
Abstract
Background
Aboriginal and Torres Strait Islander people avidly use technology for a variety of purposes. Digital health technologies offer a new way to build on Aboriginal and Torres Strait Islander peoples propensity for early adoption and innovation with technology. Only limited research has focused on mature aged adults in non-urban locations as partners in digital health research and there is no research related to wearables for health tracking for this cohort.
Objective
This paper provides insights into mature aged Aboriginal and Torres Strait Islander adults interest, use and trust of social media, apps and wearables to gain health information and manage health.
Methods
This cross-sectional survey study was co-designed and co-implemented with Aboriginal Community Controlled Health Services (ACCHS) in three locations in New South Wales, Australia. The 13-item survey was administered via a semi-structured interview.
Results
Aboriginal and Torres Strait Islander adults (n = 78), in regional, rural and remote locations indicated their interest in and use of apps and wearables for health purposes. Mature aged participants, particularly women, used Facebook, ACCHS websites and YouTube for acquiring health-related information which they then shared online and in real life with a diversity of family, friends and colleagues.
Conclusions
Aboriginal and Torres Strait Islander people are using digital health technologies to acquire and share health information and want to use apps and wearables for health management. Co-designed research enables a greater understanding of the diverse needs for different cohorts and informs culturally responsible design. Broader use of co-design will foster effective user-focused digital health communication and health-management.
Keywords
Introduction
Rapid advancements in digital health technologies are shifting how we approach health care. According to the World Health Organisation, these digital innovations offer new avenues to care for underserved populations. 1 Correspondingly, the Australian government has encouraged research that uses technology to help Aboriginal and Torres Strait Islander people manage and promote better health outcomes. 2
Since the early 1990's, people worldwide have used static websites to access information about their health and wellbeing. By 2003, Eysenbach and Kohler found that health-related searches accounted for 5% of internet searches. 3 Each web iteration has sparked adaptations not previously imagined. Recent advancements have contributed to a proliferation of user-based digital health technologies that have potential to empower people to take charge of their health. And people are seizing the opportunity to use technology to participate in their health care more actively.
Social media
Social media has empowered people to not only access information from professional sources but also tap into the knowledge and experiences of friends, and trusted sources.4,5 Social media's immediacy and interactive nature mean that individuals can access specific personalised recommendations from within their network, potentially contributing to greater trust.6,7 Cultural safety and trust are particularly relevant for communities underserved by centrally-controlled, mainstream-focused health messaging, including Aboriginal and Torres Strait Islander people.8–10
Tailored, trusted and effective health communication is particularly relevant for Aboriginal and Torres Strait Islander people. Research indicates that Aboriginal and Torres Strait Islander people have died from avoidable causes at three times the rate of other Australians and have also experience significant health gaps. 11 Nolan-Isles and colleagues found that ineffective health messaging creates a barrier to service utilisation for Aboriginal and Torres Strait Islander people. 12 Communication that is racist, not sensitive to health needs, marginalises cultural identity or fails to recognise the context of colonialism may reduce Aboriginal and Torres Strait Islander people's understanding of western health concepts and practices. 13 Reduced understanding of these concepts and practices is associated with less engagement in preventive services such as screenings and protective health practices, reduced understanding of medical advice and poorer health self-management. 14 Social media can provide an avenue for engaging Aboriginal and Torres Strait Islander community members in designing and disseminating health messaging, thereby ensuring relevance and cultural safety.
Aboriginal and Torres Strait Islander people embraced social media early and have been innovators in using social media for social and political empowerment, and activism.15,16 Carlson & Dreher noted that social media, with its emphasis on peer-to-peer connectivity and movement away from hierarchal top-down centrally controlled messaging is more in keeping with Aboriginal and Torres Strait Islander ways of learning and being. 8 Likewise, Rice et al. observed that the nature of social media is culturally compatible with orally and visually focused cultures. 17 Moreover, the Aboriginal health sector was an early adopter of social media for advocacy, public health promotion and community development. 18 Building on these strengths, social media-based health messaging has the potential to tap into the inherent assets of community and connection to facilitate greater empowerment.
While there has been some excellent research examining Aboriginal and Torres Strait Islander peoples’ perspectives on and use of social media for health enhancement,19–21 most studies are qualitative with small samples and have included few mature aged adults and research has rarely segregated results by gender binary, non-binary or age cohort. Mature aged adults, particularly those residing outside of urban settings, have had significantly different technology experiences than Millennials, who grew up with the internet. Likewise, mature aged Aboriginal and Torres Strait Islander people of different genders differ from each other and from younger Aboriginal and Torres Strait Islander adults in terms of health needs. Understanding the perspectives and practices of each of these cohorts is an essential next step in understanding how to best use social media for health promotion and health management. We address this shortcoming in this study with Aboriginal and Torres Strait Islander people from three non-urban locations one regional, one rural and one remote location as classified by the Accessibility/Remoteness Index of Australia (ARIA). 22
mHealth
Social media and the internet remain important forces in how people interact with technology to enhance their health. However, we are on the cusp of a digital revolution which is likely to disrupt health care in multiple ways. Examples range from using big data to diagnose and treat cancers and rare diseases 23 to technologies such as blockchain that enable personal ownership, control and potential monetisation (or other rewards) for sharing of personal health data. 24 User-based apps and wearables are enabling people to track their bio-data. 25 Innovations in artificial intelligence create opportunities for individual citizens to use their bio-data in real-time to make informed choices about health-related behaviours. While the rate of technology development is important, personal confidence, comfort and government policies will contribute to the speed of uptake and efficacy these technologies will have in shaping health and health care.
The COVID pandemic has accelerated comfort and expertise in using mobile health technologies. Likewise, mobile apps and wearables are becoming ‘smarter’ and easier to use, and individual citizens are taking up the opportunity to access personal health data through self-tracking devices. Corbett & Schwager surveyed a representative sample of 2000 Australians aged between 18 and 75 and found that Australians using wearables increased from 28% in 2020 to 58% in 2021, which they attributed to a greater focus on fitness and health during COVID. 26 The most common aspects of fitness tracked by Australians in this study were steps (45%) followed by heart monitoring (29%) and sleep (25%). 26 In contrast to common beliefs, Corbett & Schwager found that older generations represented the most growth in the uptake of wearables, with the use of fitness bands growing from 17% in 2020 to 23% in 2021 for this segment of the population. 26
Early research suggests that wearables contribute to health self-efficacy. For example, Paré and colleagues (2018) surveyed 4109 Canadian adults stratified by region and used a quota method to ensure representation of age and gender. They found that adults who use digital trackers reported feeling more knowledgeable and informed about their health. Moreover, 70% of users in this same study believed they had maintained or improved their health status by using self-tracking devices. 27 Mobile apps and wearables look set to be an important component of health care in the future, encouraging greater health self-awareness, detection, monitoring and increasing health self-efficacy. However, access is not equitable in Australia. Affordability and connectivity limit choices and opportunities to use current heath technologies for many Australians, including those with lower incomes, people living remotely and Aboriginal and Torres Strait Islander people. Moreover, systemic racism, including unwanted surveillance (observation for health or other purposes) and deficit discourse (written or verbal communication represents Aboriginal and Torres Strait Islander people in terms of deficiency or failure) 28 that has historically informed Western health systems’ approach, impacts the choices offered to and the services/products requested by Aboriginal and Torres Strait Islander people. These same barriers may also influence Aboriginal and Torres Strait Islander peoples’ uptake of wearables. The systemic obstacles that have contributed to the current gap in health and life span remain and threaten to widen the gap as new technologies become ubiquitous in the broader Australian population. Therefore, it is critical that we understand Aboriginal and Torres Strait Islander peoples’ needs and requirements for new health technologies, including wearables, and design policies and practices to meet these needs.
Minimal research exists which relates to wearables among Aboriginal and Torres Strait Islander people. No research has specifically targeted mature aged Aboriginal and Torres Strait Islander people, despite the fact that the percentage of mature aged Aboriginal and Torres Strait Islander people is growing and is predicted to continue to grow to over 20% by 2031. 29 This lack of research attention is significant because Aboriginal and Torres Strait Islander people experience poorer health and chronic illness significantly higher than the broader population. 11 Moreover, the approach to health care innovation has typically been to adapt what works best for the wider population rather than understanding and incorporating the needs of Aboriginal and Torres Strait Islander people in the design of the system, policy or practice. We are aware of only one study related to wearables that purposefully included Aboriginal and Torres Strait Islander adults. Maxwell et al. conducted a study that included eight Aboriginal and Torres Strait Islander women students and concluded that wearables could improve the outcomes and experience of physical activity for Indigenous women. They identified three themes associated with Indigenous women's use of wearables: (1) quantified self, (2) governance by micro-nudge and (3) increased agency and empowerment. 30 Specifically, they found that measurement enhanced self-efficacy. Participants indicated that the quantitative data they got from trackers increased their self-health knowledge. This data included understanding their requirements for sleep, awareness of elevated heart rate and the amount of exercise they engaged in. 30 Participants uniformly interpreted micro nudges in the form of a buzzer as motivating and assisted participants in making healthier choices. 30 The flexibility afforded by the trackers enabled participants to choose activities that suited their circumstances and constraints and address common barriers such as being time-poor, which increased their feelings of agency and empowerment. 30 These findings are encouraging and warrant further investigation. An essential next step is to determine if Aboriginal and Torres Strait Islander people are currently using phone apps or wearables to track their health.
Aims
This study aimed to determine if mature aged Aboriginal and Torres Strait Islander adults living in rural, regional and remote locations:
use social media to acquire and share health information and, if so, what platforms they use and trust; use mobile apps or wearable trackers and, if so, what aspects of health they track; are interested in using mobile apps and wearables to track health.
Methods
Ethics
The study adhered to the guidelines for ethical research in Aboriginal and Torres Strait Islander populations and relevant ethics committee approvals. We obtained approvals from the Aboriginal Health and Medical Research Council Ethics Committee (AH&MRC) (reference 1862/21) approved 1/12/2021, and an amendment specific to this study was approved on 12/05/2022, and this manuscript was reviewed and approved by our APG and the ethics committee of the AHMRC.
Aboriginal and Torres Strait Islander governance
An Aboriginal Governance Group (APG) who are also overseeing a larger program of research provided governance for the research. A senior Aboriginal member of the research team, an Elder and an Associate Professor (BR) oversaw the project. The study was co-designed and co-implemented with the local Aboriginal Community Controlled Health Services (ACCHS) in each community. Our research team has a long-standing and trusted relationship with each of these ACCHS and this specific research extends previous co-designed studies examining health awareness and monitoring and management. The research team was comprised of Aboriginal (BR, BC, FC, GS) and non-Aboriginal people (CH, JC, JG, DM, KW, KG), and Aboriginal peoples’ perspectives were privileged throughout the design, data analysis and interpretation of the findings.
Design
We administered a cross-sectional survey via an in-person semi-structured interview in collaboration with the local ACCHS in three New South Wales locations (one each: rural, regional and remote). 22 Aboriginal adults who attended a health promotion event which was facilitated by the local Aboriginal Medical Services Centres (AMS) in each location, were approached in-person and asked if they were willing to participate in a brief interview to share their perspectives about using social media and wearables to gain health information. The health promotion event was promoted by the AMS's via posters, social media and radio in the community and patients of the service were also directly invited to attend the event by their health care providers. Virtually all attendees we approached agreed to participate. Aboriginal and Torres Strait Islander adults were eligible for the study if they were 18 years or older and able to give informed consent to participate. Participants consented to participate and were free to withdraw at any time.
The 13-item survey was co-designed with the APG and included yes/no, multiple-choice (choose one option) and multiple-choice (choose all that apply) questions related to the use of and trust in social media in obtaining and sharing health information and the use of apps and wearables for tracking personal health information. The survey also included demographic questions (birth year and multiple-choice self-identified gender – options included: binary (female, male), nonbinary, trans, other and prefer not to say). 31 1
Data from the in-person semi-structured interviews were entered directly into Lime Survey 32 using a tablet during the interview and later exported to MS Excel version 16.61.
Results
This study included n = 78 participants from three locations: n = 19(24%) regional, n = 25(32%) rural and n = 34(44%) remote. 22 We create two age cohorts: mature aged, comprising Seniors, Baby Boomers and Generation X, who were born prior to 1981 (>41years old) and a younger cohort, comprising Millennials and Generation Z who were born 1981 or later (≤41 years old), and who grew up with the internet. 33 See Table 1 for specifics including age, gender and location cohorts. Notably, n = 59(76%) were over 41 years old and n = 39(50%) were women aged over 41 years old.
Demographics.

Note: Denominator is full sample n = 78.
Social media use
Most participants, n = 56(72%), used social media, and n = 43(55%) described daily use. Only n = 20(25%) of all participants indicated that they did not use social media. More than double the proportion of mature aged women used social media daily (56%) compared to mature aged men (17%), and less than half the proportion of mature aged women indicated they never use social media (23%) compared to mature aged men (50%) (see Table 2).
Frequency social media use.

Note: Denominator = n for each cohort listed on top row.
While younger participants were more frequent (daily) users of social media compared with mature aged participants n = 16(89%) and n = 26(44%) respectively the majority of mature aged participants n = 38(64%) used social media. Moreover, of the n = 39 mature aged women, n = 30(77%) used social media and n = 22(56%) used it daily. Only younger women were more likely use social media with 100% reporting at least some use and n = 11(92%) daily use. Mature aged men were the least frequent users n = 7(39%). Just over 70% of participants in each of the three locations reported using social media, with around 50% using it daily.
Acquiring health information
Participants who described themselves as using social media, used one or more platforms for acquiring health-related information (see Table 3). Facebook was the most common platform, with n = 27(48%) of those who use social media acquiring health-related information through Facebook. Notably, Facebook was the platform most frequently cited by each cohort for acquiring health information. The ACCHS website was used by n = 14(25%) of all participants, and n = 13(23%) participants used YouTube to acquire health information.
Social media platforms/websites used to acquire health information.

Note: Denominator = n for each cohort listed on top row.
Sharing health information
Participants also used social media to share health-related information. Facebook was the most frequently used by all cohorts for sharing health information. The ACCHS site and YouTube were also used frequently (see Table 4).
Social media platforms/websites used to share health information.
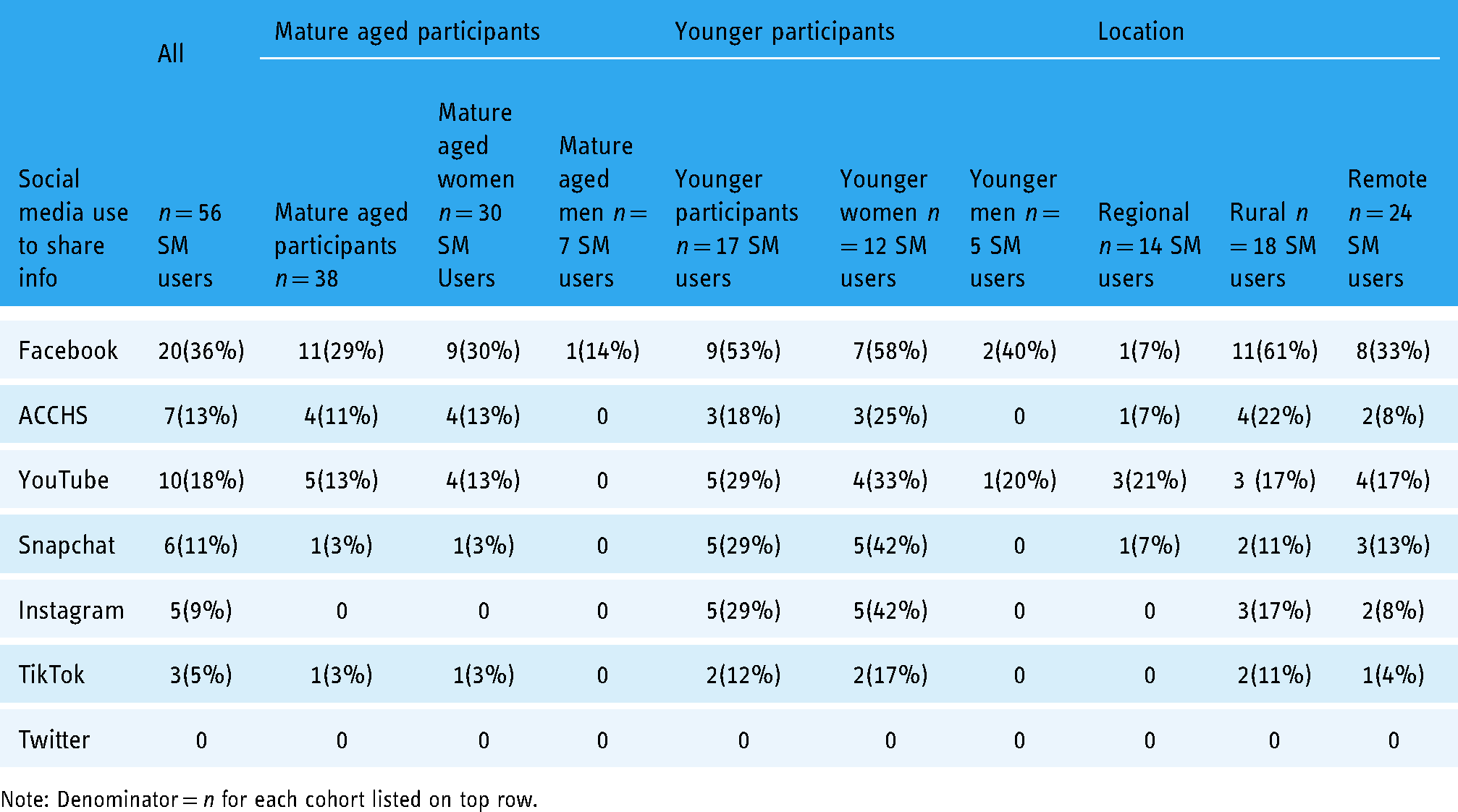
Note: Denominator = n for each cohort listed on top row.
Participants shared health-related information online and more frequently in real life (IRL). Both mature aged and younger women more frequently than men shared health information with a wide variety of people, most frequently with family members but also with friends, colleagues and others (see Table 5).
Shared health information online and in real life (IRL) (age and gender cohorts).

Note: Denominator = n for each cohort listed on top row.
Participants in all geographic locations shared health information with rural and remote locations sharing in real life more frequently and regional users sharing more frequently online (see Table 6).
Social media platforms/websites used to share health information online and IRL (location cohorts).

Note: Denominator = n for each cohort listed on top row.
Trusted source of health information
The two platforms most frequently trusted to provide accurate health information by the social media users were the ACCHS website n = 20(36%) and Facebook n = 18(32%). Social media users also indicated they trusted n = 10(18%) other government websites and n = 9(16%) indicated they trusted YouTube to provide accurate health information. A little over a third of participants n = 20(36%) indicated that they did not trust any social media platform to provide accurate health information (see Table 7).
Social media platforms/websites trusted to provide accurate health information.

Note: Denominator = n for each cohort listed on top row.
Fitness tracker use
Participants used a smart phone n = 15(19%) or a wearable fitness tracker n = 7(9%) to track some aspect of their health or fitness, including steps, other types of exercise, diet, sleep and period. Younger people were the more frequent users of tracking apps and wearables with n = 6(50%) younger women indicating they had used a smart phone and n = 4(25%) had used a wearable fitness tracker. No mature aged men had used either device for health tracking (see Table 8).
Fitness tracker use.
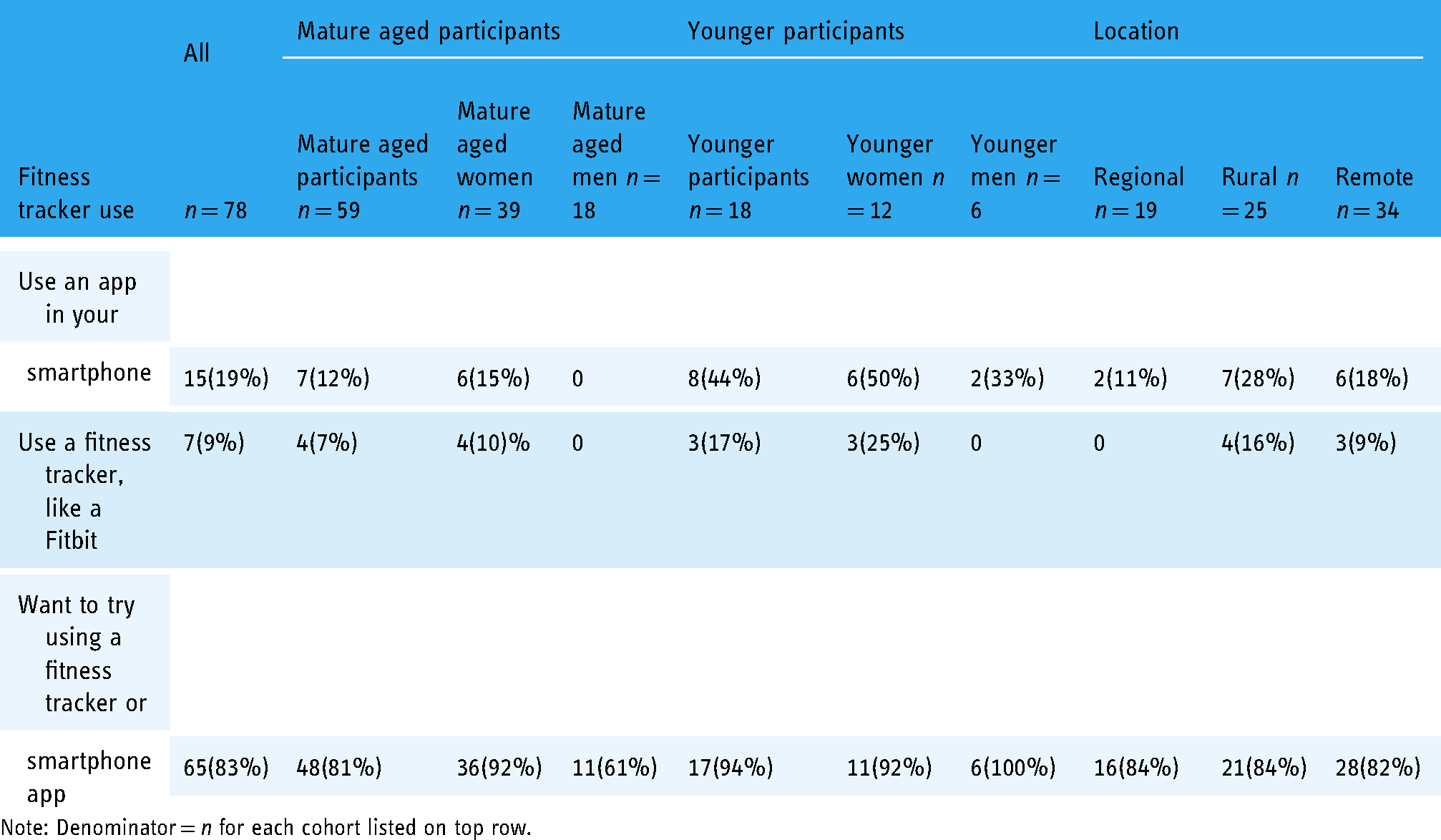
Note: Denominator = n for each cohort listed on top row.
Most participants indicated they would like to try a fitness tracker n = 65(83%), which was consistent across each of the location types. Likewise, 100% of younger men, and 92% of mature aged and younger women expressed interested in trying a fitness tracker.
Discussion
Our co-designed study, which recruited from three geographically diverse locations, is the largest study of Aboriginal and Torres Strait Islander adults’ use of wearable health trackers. The study, mainly comprising mature aged adults, found that individuals in these non-urban locations use digital technologies to acquire and share health information despite well-documented barriers, including connectivity and affordability. 34 Moreover, while only a few participants (7%) had actually used a fitness tracker an overwhelming number of participants (83%) expressed a desire to try a fitness tracker or smart phone app to track exercise, diet, or other habits.
The present study builds on work by Maxwell et al., which found that Indigenous women students perceived wearables as enhancing their experiences and assisted in achieving goals of being more active. 30 Findings from our community sample indicated that Aboriginal and Torres Strait Islander mature aged adults, particularly mature aged women, are interested in trying a fitness tracker. Our study also builds on the growing body of work that has shown the Aboriginal and Torres Strait Islander people use social media for a variety of purposes, including for health communication.8,19,35,36
Disaggregating data for mature aged and younger Aboriginal and Torres Strait Islander women and men in this study illuminates differences in how different age and gender cohorts use social media for health. In keeping with Corbett & Schwager finding that older Australians represent the most growth in use of wearables, 26 81% of the mature aged participants in this study expressed an interest in using a health tracker, and 92% of the 39 mature aged women indicated their interest in using a health tracker. An important next step is research to better understand discrepancy between desired and actual use of fitness trackers and phone apps, including specifically exploring the barriers for Aboriginal and Torres Strait Islander people living in non-urban locations to use of apps and trackers,
This study found that mature aged participants were active social media users, with 43% using one or more platforms daily. In keeping with previous studies, women and particularly younger women in this study used social media more compared to men. 37 However, the observation that mature aged Aboriginal women frequently use social media to acquire health information and that they shared health information they acquired with a diversity of family, friends and colleagues (both online and in real life) is a particularly valuable finding. This insight points to a community strength that could be used to help disseminate relevant and timely health information to not only social media users but also community members that do not use social media themselves. This is particularly relevant in Aboriginal and Torres Strait Islander communities where mature aged women are often seen as influencers and trusted advisors.38–40 An important next step is to explore what types of health information each cohort finds most relevant and examine other characteristics of the messaging that impact trust and sharing.
Whilst the numbers are small, participants in rural and remote locations more frequently used social media (other than YouTube) to acquire and share health information compared to regional. This finding is intriguing considering previous findings that remoteness in Australia is associated with less internet use. 41 Given that only three locations were included in this study, additional research that specifically examines how frequently people living in other rural, remote or very remote locations, seek and share health information obtained online is needed. It will also be important to understand if different cohorts from the locations differ in frequency and how they use social media to acquire or share health information.
The two most used and trusted platforms across all cohorts were the ACCHS website and Facebook. These platforms may provide an avenue to reach Aboriginal and Torres Strait Islander people, including mature aged adults, with accurate and timely health information. Likewise, YouTube, while not as popular, is used and trusted by a reasonable proportion of social media users and may provide an opportunity to provide health information in visual or oral narrative formats identified as appealing to Aboriginal and Torres Strait Islander people. 17
Strengths and limitations
This study is a preliminary exploration of mature aged Aboriginal and Torres Strait Islander peoples’ use of and interest in user-focused technologies, including social media, phone apps and wearable trackers to acquire health information/data. Social media and phone app use require at least intermittent internet connectivity. Rural and remote locations in Australia are known to have less reliable internet connectivity compared to urban locations. Moreover, costs can reduce or prohibit internet use particularly for individuals using pre-paid services. We did not ask participants about the consistency of or any barriers to connectivity such as availability or costs, which may impact use and even interest in these technologies. Gathering this information in subsequent studies may help to explain differences between desired use of apps and wearables and previous use. Likewise, a brief survey with a convenience sample across three non-urban locations provides useful information for the ACCHS serving these locations but limits the generalisability of the findings Aboriginal and Torres Strait Islander people living in other localities. While the short survey provided valuable data, it did not give a rich picture of how these technologies are currently used or detail what Aboriginal and Torres Strait Islander people want and need from these technologies. Also, the sample size, while the largest community sample to explore the use of wearables, is too small to enable more sophisticated statistical comparisons between different age, gender and location cohorts. Another limitation is the potential impact of social desirability on participant responses, causing participants to describe more frequent use of social media and wish to try health trackers.
Despite these limitations, this study demonstrated that Aboriginal and Torres Strait Islander people, including mature aged adults from non-urban geographically diverse communities, are interested in and use social media, phone apps and wearables for health purposes.
This research benefited from Aboriginal and Torres Strait Islander governance, leadership and community engagement. Historically, new health care practices and technologies have been developed with little or no input from cultural experts. The move to digital health provides an opportunity to shift to an approach that privileges Aboriginal and Torres Strait Islander perspectives, thus building on the inherent strengths of adaptability and innovation. The collaborative co-design approach which privileged Aboriginal researcher perspectives helped to ensure the design was culturally safe and that we collected relevant data. Moreover, the results of this research will be disseminated in lay language (video and written) to each ACCHS. Likewise, data disaggregated by location enables each ACCHS to better understand the people it serves and use the data to inform health messaging and determine the relevance of future translational research related to digital health in their community. This disaggregation is an important first step in recognising the significant diversity of Aboriginal and Torres Strait Islander people and designing digital health products and services to meet the specific needs of different cohorts.
Knowledge to action
Co-designed digital health research which privileges Aboriginal and Torres Strait Islander perspectives to better understand the needs and requirements of different cohorts within communities is the next step. In-depth qualitative and quantitative research is necessary to understand the enablers and barriers that impact the use and efficacy for Aboriginal and Torres Strait Islander people of different ages, genders and community types. Privileging the perspectives of Aboriginal and Torres Strait Islander people is critical to inform practices, programs and policies related to implementing user-focused technologies for health communication and self-tracking. Building in user expertise through co-designed research will help to ensure that the subsequent programs and services are culturally safe and efficacious for Aboriginal and Torres Strait Islander people.
Conclusion
Aboriginal and Torres Strait Islander peoples’ propensity for early adoption and innovation suggests a path for addressing health disparities as digital health solutions become available. The promising findings of this research highlight the need for in-depth co-designed research to understand the unique needs and requirements of Aboriginal and Torres Strait Islander people to inform the design of user-focused health communication and health-tracking programs and services.
Footnotes
Acknowledgements
We thank Armajun Aboriginal Health Services and Brewarrina Aboriginal Medical Services as key partners and thank the staff members in these services for their assistance in this research. We would like to thank Walanga Muru for their support of this research. We thank Djurali Aboriginal and Torres Strait Islander Health Research Group for their support. We would also like to thank our APG for their leadership and guidance in this research.
Contributorship
CH, KG, GS and FC researched literature and conceived the study. CH, KG, GS, FC were involved in protocol development, gaining ethical approval, GS, KW, DM were involved participant recruitment, JC, FC, GS, CH, KG were involved in survey design and CH, KG, JG, GS, FC data analysis and interpretation. BR, FC and GS provided cultural oversight. CH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study adhered to the guideline for ethical research in Aboriginal and Torres Strait Islander populations and relevant ethics committee approvals. We obtained approvals from the Aboriginal Health and Medical Research Council Ethics Committee (AH&MRC) (reference 1862/21) approved 1/12/2021, and an amendment specific to this study was approved on 12/05/2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Macquarie University (grant number 20213896 Allocation for PhD students).
Guarantor
CH.
Statement related to gender and age language in this manuscript
This research is focused on how mature aged Aboriginal and Torres Strait Islander women use digital health. Our definition of ‘mature aged’ is in keeping with a person's age when internet usage became common. We are therefore defining ‘mature aged’ as generations known as Seniors, Baby Boomers and Generation X, who did not grow up with the internet. 42 Millennials who were born after 1980 (<41 years old) are generally thought to be more comfortable with technology and especially social/interactive media compared with mature aged generations. 43
With regard to gender, we are aware and respect that Aboriginal and Torres Strait Islander people of all ages describe themselves as gender-binary, non-binary, trans and/or other. 44 Participants in our studies self-identify their gender. Therefore, an Aboriginal and Torres Strait Islander person who identifies themselves as a women some or all of the time, are included in the studies focused on women. For our studies that include people other than women, we provide a variety of gender options and people are encouraged to self-identify with any description or to choose to not to provide a description of their gender. 44