
Abstract
Background
Memory complaints are the early symptoms of cognitive impairment, and they usually bring anxiety about cognitive deterioration among the elderly population. Musical interventions were demonstrated to relieve dementia symptoms. This pilot study investigated the potential benefits of rhythmic musical intervention, African drumming, on cognitive function and mood status with traditional and digital assessments for elderly participants.
Method
Participants were recruited through social media. The musical intervention was arranged by drumming instructors certified by the Hong Kong Association of African Drumming. Participants joined regular training classes with eight lessons, which covered rhythmic clapping and drumming, power control, and overall performance with songs. The inclusion criteria included the following: (1) age over 50; (2) self-reported complaints of memory loss; (3) the ability to use digital devices, such as a smartphone; and (4) can understand the content of questionnaires and follow the intervention schedules. Those with hearing impairment, failure to use Chinese, and active psychosis or dementia were excluded. Cognitive function was measured by the Hong Kong version of the Montreal Cognitive Assessment (HK-MoCA) and a digital platform, ScreenMat. Anxiety and depression levels were assessed by the State–Trait Anxiety Inventory (STAI) and Geriatric Depression Scale (GDS-15). All assessments were performed before and after the drumming classes. The outcomes were compared using the Wilcoxon signed rank test with 0.05 as the significance level.
Result
Twenty-two participants joined this study with an attendance rate of 90%. The overall cognitive function of the participants was good with an average score of 27 for HK-MoCA. After eight sessions of African drum intervention, the cognitive function did not show a significant improvement, but the response time of answering the digital cognitive questions was significantly faster than before the intervention (−39.9 s, p = 0.03). The response time for the short-term memory function was most significantly reduced (−13.5 s, p = 0.017). The anxiety and depression scores (i.e. STAI and GDS) also significantly improved (p < 0.001) after the intervention.
Conclusion
Rhythmic musical intervention is not only effective in improving emotional status, but also potentially good for improving cognitive symptoms, including the response time of the memory test. Digital behavioral analysis may bring new insights for future research on cognitive assessment.
Keywords
Introduction
Age-related cognitive impairment is a common condition among the elderly. 1 The worldwide prevalence of cognitive impairment currently ranges from 7% to 34% for those between 50 and 59 years old, 5% to 38% for those between 60 and 69 years old, and from 12% to 41% for those ≥70 years old. 2 Cognitive impairment is typically characterized by progressive memory loss, learning difficulties, and inability to concentrate on tasks.3,4 These symptoms may eventually significantly debilitate the elderly's activities of daily living and substantially impact the patient's and their caretaker's quality of life. 5 Cognitive impairment is also associated with worse mental well-being, such as depression, anxiety, and stress. 6 Furthermore, as cognitive impairment may progress to dementia, it may impose a heavy financial burden on healthcare systems all over the world. 7 Given global demographic aging, elderly patients with cognitive impairment will only become an increasingly important population. Therefore, taking a multidirectional approach and innovating in prevention and screening are crucial.
However, there is no definitive pharmacological treatment for cognitive impairment. 8 Psychosocial interventions, including musical intervention, are widely adopted and accepted as a method of management for elderly with cognitive impairment.9,10 Musical intervention, including receptive and interactive music therapy, is an emerging, but effective psychosocial and non-pharmacological intervention for cognitive impairment.10–12 Generally, group rhythmic music interventions have been shown to improve symptoms of depression and anxiety.13,14 Musical interventions have further been shown to improve verbal fluency, enhance memory, and promote language ability for patients with Alzheimer's disease. 15 As associations have been shown between mood symptoms and cognitive impairment in older people, rhythmic musical intervention may be important to manage cognitive impairment and its comorbidities.16–18
Cognitive function is usually evaluated by healthcare professionals through face-to-face interviews with traditional questionnaires, such as the Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE).19,20 These assessments may struggle to capture the early signs of cognitive deterioration or even Alzheimer's disease due to the operator's biases and inability to measure precise movements.21,22 Therefore, digital screening platforms were recently proposed as an alternative method to evaluate cognitive impairment.23–25 These platforms are able to digitalize and analyze precise response times and patterns as an additional evaluation parameter apart from the scoring of the test.26,27 Digitalization of cognitive tests may also further increase the accessibility for self-administration at home. Compared to traditional assessments, digital assessments are not limited by assessor and resource availability for community screening and provide more opportunities for rural or remote communities. 28 Reliable digital cognitive tests that are more sensitive and accessible may become essential to future cognitive impairment screening programs.
A simple cognitive evaluation platform was developed for individuals who were suspected to have cognitive impairment. 29 This pilot study used this platform along with traditional screening tools, such as MoCA, to investigate the potential benefits of rhythmic musical intervention on cognitive functions and mood status among older adults.
Method
Study design
This is a prospective pilot study to evaluate the benefits of rhythmic musical intervention (i.e. activities with an African drum) on cognitive function. A digital system was used to measure the response time of the cognitive questions. Ethics approval was obtained from the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (reference number CREC 2022.087).
Participants
Participants were recruited through social media if they met the following inclusion criteria: (1) an adult aged over 50 years old; (2) self-reported complaints of memory loss symptoms; (3) a user of any digital devices, such as a smartphone; and (4) an adult can understand the content of questionnaires and follow the intervention schedules for drum classes. Individuals were excluded from the study if they: (a) had hearing impairment; (b) could not understand Chinese; or (c) had been diagnosed with active psychosis or dementia. The personal identity of all participants was removed, and written consent was signed before the intervention.
Intervention
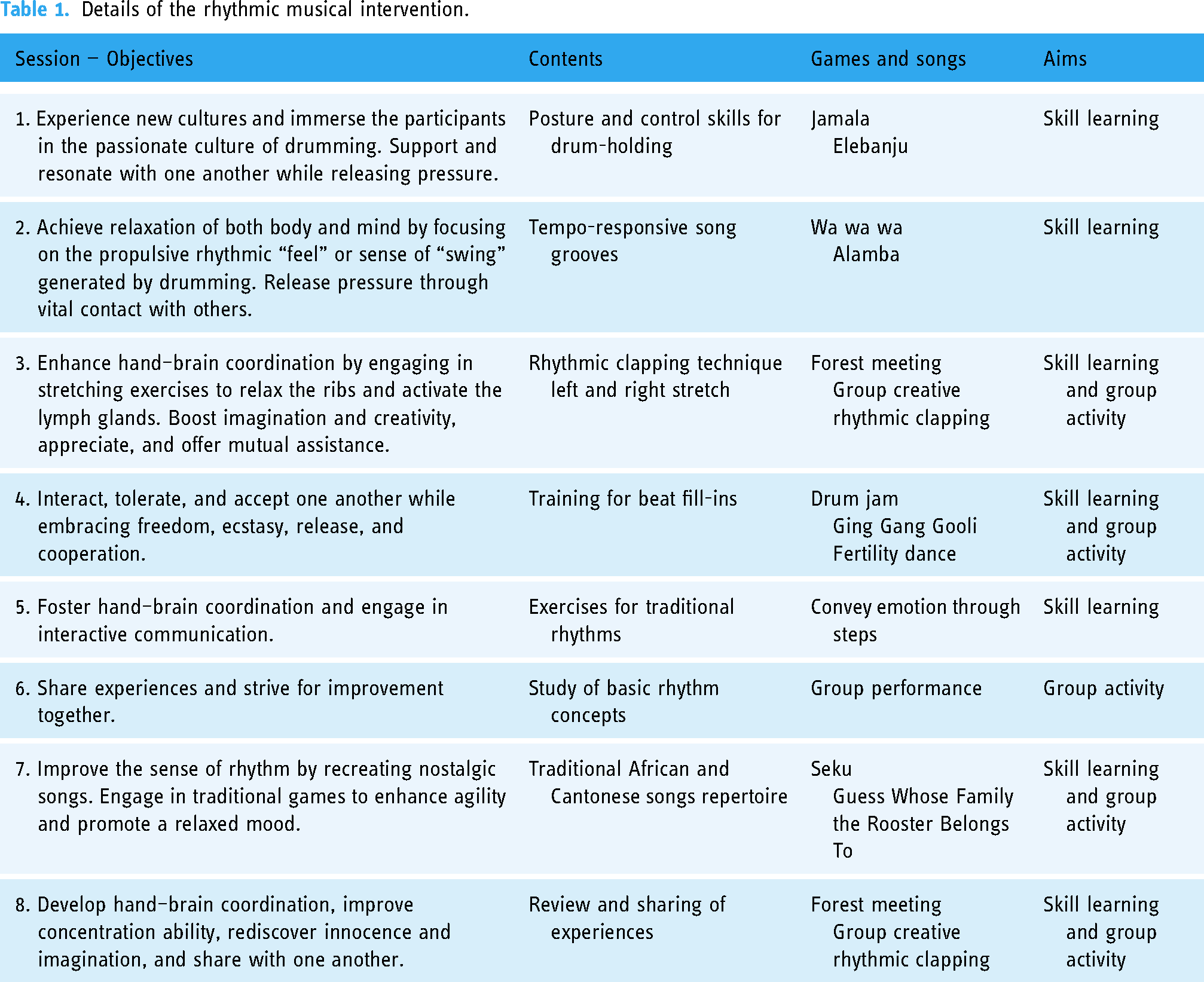
The musical intervention was arranged by drumming instructors who were certified by the Hong Kong Association of African Drumming. Participants joined regular training classes with eight lessons arranged in four weeks in July 2022 (Figure 1). The length of each class was 1.5 h. The classes were arranged in a community social center in downtown Kowloon. The structure of classes included (1) rhythmic musical training with the application of an African drum and/or (2) group engagement activities, where participants applied their drumming skills as a team (Table 1). In each lesson, participants were seated in a large circle to learn the drumming patterns in a call-and-response format. The learning objectives were introduced during the warm-up period. Participants were then engaged in sequenced drumming that trained their memory function and hand–eye coordination. A debriefing discussion was arranged by the end of each lesson that summarized and reviewed the learning outcomes.

Conceptual framework of the rhythmic musical intervention.
Details of the rhythmic musical intervention.
Outcomes
Baseline characteristics of participants, namely, age, sex, weight, height, waist circumference, smoking and drinking habits, and level of physical activity, were collected before the start of the program. Cognitive function was measured by the Hong Kong version of the Montreal Cognitive Assessment (HK-MoCA) and a digital platform, called ScreenMat (Table 2, Supplemental Figure 1), which measures both cognitive scores and response time. The questions were designed with reference to the traditional questionnaires of MoCA and MMSE on five domains, namely, orientation, calculation, visual coordination, and short-term and long-term memory. Each question contributed four marks, and the total score of ScreenMat was 20 marks. The ScreenMat questions were randomized from a question bank for each assessment, preventing repeated questions before and after the intervention. The HK-MoCA was translated into Chinese and subsequently validated in 2014. 30 This is a 30-question questionnaire that requires around 10 to 12 min to complete. The HK-MoCA assesses short-term memory, visuospatial abilities, executive functions, attention, concentration, working memory, language, and orientation to time and place. Scores on the MoCA range from 0 to 30. A score of 26 and higher is considered normal. Anxiety and depression levels were assessed by the State–Trait Anxiety Inventory (STAI) and the Geriatric Depression Scale (GDS-15) separately. The STAI was validated for the Chinese population, and it comprised 40 items that measure two types of anxiety, state and trait. 31 Each type of anxiety is measured with 20 items, each rated through a 4-point Likert scale. Scores were then summated to give a score range of 20 to 80. A higher score correlates with greater anxiety. The GDS-15 was validated among the Hong Kong population. 32 This tool is a self-report “Yes/No” survey with a maximum score of 15, with a higher score corresponding to the likely severity of the depression. All measurements were conducted before and after the intervention at the community social center by trained researchers.
Five cognitive items in digital platform (ScreenMat).
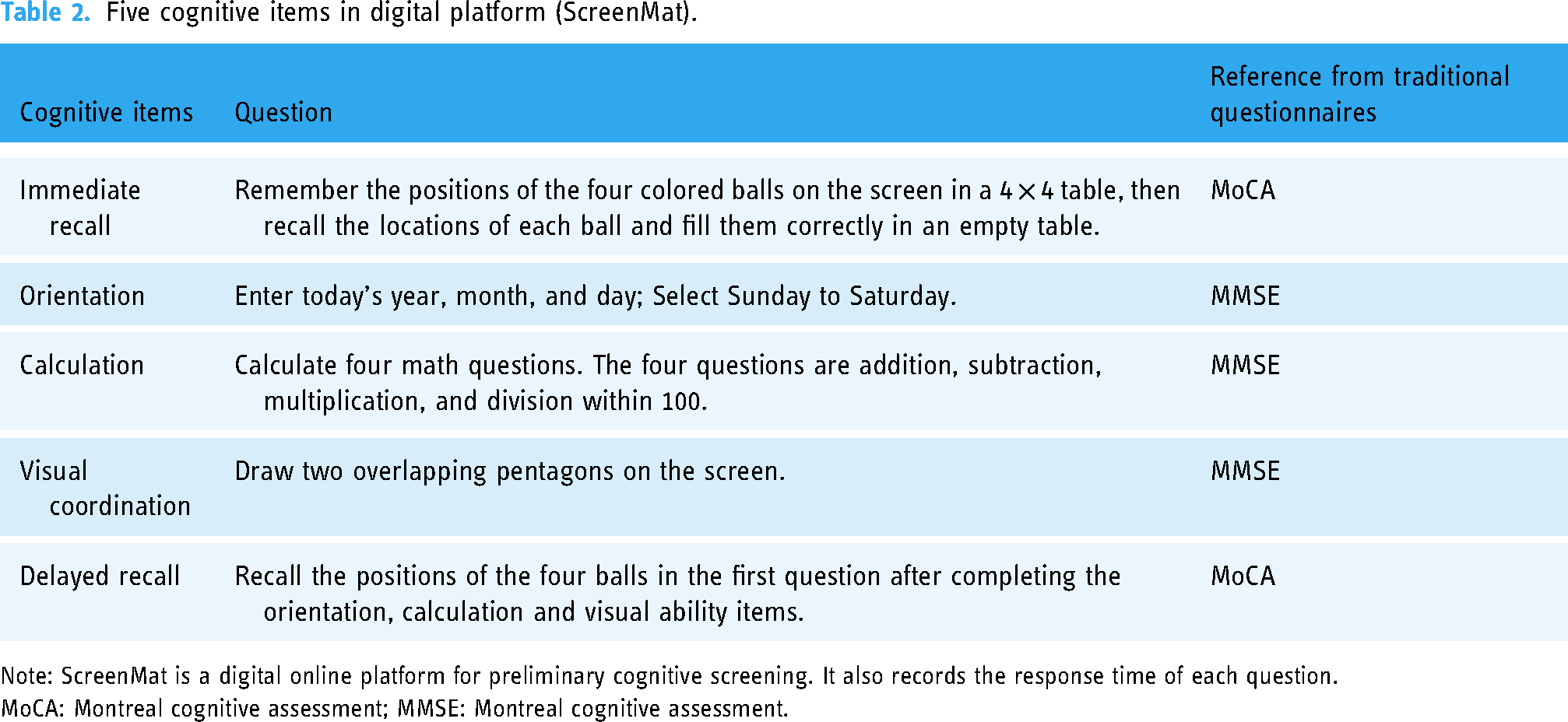
Note: ScreenMat is a digital online platform for preliminary cognitive screening. It also records the response time of each question.
MoCA: Montreal cognitive assessment; MMSE: Montreal cognitive assessment.
Statistical analysis
The variables were described as mean differences before and after the musical intervention, and a 95% confidence interval was constructed. The p-value was derived by the Wilcoxon signed rank test, with 0.05 as the significance level. A subgroup analysis was performed for those who attended all classes of the intervention. The data analysis was conducted through IBM SPSS Statistics version 26.
Results
A total of 22 participants were recruited, with an overall attendance rate of 90%. The median age of the participants was 62 years, ranging from 53 to 73 years. Four of them (18%) were male, and none of them were smokers. The median body mass index (BMI) was 23.1 (3.8) kg/m2. Thirteen of the participants (59%) engaged in regular exercise with at least 150 min of moderate-intensity exercise or 75 min of vigorous-intensity exercise per week. Nine participants (41%) were diagnosed with high blood pressure, of which six (67%) were currently receiving hypertension treatment.
The results of HK-MoCA and ScreenMat are shown below. The baseline scores, mean (SD), of MoCA and ScreenMat were 27.1 (2.1) and 19.2 (1.3), respectively. No statistically significant improvement in cognitive function was observed after a month of rhythmic musical intervention (Table 3). Some domains of MoCA demonstrated improvement, including visuospatial/executive function, abstraction, immediate recall, and delayed recall (p-value < 0.05). The response time of the cognitive questions was captured by ScreenMat. Participants reduced the time spent on the cognitive questions by 40 s (p-value = 0.031) (Table 4). Calculation and immediate recall questions contributed more to the shortened response time. A total of 12 participants attended all classes of the rhythmic musical intervention. The overall cognitive function score by MoCA in these participants was shown to be significant (p-value = 0.025) (Supplemental Table 1). The improvement was mainly attributed to the immediate and delayed recall. In ScreenMat, this subgroup demonstrated similar benefits in the shortened response time on immediate recall (Supplemental Table 2).
Comparison of cognitive function scores before and after the intervention.
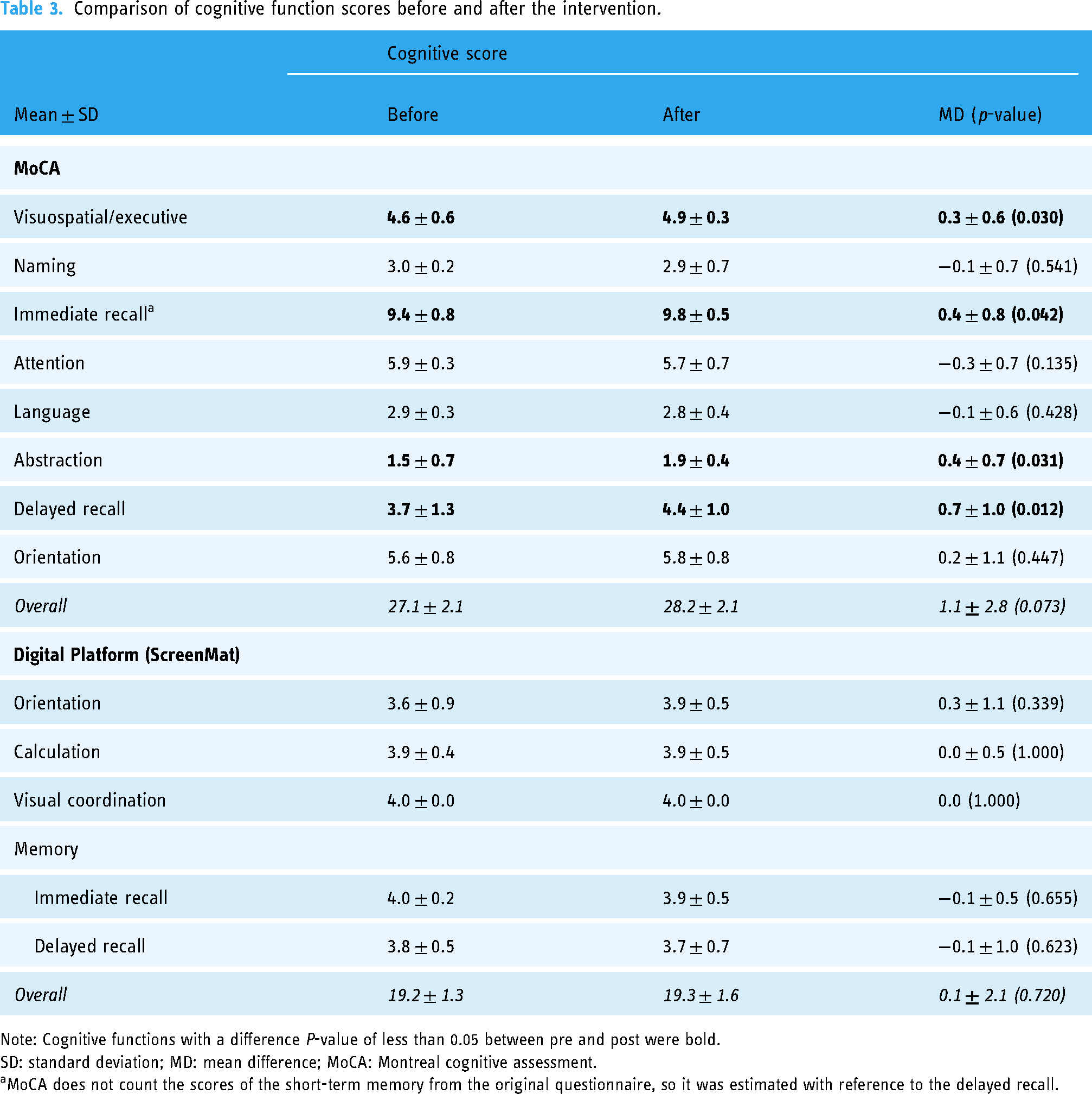
Note: Cognitive functions with a difference P-value of less than 0.05 between pre and post were bold.
SD: standard deviation; MD: mean difference; MoCA: Montreal cognitive assessment.
MoCA does not count the scores of the short-term memory from the original questionnaire, so it was estimated with reference to the delayed recall.
Comparison of cognitive function (response time by ScreenMat) before and after the intervention.

Note: Cognitive functions with a difference P-value of less than 0.05 between pre and post were bold.
SD: standard deviation; MD: mean difference; MoCA: Montreal cognitive assessment.
According to the anxiety and depression assessments, the baseline scores, mean (SD), were 37.4 (6.5) for STAI-S, 39.5 (7.0) for STAI-T, and 2.0 (2.1) for GDS-15. Significant improvements were demonstrated across the assessments after a month of rhythmic musical intervention (Table 5). In the subgroup of participants who had full attendance, the improvements in the anxiety and depression assessments were even stronger (Supplemental Table 3). The rhythmic musical intervention did not show any benefits in blood pressure management.
Comparison of anxiety, depression, and blood pressure levels before and after the intervention.

Note: Cognitive functions with a difference P-value of less than 0.05 between pre and post were bold.
Discussion
This pilot study investigated the cognitive and mood benefits after a month of rhythmic musical training (i.e. African drum intervention) in young elderly participants. A simple cognitive evaluation platform was used to capture the response time of answering the cognitive questions. Rhythmic musical intervention is not only effective in improving emotional status, but also potentially good for improving cognitive symptoms, such as memory function.
Musical interventions are generally demonstrated to better mood and potentially to improve cognitive function. 33 African drumming, as a rhythmic musical intervention, has been proposed as a rehabilitation program to alleviate negative emotions, including depression, 34 stress, 35 anxiety, 36 and agitation. 37 Studies also demonstrated that musical intervention may stimulate cognitive protection at the early stage of Alzheimer's disease.38,39 In fact, the cognitive benefits from rhythmic musical intervention may be due to the acoustic engagement of large-scale bilateral networks among temporal, frontal, parietal, and cerebellar brain areas, 32 but the current evidence is still uncertain.40,41 Digital cognitive tests already demonstrated good performances in the detection of cognitive decline,42,43 with the detection of mild cognitive impairment providing better opportunities for early intervention. 44 Response time on other cognitive domains, such as processing speed, working memory, and declarative memory, may enhance screening accuracy.45–47 Therefore, the digital behavioral analysis may bring new insights for future research.
Other than the traditional cognitive screening questionnaires, digital behavioral analysis is potentially applicable to further the real-time evaluation of cognitive function. The response time of answering the questions on the digital platform is a strength of this study, but there are still some limitations. First, digital versions of existing screening tools, such as Digital MoCA, 48 are not mature for digital behavioral analysis for this study; hence, we used our self-developed platform to further capture the response time on a digital device. Second, rhythmic musical intervention is an intensive training that can only be run in a small class format. Therefore, the sample size of this pilot study was constrained. A larger cohort study will further confirm the benefits of using digital behavioral data for cognitive assessment. Third, the long-term interventional effect may not be sustainable if the participants do not regularly play the musical drum after the classes. Digital home-based versions of rhythmic musical instruments should be developed for long-term cognitive function training. The test–retest practice effect cannot be eliminated. Further randomized clinical trials can strengthen the evidence for the benefit of music intervention on cognitive function.
Conclusion
The potential benefits to cognitive function and mental health are demonstrated after rhythmic musical training. Cognitive evaluation platforms can be further developed and applied to precisely capture the outcome indicators, such as response time, of relevant cognitive assessments. Future research on the use of digital devices for individual behavioral data will generate new insights for the development of personalized cognitive interventions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241271875 - Supplemental material for Rhythmic musical intervention improves response time of memory tests: A pilot study on the application of a digital cognitive assessment
Supplemental material, sj-docx-1-dhj-10.1177_20552076241271875 for Rhythmic musical intervention improves response time of memory tests: A pilot study on the application of a digital cognitive assessment by Ziyu Hao, Joshua YS Tran, Baker KK Bat, Karen KL Yiu, Joyce YC Chan and Kelvin KF Tsoi in DIGITAL HEALTH
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.