experience of wearing the devices in positive terms, with 6 of 10 rating the watch as either very comfortable or comfortable. Likewise, 9 of 11 of the participants rated the patches as very comfortable or comfortable (see Table 3).
Day 1 initial perceptions.

Most participants indicated no concerns about the devices (n = 8/9 using watches and n = 9/11 using patches). On further discussion, participants raised several questions: including how to use some of the other functions on the watch and could they go swimming and shower with the patch. Additional instruction was provided, and participants were reminded that while they could shower and swim with the watch, the patch could not get wet.
Eight participants indicated they expected to use the watch 24 h per day. One person predicted they would wear it 15 h per day. Most expected to use the patch for 16–24 h, recognizing they would remove it for showering and may leave it off until they return to the clinic later in the day.
Throughout the study, it was apparent that the participants were excited about participating. Several stated that they believed that historically they were not prioritized for trying new health technologies because they lived remotely. Ten participants spontaneously offered to participate in future studies of this type.
Daily yarns: Days 2–5
Participants attended the clinic on days 2–5 to meet one-on-one with the researcher. A few participants requested to attend the daily sessions together, which the researcher agreed to. This adaptation also proved to be an opportunity to facilitate a discussion, assisting the participants in sharing their experiences. The participants expressed an appreciation for the comradery. Likewise, other participants recommended that future programs register and meet with participants in cohorts of two to five people.
Proactive health monitoring
In addition to changing the adhesive on the patches and allowing the participants’ phones to sync with the dashboard during the daily sessions, we encouraged participants to practice using the watch to take ECG readings. We answered any questions related to other watch functions. We also included at least one ECG screening with the watch during these daily sessions. These records were uploaded to the researcher's computer and were immediately deidentified during the process. While analysis of the EEG data was beyond the scope of this study, determining if the data could be easily uploaded during the participants’ visit to the clinic provided important information the participants’ comfort in having their data uploaded. It also provided information about the feasibility of implementing a wearable program through an AMS for people who do not have independent access to the internet.
Participants consistently demonstrated high interest in data generated by the watch. A few participants explored other functions on the watch and collected ECG data while away from the clinic. Others were less adventurous, preferring to work alongside the researcher to explore the data and functions. Some expressed disappointment that the phone app for the patch did not display data as the watch app did. A couple of participants participated in specific physical activities at certain times and asked the researcher to review their data during those times. Many were also curious about their data related to sleep. In addition to wanting to know about AF, heart rate, and sleep, participants were particularly keen to track their steps.
Atrial fibrillation care pathway ensured safe and effective care following AF detection
On day 3, one participant's watch detected an episode of possible AF. The AMS team followed the care pathway (Figure 2), and the participant received a 12-lead ECG, which the AMS GP reviewed immediately. Because the participant was being seen by a GP outside of the AMS, with the participant's permission, the AMS GP contacted this doctor, who saw the participant and made a referral for a cardiology review. The participant had attended the research yarn with another participant. Once AF was confirmed during the session, the participant requested their companion accompany them through the care pathway. The participant returned the following day for their daily research session and expressed appreciation that the watch had detected AF. The participant indicated feeling safe and confident throughout the care pathway. There were no other cases of AF detected during the five-day study.
Themes
Participants’ experiences with watches
On the whole, the participants found the watches comfortable, safe, and convenient. As shown in Table 4, most (6/8 who provided data on day 5) rated the watches as very comfortable or comfortable, and seven of eight rated them as very culturally safe or culturally safe. No participants rated the watches as uncomfortable or unsafe. Their comments suggested ease and enjoyment associated with using the watches. “Once you get the hang of it, it's easy.” “I enjoyed it.”
Contributions to the acceptability of using watches.

“When I opened the gate I sort of knocked it a bit and I'm thinking, gee, bit bulky, but if they can downsize.”
The qualitative data help to paint a clearer picture of participants’ experiences; for example, one participant acknowledged that their rating of inconvenience was due to wearing the watch on the right arm because they wanted to continue to wear their other watch on the left. A quote from this participant illustrates his reaction. “I think someone without a watch would treasure one like this, but for me, I already have a smartwatch that I am used to, and this one was a bit in the way on my other arm.”
Participants were prompted to specifically report any concerns about data privacy or the technical accuracy of the devices. Most participants indicated they had no concerns. Two indicated they had a little concern, citing worries about tech companies. One participant said they trusted the university with their data but were less sure about the tech companies. Likewise, all participants expressed confidence in using the watch.
Seven participants described enjoying or very much enjoying the watch, and one rated their enjoyment as neutral. Factors contributing to their enjoyment included liking how the watch looked and feeling motivated to exercise and move more while wearing the watch. Four also described enjoying experimenting with different functions on the watch. “I like just fiddling around and getting used to the—the technology of it—of the watch. That may be useful in the future for me.”
Participants recalled favorable comments from their family members or friends about the watch, mostly commonly praising the participant for choosing to focus on their health. Several participants indicated that family and friends wanted to try using a smart watch themselves. “Well, they were interested. My brother was even interested ‘cause he has heart problems, - - and that's what he said, he said, “Oh, I should be in that” and I said, “Yeah, well you’ve got five more years bro.” Because he's only 50.” “They were really excited about it. They wanted—wanted to know more, what to do and…so they went and put their hands up for when you came back.
Participants’ experiences with patches
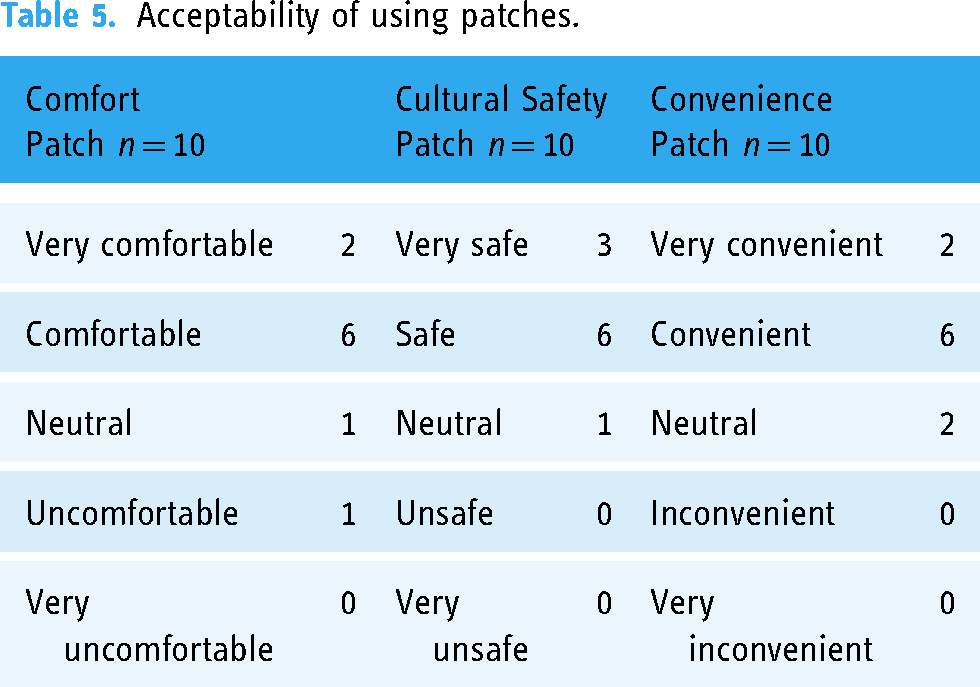
The participants described the patches as comfortable, culturally safe and convenient. As illustrated in Table 5, 8 of 10 (who provided data on day 5) described the patch as comfortable or very comfortable. Most stated they did not notice the patch as they went about their daily activities. Interestingly the person who rated the patch as neutral stated that it was neutral because they did not notice it. Two people experienced mild discomfort due to itching around the edge of the patch. One participant removed the patch for about an hour and then reapplied it without additional discomfort. “Just with the—with being irritable on day three.” “It got a bit itchy and irritating.”
Acceptability of using patches.
There were abundant spontaneous comments about the patch. Most commonly, there was discussion about the lights on the patch coming on and off at night. This presented some amusement and confusion on the first night, with several participants wondering what the lights meant—explanations of how the lights were related to the 15-min interval between active heart health measures reduced confusion immediately. However, the humor remained with participants showing the lights to grandchildren and joking about looking like robots. This became a running joke among the participants who knew each other.
Participants did not describe specific concerns about the patches. Although they indicated they wanted the patch to be waterproof so they could shower or swim without taking it off. “Only the waterproof with this (patch)” “None really. Good, comfortable—what can I say?” “Informative.” “Yeah, educational. Informative.”
“No. Doesn’t worry me.”
“Whoever's looking at me phone knows everything about me anyhow.”
Participants felt very confident (6/10 or confident (4/10) that the technology produced accurate data.
“Technology's good. I like—I like technology.”
Seven participants indicated that they enjoyed (3/10) or very much enjoyed (4/10) using the patch. Three rated their enjoyment as neutral. The most common contribution to enjoying the patch was that it reminded them to focus on their health. Similar to the watches, participants indicated that using the patch made them more conscious of their health behaviors. One person described using the patch lights coming on as a cue to move more.
“It's got me, like I said, active and that's what I need.”
“And like I said, in the last four days I think I’ve been more active than I have been for months.”
Participant learning and overall experience with the wearable program
Six participants indicated they learned a lot about heart health by participating in the wearable program. While three indicated, they learned some or a little. In contrast, one participant indicated they did not learn anything. Their perceptions of changes in digital health literacy were similar, with seven indicating they learned a lot, two learning some or a little, and one describing no learning. “Well, I’ve learnt a lot more than what I thought I knew about my heart.” “I never knew that we could put a patch on our chest to monitor our heart.” “Just to know that there is something out there for … something out there like this that's easy for—to have people to use.”

World cloud of participants’ responses to “A few words to describe your experience in the wearable program.”
The more detailed results were also shared during the online session, and the participants were asked if the data resonated and to identify additional comments or adjustments to the researcher's interpretation. Participants indicated that the qualitative and quantitative findings were consistent with their experiences. During this videoconferencing session and throughout the program, participants provided suggestions for improving the next program. Recommendations included adding a more intense educational/training component, including brief videoconferencing sessions to learn about heart health and hands-on training to use other watch functions. Participants were also interested in integrating an exercise (walking) component to improve their health. Table 6 includes a summary of these recommendations.
Summary of participants’ recommendations for designing a wearable program for ≥55 Aboriginal people.

Discussion
Our codesigned study, conducted in a remote location, is the first to examine a health-wearable program for older Indigenous adults. The key finding is that older Indigenous adults at risk for AF found using wearables to detect AF acceptable. High ratings of comfort, cultural safety and convenience indicate that using patches and watches to detect AF was acceptable for users despite being conducted in challenging conditions, including hot weather and inconsistent access to the internet. Confidence, perceptions of learning, and curiosity about heart and digital health suggest that user-based digital health programs have the potential to engage older Indigenous people in learning about and monitoring their health.
Although most participants expressed disappointment that they would be unable to keep the watches, the care they showed for the devices was remarkable—including spontaneously polishing the watches before handing them back to the researcher on the last day of the study. This finding is significant because new digital health technologies are often not offered to people in remote locations due to the inconvenience to the research team and an inaccurate belief that programs in these locations are too challenging to implement or that the potential participants are not sufficiently motivated or capable of providing valuable data. In contrast to these assumptions, our research has consistently found high participation rates in remote locations.12,22 In addition to attending daily clinic sessions, there were multiple examples of participants taking an extra step to ensure they provided helpful information about their experiences with the patches and watches to inform future programs, demonstrating compassion and sophistication in understanding the value of evidence to improve health. We found that the collaboration, enthusiasm, and proactivity of the staff and participants in this study rewarding, and we are acutely aware that codesign was a fundamental success factor contributing to getting the study results.
Limitations and strengths
The chief limitation for this study is the sample size, which were 11 people. Complete data were only available for ten, thus limiting the generalizability of the findings. A second limitation is the length of the study. The relatively short five-day length of the study limited the opportunity to explore the long-term use and acceptability of the devices once the novelty wears off. A third limitation is that only participants with access to a smartphone were included in the study. While limiting generalizability to older Indigenous people with a smartphone, this practical limitation mirrors the limitations for any wearable program implementation that requires smartphone applications. A final limitation is that the qualitative codesign of this study meant that participants worked closely with the researcher daily, which the participants indicated was a valuable aspect of the program. This level of individual attention is not scalable. It is, therefore, essential to use the findings from this study, especially the recommendation offered by the participants to experiment with methods for scaling wearable programs, such as blended programs that include digital tech within peer-based and group programs. It is also vital to examine changes in digital health literacy and health self-efficacy over time for older Indigenous people using wearables.
Strengths of this study included being the first to explore the acceptability and feasibility of using wearables to detect AF and BP for Indigenous people. It is also the first study to explore using these devices with older people living in a remote location during hot weather, with inconsistent access to the internet, thereby providing vital information about the potential performance of a wearables program for people in similarly challenging circumstances. A second significant strength is the codesign approach. A long-standing trusted relationship with the AMS provided the foundation to work together in real time to incorporate data and refine the implementation process. The participants were active partners in the implementation, working alongside the researchers to adapt schedules and timelines to accommodate longer-than-expected times for downloading apps. Participants were also proactive in providing feedback and suggestions to help themselves and future participants learn how to use the devices most effectively and efficiently. Finally, the participants actively reviewed the preliminary findings and provided additional interpretation of the data. The strength of the codesign approach enabled us to collect extensive data with a small sample size in a relatively short period of time. Examining the data through the lens of Indigenous ways of thinking, being and doing ensured that data interpretation was culturally safe and provided accurate and useful information. Moreover, codesign contributed to Indigenous leadership in health research that affects Indigenous people, thus enhancing trust and subsequent use of the findings.
Knowledge to action
The next step is to codesign a longer study to examine the acceptability and feasibility for older Indigenous people to use watches over a longer period of time. In-depth qualitative research is critical to understanding the enablers, barriers, and heart health knowledge changes that become apparent beyond the initial novelty of using watches and patches. Codesigned research that explores the participant's recommendations for incorporating exercise, health education, and cohort-based programming will help address issues they have identified as relevant and useful to them. Codesigned programs that are desired and requested by Indigenous people have demonstrated greater acceptability, efficacy, and sustainability. Additionally, the participant's interest in cocreating cohort-based health education is an important enabler to help create programs that can be delivered at scale within the existing healthcare system.
Conclusion
Older Indigenous people are motivated and capable of using wearable devices to care for their health. It is also clear from this study that older Indigenous people are effective research partners and keen to participate as codesigners meaningfully. Likewise, they value integrating their perspectives into the study in real time.
The findings highlight that privileging the perspectives of Indigenous people and Indigenous-controlled organizations such as AMSs is critical to the success of translational research. The vital next step is codesigned research to explore how to create and implement scalable digital health programs for Indigenous people targeting chronic illnesses known to be prevalent among older Indigenous people. Five days are the maximum time the manufacturers recommend for using patches. Participants were willing to use the patches for five days. In addition to the user-based focus of this study, future research should also consider how patches might be integrated into care within the AMS, potentially as a substitute for a halter ECG monitor or as a clinical tool to add easily obtainable information to clinical decision-making.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241277039 - Supplemental material for Wearables are a viable digital health tool for older Indigenous adults living remotely in Australia (research)
Supplemental material, sj-docx-1-dhj-10.1177_20552076241277039 for Wearables are a viable digital health tool for older Indigenous adults living remotely in Australia (research) by Connie Henson, Ben Freedman, Boe Rambaldini, Bronwyn Carlson, Carmen Parter, Chrishan J Nalliah, Felicity Chapman, Gina Shepherd, Jessica Orchard, John Skinner, Josephine Gwynn, Rona Macniven, Robyn Ramsden, Sophia Nala ‘Ḵixsisa̱'las Speier, Suud Mohamed Nahdi, Vita Christie, Yansong (Harry) Huang, Katrina D Ward and Kylie Gwynne in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241277039 - Supplemental material for Wearables are a viable digital health tool for older Indigenous adults living remotely in Australia (research)
Supplemental material, sj-docx-2-dhj-10.1177_20552076241277039 for Wearables are a viable digital health tool for older Indigenous adults living remotely in Australia (research) by Connie Henson, Ben Freedman, Boe Rambaldini, Bronwyn Carlson, Carmen Parter, Chrishan J Nalliah, Felicity Chapman, Gina Shepherd, Jessica Orchard, John Skinner, Josephine Gwynn, Rona Macniven, Robyn Ramsden, Sophia Nala ‘Ḵixsisa̱'las Speier, Suud Mohamed Nahdi, Vita Christie, Yansong (Harry) Huang, Katrina D Ward and Kylie Gwynne in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank Brewarrina Aboriginal Medical Services as key partners and thank the staff members in these services for their assistance in this research. The authors also acknowledge and thank the participants who were active codesigners of this research. The authors thank Walanga Muru for their support of this research. The authors thank Djurali Centre for Aboriginal and Torres Strait Islander Health Research Group for their support. The authors also thank our Aboriginal governance group (APG) for their leadership and guidance in this research.
Contributorship
Researched literature and conceptualized the study: CH, KG; Protocol development and Ethics approval: CH, KG; Recruitment: KW; Data collection: CH; Data analysis: CH, KG, FC; Cultural oversite: BR, FC, GS, CP, BC; Drafting manuscript: CH; Review and edit manuscript: all authors.
Consent
All participants provide written consent to participate in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by The Aboriginal Health and Medical Research Council of NSW; AHMRC HREC Reference Number: 1135/15. The AHMRC ethics committee and the Djurali Aboriginal Governance Panel reviewed and approved the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MRFF Cardiovascular Health Mission – 2021 Cardiovascular Health Grant 2015841 Early Af Screening for Indigenous people (EASI) and Macquarie University (grant number 20213896 Allocation for PhD students).
Guarantor
CH
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.