
Abstract
Objective
Technologically adapted mirror therapy shows promising results in improving motor function for stroke survivors. The treatment effects of a newly developed multi-mode stroke rehabilitation system offering multiple training modes in digital mirror therapy remain unknown. This study aimed to examine the effects of unilateral mirror visual feedback (MVF) with unimanual training (UM-UT), unilateral MVF with bimanual training (UM-BT), and bilateral MVF with bimanual training (BM-BT) on clinical outcomes in stroke survivors, compared to classical mirror therapy (CMT).
Methods
Thirty-five participants were randomly assigned to one of four groups receiving fifteen 60-minute training sessions for 3–4 weeks. The Fugl-Meyer Assessment for Upper Extremity (FMA-UE), Chedoke Arm and Hand Activity Inventory (CAHAI), Revised Nottingham Sensory Assessment (rNSA), Motor Activity Log (MAL), and EQ-5D-5L were administered at pre- and post-intervention and at 1-month follow-up.
Results
After intervention and follow-up, significant within-group treatment efficacies were found on most primary outcomes of the FMA-UE and CAHAI scores in all four groups. Significant within-group improvements in the secondary outcomes were found on the MAL and EQ-5D-5L index in the UM-BT group, and the rNSA tactile sensation and MAL quality of movement subscales in the BM-BT group. No significant between-group treatment efficacies were found.
Conclusions
UM-UT, UM-BT, BM-BT, and CMT led to similar clinical effects on the FMA-UE and can be considered effective alternative interventions for post-stroke upper-limb motor rehabilitation. UM-BT and BM-BT showed within-group improvements in functional performance in the patients’ affected upper limbs in real-life activities.
Keywords
Introduction
Stroke still prevails as the third leading cause of global disease burden, 1 as well as accounting for almost 6% of global disability-adjusted life-years. 2 One of the most common post-stroke problems is upper-limb motor impairments, which often cause difficulty in motor skills and incoordination of movements that can interfere with performing daily activities. 3 Over half of stroke survivors who manifest deficits in motor and daily functions become chronically disabled. 4 Because upper-limb functional recovery is viewed as the most important goal for stroke survivors, 5 attention should be devoted to delivering effective and specific interventions for upper-limb motor rehabilitation.
Recently, mirror therapy, a therapeutic treatment with a mirror to create a visually illusory reflection for relieving amputee pain and improving motor function,6,7 has become a promising and effective intervention for improving the upper-limb motor function of stroke survivors. Classical mirror therapy (CMT) entails stroke survivors practicing repetitive motor training while watching a visually illusory reflection of the motor acts of the unaffected upper limb in a plain mirror 8 or mirror box. 9 The image is superimposed on the affected upper limb, providing what is known as mirror visual feedback (MVF). MVF, as visual stimulation, is believed to activate the neural network and cause cortical reorganization in the patient's brain to alleviate phantom pain or enhance upper-limb motor function following stroke. 10 Two meta-analyses found that in comparison with control interventions, CMT had significantly medium effect sizes on upper-limb motor impairment and function,11,12 as well as on activities of daily living. 12 However, some limitations of CMT include the following: (1) a mirror or a mirror box vertically set in the midsagittal plane of patients may cause neck tension and trunk postural pressure of users13,14; (2) CMT cannot provide bilateral reciprocal or alternating movements 15 ; and (3) the types and small sizes of mirror boxes limit the diversity of movements or tasks. 16
Notably, the various intervention protocols of CMT include differences in the MVF and manual exercise. There are two different kinds of MVF, namely, unilateral MVF and bilateral MVF, which have different brain activation effects. Unilateral MVF provides the illusory mirrored reflection of the unaffected limb movement, whereas bilateral MVF provides the actual visual stimulation of the unaffected limb movement in addition to unilateral MVF. That is, depending on the specific nature of the feedback, unilateral MVF affects the primary and secondary visual processing areas, whereas bilateral MVF activates more frontal and parietal regions, which are connected with higher cognitive functions such as attention and action monitoring. 10 During bilateral MVF, the movements of the unaffected limb and its mirror reflection may be hard to comprehensively observe for stroke survivors, especially from the side. Regarding manual exercise, a recent systematic review revealed that the number of CMT studies using unimanual training of the unaffected limb was equivalent to the number using symmetrically bimanual training of both the unaffected and affected limbs. 17 A previous meta-analysis revealed that during CMT, unimanual movement of the unaffected upper limb had a greater treatment effect on motor impairment and function in stroke survivors than did bimanual movement of both the unaffected and affected upper limb. 16 Nevertheless, the treatment effects of mirror therapy in different MVF conditions and training modes in stroke survivors remain unknown.
With advances in digital imaging technology, a novel multi-mode stroke rehabilitation system, which addresses some disadvantages of CMT and provides digital mirror therapy with multiple training modes of mirror therapy, has been developed and validated for usability and feasibility. 18 This system can capture images of the movement of the unaffected upper-limb movement and simultaneously transform them into a mirrored version representing the affected upper-limb movement. Both versions are presented on the screen over both upper limbs as bilateral MVF for observation from the front, thus overcoming the limitation of CMT, which is viewed from the side. Thus, based on the two different kinds of MVF (unilateral and bilateral MVF) in combination with two types of manual exercise (unimanual training vs. bimanual training), the multi-mode stroke rehabilitation system can provide three different modes of digital mirror therapy: unilateral MVF with unimanual training (UM-UT), unilateral MVF with bimanual training (UM-BT), and bilateral MVF with bimanual training (BM-BT). Further investigation into the treatment effects of these three modes of digital mirror therapy in stroke survivors is warranted.
This study aimed to examine the clinical efficacies of UM-UT, UM-BT, and BM-BT on different aspects of clinical outcomes in chronic stroke survivors and to compare them with the efficacy of dose-matched CMT. The hypotheses of this study were as follows: (1) The UM-UT, UM-BT, BM-BT, and CMT would have effects of different extents on clinical outcomes in stroke survivors; (2) regarding the manual exercise effect, the UM-UT (i.e., unimanual training) and UM-BT (i.e., bimanual training) would have effects of different extents on clinical outcomes in stroke survivors; and (3) regarding the MVF effect, the UM-BT (i.e., unilateral MVF) and BM-BT (i.e., bilateral MVF) would have effects of different extents on clinical outcomes in stroke survivors.
Methods
Participants
A total of 35 participants were recruited from the physical medicine and rehabilitation departments of three urban hospitals in northern Taiwan. The participants were recruited if they met the inclusion criteria: (1) diagnosis of unilateral stroke; (2) stroke with the onset of more than 6 months before participation; (3) age between 20 and 80 years; (4) Fugl-Meyer Assessment for Upper Extremity (FMA-UE) score at baseline between 20 and 60 19 ; and (5) ability to follow the study instructions (i.e., a Mini-Mental State Examination, 2nd Edition: Standard Version [MMSE-2:SV] score ≥ 21). 20 The exclusion criteria were: (1) diagnosis of global or receptive aphasia; (2) severe neglect, as indicated by a mean deviation ≥ 1.5 inches on the line bisection subtest of the Behavioral Inattention Test; and/or (3) major medical problems or comorbidities that could interfere with upper-limb usage or result in severe pain.
This study was approved by the Institutional Review Boards of the Chang Gung Memorial Hospital, Linkou (approval number: 202002234A3); the Taipei Hospital, Ministry of Health and Welfare (approval number: TH-IRB-0021-0030); and the Cheng Hsin General Hospital (approval number: (861)110A-07), and written informed consent was obtained from each participant before data collection.
Study design and procedure
This study was a four-arm, single-blind, randomized controlled trial. Each participant received routine rehabilitation intervention (e.g., 30–60-minute occupational and/or physical therapy sessions per day for 2–4 days per week) and the study intervention protocol of fifteen 60-minute training sessions for 3–4 weeks as an additional treatment. Well-trained research staff (occupational therapists) provided verbal instructions, assistance, and feedback to the participants as appropriate for the study treatment. In addition, the same rater, who was blinded to the study intervention group allocation, administrated the outcome measures to each participant at pre- and post-intervention and at 1-month follow-up.
Following the baseline assessment, the participants were randomly allocated to one of the four arms of the study groups in a 1:1:1:1 ratio according to the stratified random sampling method (i.e., FMA-UE score of 20–40 [moderate-to-severe] versus 40–60 [mild-to-moderate], 19 and right- versus left-sided brain lesion). The randomization was carried out online on the Research Randomizer website (http://www.randomizer.org). For concealment of the random allocation, a research assistant was independently responsible for the randomization procedure and allocation of patients to the intervention groups. The study protocol was prospectively registered at ClinicalTrial.gov (registration number: NCT04813120).
Intervention
The three experimental groups, namely, the UM-UT, UM-BT, and BM-BT, received the treatment protocols of digital mirror therapy delivered by the multi-mode stroke rehabilitation system, 18 whereas the dose-matched CMT group received traditional mirror therapy using a mirror box (Figure 1). Three common categories of movements and tasks (active range of motion [AROM], reaching movements, and object manipulation) were provided during therapy in each session, and 20 minutes were scheduled for each.
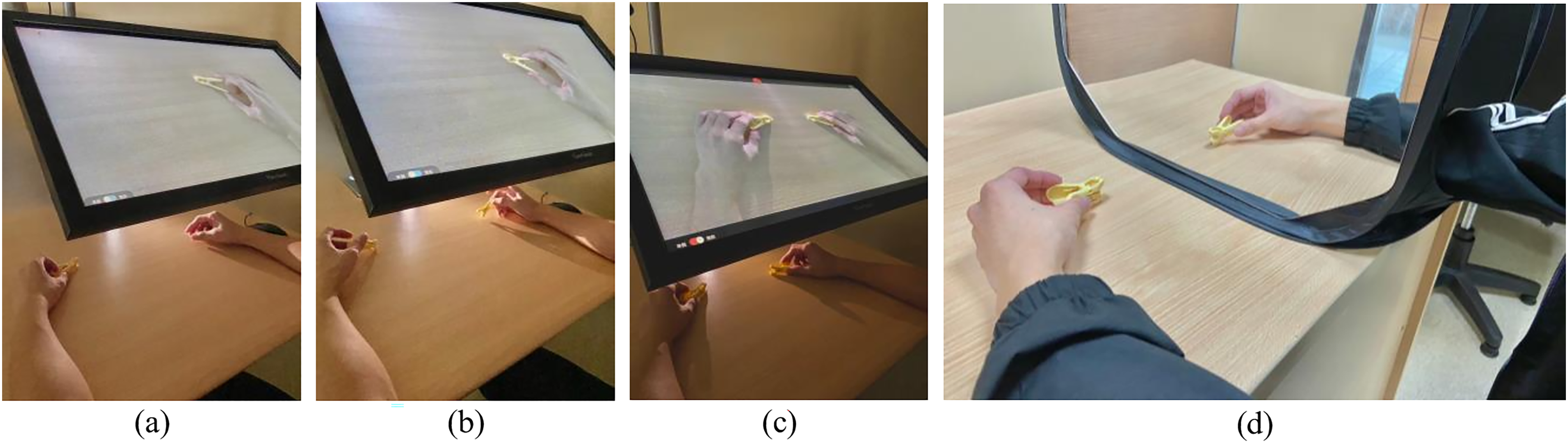
Demonstration of three different modes of digital mirror therapy: (a) UM-UT, (b) UM-BT, and (c) BM-BT; and (d) CMT. BM-BT: bilateral mirror visual feedback with bimanual training; CMT: classical mirror therapy; UM-BT: unilateral mirror visual feedback with bimanual training; UM-UT: unilateral mirror visual feedback with unimanual training.
Unilateral MVF with unimanual training. For the UM-UT group, the participants sat in front of a computer screen and were instructed to carefully watch the instantly transformed, real-time image reflection of motor acts of the unaffected arm and hand on the screen, which was superimposed on the affected arm and hand (i.e., unilateral MVF). Meanwhile, the participants were instructed to imagine that the motor acts were being performed by the affected arm and hand. In this UM-UT group, only the unaffected limb was required to perform the movements (i.e., unimanual training).
During the AROM exercises period, the participants carefully observed the instantly transformed, real-time image reflection of AROM exercises performed by the unaffected arm and hand on the screen while they simultaneously imagined that the exercises were performed by the affected arm and hand. The AROM exercises consisted of elbow, forearm, wrist, and finger movements. During the reaching movements and object manipulation periods, depending on each participant's motor ability and progress, the participants were asked to execute 1–2 reaching movements and 1–2 object manipulation tasks every session. Similarly, the participants carefully observed the instantly transformed, real-time image reflection of reaching or object manipulation movements of the unaffected arm and hand on the screen and simultaneously imagined that the movements were those of the affected arm and hand. The object manipulation tasks consisted of in-hand manipulation, grip and pinch, grasp and release, and transport and turning objects.
Unilateral MVF with bimanual training. During the UM-BT, as with the UM-UT group, the participants were also instructed to carefully watch the instantly transformed image reflection of motor acts of the unaffected arm and hand on the screen (i.e., unilateral MVF) and to imagine that the motor acts were performed by the affected arm and hand. However, in this UM-BT group, while the unaffected limb performed the movements, the participant attempted to use the affected arm and hand to perform them simultaneously to the extent that they were able (i.e., bimanual training).
Bilateral MVF with bimanual training. During the BM-BT, the participants were instructed to carefully view the instantaneously transformed image reflection of motor acts of the unaffected arm and hand on the screen, which was superimposed on both the affected arm and hand and the unaffected arm and hand (i.e., bilateral MVF). Meanwhile, the participants needed to imagine that the motor acts were performed by both the affected and unaffected arms and hands. However, in this BM-BT group, as in the UM-BT group, while the unaffected limb executed the movements, the affected one simultaneously did so to any extent possible (i.e., bimanual training).
Classical mirror therapy. For the CMT group, the participants sat in front of a mirror box placed at their midsagittal plane. They then placed the affected arm and hand inside the mirror box and the unaffected arm and hand in front of the mirror. The participants were instructed to carefully observe the mirrored images of the movements performed by the unaffected arm and hand in the mirror, as the images were superimposed on the affected arm and hand in the mirror. Meanwhile, the participants had to imagine that the movements were performed by the affected arm and hand. In this CMT group, only the unaffected arm and hand were required to perform the movements.
Outcome measures
Primary outcomes. The FMA-UE, a measure with sound psychometric properties, evaluates upper-limb hemiparesis after stroke21,22 by assessing the reflexes and movements of the shoulder/elbow/forearm, wrist, and hand, as well as coordination/speed. The FMA-UE has 33 items and a score range of 0–66. The scores can be further divided into proximal and distal parts with score ranges of 0–42 and 0–24, respectively. 19 A higher score indicates better upper-limb motor function.
The Chedoke Arm and Hand Activity Inventory (CAHAI), a reliable and validated measure, assesses the functional ability of stroke patients to perform daily activities by using their affected upper limbs. 23 It includes a total of 13 real-life functional tasks, such as opening a coffee jar and zipping up a zipper. The total score is between 13 and 91, 24 and a higher score indicates greater functional independence.
Secondary outcomes. The Revised Nottingham Sensory Assessment (rNSA) is a standardized measure with sound reliability, validity, and responsiveness for assessing sensory function in patients with stroke.25,26 The tactile sensation subscale of the rNSA was applied. This subscale has a total maximum score of 108 and includes six aspects: light touch, temperature, pinprick, pressure, tactile location, and bilateral simultaneous touch. Each aspect consists of a three-point ordinal scale scored from 0 to 2 for each region of the body. Higher scores indicate better somatosensory function.
The Motor Activity Log (MAL), a semi-structured questionnaire with good psychometric properties, evaluates the performance level of using the affected upper limb in 30 real-life daily tasks, including two aspects: the amount of use (AOU) and quality of movement (QOM). Each aspect consists of a six-point ordinal scale with a total maximum mean score of 5. 27 Higher mean scores indicate greater use and quality of the affected upper limb in daily activities.
The EQ-5D-5L is a standardized measure to assess health status with different degrees of severity. 28 The description system of the EQ-5D-5L contains five dimensions, namely, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, scored on a five-point ordinal scale. According to the Chinese EQ-5D-5L value set, the worst (55555) health state produces an index score of −0.391, while the best (11111) health state produces an index score of 1. 29
Statistical analysis All data analyses were performed in IBM SPSS 22.0 software. A two-sided p-value of <0.05 was considered to indicate significance. Nonparametric tests were used because of the small sample size in each group. The demographic and baseline clinical characteristics among the four groups were compared using the nonparametric Kruskal–Wallis test. The intention-to-treat analysis with the last observation carried forward method was used to deal with the data of the dropout participants.
The within-group differences in the scores of outcome measures between pre- and post-intervention and between pre-intervention and 1-month follow-up were examined using the nonparametric Wilcoxon signed rank test. The between-group differences in outcome measures from pre- to post-intervention and from pre-intervention to 1-month follow-up among the four groups were examined using the nonparametric Kruskal–Wallis test. If the Kruskal–Wallis test was significant, Dunn's test with Bonferroni correction was performed for post hoc multiple pairwise comparisons.
For subgroup analysis, the manual exercise effect of the UM-UT versus UM-BT groups (i.e., unimanual vs. bimanual training) and the MVF effect of the UM-BT versus BM-BT groups (i.e., unilateral vs. bilateral MVF) from pre- to post-intervention and from pre-intervention to 1-month follow-up were examined using the nonparametric Mann–Whitney U test.
Results
Demographic and baseline clinical characteristics
During the coronavirus disease 2019 (COVID-19) pandemic, between October 2021 and June 2023, a total of 132 stroke survivors were recruited. Of them, 97 were excluded and the remaining 35 were randomized to one of the four study interventions (Figure 2). Table 1 lists the demographic and baseline clinical characteristics of the stroke survivors. No statistically significant differences were found in the baseline characteristics among the four groups (Table 1). In addition, all the participants complied with and completed the intervention protocols, except for those who dropped out due to COVID-19 (n = 2) and a fall (n = 1). During the study intervention period, no adverse effects were reported.

Flowchart of study participants.
Demographic and baseline clinical characteristics of participants.

AOU: amount of use; BM-BT: bilateral mirror visual feedback with bimanual training group; CAHAI: Chedoke Arm and Hand Activity Inventory; CMT: classical mirror therapy group; FMA-UE: Fugl-Meyer Assessment for Upper Extremity; H: hemorrhagic; I: ischemic; MAL: Motor Activity Log; MMSE-2:SV: Mini-Mental State Examination, 2nd Edition: Standard Version; QOM: quality of movement; rNSA: Revised Nottingham Sensory Assessment; SD: standard deviation; UM-BT: unilateral mirror visual feedback with bimanual training group; UM-UT: unilateral mirror visual feedback with unimanual training group.
Within-group and between-group comparisons
On primary outcome measures (Table 2), statistically significant differences were found between pre- and post-intervention in the UM-UT, UM-BT, BM-BT, and CMT groups on the FMA-UE total (p = 0.011–0.027), FMA-UE proximal (p = 0.017–0.041), and FMA-UE distal (p = 0.017–0.026). By contrast, all but the BM-BT group showed significant improvements in the CAHAI (p = 0.008–0.027). Furthermore, statistically significant differences were found between pre-intervention and 1-month follow-up in the UM-UT, UM-BT, BM-BT, and CMT groups on the FMA-UE total (p = 0.011–0.028), FMA-UE proximal (p = 0.017–0.027), and FMA-UE distal (p = 0.007–0.043). However, only the UM-BT and CMT groups showed significant improvements in the CAHAI (p = 0.012 and p = 0.046, respectively).
Within-group and between-group comparisons of primary outcome measures among the four groups.

BM-BT: bilateral mirror visual feedback with bimanual training group; CAHAI: Chedoke Arm and Hand Activity Inventory; CMT: classical mirror therapy group; FMA-UE: Fugl-Meyer Assessment for Upper Extremity; SD: standard deviation; UM-BT: unilateral mirror visual feedback with bimanual training group; UM-UT: unilateral mirror visual feedback with unimanual training group.
*p < 0.05.
On the secondary outcome measures (Table 3), statistically significant differences were found between pre- and post-intervention in the UM-BT group on the MAL AOU (p = 0.038), MAL QOM (p = 0.008), and EQ-5D-5L index (p = 0.028), and in the BM-BT group on the rNSA tactile sensation subscale (p = 0.042) and MAL QOM (p = 0.018). Moreover, statistically significant differences were found between pre-intervention and 1-month follow-up in the UM-BT group on the MAL AOU (p = 0.008), MAL QOM (p = 0.021), and EQ-5D-5L index (p = 0.030), and in the BM-BT group on the rNSA tactile sensation subscale (p = 0.042).
Within-group and between-group comparisons of secondary outcome measures among the four groups.

AOU: amount of use; BM-BT: bilateral mirror visual feedback with bimanual training group; CMT: classical mirror therapy group; MAL: Motor Activity Log; QOM: quality of movement; rNSA: Revised Nottingham Sensory Assessment; SD: standard deviation; UM-BT: unilateral mirror visual feedback with bimanual training group; UM-UT: unilateral mirror visual feedback with unimanual training group.
*p < 0.05.
Among the four groups, no statistically significant differences were found in the change scores between pre- and post-intervention on primary and secondary outcome measures (Tables 2 and 3). A statistically significant difference between pre-intervention and 1-month follow-up was found on the MAL AOU (p = 0.024); however, no significant post hoc comparisons were noted (Tables 2 and 3).
Manual exercise and MVF effects
Regarding the manual exercise effect, no statistically significant differences between the UM-UT and UM-BT groups from pre- to post-intervention or from pre-intervention to 1-month follow-up were found on primary and secondary outcome measures (Table 4). However, regarding the MVF effect, statistically significant differences were found between the UM-BT and BM-BT groups from pre- to post-intervention on the CAHAI (p = 0.041) and EQ-5D-5L index (p = 0.039), and from pre-intervention to 1-month follow-up on the MAL AOU (p = 0.012), with the UM-BT group improving the most (Table 4).
Manual exercise effect and MVF effect on outcome measures.

AOU: amount of use; BM-BT: bilateral mirror visual feedback with bimanual training group; CAHAI: Chedoke Arm and Hand Activity Inventory; FMA-UE: Fugl-Meyer Assessment for Upper Extremity; MAL: Motor Activity Log; MVF: mirror visual feedback; QOM: quality of movement; rNSA: Revised Nottingham Sensory Assessment; UM-BT: unilateral mirror visual feedback with bimanual training group; UM-UT: unilateral mirror visual feedback with unimanual training group.
*p < 0.05.
Discussion
To the best of our knowledge, this is the first study to examine the clinical efficacies of UM-UT, UM-BT, and BM-BT delivered with the digital mirror therapy system on different aspects of rehabilitation outcomes in chronic stroke survivors in comparison with those of CMT, and further to compare the manual exercise effects of UM-UT versus UM-BT and the MVF effect of UM-BT versus BM-BT. The results of within-group comparisons demonstrated that, after the study intervention, the UM-UT, UM-BT, and CMT groups had significant improvements in the primary FMA-UE total, proximal, and distal scores, and on the CAHAI; by contrast, the BM-BT group showed significant improvements in the FMA-UE scores but not on the CAHAI. For secondary outcomes, the UM-BT group demonstrated significant improvements in the MAL AOU, MAL QOM, and EQ-5D-5L index scores, whereas the BM-BT group had significant improvements in the rNSA tactile sensation and MAL QOM scores. However, after 1-month follow-up, most of the significant improvements after intervention persisted, except for those on the CAHAI score in the UM-UT group and MAL QOM score in the BM-BT group. Our preliminary findings revealed that all four study interventions (i.e., UM-UT, UM-BT, BM-BT, and CMT) had treatment efficacies on arm and hand motor function measured by the FMA-UE; however, UM-BT and BM-BT had within-group improvements on functional activities of daily living. In addition, no manual exercise effect was found between the UM-UT and UM-BT groups; however, between the UM-BT and BM-BT groups, there were statistically significant MVF effects on the CAHAI and EQ-5D-5L index after the study intervention, as well as on the MAL AOU at 1-month follow-up, with the UM-BT group showing greater improvement.
Based on the same motor priming paradigm (i.e., mirror therapy), 30 different MVF conditions and training modes (i.e., UM-UT, UM-BT, and BM-BT) delivered by the digital mirror therapy system and the traditional mirror therapy (i.e., CMT) all demonstrated significant improvements in upper-limb motor function, except for the BM-BT group on the CAHAI score. However, only the UM-BT and BM-BT groups had significant within-group gains in performance in daily activities. One possible reason behind the smallest and nonsignificant improvements in the CAHAI for the BM-BT group might be that the BM-BT group had the greatest percentage of stroke survivors with the dominant hand affected, in addition to the CAHAI only assessing the contribution of the affected upper limb to everyday bimanual, gender-neutral tasks. Moreover, a potential explanation for the improvements in the MAL after the UM-BT and BM-BT interventions may be that bimanual training had more treatment efficacy on QOM. 5 This greater efficacy might be attributed to both the increase in functional magnetic resonance imaging (fMRI) activation in the contralesional (intact) superior frontal gyrus, which correlated with faster functional motor performance, 31 and the recruitment of fMRI activation in the ipsilesional (impaired) cerebellum, which was mostly interconnected with the contralesional hemisphere, which correlated with good functional recovery (i.e., high degrees of upper-limb motor recovery). 32
Our study findings showed that, for the manual exercise effect, there were no statistically significant differences between unimanual training (i.e., UM-UT) and bimanual training (i.e., UM-BT) in the change scores on primary and secondary outcome measures. These findings, to some extent, coincided with the discrepancies between the results in the study of Geller et al. 33 and in a meta-analysis by Morkisch et al. 16 The former reported finding no statistically significant between-group differences, but in comparison with the UM-BT, upper-limb recovery in motor impairments and activity gains were higher in the UM-UT group; in contrast, the latter stated that UM-UT, with more robust changes, had greater effects on both motor function and motor impairment than UM-BT did. In addition, the kinematic study results of Selles et al. revealed that UM-UT also had more efficacy in movement time than did UM-BT. 34 However, the effects of UM-BT versus UM-UT on upper-limb motor function appear equivocal. A further large-scale study is warranted to confirm the results of this preliminary study.
Regarding the MVF effect, the results of this study revealed statistically significant differences indicating greater efficacy of UM-BT over BM-BT on the change scores of the CAHAI and EQ-5D-5L index after intervention, and on the MAL AOU after follow-up. An explanation might be that under the bilateral MVF condition, the actual visual stimulation of the unaffected limb movement might have distracted attention from the illusory mirroring reflection of the unaffected limb movement provided under the unilateral MVF condition, which might have decreased the treatment efficacy. Some other studies have investigated the neurophysiological effects of MVF in stroke patients, employing various MVF conditions. Bartur et al. investigated the neurophysiological effects of multiple conditions (i.e., non-paretic upper-limb, without MVF, with MVF, bilateral movements with MVF), and they found that MVF reduces the hemispheric asymmetry and the magnitude of low-beta event-related desynchronization during unilateral movement. 35 Furthermore, Chang et al. compared the effects under the conditions of no MVF, bilateral synchronized, and reciprocal MVF, and they observed increased cortical activation in the supplementary motor area with bilateral reciprocal MVF. 15 Additionally, Tai et al. showed that in a stroke group, the percentage change of M1 beta oscillatory activity decreased significantly more in the condition of MVF with bilateral hand movements, indicating greater M1 neural activities with MVF during bilateral hand movements. 36 Fong et al. found that stroke individuals showed a shift in sensorimotor event-related desynchronization toward the contralateral hemisphere in response to MVF that accompanied unimanual movement. 37 Overall, MVF appears to promote more symmetrical and balanced neural activities in stroke patients. However, the neurophysiological mechanisms of unilateral and bilateral MVF in stroke patients still need to be further investigated.
The key contribution of this preliminary study is that it reports the first examination in the clinical use of UM-UT, UM-BT, and BM-BT delivered by the multi-mode stroke rehabilitation system and provides comparisons of manual exercise and MVF effects during digital mirror therapy. Given the clinical treatment efficacies of the four study interventions, UM-UT, UM-BT, BM-BT, and CMT might be considered as effective alternative approaches to one another for improving upper-limb motor function measured by the FMA-UE. The UM-BT and BM-BT showed within-group improvements in functional performance in real-life activities. The overall preliminary findings might support the clinical use of digital mirror therapy with different MVF conditions and training modes (i.e., UM-UT, UM-BT, and BM-BT) for individualized stroke rehabilitation in stroke survivors.
There were some limitations in this study. One limitation was the potential selection bias of study participants during the COVID-19 period. The study results of Held et al. reported that over 70% of stroke survivors living in the community decreased their attendance in outpatient physical and occupational therapy due to the COVID-19 shutdown. 38 Similarly, the study results of Jeng et al. reported that overall monthly visits for regular outpatient medical appointments declined by 39% due to the COVID-19 pandemic. 39 This trend may have led to the recruitment of stroke patients with higher rehabilitation motivation. Thus, the results of this preliminary study need to be interpreted with caution. Another limitation was the insufficiently large sample size to achieve statistical significance in the between-group comparisons on outcome measures among the four groups. However, the significant within-group findings still deserve our attention, even with the limitation of the sample size. Further studies with larger sample sizes are suggested to draw more solid conclusions.
Conclusions
In conclusion, UM-UT, UM-BT, BM-BT, and CMT all had within-group treatment efficacy on primary FMA-UE motor outcome, whereas UM-BT and BM-BT had additional within-group treatment efficacy on functional performance of daily activities. Our preliminary study findings show that the three different modes of digital mirror therapy, namely, UM-UT, UM-BT, and BM-BT, might be taken as effective alternative intervention strategies to one another for improving arm and hand motor function in chronic stroke survivors.
Footnotes
Acknowledgments
The authors would like to acknowledge all the study participants for their involvement.
Contributorship
YWH made substantial contributions to study conception, and study design and methodology, MTL to data analysis and interpretation, CCC and YWH to resources, and HLL to project administration. YWH supervised the study and acquired the funding for the study. MTL and YWH participated in drafting the manuscript, and CCC and HLL revised it critically. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Boards of the Chang Gung Memorial Hospital, Linkou (approval number: 202002234A3); the Taipei Hospital, Ministry of Health and Welfare (approval number: TH-IRB-0021-0030); and the Cheng Hsin General Hospital (approval number: (861)110A-07).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Council (grant numbers: NSTC 111-2628-B-182-009, NSTC 112-2628-B-182-006, and NSTC 112-2326-B-182-004-MY3) and the Chang Gung Memorial Hospital (grant number: BMRPD25) in Taiwan.
Guarantor
YWH.
Trial registration
The study protocol was prospectively registered at ClinicalTrial.gov (registration number: NCT04813120).