
Abstract
Objective
Clinician experiences with technical issues during video consultations can have a negative impact on their willingness to use technology in practice. The objective of this study was to evaluate the presence and impact of technical issues during exercise video consultations on exercise intensity achieved in-session for people with complex chronic conditions.
Methods
Twenty-one people (9 men, 12 women, mean age: 50 ± 14 years) with kidney or liver disease and at least one feature of the metabolic syndrome who participated in an exercise video consultation intervention were included. All treatment notes from consultations were audited for exercise intensity, presence and types of technical issue experienced, troubleshooting techniques attempted and resolutions. Between-group comparisons were conducted to examine differences in exercise intensity indicators between sessions with and without technical issues.
Results
Out of 270 video consultations, 15% (n = 40) experienced technical issues, primarily related to audio-visual quality. Presence of technical issues did not result in lower exercise intensity based on any measure. Many sessions (46%) did not meet prescribed intensity targets, primarily due to participant fatigue, pain, and session time constraints.
Conclusions
Technical issues in this exercise video consultation intervention were not common and did not adversely affect exercise intensity attainment in-session. However, many participants did not achieve target intensities, possibly due to metabolic co-morbidities. These findings support the viability of video consultations for exercise delivery, emphasizing the need for tailored training and support to optimize exercise in complex patient populations. Future research should explore strategies to enhance exercise intensity during virtual consultations for people with metabolic co-morbidities.
Introduction
Higher physical activity levels are associated with decreased risk of lifestyle-related chronic conditions, such as type 2 diabetes and cardiovascular disease.1,2 Approximately one third of adults are not sufficiently active worldwide, 3 with only 25% of Australians reaching physical activity, aerobic and resistance training guidelines. 4 There is an ongoing need to evaluate service delivery for physical activity and exercise support. Video consultations involve the use of synchronous telecommunication in the form of a video-linked appointment between a clinician and healthcare recipient, and provide an opportunity to deliver sustainable, convenient and effective health service. 5 In response to COVID-19 public health restrictions, Australia's universal healthcare system (Medicare) introduced temporary reimbursable item codes for telehealth allied health services (telephone and/or video consultation) in 2020, which became permanent in 2022. 6 Despite rapid initial uptake resulting from restrictions to in-person care, sustained uptake and adoption of telehealth services across allied health professions has not been realised. 7 Specifically, delivery of exercise physiology services via video consultation during Australian public health restrictions averaged ∼0.5% of total reimbursable claims nationally in 2021. 8
An Australian survey identified that audio-visual disruptions to video consultations were the most frequently made complaint by allied health professionals during the COVID-19 pandemic. 9 Perception of technical issues during consultations can have a profound negative impact on clinician willingness to use telehealth for practice.9,10 However, recent evidence in physiotherapy video consultations for people with knee osteoarthritis suggests that while technical issues occur, they are typically minor and have negligible impact on session quality. 11 Similar observations are made in exercise-specific video consultations across chronic disease groups, where technical issues are uncommon and most often able to be resolved quickly through troubleshooting. 12 These findings suggest that technical issues related to video consultations may not influence the delivery of the clinical session for health professionals to a substantial extent.
There is a perception among exercise physiologists that technical disruptions during video consultations reduce the intensity at which participants exercise. 12 Exercise intensity is a core component of clinical exercise prescription, and factors that constrain sufficient intensity are important to identify and address. Participants not reliably attaining exercise intensity may discourage clinicians from using video consultations as an exercise delivery tool. 13 Therefore, the primary aim of this study was to evaluate the potential presence and impact of technical issues in exercise video consultations on exercise intensity in-session. The secondary aim was to describe the nature and frequency of all technical issues present in an exercise video consultation intervention. Based on the findings of previous research in physiotherapy practice, 11 it was hypothesized that technical issues would not adversely affect the exercise intensity achieved within video consultations for participants with complex chronic conditions.
Methods and materials
Study design
The current study used data from the U-DECIDE feasibility randomised controlled trial. 14 U-DECIDE was prospectively registered with the Australian New Zealand Clinical Trials Registry (ANZCTR: 12620001282976) and evaluated a digital health diet and exercise intervention for people living with complex chronic disease. The trial was approved by the Metro South Hospital and Health Service's Human Research Ethics Committee (HREC/2019/QMS/58285) and the University of Queensland Human Research Ethics Committee (2020000127). All participants provided written informed consent prior to enrolment.
Participants
Eligibility for the U-DECIDE study has been previously described.14,15 In brief, adults living with kidney or liver disease exhibiting at least one feature of the metabolic syndrome and receiving specialist care at the Princess Alexandra Hospital in Brisbane, Australia, were recruited by dietetics referral. The study was conducted between December 2020 and June 2022. Participants were randomly allocated 1:1 to intervention or comparator. All study participants received a dietary consultation, a physical activity monitor and usual care. Intervention participants selected which digital health option they wished to engage with. They were offered one semi-personalised and unidirectional lifestyle-related text message per week and access to additional digital health service options (increased text message frequency, nutrition app, exercise app, group-based monthly diet and/or weekly exercise video consultations). The sample for this study comprised of sessions completed by intervention participants selecting the exercise video consultation option who attended at least one video consultation.
Procedures
The current study was a retrospective audit of technical issues related to exercise video consultations in the U-DECIDE RCT and exercise intensity metrics. Exercise video consultations were conducted through the Queensland Health Telehealth Portal (Queensland Government, Brisbane). The telehealth portal consisted of a secure live audio-visual videoconferencing platform for participants to access using their personal devices (tablet, phone or computer). Participants were orientated to the telehealth portal at the baseline assessment and were provided with an instruction booklet. The 60-min consultations were conducted weekly and supervised by an Accredited Exercise Physiologist (AEP). Each participant was provided with exercise equipment (light- and medium-grade resistance bands) to facilitate resistance and aerobic training. Exercise prescription for the video consultations consisted of 20 min of aerobic exercise and 30 min of resistance exercise, incorporating a 5-minute warmup/check in and cool down. AEPs facilitating exercise video consultations underwent telehealth-specific training including completion of online modules 16 and one familiarisation session (i.e., how to use and troubleshoot the telehealth portal).
The repetitions in reserve method (RiR) was used for prescribing resistance exercise intensity, and refers to the estimated number of additional repetitions a participant believes they could complete with correct technique at the end of a set of a resistance training exercise. 17 Target resistance training intensity was set at 1–4 RiR per exercise, which correlates to moderate-vigorous exercise. 17 The OMNI-Resistance Exercise Scale (OMNI-RES) of perceived exertion was used in combination with RiR for resistance intensity monitoring. Aerobic exercise intensity was monitored using the ‘talk test’ method. Participants were asked to exercise between an intensity where they could talk but not sing (moderate intensity) and where they could not say more than a few words without pausing (vigorous intensity) during each session. This correlates to a rating from 3 to 7 (‘moderate’ to ‘severe’) on the category-ratio 10 (CR10) Borg rating of perceived exertion scale (RPE; license number LFNZ2Y). 18 For both aerobic and resistance exercise, percentage of age-predicted heart rate maximum (%APHRM) was used to track intensity in combination with target approaches. This was calculated as 208−(0.7×age), 19 or 168−(0.51×age) 20 for people on beta-blocker medication. Given the low fitness and multimorbidity in people with these conditions, 14 participants were given until session 8 of the intervention to meet exercise intensity prescription. Due to this, between-group comparisons were only analysed from session 8 to 26 of the intervention.
Demographics and medications
Sociodemographic and medical data were obtained at baseline via online surveys, review of electronic medical records and phone calls prior to the baseline assessment. Metabolic-related co-morbid conditions were consolidated and recorded at the baseline appointment as hypertension, obesity, type 2 diabetes and/or dyslipidaemia for each participant. Participants completed the Modified Nordic Musculoskeletal Questionnaire (MNMQ) to quantify muscle pain. 21 Medication usage was verified with participants verbally at the baseline appointment by a member of the research team.
Clinical parameters and metabolic syndrome severity
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in triplicate, with measures taken approximately two minutes apart with the participant in a seated position and having rested for at least 10 min. The first BP measurement was discarded, and the mean of the last two readings was used. Waist circumference (WC) was measured by a health care professional at the level midway between the lower rib margin and iliac crest in the horizontal plane 22 and mean recorded. If there was >1.5% difference between measures, a third measure was taken, and the median was recorded. 22 Blood measures were collected and measured after an 8-h overnight fast via specialist referral to a National Association of Testing Authorities accredited pathology laboratory prior to baseline assessments.
The Metabolic Syndrome Severity Score (MetSSS) is a continuous risk assessment score for quantifying severity of the metabolic syndrome. 23 MetSSS was calculated using an algorithm developed from SBP, DBP, WC and fasting blood measures (triglycerides, high-density lipoprotein cholesterol and glucose). RStudio Version 1.3.959 was used for the calculation (R Foundation for Statistical Programming, Vienna, Austria).
Main outcome: exercise intensity and technical issues during video consultations
Attendance, exercise intensity and technical issues data were recorded for each video consultation by the AEP facilitating the session using a standardised treatment notes template. Type of technical issue experienced, troubleshooting techniques attempted and resolutions, and whether the exercise session was unable to be commenced or continued due to technical issues present was also documented. Exercise intensity metrics for each exercise were recorded in real-time and coded within 24 h after the session using a Microsoft Excel spreadsheet (Microsoft, Redmond, WA, USA). For sessions not meeting aerobic or resistance prescription targets for intensity, reasons for non-adherence were documented by the AEP from an a priori list.
All exercise treatment notes were audited by one author (RCCB) after U-DECIDE project completion and the nature of technical issues, exercise intensity achieved and reasons for non-adherence were coded. Type of technical issues was coded as decreased audio and/or visual quality or complete loss of the audio-visual link. Sessions could be coded to have multiple technical issues. Issues not pertaining directly to exercise video consultations (e.g., failed synchronisation with the wearable activity monitor) were not logged as technical issues.
Data analysis
Demographic and exercise video consultation data are reported using descriptives for the entire intervention period. Data were analysed using Statistical Package for the Social Sciences (version 28.0; IBM Corp., Armonk, NY, USA). Since participants were given a lead-in period to reach exercise intensity targets, between-group comparisons were analysed using only data from consultations 8 to 26 of the intervention. Data were tested for normality using the Shapiro-Wilk test and visual inspections of histograms and residual Q-Q plots. Independent t-tests or Mann–Whitney U tests were conducted to examine potential differences for all exercise intensity measurements [%APHRM (aerobic and resistance), RPE, OMNI-RES, RiR] between sessions completed as planned (i.e., those with no technical issues) and those sessions with technical issues. Data are presented as mean ± standard deviation if normally distributed or median [interquartile range (IQR)] if not, unless otherwise stated. Effect sizes are reported as Cohen's d for normally distributed data with 95% confidence intervals. These were interpreted as small (0.2), medium (0.5) or large (0.8). 24 Where data were not normally distributed, ƞ2 was reported. These were interpreted as negligible (0.00), small (0.01), small-to-moderate (0.01–0.09), medium-to-large (0.10–0.25), and large (>0.25). 25 Assumptions for between-group comparisons were verified. Spearman's Rank Correlation analyses were run to assess for correlation between age and number of sessions with technical issues. A chi-squared test of independence was run for sessions with technical issues between those over and under 55 years of age. Between-group comparisons were conducted between the analytical sample of the current study, and the rest of the U-DECIDE RCT cohort. The analyses were two-tailed, and the level of significance was set at p < .05.
Results
Participant characteristics
Participant summary characteristics and study flow are presented in Table 1 and Figure 1 respectively. Exercise video consultation data from a total of 21 participants (9 men and 12 women) were included. Mean age was 50 ± 14 years, with 88% of participants referred from chronic kidney disease (n = 11), or kidney (n = 8) or liver (n = 2) transplant clinics. Participants had a median of 2 out of 4 (range: 0–4) metabolic-related co-morbid conditions (consolidated and recorded as hypertension, obesity, type 2 diabetes and/or dyslipidaemia) and a MetSSS consistent with profound clinical complexity (n = 16, 3.59 ± 1.39). Muscle pain over the last week was reported by 76% of participants. Over one-third (43%) of participants reported taking ten or more prescribed medications daily. Between-group comparisons of the analytical sample for the current study and the rest of the U-DECIDE RCT cohort are reported in Supplementary Material 1. Diastolic blood pressure was significantly lower at baseline for the analytical sample (MD = 4.8 mmHg, p = .02). No other differences were observed. Data from 270 exercise video consultations were included in the current study.

Participant flow.
Baseline summary participant characteristics.

Note. Data presented as mean ± standard deviation unless otherwise stated. n: number; M/F: male/female; km: kilometres; PAH: Princess Alexandra Hospital.
n = 16.
Number of medications prescribed to be consumed daily.
Technical issues
Technical issues and aerobic/resistance exercise sessions not meeting intensity prescription data for video consultations across the entire intervention are presented in Table 2. AEPs reported experiencing technical issues in 15% of video consultations (40/270), with a total of 52 identified in total (sessions could be coded for more than one technical issue). All technical issues identified were problems with audio and/or visual functionality. These included decreased visual functionality (e.g., video lag), decreased audio functionality (e.g., audio and microphone dropout) or complete loss of audio-visual link. Almost three quarters of the video consultations with technical issues were able to be continued without troubleshooting (73%, n = 29/40). Only two video consultations (1% of total) could not be completed after troubleshooting was attempted. No sessions were unable to be commenced due to technical issues. The most common troubleshooting technique was exiting and re-entering the telehealth portal (20% of all techniques, n = 8). No significant correlation was observed between age and number of sessions with technical issues (r = .34, p = .13). While a higher proportion of older adults (≥55 years) experienced at least one technical issue compared to younger participants [7/11 older participants (64%), 4/10 younger participants (40%)], no statistically significant differences were observed (p = .39).
Technical issues and exercise intensity prescription target data for the whole intervention period (26 sessions), and from session 8 to 26.

Sessions could be coded for multiple of the listed reasons. n: number.
The frequency and impact of technical issues was similar to the overall sample for sessions 8–26, with 18% (28/155) experiencing technical issues. All identified issues were problems with audio and/or visual functionality (e.g., frame skipping, microphone signal instability). The majority of sessions were also able to be continued without troubleshooting (23/28, 82%).
Exercise intensity
Across all consultations, 46% (123/270) of sessions did not meet aerobic and/or resistance intensity prescription targets combined for reasons not related to technical issues. For aerobic exercise intensity, 23% of all sessions (n = 63/270) did not meet prescription targets. For resistance exercise intensity, 31% of all sessions (85/270) did not meet prescription targets. From sessions 8 to 26, 32% of sessions did not meet aerobic intensity targets (49/155), and 43% did not meet resistance intensity targets (66/155). Common reasons for not meeting aerobic and/or resistance exercise intensity prescription targets included fatigue and pain experienced by participants resulting in longer rest periods, and prescribed duration at intensity levels not being possible due to time constraints in the session, not issues related to technical disruptions.
Impact of technical issues on exercise intensity
Table 3 presents between-group analyses for exercise intensity measures for video consultations with technical issues compared to those without technical issues, from session 8 to 26 of the intervention (participants given until session 8 to meet exercise intensity targets). For sessions where technical issues occurred, %APHRM for aerobic exercise was higher than those without technical issues [mean difference (95% CI): 4.2% (0.3%–8.0%); p = .03]. No difference was seen in other exercise intensity metrics for either aerobic or resistance exercise (Table 3). Presence of technical issues during sessions did not result in lower exercise intensity for any of the aerobic or resistance exercise monitoring techniques (Figures 2 and 3).
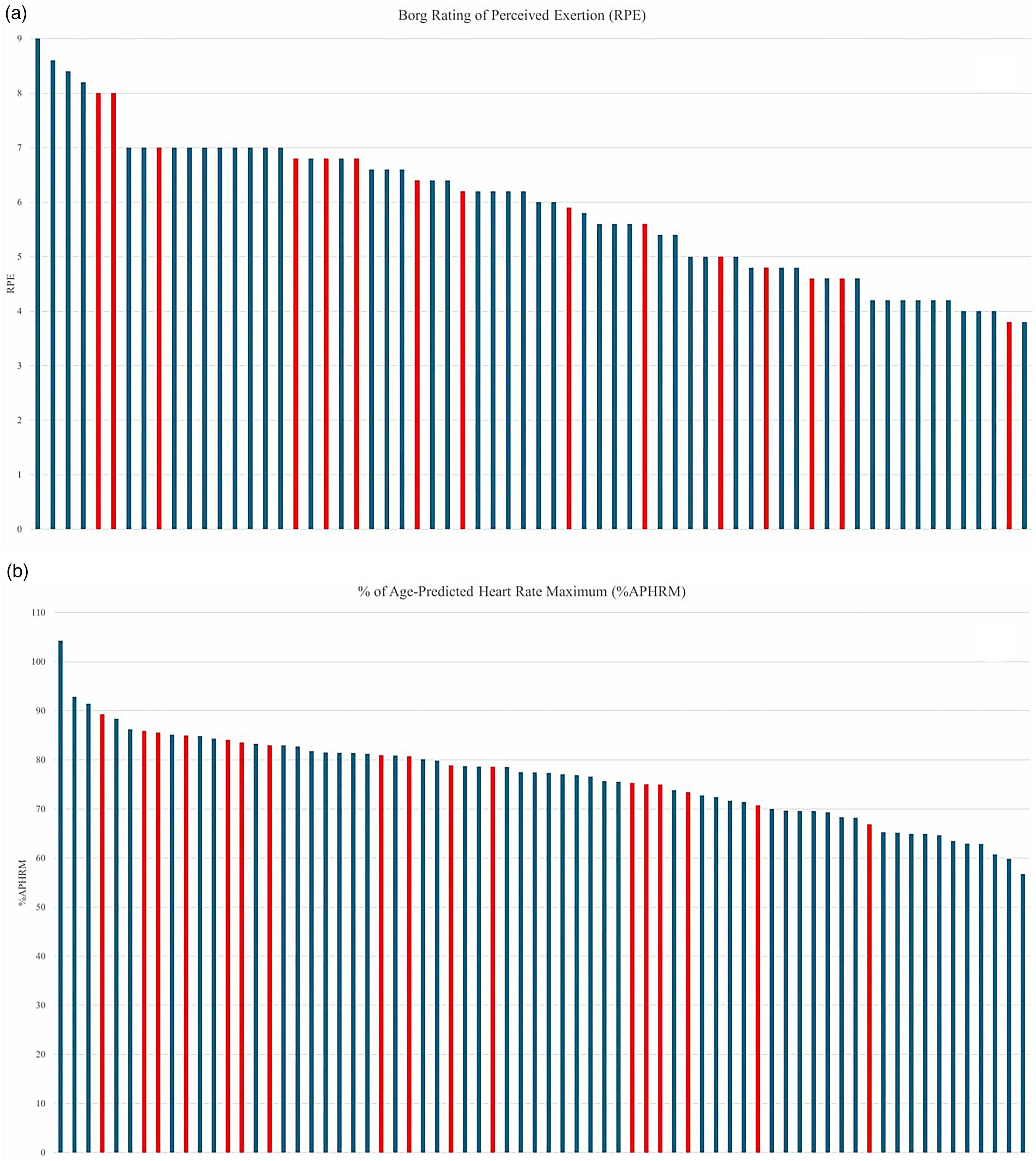
CR10 Borg rating of perceived exertion (a) and % of age-predicted heart rate maximum (b) intensity ratings for aerobic training from session 8 to 26 of the intervention for sessions with technical issues (red) and sessions completed as planned (blue).
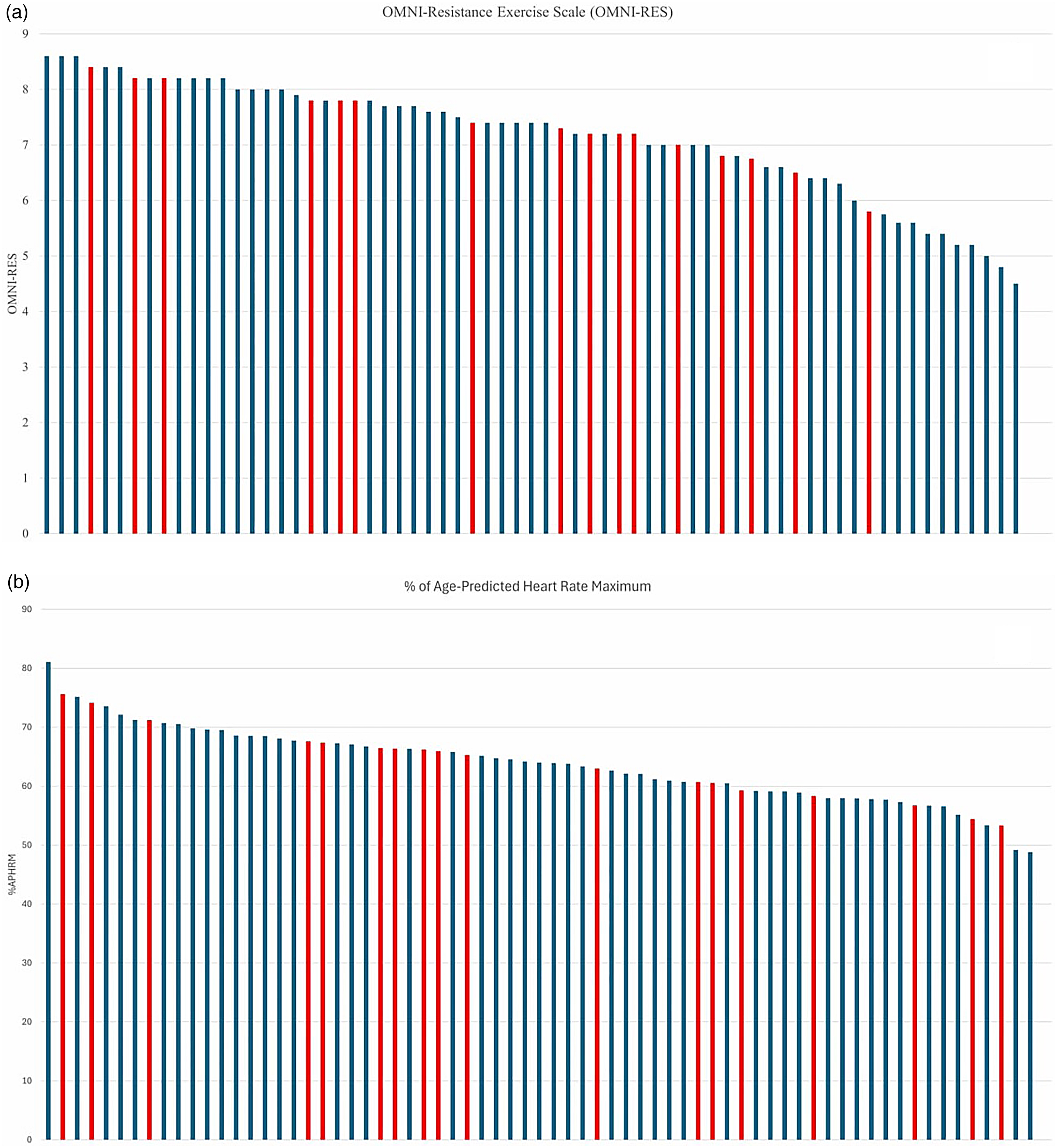
OMNI-Resistance Exercise Scale (a) and % of age-predicted heart rate maximum (b) intensity ratings for resistance training from session 8 to 26 of the intervention for sessions with technical issues (red) and sessions completed as planned (blue).
Exercise intensity target data from week 8 to 26 of the intervention.

Note. Data presented as mean ± standard deviation unless otherwise stated. n: number; %APHRM: percentage of age-predicted heart rate maximum; AE: aerobic exercise; RPE: Borg's rating of perceived exertion; OMNI-RES: OMNI-Resistance Exercise Scale; RiR: repetitions in reserve; MD: mean difference; CI: confidence intervals; N.A.: not available; RE: resistance exercise.
Median [interquartile range].
Eta-squared (ƞ2).
Discussion
This study evaluated the presence and potential impact of technical issues in video consultations on exercise intensity. Presence of technical issues was low, and did not result in lower exercise intensity for either aerobic or resistance training. Additionally, technical issues encountered in the exercise video consultations typically did not require any troubleshooting to fix and were minor in nature. There was no difference between sessions with and those without technical issues for most exercise intensity indicators. These results have important ramifications for the promotion and use of video consultations as a viable tool for exercise service delivery.
The high majority of exercise video consultations in this study were completed without technical issues (∼85% of all sessions). It was observed that ∼15% of sessions encountered at least one technical issue, which is broadly consistent with previous literature in the exercise and health fields.11,12,26,27 A 2021 Cochrane systematic review of telerehabilitation for chronic respiratory disease identified that minor technical issues were present in 12–14% of included trials. 27 However, only a very small portion of sessions had to be ceased due to consistent disruptions (∼0.01% of total sessions run). 27 Of the consultations with technical issues in the current study, most either required no resolution or were fixed through easy-to-implement troubleshooting techniques (e.g., exiting and re-entering the telehealth portal). Similar to previous literature, this indicates that technical issues had no discernible adverse influence on completion of the exercise video consultations. 27 These findings are also comparable to a recent descriptive study of physiotherapy telerehabilitation consultations from an Australian randomised controlled trial, where technical issues were shown to have limited impact on clinical sessions. 11 Specifically, most technical issues identified were audio/visual in nature, transient and caused no significant increase in total consultation time, although more time was dedicated to technical setup for video consultations compared to in-person sessions. 11 It was also observed that a higher number of technical issues were experienced in initial consultations via videoconferencing compared to final consultations (37% vs. 19% respectively), suggesting that experience using telehealth may predict better technical outcomes. 11 Combined with the results of the current study, this seems to suggest that presence of technical issues during videoconferencing may not be as influential as once thought by clinicians. 9 While clinician confidence in telehealth can be influenced by multiple factors (e.g., telehealth-specific training received, perceived effectiveness compared to in-person care),28,29 the current study suggests that beliefs regarding adverse impact on exercise performance may not be warranted.
Around half of the video consultations in this study did not reach prescribed exercise intensity targets. This was primarily due to factors such as participant fatigue and/or pain experienced resulting in longer rest periods, and the prescribed duration at intensity levels not being possible due to time constraints of the exercise sessions themselves, and not technical issues. The participants in this study often presented with multimorbidity, significant polypharmacy and profound clinical complexity(e.g., musculoskeletal impairment, muscle pain and profound fatigue). 14 These factors are well-known barriers that could constrain ability to achieve prescribed exercise intensity for people living with metabolic multimorbidity, particularly if starting from a low level of exercise tolerance. 14 30–33 While a similar study in a population group with a comparable metabolic profile was able to achieve high intensity heart rate targets with in-person supervision, 34 the current study indicates challenges for exercise intensity with video consultation exercise supervision (other than technical issues). In contrast to the current study results, a recent RCT demonstrated that most exercise video consultations reached prescribed intensity markers for aerobic training in people with chronic obstructive pulmonary disease despite breathlessness symptoms. 35 However, in the current study participants had profound metabolic and musculoskeletal multimorbidity compared to this previous cohort, which may in part explain reasons of pain and fatigue limiting prescribed exercise intensity attainment.14,35
The findings of this study support the promotion and use of video consultations as a delivery modality for exercise service. However, for video consultation services to be optimised and sustainable for exercise delivery, certain requirements must be met. This includes the development of a skilled workforce competent in both the delivery and administrative requirements (including troubleshooting technical issues) of service delivery via videoconferencing. 36 For the exercise professional, this may include: (a) undertaking a formal needs assessment to identify whether a telehealth service is appropriate and feasible considering individual patient factors (e.g., clinical complexity, access to technology), 37 (b) selecting a video consultation mode of delivery appropriate for participant digital literacy, preferences and goals, 38 (c) undertake appropriate telehealth-specific training for facilitating exercise video consultations, and conduct sessions in line with professional recommendations and standards 16 39–41 to minimise impact of technical issues on the clinical session and (d) selection of exercise assessments and prescription easily accessible, adaptable and deliverable in video consultations.
Study limitations and future work
This study has several important limitations to consider. This study was nested in a larger randomised controlled trial conducted in a large metropolitan hospital using a state government managed video consultation portal and may not reflect ‘real-world’ practice for many exercise professionals operating in small private practices with privately purchased digital health tools (e.g., Zoom, Microsoft Teams). Real-world professional practice has unique challenges to the implementation of telehealth services that are not typically present in highly controlled research environments (e.g., financial stress of private practice clinicians). 42 In the current study, AEPs facilitating exercise video consultations underwent telehealth-specific training prior to involvement, which may not reflect general professional practice. Therefore, the findings of this study may not be generalizable across different working contexts. While the number of consultations included in this audit was high (n = 270), the data were based off a small subset of participants from the U-DECIDE RCT (n = 21). The overall proportion of technical issues and intensity-limiting factors may have been different in a larger sample, with less potential for individual participant data points to influence findings. Participant attendance to exercise video consultation was lower than anticipated in U-DECIDE (not due to video consultation technical issues), which limited the data available. It may be that more technical issues would have been identified with a larger sample of sessions. In turn, this may have demonstrated different effects of the impact of technical issues on exercise intensity in the current study. Additionally, technical issues identified in this study were recorded as observed by the AEP, and not necessarily those experienced by the participant. Due to sessions being group-based and only one AEP being present to facilitate exercise and record potential issues, the duration of individual technical issues in the session was not recorded. This would provide further descriptive information regarding the potential impact of technical issues on exercise prescription. This is especially important given that prescribed duration at intensity levels was often not possible due to time constraints in exercise video consultations was a common reason recorded by the AEP for participants not meeting prescribed exercise intensity. Non-English-speaking participants were excluded from U-DECIDE. Therefore, these findings may not be generalisable for people with limited English proficiency.
Conclusions
This study observed that technical issues during exercise video consultations were relatively infrequent and did not seem to noticeably affect aerobic or resistance training intensity. Technical issues were typically minor and quick to resolve, often with no troubleshooting required. However, results demonstrated that many consultations did not reach the target exercise intensity, which may reflect other constraints such as participant metabolic co-morbidities and pain and fatigue experienced during video consultations. These findings may help to alleviate AEP concern about the use of videoconferencing for exercise practice and provide a direction for future research to examine other factors to enable clients to achieve exercise intensity targets during exercise video consultations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251410986 - Supplemental material for Technical issues in exercise video consultations do not negatively impact exercise intensity for participants with complex chronic conditions: a retrospective audit
Supplemental material, sj-docx-1-dhj-10.1177_20552076251410986 for Technical issues in exercise video consultations do not negatively impact exercise intensity for participants with complex chronic conditions: a retrospective audit by Riley C.C. Brown, Megan H. Ross, Jeff S. Coombes, Ingrid J. Hickman, Nicola W. Burton, Jaimon T. Kelly, Trevor G. Russell and Shelley E. Keating in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251410986 - Supplemental material for Technical issues in exercise video consultations do not negatively impact exercise intensity for participants with complex chronic conditions: a retrospective audit
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251410986 for Technical issues in exercise video consultations do not negatively impact exercise intensity for participants with complex chronic conditions: a retrospective audit by Riley C.C. Brown, Megan H. Ross, Jeff S. Coombes, Ingrid J. Hickman, Nicola W. Burton, Jaimon T. Kelly, Trevor G. Russell and Shelley E. Keating in DIGITAL HEALTH
Footnotes
Acknowledgements
The study authors would like to thank the participants of the exercise video consultations. Specifically, the authors would like to thank Chloe Salisbury and Ivana Steyn for their efforts with video consultation facilitation. JTK was supported by a Postdoctoral Fellowship (106081) from the National Heart Foundation of Australia.
Ethical considerations
The U-DECIDE RCT was approved by the Metro South Hospital and Health Service's Human Research Ethics Committee (HREC/2019/QMS/58285) and the University of Queensland Human Research Ethics Committee (2020000127).
Consent to participate
All participants provided written informed consent prior to enrolment.
Author contributions
RCCB, MHR and SEK contributed to study conception. All authors contributed to study design. RCCB conducted the data audit. RCCB, MHR and SEK contributed to data analysis. All authors contributed to data interpretation. RCCB was the principal writer of the manuscript. All authors contributed to manuscript writing and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Metro South Research Support Scheme 2020–21, Queensland Health Practitioner Grant 2019–20 (grant number N/A).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.