
Abstract
Background
Obesity in adolescence is associated with many adverse health and well-being outcomes. Physical activity plays an important role in the prevention of obesity; however, many adolescents with overweight and obesity are physically inactive. Digital behaviour change interventions (DBCI) are increasingly used to increase physical activity; however, there is insufficient evidence on their use in promoting physical activity among adolescents with overweight and obesity, including its active components. This review aims to evaluate the effectiveness of DBCIs in promoting physical activity among adolescents with overweight and obesity and to identify the behaviour change techniques (BCTs) used in these interventions.
Methods
Seven electronic databases were searched for randomized controlled trials and quasi-experimental studies evaluating DBCIs for physical activity promotion in adolescents with overweight and obesity aged 10–19 years. The risk of bias in the included studies was assessed using Cochrane's Risk of Bias tool 2 and ROBINS-I tool. Meta-analyses were performed using random effects models. The BCTs used within the DBCIs were coded using the Behaviour Change Technique taxonomy (v1).
Results
Eighteen studies involving 1769 participants were included. DBCIs showed a large, significant positive effect on total physical activity (SMD = 1.61, 95% CI: [0.56, 2.66], p = 0.003), but non-significant effects on moderate-to-vigorous physical activity (MVPA) (SMD = 0.16, 95% CI: [−0.39, 0.71], p = 0.56) and step count (SMD = −0.10, 95% CI: [−0.52, 0.32], p = 0.65). High heterogeneity was observed in total physical activity and MVPA analyses. The most frequently used BCTs were information about health consequences, goal setting, self-monitoring, feedback on behaviour and social support.
Conclusion
DBCIs can effectively promote overall physical activity among adolescents with overweight and obesity, although their impact on MVPA and step count remains unclear. Future research should focus on optimizing BCT combinations and improving long-term engagement while addressing intervention effect variability.
Systematic review registration
PROSPERO CRD42021270008
Keywords
Background
Overweight and obesity among adolescents have become a significant global health concern. According to the World Health Organization (WHO), the prevalence of overweight or obesity in children and adolescents aged 5–19 years increased from 10% in 1990 to 28% in 2022. 1 This trend is particularly concerning, as obesity during adolescence tends to persist into adulthood, increasing the risk of chronic health conditions. 2 Adolescents with overweight and obesity face numerous health consequences, 3 including metabolic disorders, 4 cardiovascular diseases 5 and psychological challenges such as low self-esteem, poor body image and increased risk of mental health disorders.6,7 These health risks, combined with social stigmatization and discrimination, 8 highlight the urgent need for effective interventions to promote healthy lifestyles in this population.
Physical activity is crucial in managing obesity among adolescents, with WHO recommending at least 60 minutes of moderate-to-vigorous physical activity (MVPA) daily, including muscle- and bone-strengthening activities three times weekly. 9 Despite the well-established benefits of physical activity, including improved body composition, 10 cardiovascular fitness, 11 and mental health outcomes, 12 many adolescents with overweight and obesity fail to meet the recommended levels of MVPA. 13 Common barriers include low motivation, body image concerns, limited access to physical activity opportunities, and the increasing prevalence of sedentary behaviours.14–17
Digital behaviour change interventions (DBCIs) have emerged as a promising approach to promote physical activity, using technologies such as smartphones, wearable devices, and the internet to deliver behaviour change strategies. 18 These interventions offer advantages such as broad reach, cost-effectiveness and personalized content delivery.19–21 Previous reviews have shown that technology-based interventions can effectively promote physical activity in adolescents.22,23
A crucial aspect of understanding intervention effectiveness is examining the specific components that drive behaviour change. The Behaviour Change Technique (BCT) Taxonomy v1 provides a standardized method for identifying and coding the ‘active ingredients’ of interventions. 24 This taxonomy comprises 93 distinct BCTs organized into 16 clusters, enabling systematic description, replication and synthesis of successful intervention approaches. 24 DBCIs commonly incorporate various BCTs, such as goal setting, self-monitoring, feedback and social support, delivered through engaging features such as gamification and virtual coaching.25–27 Understanding which BCTs are most effective in digital interventions targeting adolescents with overweight and obesity is essential for optimizing future intervention designs.
While individual studies have examined digital interventions for physical activity promotion in adolescents with overweight and obesity, several knowledge gaps exist. These include the lack of a systematic synthesis specifically focusing on this population, limited understanding of effective BCTs, and the need for an updated review capturing recent technological advances. Furthermore, most reviews have focused on the general adolescent population, without specifically examining the effectiveness of DBCIs among adolescents with overweight and obesity, who may face unique barriers to physical activity engagement. 14 Therefore, this systematic review and meta-analysis aims to address two research questions: (1) What is the effectiveness of DBCIs in promoting physical activity among adolescents with overweight and obesity? and (2) Which BCTs are most commonly used in DBCIs targeting physical activity promotion in adolescents with overweight and obesity? This review will provide an overview of the current state of evidence into the overall effectiveness of these interventions, and inform the development and implementation of digital interventions promoting physical activity among adolescents with overweight and obesity.
Methods
This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 28 (Supplementary Appendix A). The systematic review protocol has been described in full elsewhere 29 and was registered with the International Prospective Register of Systematic Reviews (PROSPERO) prior to the commencement of data extraction (CRD42021270008).
Eligibility criteria
Studies were included in the systematic review if they met the following criteria, defined using the PICOS framework:
Population
The study participants were adolescents aged 10–19 years, classified as overweight or obese according to age- and sex-specific body mass index (BMI) percentiles, with overweight defined as a BMI between the 85th and 95th percentile and obesity defined as a BMI at or above the 95th percentile. 30 Studies that included a mixed population of overweight, obese, and normal-weight adolescents were eligible if they reported subgroup analyses for the overweight and obese participants or if the majority (>50%) of the study population was overweight or obese.
Intervention
Eligible studies included DBCIs aimed at promoting or increasing physical activity, either as a primary or secondary goal. Digital interventions included, but were not limited to, smartphone apps, websites, wearable devices, exergames, text messaging programmes or social media-based interventions. Interventions combining digital and non-digital components were included if the digital technology was integral to delivering the core intervention content, rather than serving only as a supplementary tool.
Comparators
Studies were eligible if they compared the effectiveness of DBCI to a control condition, such as no intervention, usual care, waitlist control or non-digital intervention (e.g. face-to-face counselling, printed materials). Studies that compared two or more DBCIs without a control condition were also eligible, as they could provide valuable information about the relative effectiveness of different intervention designs, BCTs or delivery modes.
Outcomes
The primary outcomes of interest were objectively or subjectively measured changes in physical activity levels. Objective measures of physical activity included accelerometers, pedometers or heart rate monitoring, which provide direct and reliable data on the frequency, duration and intensity of physical activity. 31 These devices could capture various aspects of physical activity, such as minutes spent in MVPA, steps per day or metabolic equivalence of task (MET) hours. 32 Subjective measures included self-reported questionnaires, diaries or interviews, which rely on participants’ recall and perceptions of their physical activity levels. 33 Secondary outcomes (if reported) included changes in body composition (e.g. BMI, waist circumference, body fat percentage), changes in fitness measures (e.g. cardiovascular fitness, muscle strength), psychosocial outcomes (e.g. self-efficacy, motivation, quality of life), behavioural outcomes (e.g. sedentary behaviour, screen time, or dietary habits) or physiological outcomes (e.g. blood pressure, lipid profiles).
Study designs
Eligible study designs included randomized controlled trials (RCTs), cluster RCTs and quasi-experimental studies with a control group.
Non-eligible studies
Studies were excluded from the review if (a) they focused solely on children (<10 years) or adults (>19 years); (b) studies where the digital component was not the primary mode of intervention delivery (i.e. digital technologies were used only for data collection or as a minor supplement to a primarily non-digital intervention). Hybrid interventions were excluded if the digital components were not central to delivering the core intervention content; (c) interventions targeting only diet or other health behaviours without a physical activity component; (d) studies without a control or comparison group; (e) cross-sectional studies, case reports, qualitative studies, conference abstracts, protocols and review articles; and (f) studies not published in English. No restrictions were placed on the publication date of studies.
Information sources and search strategy
A comprehensive literature search was conducted to identify relevant studies published up to April 2024. The following electronic databases were searched: PubMed/MEDLINE, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), PsycINFO, EMBASE and CINAHL. The search strategy included a combination of Medical Subject Headings (MeSH) terms and free-text keywords, adapting the search strategy for each database as necessary. The search strategy included terms related to four main concepts: (a) population: adolescents, teenagers, youth; (b) condition: overweight, obesity; (c) intervention: digital interventions, eHealth, mHealth, apps, web-based; and (d) outcome: physical activity, exercise, fitness. The search terms were adapted for each database and were combined using Boolean operators (AND, OR) and proximity operators (e.g. ADJ, NEAR) as appropriate. An example of the full search strategy used for PubMed/MEDLINE is provided in Supplementary Appendix B. This strategy was adapted for use in other databases, accounting for database-specific syntaxes and subject headings. To ensure comprehensive coverage, the reference lists of included studies and relevant systematic reviews were manually searched to identify additional eligible studies. No date restrictions were applied to ensure a comprehensive review of all relevant literature.
Study selection process
The study selection process for this systematic review and meta-analysis followed a two-stage approach, which included an initial screening of titles and abstracts, followed by a full-text review of potentially eligible studies. This process was conducted independently by two reviewers (PS and NF) to minimize the risk of bias and ensure the reliability of the study selection. In the first stage, the titles and abstracts of all records identified through the search strategy were screened against the predefined eligibility criteria using a standardized screening tool. Records that did not meet the eligibility criteria were excluded at this stage. If there was insufficient information in the title and abstract to determine eligibility, the record was retained for full-text review. Any disagreements between the reviewers were resolved through discussion or by consulting a third reviewer (NAM) if necessary. In the second stage, the full-text articles of all potentially eligible records were retrieved and reviewed. The reviewers independently assessed each full-text article against the eligibility criteria using a standardized data extraction form. Any disagreements were resolved through discussion or by consulting a third reviewer (NAM) if necessary. The reasons for excluding studies during the full-text review were recorded. Studies were excluded at this stage if they did not meet the eligibility criteria related to the population, intervention, comparator, outcomes, or study design, or if the full text was not available or the article was a duplicate publication. The study selection process was documented using a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. 34
Data extraction and management
All search results were imported into EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA) for deduplication. After deduplication, the remaining records were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) for screening and data extraction. Following the study selection process, relevant data were extracted from the included studies using a standardized data extraction form. Two reviewers (PS and NF) independently extracted data from each included study. Any discrepancies in the extracted data were resolved through discussion, and if necessary, by consulting a third reviewer (NAM).
The following information was extracted from each study:
Study characteristics: first author's name, year of publication, country of study, study design (e.g. RCT, cluster RCT, quasi-experimental), sample size (total and per group), study duration and follow-up periods Participant characteristics: age (mean, range), gender distribution, baseline BMI or weight status, any relevant sociodemographic information Intervention details: type of digital technology used (e.g. smartphone app, website, wearable device), description of the intervention components, duration and frequency of the intervention, theoretical framework used (if any), BCTs employed (coded using the BCT Taxonomy v1), details of any non-digital components (if applicable) Comparison group details: description of the control or comparison condition Outcome measures: (a) primary outcome: physical activity measures (e.g. minutes of MVPA, steps per day, total physical activity), including measurement tool used (e.g. accelerometer, pedometer, self-report questionnaire), and time points of measurement; (b) secondary outcomes (if reported): body composition measures (e.g. BMI, body fat percentage), physical fitness measures, including measurement tools and units, and time points assessed Results: (i) main findings for primary and secondary outcomes; (ii) between-group differences and effect sizes (if reported); (iii) mean and standard deviations or other relevant statistical analyses used. Additional information: (a) funding sources, (b) conflicts of interest, (c) ethical approval.
For studies with multiple intervention arms, data for all relevant comparisons were extracted. If any required data were missing or unclear in the included studies, attempts were made to contact the study authors for clarification. If the authors did not respond or were unable to provide the requested information, the study was analysed using the available data, and the missing data were noted in the review. To ensure accuracy and consistency in data extraction, the data extraction data form was piloted on a random sample of five included studies. This process allowed us to refine the form and establish a common understanding among reviewers before proceeding with full data extraction. All extracted data were entered into a spreadsheet with each study assigned a unique identifier. For the BCT coding, two reviewers (PS and NF) independently coded the BCTs used in each intervention using the BCT Taxonomy v1.
24
Any disagreements in coding were resolved through discussion or by consulting a third or fourth reviewer (NF/CE).
Assessment of risk of bias
The quality of the included studies was assessed independently by two reviewers (PS and NF) using standardized tools. For randomized controlled trials (RCTs) and cluster RCTs, the risk of bias was assessed using the Cochrane Risk of Bias Tool (RoB 2). 35 This tool evaluates the risk of bias across five domains: (a) randomization process, (b) deviations from intended interventions, (c) missing outcome data, (d) measurement of the outcome, and (e) selection of the reported result. Each domain was judged as having a low risk, high risk, or some concerns of bias, and an overall risk of bias judgment was made for each study based on the domain-level judgements. For quasi-experimental studies, the risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool. 36 This tool evaluates the risk of bias across seven domains: (a) confounding, (b) selection of participants into the study, (c) classification of interventions, (d) deviations from intended interventions, (e) missing data, (f) measurement of outcomes, and (g) selection of the reported result. Each domain is judged as having a low risk, moderate risk, serious risk, or critical risk of bias, and an overall risk of bias judgment is made for each study based on the domain-level judgments. Any disagreements between the reviewers regarding the quality assessment were resolved through discussion or by consulting a third reviewer (NAM).
Data synthesis and analysis
The extracted data from the included studies were synthesized using both qualitative and quantitative methods. The approach to data synthesis was as follows:
Qualitative synthesis
A narrative synthesis was conducted to summarize the key characteristics, methodological quality, and main findings of the included studies. This synthesis was structured around the following aspects: (a) characteristics of the digital interventions (e.g. type of technology used, duration, frequency of use); (b) BCTs employed in the interventions; and (c) patterns in the effectiveness of interventions across different study characteristics.
Quantitative synthesis (meta-analysis)
A meta-analysis was conducted using Review Manager 5.4 (The Cochrane Collaboration, 2020) for outcomes reported by at least two studies with comparable measures. The meta-analysis followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions and was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 37
The primary outcome of the meta-analysis was changes in physical activity levels from baseline to post-intervention. If studies reported multiple physical activity outcomes, objective measures (e.g. accelerometer data) were prioritized over self-reported measures. If studies report outcomes at multiple time points, the longest follow-up data was used to assess the sustained effects of the interventions. For physical activity outcomes, standardized mean differences (SMDs) were calculated to account for differences in measurement tools and units across studies. The meta-analysis was conducted using a random-effects model due to the expected heterogeneity among studies. The inverse variance method was used to weight the studies. Statistical heterogeneity was assessed using the I² statistic and the chi-squared test, with values of 25%, 50% and 75% indicating low, moderate and high heterogeneity, respectively. Sensitivity analyses were performed to assess the robustness of the meta-analysis results, by excluding studies with high risk of bias and non-randomized studies. All statistical tests were two-sided, with p < 0.05 considered statistically significant. Outcomes that could not be meta-analysed were narratively reported due to insufficient data or incompatible outcome measures. To address the issue of missing data, we contacted study authors for additional information when necessary. If data remained missing, we used available information (e.g. t-values, p-values) to calculate effect sizes where possible.
Behaviour change techniques (BCT) analysis
The BCTs used in each intervention were coded using the BCT Taxonomy v1. 24 Two reviewers (PS and NF) independently coded the BCTs, with disagreements resolved through discussion or consultation with a third and fourth reviewer (NAM/CE). The frequency of each BCT across interventions was calculated using descriptive analysis.
Results
The study selection process, following the PRISMA guidelines, is summarized in Figure 1. The initial electronic database search yielded a total of 2497 records. After removing duplicates, 2125 records were screened based on their titles and abstracts. Of these, 1954 records were excluded as they did not meet the inclusion criteria. The remaining 171 articles underwent full-text review to assess their eligibility for inclusion in the systematic review and meta-analysis. During this stage, 152 articles were excluded for the following reasons: not targeting adolescents with overweight or obesity (n = 49), not using a DBCI (n = 37), not focusing on physical activity promotion (n = 29), not a randomized controlled trial or quasi-experimental study (n = 19), no relevant physical activity outcomes reported (n = 17), and duplicate or secondary analysis of an included study (n = 2). The study selection process was conducted independently by two reviewers (PS and NF), with disagreements resolved through discussion or by consulting a third reviewer (NAM). The high level of agreement between the reviewers (Cohen's κ = 0.86) indicates the reliability of the study selection process. Additionally, two articles were identified through hand-searching the reference lists of the included studies and relevant systematic reviews. These articles underwent the same selection process as the records identified through the electronic database search. In total, 18 studies met all the inclusion criteria and were included in the qualitative synthesis. These studies comprised 15 randomized controlled trials and three non-randomized controlled studies. Of these, 13 studies provided sufficient data for inclusion in the meta-analysis.

PRISMA flow diagram.
Study characteristics
The key characteristics of the 18 studies included studies in the systematic review are summarized in Table 1. The included studies were published between 2006 and 2022, and were conducted across various regions, with the majority being the USA (n = 7),38–44 followed by Europe (n = 5),45–49 Asia (n = 4)50–53 and Australia (n = 2).54,55 The study designs were predominantly randomized controlled trials (RCTs) (n = 15, 83.3%), with the remaining studies being non-randomized studies. The total number of participants across all included studies was 1769, with sample sizes ranging from 31 to 361 participants. The mean age of participants ranged from 10.5 to 16.8 years. The proportion of female participants varied across studies, with some studies having an equal distribution of males and females, while others had a higher proportion of either gender,41,42,45,47,52 or only one gender (girls).38,39,49,54
Summary of study characteristics.
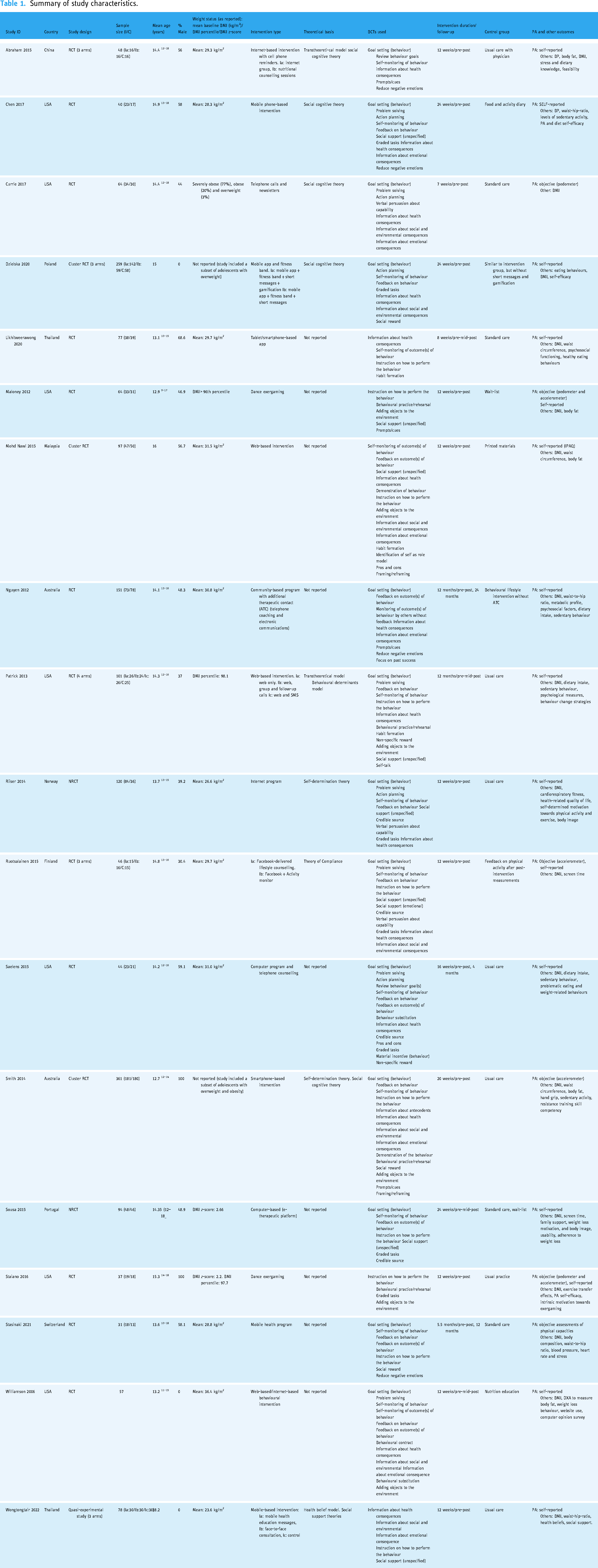
All included studies targeted adolescents with overweight or obesity, with most studies using BMI percentile or z-score to define overweight and obesity status. The mean baseline BMI ranged from 28.3 kg/m2 to 36.4 kg/m². Some studies also used waist circumference,44,51,52 waist-to-hip ratio44,45,55,56 or body fat percentage41,45,51,53,54 as additional measures of obesity. The duration of the intervention ranged from 4 weeks to 24 months, with the majority of studies lasting between 3 and 6 months.
The digital platforms used to deliver the behaviour change interventions included websites (n = 5),38,41,46,48,51 mobile devices (n = 5),44,45,50,52,54 wearable devices (n = 2),47,49 social media (n = 1), 47 telephone calls (n = 3)40,43,55 and dance exergaming (n = 2).39,42 Some studies used a combination of digital platforms to deliver the intervention components.40,41,47,49,53,55
The most common BCTs incorporated in the interventions were goal setting (behaviour) (n = 13), information about health consequences (n = 12), self-monitoring of behaviour (n = 11) and feedback on behaviour (n = 9), as coded using the BCT Taxonomy v1. 24 The number of BCTs used in each intervention ranged from 4 to 14, with a median of eight BCTs per intervention.
The included studies utilized various theoretical frameworks as guidance for the interventions. Social Cognitive Theory was the most prevalent, serving as the foundation in five studies (27.8%).43,44,49,53,54 Two studies utilized the Transtheoretical Model as their theoretical framework,41,53 while two others based their intervention on Self-Determination Theory.48,54 Additionally, several studies drew upon other theoretical frameworks, including Behavioural Determinants Model, 41 Theory of Compliance 47 and Health Belief Model. 50
The comparison groups in the included studies varied, with the majority using a no-intervention/wait-list control group (n = 8)39,46–48,50,52–54 or a minimal intervention/active control group (n = 10),38,40–45,49,51,55 such as providing general health information or a single educational session.
Physical activity was measured as the primary outcome in seven studies,39,40,42,44,46,47,57 and as a secondary outcome in 10 studies.38,41,45,48,50–55 Objective measures included accelerometers,39,42,47,54 pedometers39,42,43 and physical capacity tests, 45 while self-report questionnaires were also used.38–44,46–53,55 Secondary outcomes reported in the studies included sedentary behaviour, diet, BMI and body composition. Additionally, some studies assessed fitness and psychosocial variables such as self-efficacy and motivation.
The included studies varied in their approach to follow-up assessments. More than half of the studies (13 studies, 72.2%) conducted assessments only immediately post-intervention, offering valuable data on the short-term impact of DBCIs. Three studies included follow-up periods ranging from 3 to 6 months post-intervention.40,44,49 Notably, two studies45,55 extended their follow-up to more than 6 months post-intervention, providing crucial information on the long-term maintenance of physical activity behaviours and other outcomes.
Risk of bias assessment
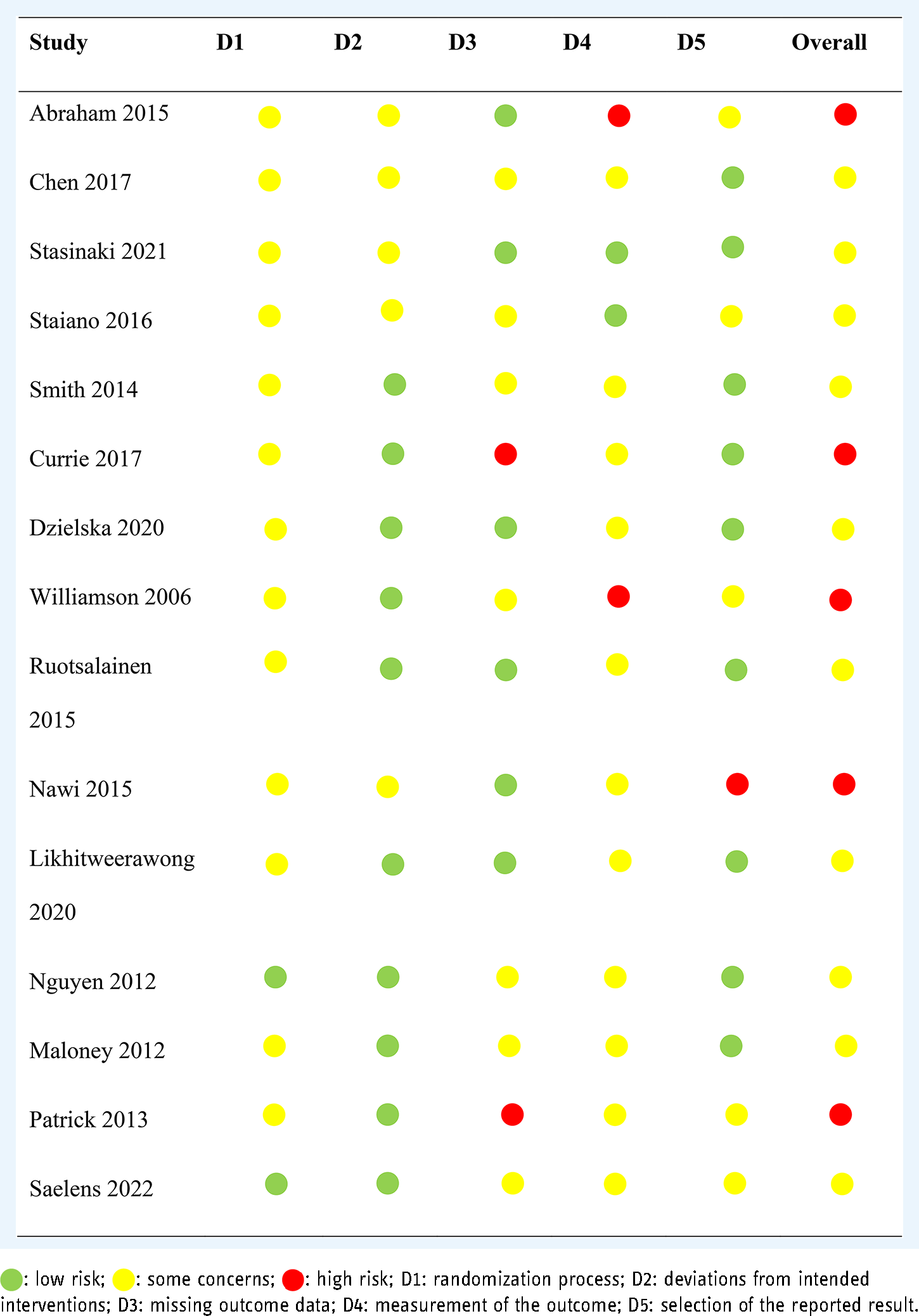
The risk of bias assessment for all included studies is shown in Table 2 (for RCTs) and Table 3 (for Non-Randomized Studies of Interventions). Among the 15 RCTs, no studies were judged to have a low risk of bias across all domains, 10 studies had some concerns, and five studies were considered to have a high risk of bias.38,41,43,51,53
Risk of bias of included RCTs.
Risk of bias of non-randomized studies of interventions.
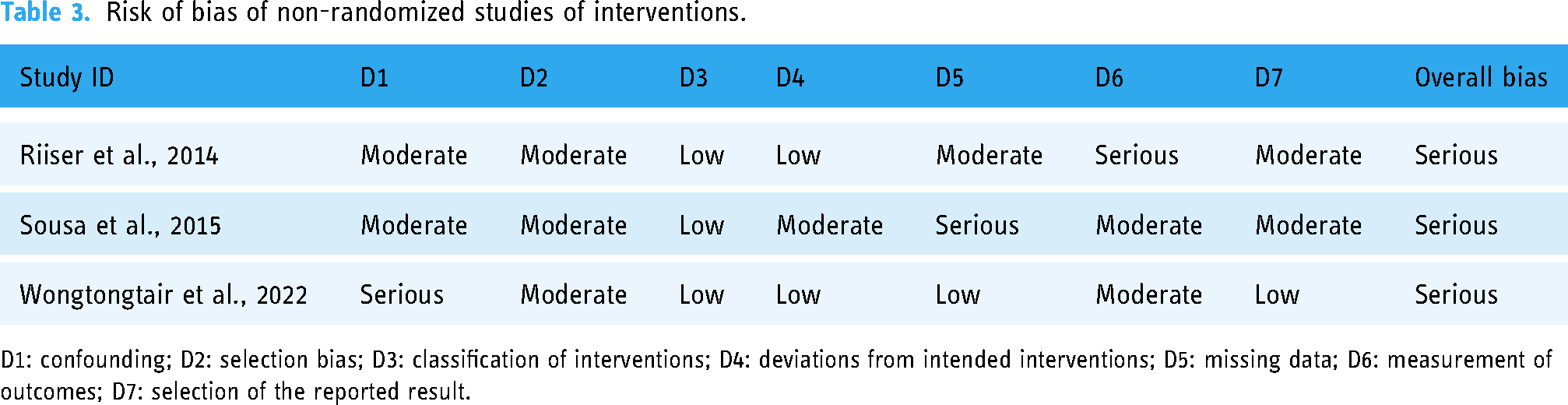
D1: confounding; D2: selection bias; D3: classification of interventions; D4: deviations from intended interventions; D5: missing data; D6: measurement of outcomes; D7: selection of the reported result.
The main reasons for the high risk of bias were primarily due to concerns about the measurement of the self-reported physical activity outcome, some concerns about attrition, lack of information on allocation concealment, and some missing outcome data. Only two studies reported allocation sequence concealment in addition to the use of computer-generated randomization system hence was judged to have low risk of bias in the randomization process.40,55 Outcome data were reasonably well-reported in all RCTs; however, only three studies reported blinding of the outcome assessors.39,52,55 With regards to the selection of the reported result, five studies were judged to have some risk of bias as no previous protocol publication with specified analysis plan could be identified. 38 ,39–41,53 Based on the risk of bias assessment using the ROBINS-I tool, all three non-randomized studies were judged to have an overall serious risk of bias (Table 3). The main areas of concern were confounding, selection of participants and measurement of outcomes. These limitations should be considered when evaluating the strength of evidence provided by these non-randomized intervention studies.
Effectiveness of DBCIs
Qualitative synthesis
Narrative synthesis of the included studies revealed several key themes and patterns in the effectiveness and implementation of DBCIs for promoting physical activity among adolescents with overweight and obesity. Of the 18 studies included in this review, eight studies reported significant improvements in physical activity outcomes in the DBCI group compared to the control group.38,39,42,44,45,48–50 Notably, mobile-based interventions, particularly those utilizing smartphone apps, were associated with better outcomes and greater effectiveness compared to other digital platforms,44,45,49,50 as well as higher engagement rates.44,49,54 The effectiveness of DBCIs appeared to be influenced by the duration of the intervention. Studies with longer intervention periods (≥12 weeks)39,42,44,50 generally reported larger and more sustained improvements in physical activity compared to studies with shorter intervention periods (≤8 weeks).43,52
The specific BCTs used in the interventions varied across studies. However, some common techniques that were associated with effective interventions included goal setting, action planning, self-monitoring, feedback and social support44,49 as studies that incorporated combinations of these BCTs, tended to show more positive outcomes. Many interventions incorporated social elements, either through direct social support or by facilitating peer interactions within the digital platforms.41,42,44,46–51
Meta-analysis results
Meta-analyses were conducted for three physical activity outcomes: MVPA, total physical activity (PA), and daily step counts. A total of 13 studies provided sufficient data for inclusion in these analyses.
The meta-analysis comparing DBCIs to control conditions on MVPA included three studies (n = 231 in control, n = 218 in DBCI) (Figure 2). The pooled effect size was 0.16 (95% CI: [−0.39, 0.71]), indicating a small positive effect favouring DBCIs, but this effect was not statistically significant. Moderate heterogeneity was found between the studies (I2 = 75%, p = 0.02).

Forest plot on the effect of DBCIs on MVPA.
Eight studies (n = 220 in DBCI, n = 213 in control) were included in the meta-analysis of DBCIs on total physical activity (Figure 3). The pooled effect size was 1.61 (95% CI: [0.56, 2.66]), indicating that DBCIs were effective in promoting total physical activity among adolescents with overweight and obesity compared to control conditions, which was statistically significant (Z = 2.99, p = 0.003). However, significant heterogeneity was observed among the studies (I2 = 95%, p < 0.00001).

Forest plot on the effect of DBCIs on total PA.
Two studies were included in the meta-analysis of daily step counts (n = 48 in DBCI, n = 40 in control). The pooled effect size was −0.10 (95% CI: [0.52, 0.32], p = 0.65), indicating a small, non-significant difference slightly favouring the control group (Figure 4). No significant heterogeneity was found between the studies (I² = 0%, p = 0.51).

Forest plot on the effect of DBCIs on daily step counts.
Subgroup and sensitivity analyses
Due to the limited number of studies included in each meta-analysis and the diverse range of DBCIs, subgroup analyses were not performed. The interventions varied considerably in terms of their design, content, delivery mode and technological platforms, making it challenging to categorize them into distinct and meaningful subgroups.
A sensitivity analysis was conducted by excluding studies with a high risk of bias. After this exclusion, the pooled effect size for total physical activity remained significant and positive (SMD = 1.48, 95% CI: [0.16, 2.80], p = 0.028, I2 = 97%), indicating a large effect of DBCIs on total physical activity compared to control conditions, though slightly smaller than the main analysis. Another separate sensitivity analysis including only randomized controlled trials (RCTs) (n = 6) was performed, excluding quasi-experimental studies. The effect size remained similar (SMD = 1.21, 95% CI: [0.12, 2.32], p = 0.03, I2 = 94%), indicating that the inclusion of quasi-experimental studies did not substantially impact our overall conclusions.
Secondary outcomes
In addition to physical activity, the included studies reported several secondary outcomes, including changes in BMI, body weight, sedentary behaviour and health-related quality of life (HRQoL). BMI and body weight outcomes were reported in 16 studies. Of these, eight studies found significant reductions in BMI and/or body weight in the intervention group,38,40,44,45,48,50,52,55 while eight studies reported no significant differences between groups.41,43,46,47,49,51,53,54 Sedentary behaviour outcomes were reported in eight studies. Four studies found significant reductions in sedentary time or screen time in the intervention group,39,41,47,54 while four studies reported no significant differences between groups.40,46,52,55 HRQoL outcomes were reported in three studies, using various validated questionnaires such as the Pediatric Quality of Life Inventory (PedsQL), 41 KIDSCREEN 48 and Impact of Weight on Quality of Life. 46 Two studies found significant improvements in HRQoL scores in the intervention group compared to the control group,41,46 while one study reported no significant differences between groups. 41
BCTs used in interventions
A total of 35 distinct BCTs were identified across the 18 included studies (Table 4). The number of BCTs used in each intervention ranged from four to 14, with a median of eight BCTs per intervention The most commonly used BCTs were information about health consequences (n = 13/18, 72.2%), goal setting (behaviour) (n = 12/18, 66.7%), self-monitoring of behaviour (n = 10/18, 55.6%), instruction on how to perform the behaviour (n = 10/18, 55.6%) and feedback on behaviour (n = 8/18, 44.4%). Six studies used a combination of 12 or more BCTs,38,40,41,47,51,54 while two studies used fewer than five BCTs.39,52 Less frequently used but notable BCTs included social support (unspecified) (38.9%), problem solving (33.3%,) and action planning (22.2%). Among the seven studies that reported significant improvements in physical activity outcomes, the most frequently used BCTs were information about health consequences (71.4% of effective studies), goal setting (behaviour) (57.1%), self-monitoring of behaviour (57.1%), feedback on behaviour (57.1%) and social support (unspecified) (57.1%).
Frequency of behaviour change techniques (BCTs) used in the included studies.

Discussion
This systematic review and meta-analysis provide a comprehensive evaluation of DBCIs aimed at promoting physical activity among adolescents with overweight and obesity. Our findings offer valuable insights into the effectiveness of these interventions and highlight key factors that influence their success.
DBCIs demonstrated a large, significant positive effect on total physical activity levels, which suggests that these interventions can be effective tools for increasing physical activity in adolescents with overweight and obesity. The large positive effect observed for total physical activity is notably higher than effects reported in previous meta-analyses of physical activity interventions for general adolescent populations.22,58 Our larger effect size suggests that DBCIs may be particularly effective for adolescents with overweight and obesity. However, the high heterogeneity in our analysis indicates substantial variability in intervention effects, which is consistent with findings from previous review of digital health interventions. 59 In contrast to total physical activity, our analysis showed a non-significant effect of DBCIs on MVPA. This result is somewhat surprising given that many physical activity guidelines focus on increasing MVPA. 9 It also differs from the findings of a previous review, which reported positive effects of active video games on MVPA in children and adolescents. 60 The discrepancy may be due to the specific challenges faced by adolescents with overweight and obesity in engaging in higher-intensity activities or limitations in how DBCIs target MVPA. Given the small number of studies, the small sample sizes and the non-significant overall effect, the findings on the effectiveness of DBCIs in increasing step count among adolescents with overweight and obesity are inconclusive based on the current evidence. Further research with larger sample sizes, more studies and possibly longer intervention durations may be needed to draw more definitive conclusions about the impact of DBCIs on step count in this population.
Our review identified substantial heterogeneity in intervention content and focus. Among the included studies, four interventions focused solely on physical activity promotion, while 14 adopted a multi-behavioural approach combining physical activity with dietary modifications. While this distribution of intervention types is noteworthy, formal subgroup analyses were not conducted due to the limited number of studies with compatible outcome data in our meta-analyses, which would have resulted in subgroups too small for meaningful statistical comparison. Future research with larger numbers of studies using comparable outcome measures is needed to enable such comparative analyses. Furthermore, the heterogeneity and variability in results across different physical activity outcomes underscore the complexity of digital interventions and behaviour change in this population; as well as the importance of considering factors such as intervention design, duration, and participant characteristics to optimize the effectiveness of these digital interventions.
The most frequently employed BCTs in effective interventions were information about health consequences, goal setting (behaviour), self-monitoring of behaviour, feedback on behaviour, and social support. This combination of techniques aligns with established behaviour change theories and previous research on effective intervention components.61,62 Information about health consequences serves as a foundational element, potentially enhancing motivation by increasing awareness of the benefits of physical activity. This aligns with the Health Belief Model, which suggests that perceived benefits are crucial for behaviour change. 63 The importance of this BCT is further supported by a recent systematic review, which identified ‘information about health consequences’ as a common component in promising interventions targeting physical activity and healthy eating behaviours in adolescents. 64 This analysis also aligns with findings from previous reviews which identified the use of goal-setting, self-monitoring and feedback as BCTs in technology-based interventions for promoting physical activity behaviour change in children and adolescents.22,23,65 The digital nature of the interventions may enhance the implementation of these techniques by providing real-time tracking and feedback capabilities. 66 Alongside these BCTs, a noteworthy finding of our review is the identification of social support as one of the frequently used BCTs associated with significant improvements in physical activity outcomes among adolescents with overweight and obesity, suggesting that these strategies may be key components of effective DBCIs for promoting physical activity in this population. The inclusion of social support as a key BCT in digital interventions targeting physical activity in adolescents with overweight and obesity is particularly relevant, given that this population often faces unique social challenges such as body image concerns, peer victimization, and social isolation,14,67 which can be mitigated through supportive social interactions within the digital intervention framework, potentially enhancing engagement and adherence to physical activity goals.
The review has several strengths that contribute to its value in the field of digital health interventions for adolescents with overweight and obesity. Our review employed a comprehensive search strategy across multiple databases, ensuring a thorough capture of relevant studies in this rapidly evolving field. By focusing on adolescents with overweight and obesity, our review provides targeted insights into the effectiveness of digital interventions for a high-risk group that may benefit significantly from increased physical activity. Furthermore, our analysis examined effects on total physical activity, MVPA, and step count, offering a nuanced understanding of how DBCIs impact different aspects of physical activity.
However, this review also has some limitations that should be acknowledged. A key limitation of focusing primarily on MVPA outcomes is that it may not capture the gradual progression in physical activity that is often more appropriate and achievable for adolescents with overweight and obesity. A more comprehensive approach considering reductions in sedentary behaviour and increases in light physical activity might better reflect meaningful behaviour change in this population. The substantial heterogeneity observed in our analyses, particularly for total physical activity and MVPA, limits the generalizability of our findings and highlights the variability in intervention effects. Besides, the number of included studies for the meta-analyses of MVPA and step count were small, which limits the robustness of conclusions for these specific outcomes. Furthermore, some of the included studies relied on self-reported physical activity measures, which may be subject to recall bias and overestimation, potentially affecting the accuracy of the reported effects. Notably, most included studies were conducted in high-income countries, potentially limiting the generalizability of findings to low- and middle-income settings.
Despite these limitations, the findings of this systematic review and meta-analysis support the use of DBCIs as a promising approach for promoting physical activity among adolescents with overweight and obesity. Healthcare providers and youth health programmes should consider incorporating well-designed DBCIs as part of their strategies to address physical inactivity among adolescents with overweight and obesity. Given the stronger effects observed for total physical activity compared to MVPA and step count, practitioners should design interventions that encourage a broad range of physical activities rather than focusing solely on high-intensity exercises or step goals. Future digital interventions should consider implementing graduated approaches that first target reducing sedentary behaviours and increasing light physical activity before progressing to MVPA. This ‘staircase approach’ may be more realistic and sustainable for adolescents with overweight and obesity who are initially inactive. Future studies should consider including multiple physical activity intensity measures, including sedentary behaviours and light physical activity, to better capture the progressive nature of physical activity adoption in this population.
The high heterogeneity in our results underscores the importance of tailoring interventions to individual needs and preferences. Practitioners should strive to offer personalized DBCIs that consider factors such as age, gender, initial fitness level and personal interests to maximize effectiveness. This approach may be more achievable and sustainable for adolescents with overweight and obesity. While DBCIs show promise, they should be considered as part of a comprehensive approach to adolescent health. Practitioners should explore ways to integrate digital interventions with other health promotion strategies, including in-person counselling, school-based programmes and family involvement. Ideally, practitioners should strive for a balanced approach that combines the benefits of digital interventions with face-to-face support and environmental strategies.
While digital interventions offer promising opportunities for promoting physical activity, it is essential to consider how social determinants of health and racial/ethnic factors may influence their implementation and effectiveness. Most included studies did not adequately report participants’ racial/ethnic background or socioeconomic status, limiting our understanding of how these factors influence intervention effectiveness. This gap is significant as access to digital technologies, internet connectivity and digital literacy can vary substantially across different socioeconomic and racial/ethnic groups.68–70 Cultural factors may also influence how different populations engage with digital interventions.71–73 Further research is needed to understand how to adapt digital interventions to be culturally appropriate and accessible across different populations, particularly in communities that may face greater barriers to digital technology access and use.
Long-term follow-up assessments should be prioritized to evaluate the sustained effects of DBCIs on physical activity behaviours, and to better understand factors influencing user engagement and adherence to DBCIs. This is particularly important given the chronic nature of obesity and the need for long-term behaviour change to achieve and maintain a healthy weight. Given the high heterogeneity observed in our analyses, future research should focus on identifying and understanding the factors that moderate intervention effectiveness. This could include investigating the impact of participant characteristics (e.g. age, gender, initial BMI, baseline activity levels), intervention features (e.g. specific BCTs, technological platforms) and contextual factors (e.g. socioeconomic status, cultural background). Efforts should be made to standardize physical activity outcome measures across studies to facilitate more robust comparisons and meta-analyses in future reviews. As digital technologies continue to evolve, future research could examine the potential of emerging technologies such as virtual reality, augmented reality and artificial intelligence in enhancing the effectiveness and engagement of physical activity interventions for adolescents.
Conclusion
This systematic review and meta-analysis provide evidence that DBCIs can be effective in promoting physical activity among adolescents with overweight and obesity, particularly in terms of increasing total physical activity. The use of multiple BCTs, particularly those focused on self-regulation such as goal setting, self-monitoring and feedback, as well as social support appears to enhance intervention effectiveness. While DBCIs show potential, continued research and refinement are necessary to maximize their effectiveness and address the complex challenges of behaviour change in this vulnerable population, including maintaining long-term engagement, effectively promoting higher-intensity physical activities and ensuring interventions are accessible and effective across diverse populations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251314904 - Supplemental material for Effectiveness of digital behaviour change interventions for promoting physical activity in adolescents with overweight and obesity: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251314904 for Effectiveness of digital behaviour change interventions for promoting physical activity in adolescents with overweight and obesity: A systematic review and meta-analysis by Puteri Shanaz Jahn Kassim, Noor Azimah Muhammad, Nur Faraheen Abdul Rahman, Sherina Mohd Sidik, Cecilia A. Essau and Shamsul Azhar Shah in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251314904 - Supplemental material for Effectiveness of digital behaviour change interventions for promoting physical activity in adolescents with overweight and obesity: A systematic review and meta-analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251314904 for Effectiveness of digital behaviour change interventions for promoting physical activity in adolescents with overweight and obesity: A systematic review and meta-analysis by Puteri Shanaz Jahn Kassim, Noor Azimah Muhammad, Nur Faraheen Abdul Rahman, Sherina Mohd Sidik, Cecilia A. Essau and Shamsul Azhar Shah in DIGITAL HEALTH
Footnotes
Contributorship
PSJK and NFAR performed the literature search and data extraction. PSJK, NFAR, and NAM assessed the risk of bias. PSJK and NFAR conducted the data analysis with guidance from NAM. PSJK drafted the manuscript with significant contributions from NFAR, NAM, and SAS. NAM, CAE, SAS and SMS assisted with data interpretation and manuscript revision. NAM provided overall supervision. All authors contributed to the interpretation of results, critically revised the manuscript for important intellectual content, and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable. No human subject’s involvement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This systematic review was conducted as part of a doctoral research and was supported by Fundamental Grant of the Faculty of Medicine UKM (FF-2021-414).
Consent for publication
All the authors approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.