
Abstract
Objective
Virtual Reality (VR) and Augmented Reality (AR) are innovative technologies that can serve as effective tools for creating health interventions by altering psychological distance. Based on construal level theory and the reality-virtuality continuum, we designed, tested, and compared VR and AR campaigns to encourage proactive measures against COVID-19.
Methods
143 participants were randomly assigned to one of three messages: VR, AR, and a CDC video, and completed surveys before, immediately, and one week following message exposure.
Results
VR and AR increased preventive intentions and behaviors against COVID-19 both in the short and long run. VR was particularly effective as it also increased risk perceptions, more preventive intentions in the short term, and more preventive behaviors, including social distancing and mask wearing, in the long term. VR was more efficient than AR in enhancing risk perceptions and preventive intentions right after being exposed to the messages as well as promoting behaviors such as avoiding crowds, maintaining social distance from others, and wearing a mask in indoor public areas one week later. Moreover, among the three conditions, VR was the only intervention that generated actual behavior change after one week, which indicated potential long-term advantages of VR compared to other mediums. VR decreased social, spatial, and hypothetical distances to a greater degree than AR. VR was more effective than video. However, AR was not more persuasive than video.
Conclusions
Insights gained from the findings extend beyond the pandemic phase, offering practical applications for employing VR and AR technologies in health campaigns.
Keywords
The COVID-19 pandemic has revealed the challenges to convey health risks in behavioral interventions, mainly because of psychological distance. For instance, psychological distance exists between current actions and future outcomes, thus, it becomes challenging to emphasize the need to adopt healthy behaviors today to avoid negative health consequences in the future. 1 According to construal level theory, changing psychological distance can alter the construal level, ultimately affecting risk perceptions and behaviors. Therefore, adjusting the way messages are delivered can help shape perceptions and increase the likelihood of the audience adopting healthy behaviors. 2
Virtual Reality (VR) and Augmented Reality (AR) are innovative technologies that can be employed as effective tools for creating health interventions by altering psychological distance. 3 VR immerses users in artificially created digital environment and provides simulated sensory information that makes the environment seem real to the user. 4 AR augments the physical world by projecting and overlaying virtual information on to real-life environments. 5 VR and AR allow users to feel the risks and experience the negative consequences of undesirable behavior as if they were in the real world. 3 In the health domain, VR and AR have primarily been used for training clinicians and medical students.5,6 However, several VR- or AR-driven interventions have shown promising results for promoting health behavior change.7–10 For example, VR has been used to increase the intention to receive the flu shot 11 and engage in physical activity, 6 while also reducing interest in vaping 12 and soft-drink consumption. 1 AR has been used to increase exercise aimed at preventing muscle loss due to aging, 13 perceived threat of COVID-19, 14 and negative attitudes towards smoking, 5 while also controlling food intake. 7
Nevertheless, there is a lack of empirical studies that compare VR and AR despite their differences in functional mechanisms and interfaces. Additionally, there is a common misconception that AR and VR are interchangeable in terms of their ability to process 3D images and provide enriched or enhanced user experiences. Most people can only tell their differences via the devices: if they wear a VR headset, they are interacting with VR; if they use their mobile phone camera to overlay the digital world onto their physical environment, they are in AR. 8 Little is known regarding their similarities and differences in terms of their impact on user experiences. 9
To our knowledge, no prior work has explored the differences between VR and AR in changing psychological distance as well as compared their effects on health perceptions and behaviors. Given the ongoing and rapid research on VR- or AR-based interventions, there is a need to extend construal level theory by revealing how they differ in terms of their impact on construal level and psychological distance, which in the end, affect persuasion outcomes. To fill in the gap, the objective of this study is to create, examine, and compare VR and AR campaigns utilizing the construal level theory to determine if they can effectively encourage desirable COVID-19 vaccine intentions and preventive behaviors, both immediately and one week following message exposure. Additionally, the study seeks to investigate the underlying mechanisms that facilitate changes in intention and behavior.
Construal level theory
The initial purpose of the construal level theory was to explain how individuals mentally comprehend psychologically distant concepts. 10 When psychologically distant realities are constructed abstractly, it is referred to as high construal, whereas when psychologically close realities are perceived concretely, it is known as low construal. 2 Psychological distance comprises four dimensions, including temporal (the time gap between the current moment and the future consequence), hypothetical (the degree to which the subject differs from the reality that people experience directly), spatial (the physical distance between the individual and the subject), and social (the extent to which the event impacts oneself).15,16 These dimensions can shape the construal level of messages and, subsequently, influence risk perceptions and behaviors. As psychological distance is egocentric and centers around “me, here, and now”, 2 low construal or low psychological distance is vital in decision-making regarding specific situations 16 and is inclined to produce higher levels of perceived risk and a greater probability of desired behavior modification.1,17
Based on construal level theory, VR and AR can lead to a lower level of construal and psychological distance than less immersive media, such as print and video. This is because VR and AR provide a more immersive experience that generates a stronger feeling of presence.11,18 Presence occurs when users become fully engaged in the virtual world, which reduces temporal, hypothetical, spatial, and social distances.19,20 For example, VR and AR can help people better understand the long-term consequences of unhealthy behavior by allowing them to “experience” those consequences as if they were happening now, thus reducing temporal distance. 1 Additionally, VR and AR can make potential risks more visible5,12 and increase empathy by allowing people to feel as if they are in someone else's body, thus decreasing hypothetical distance. 21 VR and AR can make physically distant subjects appear closer, thus reducing spatial distance.16,18 Finally, since VR and AR focus on personal interaction with the environment 18 and reveal the direct impact of the environment on the self, 12 they can also reduce social distance. Thus, it can be predicted that in the context of COVID-19, VR will increase risk perceptions and preventive behaviors (H1). AR will also increase risk perceptions and preventive behaviors (H2).
VR has been shown to yield better results in promoting desirable changes in health outcomes than less immersive media. 22 For instance, Nowak et al. discovered that VR leads to a heightened sense of presence and awareness of the risk of spreading influenza, resulting in an increased intention to get vaccinated compared to e-pamphlets. This heightened awareness also positively impacts beliefs about the efficacy of the flu vaccine in protecting others. 11 Similarly, Xu et al. discovered that VR generates more perceived harm of secondhand e-cigarette aerosol and less interest in vaping than print advertisements. Moreover, the effectiveness of VR in reducing vaping interest as compared to print media was enhanced after a week. 12 Thus, we predict that VR will be more effective in promoting desired perceptions and behaviors than video (H3).
However, whether AR outperforms traditional media in influencing health outcomes shows variations across research scenarios. Jung et al. found that AR results in higher levels of negative emotions towards smoking cigarettes and a greater inclination to participate in a cigarette cessation program compared to 2D images. 5 Similarly, Seals et al. discovered that AR generates higher levels of perceived threat severity and susceptibility of COVID-19 compared to 2D animations. 14 However, Lee et al. did not find a significant difference between AR and 2D images in influencing smoking intentions. 23 Thus, this study aims to explore whether AR is more effective in promoting desired perceptions and behaviors than video (RQ1).
Reality-virtuality continuum
Prior research often focuses on VR and AR's similarities in improving visualization of objects and increasing interactivity with the environment. A few have examined how VR and AR differ in their effects on consumers’ attitudes and perceptions but empirical findings remain inconsistent across different research contexts. 9 For instance, VR is more likely to improve positive attitudes towards a virtual restaurant as it provides virtual tours which enable users to engage with a “real” shopping environment in a simulated and interactive manner. 24 Another study shows that AR generates more purchase intention as it visualizes products more effectively 9 whereas VR is related to more positive attitudes toward the brand as it is better able to visualize a retail landscape. 9 A study on virtual shopping experiences revealed a positive relationship between a sense of presence and intentions to shop for the VR condition, but not the AR condition. 8 Beyond the consumer research realm, a study on science knowledge retention found that participants in the AR condition paid less attention and had less enjoyment than those who used VR on a mobile phone platform. 25 However, none of these studies have examined health behaviors.
The reality-virtuality continuum offers a way to explain the differences in user experiences with AR and VR from a technical perspective. 26 It is a framework that categorizes the space between physical and virtual environments into four types: actual reality, AR, augmented virtuality, and VR. It explains how these classifications represent different points on the continuum between the physical and virtual worlds. On the left side of the RV continuum, the actual environment is described as the physical real-world scene that is observed. On the right side, the virtual environment is defined as a computer-generated simulation in which all the information the user perceives is also computer-generated, often referred to as VR. 8
According to the Reality-Virtuality continuum, AR is closer to actual reality. Users’ perceptions are still connected to the actual world. 27 Thus, AR produces a lesser degree of visual and spatial immersion in comparison to VR, 28 which implies that AR may not reduce spatial distance as much as VR through the lens of construal level theory. Also, VR outperforms AR in surpassing the linearity of time, 29 suggesting that AR may not have as significant an impact on reducing temporal distance as VR does. Moreover, VR and AR differ in how users interact with virtual elements. In VR, users are limited to interactions within the virtual environment while in AR, users can interact with both the virtual and real world. 28 Thus, VR received notably higher ratings than AR in terms of diminishing physical risks and portraying non-existent entities. VR is better than AR at generating experiences that deviate from the physical laws governing our reality, 29 which implies that VR may reduce hypothetical distance more than AR from construal level theory's perspective. Given limited prior work, we aim to compare the effectiveness of VR and AR in reducing psychological distances (RQ2) and influencing risk perceptions and behavior change (RQ3).
Methods
Subject inclusion criteria
This study was approved by Northern Arizona University (NAU) (approval number: 1820361-4) and the University of Nevada, Las Vegas (approval number: UNLV-2022-388). A total of 158 participants were recruited from these two large public universities in the southwestern United States, and each participant provided informed consent before data collection. The participants were recruited if they were 18 years or older and could choose to receive course extra credit for completing the study. Recruitment took place between October 2022 and January 2023.
Design, and procedure
A randomized control study with a repeated measure design was utilized to compare the effects of three messages – VR, AR, and a video by the Centers for Disease Control and Prevention (CDC) – over time. Before seeing the experimental message, participants filled out a survey measuring their baseline risk perceptions and behavioral outcomes, such as preventive behaviors, self-testing, etc. (Time 1/T1). Then, participants were randomly assigned to one of three messages: VR (N = 50), AR (N = 45), and video (N = 48). Immediately after message exposure, participants answered questions regarding risk perceptions, behavioral intentions, perceived distances, and demographics (Time 2/T2). All participants also answered a manipulation check question about whether the message visualized the virus. Fifteen participants who failed to answer the question correctly were removed from the final analysis. One week following the experiment, all participants responded to a follow-up online survey measuring their risk perceptions and behavioral outcomes (Time 3/T3).
Stimuli
Participants assigned to the VR condition wore an Oculus VR headset and watched a three-dimensional VR video. It featured a college-age male inviting the participant to a party. While he was talking, coughing, and sneezing, he spread visualized and exaggerated virus to the participant (Figure 1). Participants assigned to the AR condition used their own cellphones to access an AR app. Participants pointed their cellphone camera to the research assistant and saw visualized and exaggerated virus spread from the research assistant's mouth to them while he/she was talking, coughing, and sneezing (Figure 2). Participants assigned to the video condition watched a CDC video via YouTube. The video served as a control condition. It lists behaviors that people can adapt to reduce the risk of COVID-19.

VR intervention.

AR intervention.
Measures and analysis
We measured COVID-19
Measures.
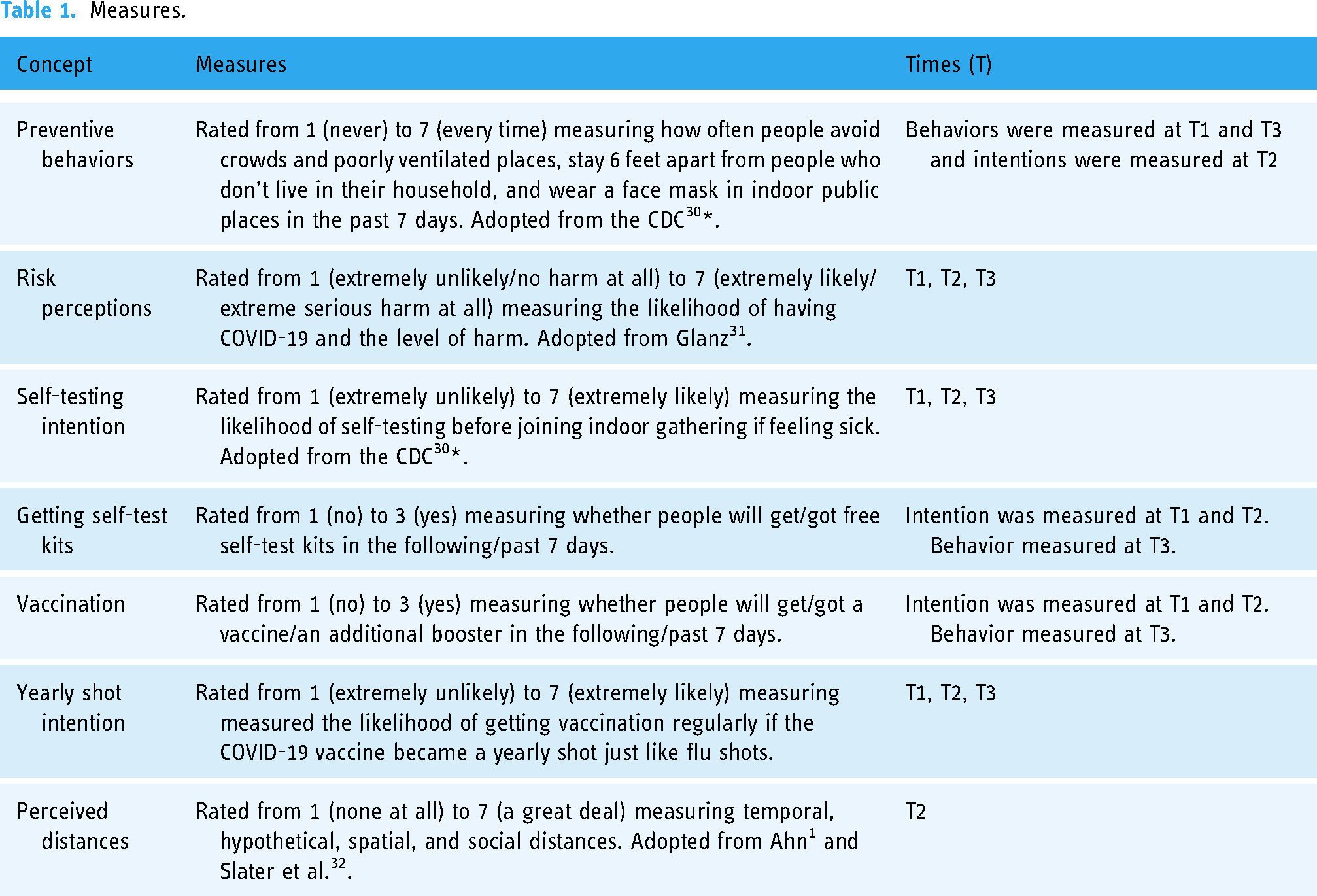
R (version 4.1.2) was used for all the analyses conducted. ANOVA and Fisher exact test were used to compare demographic variables among the three conditions. Age (p = 0.63), sex (p = 0.84), race, and ethnicity (p = 0.54) were not significantly different across all conditions. The following section outlines the analyses carried out to address the research question and hypotheses. Regarding prior exposure to VR technology, apart from one participant who dedicated less than an hour to VR in a typical week, the rest averaged zero hours. Consequently, we did not control for participants’ prior VR experience.
Results
Of the 143 total participants included in the final analysis, 74.13% (N = 106) were female, 65.73% (N = 94) were White, and 43.36% (N = 62) were Hispanic. Mean age was 20.9.
Within each message condition
H1 and H2 asked if VR and AR could promote desired perceptions and behaviors. Wilcoxon signed-rank test with continuity correction was used to compare perceptions and behaviors between T1 and T2 as well as T1 and T3. Results revealed that immediately after the experimental treatment, all three conditions increased intentions to stay 6 feet apart from people and wear a face mask in indoor public places. Besides, VR also increased perceived likelihood of having COVID-19, perceived harm of COVID-19, as well as intentions to get self-test kits, a vaccine/an additional booster, and yearly vaccine if the COVID-19 vaccine became a yearly shot. AR increased intention to avoid crowds (Table 2).
Perceptions and behaviors between T1 and T2 as well as T1 and T3 within each message condition.
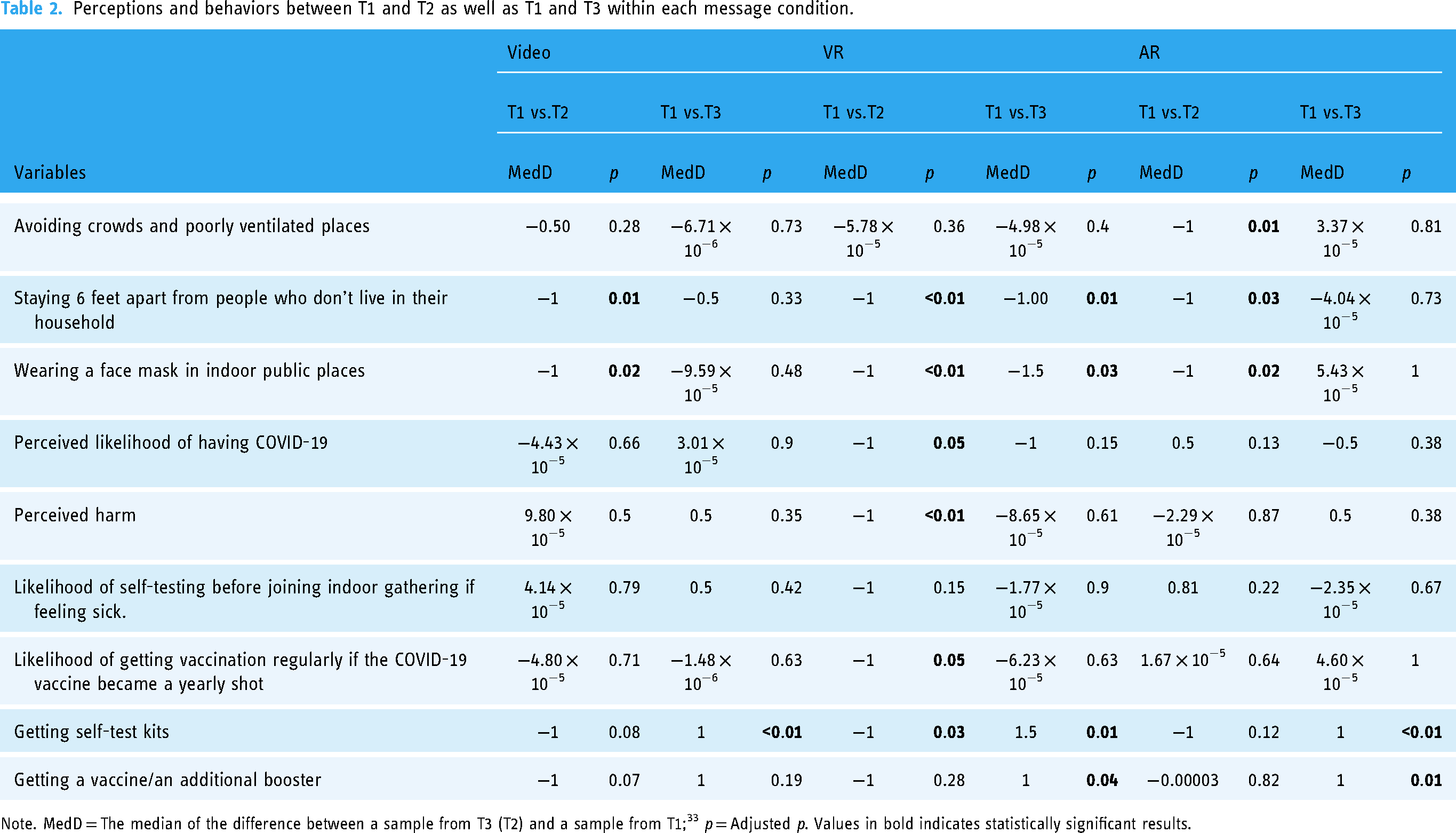
Note. MedD = The median of the difference between a sample from T3 (T2) and a sample from T1; 33 p = Adjusted p. Values in bold indicates statistically significant results.
One week later, all three conditions increased behavior to get self-test kits. VR and AR both increased behavior to get a vaccine/an additional booster. Besides, VR increased behaviors to stay 6 feet apart from people and wear a face mask in indoor public places (Table 2). Thus, H1 and H2 were supported.
Between conditions
H3 and RQ1 questioned whether VR and AR conditions were more effective in promoting desired perceptions and behaviors than video. To examine each condition's effects immediately after message exposure, linear regression was conducted for each intention or perception. In the regression model, condition was the independent variable, intention or perception measured at T2 was the dependent variable, and the corresponding behavior or perception measured at T1 was the covariate. Results revealed that VR was more effective in increasing the perceived harm of COVID-19 and intentions to get a yearly COVID-19 vaccine if available than video. AR was not significantly more effective than video (Table 3).
Perceptions and behaviors between conditions.

Note. p = Adjusted p. Values in bold indicates statistically significant results.
To examine each condition's effects after one week, linear regression was conducted with conditions as the independent variable, each behavior or perception measured at T3 as the dependent variable, and the same variable measured at T1 as the covariate. VR and AR conditions were not significantly more effective than video (Table 3). Thus, H2 was supported immediately after message exposure. H4 was not supported.
RQ2 aimed to compare the effectiveness of VR and AR in reducing psychological distances. Kruskal-Wallis test with Benjamini-Hochberg method adjusting for multiple comparisons revealed that three conditions were significantly different in perceived social, spatial, and hypothetical distances. Specifically, VR reduced more social distance than AR. VR reduced more spatial and hypothetical distances than AR and video. However, AR and video did not differ in perceived distances. Three conditions were not significantly different in perceived temporal distance (Table 4).
Psychological distances between conditions.
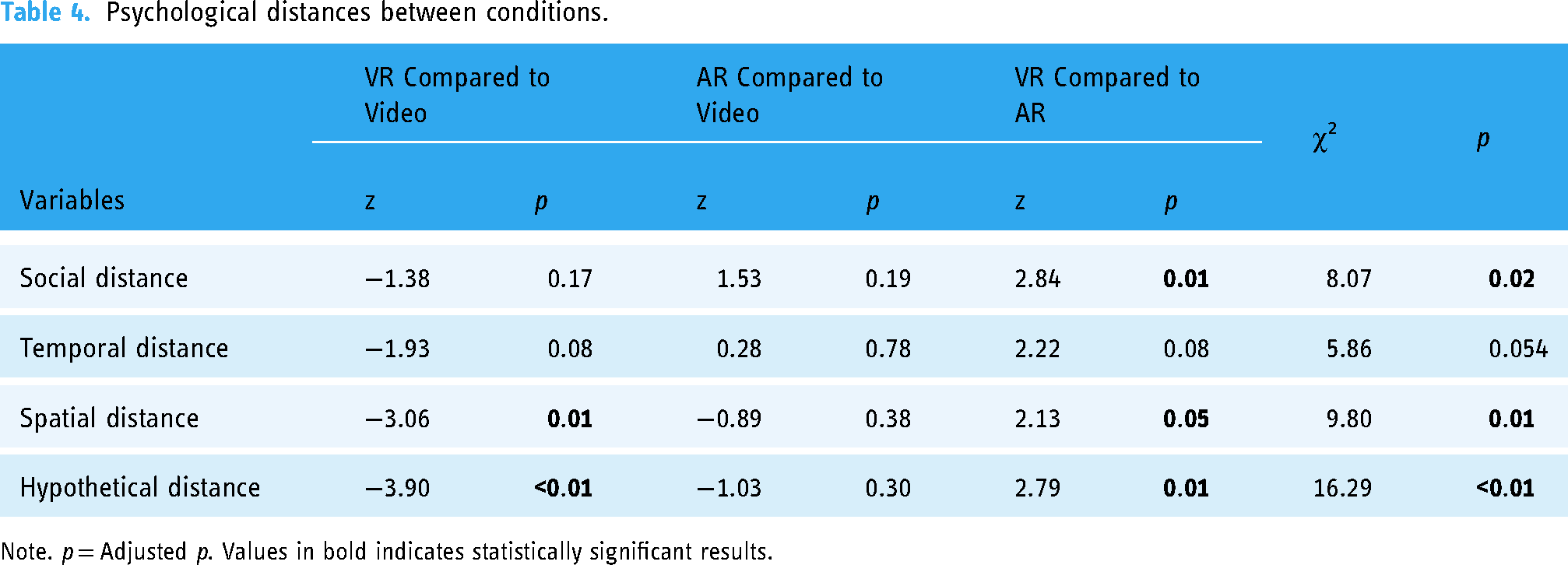
Note. p = Adjusted p. Values in bold indicates statistically significant results.
RQ3 focused on comparing the effectiveness of VR and AR in increasing risk perceptions and promote healthy behavior change. Linear regression results revealed that immediately after message exposure, VR was more effective than AR in increasing perceived likelihood of having COVID-19, perceived harm of COVID-19, as well as intentions to self-test before joining indoor gathering if feeling sick and get a yearly vaccine if the COVID-19 vaccine became a yearly shot. One week later, VR was more effective than AR in increasing behaviors to avoid crowds, stay 6 feet apart from people, and wear a face mask in indoor public places (Table 3).
Discussion
We found that both VR and AR increased preventive intentions and behaviors against COVID-19 both in the short and long run. VR was particularly effective as it also increased risk perceptions, more preventive intentions in the short term, and more preventive behaviors, including social distancing and mask wearing, in the long term. Interestingly, although all three conditions increased intentions to continue social distancing and wear masks immediately following message exposure, VR was the only intervention that generated actual behavior change after one week, which indicated a potential long-term advantage of VR compared to other mediums. Similarly, a few studies indicate that the impact of VR could have a lasting effect 1 and that VR's superiority over less immersive forms of media may become more pronounced over time. 12 Our research, in conjunction with previous studies, underscores the importance of investigating the enduring effects of VR and how it affects the various dimensions of psychological distance in future research.
Compared to the CDC video, VR proved to be a more efficient method in increasing perceived harm of COVID-19 and generating intentions to get a yearly COVID-19 vaccine immediately following message exposure. This might be because VR was able to diminish spatial and hypothetical distances to a greater extent in comparison to video, as revealed in the results, which might in the end increase risk perception and desired intention change. The VR intervention immersed users into the virtual environment where users were forced to contract the coronavirus spread by the VR character. In contrast, the CDC video was 2D and could not reduce the physical distance between the user and the risk. Moreover, as the CDC video had a lower level of immersion, it was difficult for users to imagine themselves in a hypothetical scenario where they were directly exposed to the harm of COVID-19. However, VR was not found to be more persuasive than the CDC video after one week. One possibility is that both the VR intervention and CDC video increased preventive behaviors; yet, the difference between these two conditions in behavior change was not significant enough.
Contrary to our prediction, AR was not more persuasive than video, with no significant difference between them. This could potentially be due to the AR intervention in this study and the CDC video did not differ in perceived distances. It is possible that since AR merely superimposes virtual information onto the real world, users’ thoughts are still more focused on the real world instead of the 3D images. 27 The limited immersive experience that AR provides 28 is not able to generate significantly different levels of psychological distances than video. Thus, it did not result in better outcomes than video. Moreover, the addition of information and images through AR technology to physical reality may potentially act as a distraction and negatively impact performance, 29 which may further restrict the level of immersion. Another plausible explanation is that young people often use AR face filters on social media platforms such as Instagram or Snapchat. The main motivation for using these AR filters is to experience pleasure or amusement. 34 Thus, participants might be desensitized to the AR intervention in this study, and may not have perceived the exaggerated virus to be harmful to themselves.
Findings from the AR and video extends construal level theory by revealing that more immersive media does not necessarily reduce psychological distances and lead to ideal outcomes. The message content and user motivation may be more important in influencing construal level. For example, the content in the CDC video presented several concrete strategies on how to prevent the spread of COVID-19 (e.g., avoiding crowds, getting a COVID-19 vaccine). Kim et al. suggest that messaging in high-level health campaigns address the ‘why’ whereas low-level construals address the “how”. 23 Thus, the video intervention may have achieved low-level construal through the campaign's messaging, which may explain the lack of significant psychological distances from the use of AR. Study findings offer theoretical insight on the effectiveness of various modalities for health interventions.
The limitations of the AR intervention can also help explain the reason why VR proved to be more effective than AR. Another reason may be that VR decreased social, spatial, and hypothetical distances to a greater degree than AR, as found in the present study. Previous research also suggests that by isolating users from the physical world, VR can have a larger impact on risk perception than AR. VR is more adept at illustrating imaginary scenarios and producing experiences that defy the physical laws of our world, 29 which may include portraying visual viruses. Taken together, these findings contribute to the VR/AR literature by demonstrating the advantage of VR in creating a more immersive experience, further lowering construal level, and generating better persuasive outcomes than AR.
There are several limitations worth noting. Firstly, the study's sample only consisted of individuals with some college education, and thus, future studies should investigate VR and AR interventions across different age groups and socioeconomic backgrounds. Next, VR and AR messages in this study seemed to have a narrative storyline, while the video was more informative, which could potentially influence responses. Additionally, we did not measure participants’ prior exposure to AR technology. Individuals might have varying frequencies of using AR face filters on social media platforms, potentially influencing their responses to the AR app developed in this study. Finally, although some researchers suggest that single-item measures are recommended when the measures are clear and precise,35,36 future research may consider using multi-item measures to capture the entire construct range.
Conclusions
Despite the limitations, this study was one of the first to explore the differences between VR and AR in changing psychological distance and health behaviors. It designed, tested, and compared VR and AR campaigns to encourage proactive measures to prevent the spread of COVID-19. It demonstrates how VR and AR can have both immediate and lasting impacts on promoting healthy intentions and behaviors in preventing COVID-19. Theoretically, this study extends construal level theory by investigating the differences between VR and AR in reducing psychological distances. Findings, while centered on COVID-19 prevention messaging, hold implications in light of ongoing sporadic outbreaks of coronavirus and other viruses within the general population. These insights extend beyond the pandemic phase, offering practical applications for employing VR and AR technologies in health campaigns. As VR and AR devices become increasingly affordable, the study foresees a near future where these technologies could effectively facilitate public outreach, raising awareness not only about COVID-19 but also about various other diseases and health concerns.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241269587 - Supplemental material for Comparing virtual reality vs. augmented reality in promoting COVID-19 self-testing, vaccination, and preventive behaviors
Supplemental material, sj-docx-1-dhj-10.1177_20552076241269587 for Comparing virtual reality vs. augmented reality in promoting COVID-19 self-testing, vaccination, and preventive behaviors by Zhan Xu and Linda Dam in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to thank Hao Guo for her assistance in data analysis, Jerry Thull for his support, the Strategic Communication Research Lab at NAU for producing VR and AR campaigns. We deeply appreciate the insightful comments from the editors and the reviewers.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Yes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Arizona’s Technology and Research Initiative Fund (Project number 2627006) and NAU School of Communication.
Guarantor
Arizona's Technology and Research Initiative Fund (Project number: 2627006) and NAU School of Communication.
Contributorship
Author 1: writing - original draft, conceptualization, methodology, experimentation, funding acquisition. Author 2: Writing - original draft, review & editing, conceptualization, experimentation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.