
Abstract
Background
Telerehabilitation (TR) has emerged as a feasible and promising approach for delivering rehabilitation services remotely, utilizing technology to bridge the gap between healthcare providers and patients. As new modalities of virtual care and health technologies continue to emerge, it is crucial to stay informed about the growing landscape of virtual care to ensure that telehealth service delivery is ethical and equitable, and improves the quality of services and patient outcomes.
Objective
The primary objective of this article is to present the protocol of a rapid review to examine the equity-related aspects surrounding the implementation of TR. This includes a comprehensive analysis of the ethical dimensions and fairness concerns linked to this practice.
Methods
A rapid review protocol was developed in accordance with Cochrane Rapid Reviews Methods Guidance. Medline and EMBASE databases were searched between January 2010 and March 2023. Study selection and data extraction will be conducted in two phases (Phase I) by two independent reviewers and subsequently (Phase II) by a single reviewer. Our study will utilize the PROGRESS-Plus and Equitable virtual rehabilitation in the metaverse era framework to identify dimensions where potential inequities may exist within TR interventions.
Results
This rapid review is anticipated to enhance our knowledge of TR in the fields of physiotherapy and occupational therapy, with a specific focus on its influence on ethical and equitable practices and providing a foundation for informed decision-making and improved patient care.
Conclusion
This rapid review will contribute to the advancement of our understanding of TR within physiotherapy and occupational therapy. Through synthesizing existing evidence, this study not only addresses current gaps in knowledge but also offers valuable insights for future research and clinical practice in TR services.
Introduction
In the past decade, technology and telehealth have gained prominence in rehabilitation services, particularly for reaching disadvantaged populations in remote areas. 1 Telehealth, a broad term encompassing various modalities, involves using telecommunications for healthcare delivery, including patient rehabilitation. 2 Telerehabilitation (TR), a subset of telehealth, utilizes technologies like audio, videoconferencing, and apps for rehabilitation services. TR covers a range of functions, enhancing quality of life, functionality, and accessibility for individuals with disabilities, especially those in remote locations. It has proven effective in reducing waiting times for rehabilitation services and enhancing continuity of care. 3
The use of TR in physiotherapy and occupational therapy has increased worldwide, especially following the COVID-19 pandemic. 4 Challenges and barriers in TR delivery, with associated ethical concerns, have been noted. A scoping review on telemedicine ethics identified key concerns related to confidentiality, accessibility, effectiveness, and the patient–physician relationship. Issues such as limited internet access, outdated devices, and varying payment methods were discussed. 5 However, these challenges seem relatively narrow compared to broader telehealth experiences. Additionally, the review highlighted technical hurdles like device availability, slow connections, and privacy concerns in TR implementation.
Some ethical concerns come to light when looking at digital literacy and costs of such interventions for patients and professionals. Regarding literacy, for healthcare professionals, recent studies in TR revealed varied digital literacy in healthcare, emphasizing a gap between digital growth and workforce capabilities. Training needs include establishing digital literacy standards, career-specific training for digital literacy in healthcare for professionals, including courses and programs tailored to equip healthcare professionals with the necessary digital skills; clinical data utilization in order to stay current with innovation. 6 Consistent themes are the necessity of training for improved digital literacy in delivering virtual care and ensuring secure data management.6,7 Furthermore, several studies have highlighted a lack of information regarding TR costs, including indirect costs. 8 While intervention duration and frequency are commonly reported in TR studies, there is a common lack of information regarding the ongoing costs of these interventions.8–10
Although not yet thoroughly explored with regard to TR, ethics holds a pivotal role in rehabilitation. The importance of better integrating ethical reflection in rehabilitation practice has indeed been increasingly discussed by Foye 11 and Drolet and Hudon, 12 such as in the fields of physiotherapy and occupational therapy. The study by Drolet and Hudon 12 emphasizes the need for comprehensive training for physiotherapy students and for support mechanisms for practicing physiotherapists to ensure they possess the necessary tools to analyze the ethical complexities of their professional practice. By recognizing and proactively addressing ethical considerations in practice, the healthcare and rehabilitation community could forge a more ethical practice that could better serve the people and groups to which they provide care.12,13
Among key ethical considerations in healthcare and rehabilitation are matters of equity. Health equity aligns with human rights principles and is defined as “the absence of systematic disparities in health (or in the major social determinants of health) between groups with different levels of underlying social advantage/disadvantage—that is, wealth, power, or prestige. Inequities in health systematically put groups of people who are already socially disadvantaged (e.g. by virtue of being poor, female, and/or members of a disenfranchised racial, ethnic, or religious group) at further disadvantage with respect to their health.” 14 Ethics, including aspects of equity, thus form an essential foundation in delivering rehabilitation services characterized by fairness and inclusivity. Following ethical reflection, it then becomes essential that rehabilitation clinicians and decision-makers advocate with and for patients and those close to them to receive TR care that respects their dignity, priorities, and needs. 15 Although the development of TR seems to have improved access to rehabilitation services for many people, 16 important concerns around equity have been raised regarding the capacity of technologies to meet the needs of individuals living with disabilities, such as vision, hearing, sensorimotor, and communication impairments. 17
While telemedicine has undoubtedly acquired substantial attention in terms of its potential to enhance healthcare accessibility and delivery of medical services, this has not yet been examined for telehealth solutions in the area of rehabilitation. Consequently, there is a distinct gap in our understanding of equity considerations intersecting in TR. This rapid review aims to summarize evidence from prior reviews and relevant recent studies to contribute to providing recommendations for equitable and ethical TR services. In particular, this rapid review will: (a) explore the current state and trends of TR research, including interventions used, targeted populations, and implementation barriers and facilitators and (b) identify ethics and equity-related considerations of TR service delivery.
Methodology and steps accomplished
The proposed methodology for this study is a rapid review of reviews and primary articles. A rapid review and a systematic review are two distinct approaches to synthesizing and summarizing research evidence, each with its own set of characteristics and advantages. A systematic review is a comprehensive and rigorous method of evidence synthesis. 18 It follows a structured and meticulous process. A rapid review is a more expedited approach to evidence synthesis. 18 It aims to provide a quicker overview of the available evidence while maintaining a degree of rigor. The main difference between rapid reviews and systematic reviews lies in the depth and rigor of the process. While systematic reviews offer the highest level of reliability and comprehensiveness, rapid reviews are a practical alternative when time is and resources are limited, or when time is critical for decision-making in rapidly evolving fields such as TR. 19
For our research, a rapid review methodology is the most suitable approach to efficiently summarize the extensive body of research conducted on TR over the past years, including the ethical and equity considerations that have emerged during this period. This choice was driven by the need to provide a timely and concise synthesis of this evolving field to meet the pressing demands of policymakers, healthcare professionals, researchers, and the broader community. Given the dynamic nature of TR and the urgency of addressing ethical and equity concerns, a rapid review ensures that our findings are quickly available for informed decision-making and user accessibility.
Telehealth is one of the fastest-growing healthcare sectors, and the number of studies published on this topic was increasing even before the COVID-19 pandemic. 20
The rapidly evolving landscape of virtual care in rehabilitation demands a timely assessment of the existing body of knowledge. As new technologies and practices continually emerge, it is crucial to ensure that the study is based on the most up-to-date and relevant information available.
The review consists of two main phases: (a) a review of existing reviews of TR in the areas of physical and occupational therapy and (b) a review of new studies emerging in this field. These are detailed in the following sections, highlighting the steps accomplished to date. This review follows the steps outlined in King et al.'s guide and the Cochrane Rapid Reviews—Interim Guidance from the Cochrane Rapid Reviews Method Group, which defines rapid reviews as a “form of knowledge synthesis that accelerates the process of undertaking a traditional systematic review through streamlining or omitting specific methods to produce evidence for stakeholders in a resource-efficient manner.” 20 This rapid review is part of a more extensive research study entitled “Avoiding pitfalls in virtual care: paving the road for more ethical and equitable policies and practices in rehabilitation,” in which the rapid review of the scientific literature on rehabilitation aims to inform current clinical and organizational virtual rehabilitation best practices, guidelines, and policies. Prospero ID: CRD42020207602.
The steps in the proposed review are chosen and adapted to take into account the goal of informing the subsequent steps of the study and, more rapidly, producing results that clinicians and decision-makers could use.
Needs assessment, topic selection, and topic refinement: A preliminary literature search was conducted to inform discussions with stakeholders such as representatives of professional organizations and patient associations and clinicians to establish the scope of the review, which included four fields of rehabilitation (physiotherapy, occupational therapy, psychology, and speech therapy) across the lifespan. We are working on a series of rapid reviews, and this one focuses specifically on physiotherapy and occupation therapy. The research team and the physiotherapy and occupational therapy interest groups then refined the research topic and specified the objectives. Protocol development: During this step, based on the research questions identified by the research team using the PICOTSS (Population, Intervention, Comparison, Outcome, Timeframe, Study Design, and Setting) framework, the research protocol for the review was developed. Literature search: While rapid reviews involve searching multiple databases, our approach focused on efficiency and relevance to streamline the process to gather as much relevant literature as possible while providing relevant findings more rapidly. We included two databases in which much of the rehabilitation scientific literature can be found (see search strategy on supplementaty material).
Search strategy
A librarian, in consultation with members of the research team, performed the search, and all search terms were developed based on the PICOTSS, 21 as outlined in Table 1. The identified articles were imported to Covidence, an online software for managing systematic reviews. 22
Criteria for inclusion/exclusion of studies.
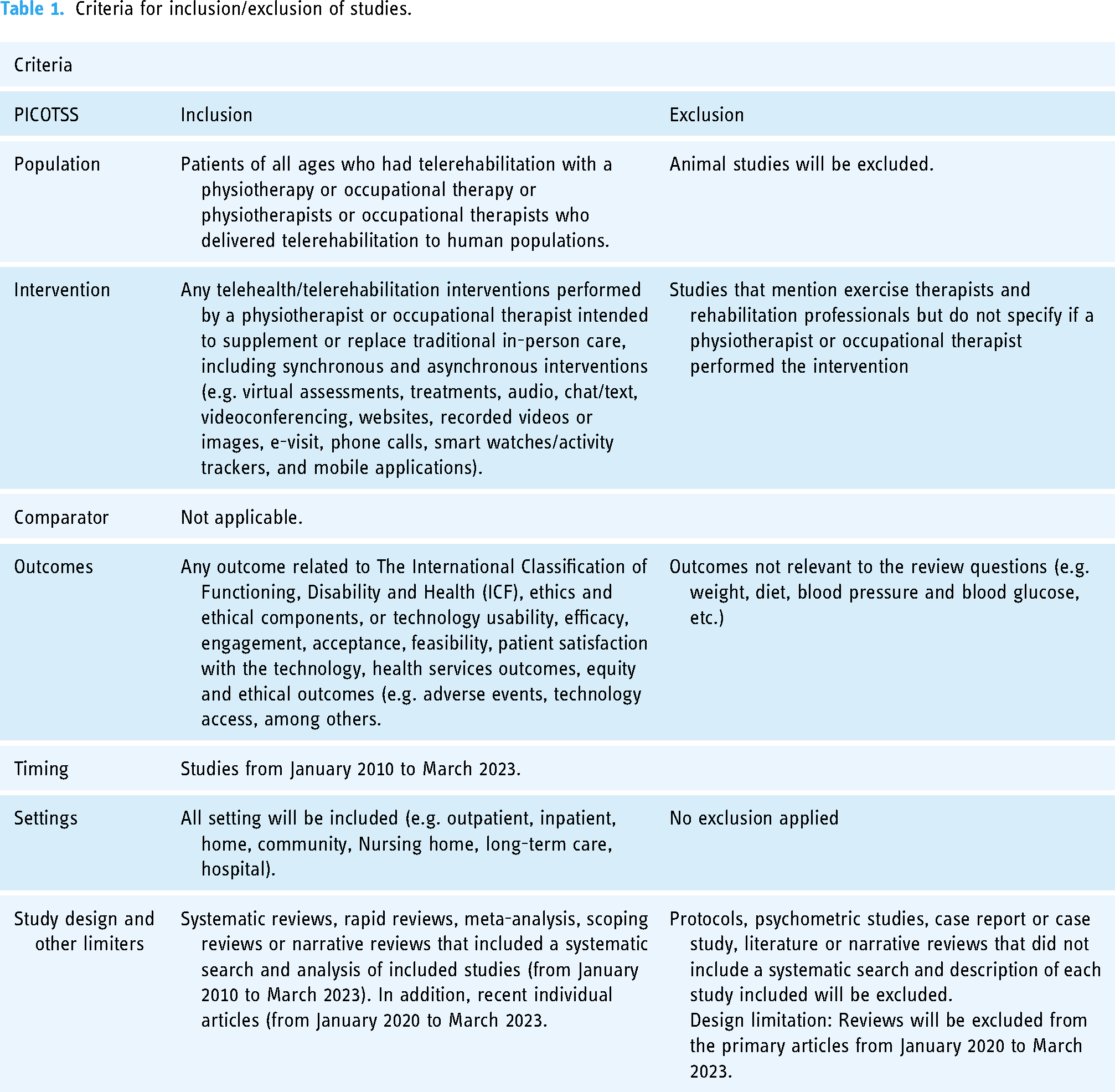
The current protocol for a rapid review includes the following databases of published works: Medline and Embase databases. These databases were selected for their comprehensive coverage of medical literature, making them well-suited for capturing relevant TR reviews and studies. It includes articles in English and French published from January 2010 to March 2023, including all study designs. Then, a selection of study designs will be applied as specified in Table 1.
The search incorporated a range of essential keywords to cover the three main concepts of TR, occupational therapy, and physiotherapy. These keywords included “telerehabilitation” and its synonymous terms, ensuring a thorough exploration of the field by using related terms like “telehealth,” “online-based intervention,” and “online consultation,” reflecting the study's broader scope in the realm of TR. The search also focused on “physiotherapy” and “occupational therapy” and their synonymous counterparts.
Screening and study selection: Rapid reviews often employ various approaches, which can vary significantly.21 In the case of this review, we opted for a specific strategy where two reviewers were responsible for applying the inclusion and exclusion criteria, while one person handled the initial screening with a subset of 10% records being independently verified by another reviewer.
23
Eligibility criteria
This review uses the PICOTSS framework to inform eligibility criteria to guide the inclusion and exclusion of studies. The included studies contain individuals of diverse age groups who underwent TR with either a physiotherapist, occupational therapist, or a combination of these. Animal studies were omitted from our study. To be included in the rapid review, reviews and studies are needed to discuss specifically TR interventions conducted by physiotherapists or occupational therapists aiming to enhance or replace conventional in-person care. This includes both synchronous and asynchronous approaches, such as virtual assessments, treatments, audio, chat/text, video conferencing, websites, recorded videos or images, e-visit, phone calls, and mobile applications (Table 1). Moreover, studies incorporating any form of technology, including gaming, apps, or digital health technologies, were considered, provided that the intervention involved interaction with a clinician—whether synchronous or asynchronous—within any setting. We have excluded studies that refer to exercise therapists and rehabilitation professionals without clarifying whether a physiotherapist or an occupational therapist carried out the intervention.
This review includes studies reporting outcomes from any domain of The International Classification of Functioning, Disability and Health (ICF). This encompasses a broad spectrum, including efficacy outcomes, technology usability, engagement, acceptance, feasibility, patient satisfaction with the technology, health services outcomes, equity, and ethics considerations, such as adverse events and technology access. Furthermore, studies without patient outcomes are also included, as it is crucial to examine gaps in outcomes.
Inclusion criteria for study design varied based on the year of publication. From 2010 to 2020, systematic reviews, rapid reviews, meta-analyses, scoping reviews, and narrative reviews (if they included a systematic search and a list/description of included studies) will be included. From 2020 onwards, primary studies with quantitative, mixed, or qualitative designs will be included, while review articles and case studies will be excluded.
The rationale for this difference in study design and timeline is as follows: The launch of the smartphone in 2007 led to significant technological advancements, including in healthcare. Therefore, from 2010 to 2020, the focus was on including review articles that provide a comprehensive overview of key developments in the field. Given the abundance of existing reviews during this period, the approach involved exclusively incorporating review articles. From 2020 onwards, the criteria shifted to capture the recent studies conducted during the COVID-19 pandemic and encompass the latest advancements and challenges in the field. We acknowledge the importance of incorporating various study designs while establishing that our criteria will not impose extensive limitations, except for excluding reviews and case studies from 2020 onwards. Recognizing the importance of incorporating experimental studies, pre-and post-intervention analyses, feasibility studies, and various study designs that contribute significantly to ethical considerations across diverse research methodologies, we further emphasize our commitment to ethical concerns throughout the research process. It is crucial not only to acknowledge ethical aspects explicitly stated in the paper but also to extend our examination to the type of evidence obtained and the ethical considerations it introduces. Our ethical analysis during the review process ensures a thorough examination of not only the content presented but also the methods employed, fostering a comprehensive understanding of the ethical implications across various dimensions of research methodologies. See Table 1 for a summary of the inclusion and exclusion criteria.
Data collection process
The initial literature search resulted in 1556 publications that met the search criteria. These publications were exported to Covidence. Two reviewers independently assessed the titles and abstracts of the identified studies for their relevance. After excluding 13 articles that were duplicates, a total of 1543 articles were screened to determine if they met the inclusion criteria. Out of these, 986 articles were deemed ineligible and excluded. This left 557 articles to undergo to a detailed title and abstract screening.
This process was divided into two steps because physiotherapists and occupational therapists frequently collaborate within multidisciplinary teams. In the first step, two independent reviewers conducted the initial title and abstract screening. They assessed the inclusion of key terms in the title or abstract and the relevance to the topic. Any conflict arising between the reviewers was resolved through discussion with a third reviewer (DK or JS) until a final consensus decision was reached. In the second step, the remaining articles were then screened by one reviewer using a similar process to identify articles related to physical and occupational therapy TR. This division helps ensure that we do not inadvertently overlook relevant TR review articles that may not pertain specifically to the physical or occupational therapy component if not included in the initial search strategy. At this time, the remaining eligible articles will undergo to full-text eligibility assessment by MV to meet eligibility criteria outlined in PICOTSS followed by data extraction when the article is retained.
Data extraction: Data extraction will be conducted by a single reviewer, with a second reviewer performing accuracy checks on a random sample of at least 10% of the extractions
We will use a predefined data extraction tool to extract data from the review studies using the Covidence systematic review software and Microsoft Excel. Key variables refer to study country, study design, population, TR mode, description of the interventions, cost, digital literacy adaptative equipment, access to technology, autonomy, data security, type of ethnicity, adverse events, results, limitations, and ethical concerns, among others. This structured approach will facilitate consistent and comprehensive data capture. Data extraction will be guided by the Metaverse Equitable Rehabilitation Therapy (MERTH) framework, which addresses equity aspects in TR.
15
The framework comprises five domains: equity, health services integration, interoperability, global governance, and humanization. These domains will be adapted to identify equity and ethical concerns in the included studies.
15
This framework allows reflection on ethical considerations using two deductive and two inductive ethical approaches. Our study will also employ the PROGRESS-Plus framework to identify dimensions across which TR inequities may exist across the interventions. This framework explores dimensions including place of residence, race/ethnicity/culture/language, occupation, gender or sex, religion, education, socioeconomic status, social capital (e.g. older adults living alone or based on marital status), age, disability, and sexual orientation.
24
For this review, we will primarily extract data on place of residence, race/ethnicity/culture/language, occupation, gender, education, socioeconomic status, age, and disability.
Equity in TR services is intricately linked to various sociodemographic factors, each presenting unique considerations for both fairness and ethical practice. The geographical aspect, including place of residence, is important as individuals in rural or remote areas may encounter challenges related to technological infrastructure and internet connectivity.
25
Cultural diversity, comprising race, ethnicity, language, and culture, demands an approach to ensure linguistic and cultural humility in TR services, reflecting a commitment to both equity and ethical standards.
26
Occupational demands and gender roles contribute to variations in accessibility, necessitating flexible scheduling to accommodate diverse needs. Educational levels can influence the ability to engage with TR, emphasizing the importance of educational initiatives to bridge disparities.
27
Socioeconomic status, age, and disability introduce further dimensions, as financial resources, age-related technology adoption, and disability accommodations play crucial roles in ensuring equitable access.
28
As providers navigate these considerations, they must strive to implement solutions that align with principles of justice, inclusivity, and respect for diversity, ultimately fostering a TR landscape that is both equitable and ethical principles. MV will conduct data extraction. JS and DK will perform accuracy checks on a random sample of at least 10% of the extractions.
Critical appraisal: In rapid reviews, the selection of an appraisal instrument can vary, encompassing both standard and customized approaches
The quality appraisal of the included studies will involve a careful review specifically related to the quality of each study. For example, we will use Joanna Briggs Institute (JBI) Critical Appraisal Checklist for systematic reviews and research syntheses.
29
A single reviewer will determine the criteria for indicating a “yes,” “no,” “unclear,” or “not applicable” response in the review context for each of the 11 items. We will use the JBI critical appraisal tools for primary studies according to the specific study design.
This critical appraisal assessment is instrumental in offering information about the overall fairness of the studies under review. The research team will examine study quality, with particular attention given to assessing the risk of bias related to ethics and equity. This analysis will aid in identifying whether all population groups have been adequately included, ensuring the incorporation of those groups that should be part of the studies, thereby addressing equity concerns.
Synthesis: This rapid review will adopt an interactive approach to the synthesis process, actively involving both the research team and stakeholders such as community organizations, patient associations, healthcare managers and decision-makers, and representatives of professional organizations
Strategy for data synthesis
For this rapid review, we will adhere to the PRISMA 2020 reporting guidelines to ensure a comprehensive, transparent, and systematic approach to conducting and reporting our review. 30 The included reviews will undergo a narrative synthesis and descriptive statistics approaches to categorize and summarize the extracted data. 31 We will organize and present the key findings from the included studies in a narrative format. Focus on common themes, patterns, or divergent results. This synthesis method will organize the findings into themes and categories, allowing for comprehensive data analysis. 31 Descriptive statistics will involve calculating and presenting basic statistical measures (e.g. means, percentages) to summarize study results. This hybrid approach involves translating quantitative findings, typically expressed numerically, into qualitative descriptions or themes. 31 Its approach consists of providing an overview of the characteristics and findings of included studies and the applicability of the evidence using PROGRESS-Plus, explaining and interpreting results, analyzing the overall strengths and weaknesses of the body of evidence, identifying gaps in the research, and comparing findings where applicable. This approach will examine the synthesized evidence of ethical and equity considerations in TR, contributing to a comprehensive understanding of the included studies to address the research questions.
Analysis of subgroups or subsets
We will conduct subgroup analyses to identify distinctions and commonalities between disciplines, patient groups, settings, and TR characteristics, among other critical components of TR. By comparing the data into these subgroups, we gain valuable insights into the factors contributing to TR practices. This understanding can help identify best practices, potential gaps, and areas for improvement within each discipline, ultimately enhancing the quality of care provided in TR settings. Additionally, subgroup analysis can extend to geographic differences, offering a comprehensive view of how TR is implemented across various regions. This can be instrumental in recognizing disparities in access, resources, and healthcare delivery, which are essential factors in ensuring equitable and effective TR services. By exploring potential geographic variations, we can tailor recommendations and interventions to address specific needs within different locales, thus advancing the reach and impact of TR.
Report production and dissemination: The research team will develop tools to summarize findings and recommendations for the different stakeholders. Emphasis will be placed on simple yet comprehensive tools. Recognizing the imperative of equity in dissemination, our approach strongly emphasizes tailoring report formatting to meet the needs of individual requesters and diverse stakeholder audiences. In addition to ensuring clarity and accessibility in presenting the results, we will actively integrate findings from research on evidence summary presentation. Importantly, we will consider the specific needs of decision-makers in both high- and low-middle-income countries, prioritizing an inclusive approach that considers the unique challenges and contexts of these settings. By integrating equity considerations into our dissemination strategy, we aim to enhance the relevance of our findings across diverse settings and contribute to a more inclusive and accessible dissemination process. This commitment aligns with our overarching goal of making the results widely accessible and applicable, fostering a more equitable impact across the spectrum of stakeholders.
Preliminary results
The initial literature search resulted in 1556 publications that met the search criteria. These publications were exported to Covidence. Two reviewers independently assessed the titles and abstracts of the identified studies for their relevance. After excluding 13 articles that were duplicates, a total of 1543 articles were screened to determine if they met the inclusion criteria. Out of these, 986 articles were deemed ineligible and excluded. This left 557 articles to undergo a full-text screening.
Discussion
This review's primary novelty and distinctive contribution lies in exploring the complex interplay between TR and equitable and ethical provision of rehabilitation services. While acknowledging the significance of incorporating grey literature, especially for policy and practice relevance, where it often contains valuable reports and documents related to healthcare policy and practice, our decision to exclude it in this review was influenced by several factors. Primarily, due to time constraints, we focused on high-quality, peer-reviewed studies in our review of TR. The extensive amount of grey literature on the topic was deemed unsuitable for our purposes and timeline, as it may contain less reliable or incomplete data. In addition, bias assessment, especially in terms of study quality, is pivotal for interpreting findings and enhancing the reliability of our conclusions. We plan to compare and contrast our results with findings from publications of other studies on the topic worldwide.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076241260367 - Supplemental material for A rapid review protocol of physiotherapy and occupational therapy telerehabilitation to inform ethical and equity concerns
Supplemental material, sj-pdf-1-dhj-10.1177_20552076241260367 for A rapid review protocol of physiotherapy and occupational therapy telerehabilitation to inform ethical and equity concerns by Mirella Veras, Jennifer Sigouin, Claudine Auger, Louis-Pierre Auger, Sara Ahmed, Zachary Boychuck, Sabrina Cavallo, Martine Lévesque, Stacey Lovo, William C Miller, Michelle Nelson, Nahid Norouzi-Gheidari, Jennifer O’Neil, Kadija Perreault, Reg Urbanowski, Lisa Sheehy, Hardeep Singh, Claude Vincent, Rosali Wang, Diana Zidarov, Anne Hudon and Dahlia Kairy in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to thank the Institut de recherche en santé du Canada, Association médicale canadienne 32 and Réseau québécois de recherche en adaptation-réadaptation (REPAR) for their support for this study.
Contributorship
All authors of this work have made substantial contributions to the research process regarding conception and design. MV, DK, AH and JS developed the protocol. MV wrote the first draft and subsequent versions. All the authors participated in editing and revising it critically for important intellectual content and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Dissemination
The authors confirm that no Ethical Committee approval is needed. This study aims to outline how TR can improve access to rehabilitation services and offer insights for fostering ethical and equitable delivery of physiotherapy and occupational therapy. Key considerations involve ensuring technology access, addressing cultural and social concerns, managing security risks, promoting patient autonomy, preventing the amplification of existing inequalities, and integrating ethical decision-making frameworks into TR practices.
Funding
Institut de recherche en santé du Canada, Association médicale canadienne 32 Réseau québécois de recherche en adaptation-réadaptation (REPAR)
Informed Consent
Not aplicable because this study does not involve direct participation of individuals. Ethics approval was not required for this review. Research Gurantor: Dahlia Kairy, Programme de physiothérapie, École de readaptation, Faculté de Médecine, Université de Montréal, 7077 Park Ave, Montreal, Quebec H3N 1X7, Canada. Email: dahlia.kairy@umontreal.ca
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.