
Abstract
Objectives
To explore the perspectives of people with osteoarthritis (OA) on the use of digital technology into their rehabilitation program, including their awareness, views on accessibility, affordability and willingness to accept digital modalities for rehabilitation delivery.
Methods
A qualitative, descriptive design was conducted. Patients with OA who receive care at a public community rehabilitation centre in the Western Cape, South Africa were eligible to participants. Semi-structured interviewed were conducted and Atlas.ti 23 software was used for thematic analysis.
Results
The findings showed that the participants had limited awareness and exposure to telerehabilitation (TR), along with minimal digital literacy and skills. They were sceptical about the effectiveness of TR and concerned about the inherent lack of physical interactions with health professionals. However, some acknowledged TR's potential benefits for accessibility, convenience, family involvement and long-term community health improvement. Participants were willing to learn more about TR.
Conclusion
Considering the benefits of TR in lower resource settings such as South Africa, investment to increase awareness and patient education and training in TR may assist in enhancing access and quality of care. Resources dedicated to TR and management buy-in in low-and-middle income countries (LMICs) is necessary to facilitate the fit-for-context roll-out of TR.
Introduction
Accessing rehabilitation services globally is challenging. Rehabilitation is associated with high cost of care for the patient and health system. Therefore, factors such as transportation barriers, and lack of accessible facilities, especially in low-and-middle income countries (LMICs) with limited resources bar access to rehabilitation. 1 Rehabilitation can optimise functioning and reduce disability in people with functioning problems due to disease, injury or congenital disorders. 2 Around 15% of the global population has a disability, with 80% residing in LMICs with particularly limited access to rehabilitation services3,4 leaving a significant unmet need.
Preliminary evidence shows that telerehabilitation (TR) presents a promising approach to expand access to rehabilitation services in LMICs. 1 In LMICs rehabilitation at primary care as well as rural and remote regions is especially limited.2–4 A key advantage of TR is the possibility to extend expertise to areas or levels of care where rehabilitation is lacking. 5 The use of TR can also empower communities, empowering community-based disability support.6,7
The potential benefits of TR illuminated during the COVID-19 pandemic when rehabilitation services were severely impacted as resources and facilities were diverted to critical care needs at tertiary levels of care, rendering primary level care even more precarious. 8 Due to limitations, rehabilitation professionals required new methods to communicate with their patients, particularly those with chronic musculoskeletal conditions that require ongoing care. Common rhematic and musculoskeletal presentations were left with no rehabilitation in most regions in SA during the pandemic. 9 Osteoarthritis (OA), one of the most common chronic musculoskeletal diseases necessitating ongoing rehabilitative care at the primary care level, 10 serves as an important example of this issue. The management includes a comprehensive approach that combines manual therapy, patient education, exercise and psychological support in primary care settings.11–13 This can significantly improve the management of OA and positively impact the lives of those affected by this chronic musculoskeletal condition.11–13 Consequently, many of these patients experienced worsening pain levels and mobility, decreased physical activity, and overall declines in health and functioning with the rehabilitation limitations. 9 However, limitations imposed on in-person services during the pandemic accelerated the adoption of TR platforms by rehabilitation providers for the prevalent patient presentations.14,15
In South Africa, providing TR for OA remains crucial as many patients lack access to quality rehabilitative care due to geographic barriers and provider shortages, especially in rural areas. 16 TR could potentially help address these access gaps by connecting underserved communities remotely. 16 Additionally, a review done by Nagel et al. 17 on various musculoskeletal conditions has also shown that digital exercises have a positive impact on pain, function and quality of life. While TR holds promise for boosting healthcare access in resource-limited settings, there are barriers like lack of infrastructure, internet connectivity, required training, provider knowledge and funds to roll out TR.18,19 Additionally, there is a shortage of rehabilitation professionals adequately trained in TR modalities as it is not included in undergraduate currculae. 20 Individual-level barriers like low technical literacy, digital skills or awareness/acceptance of technology use in health care can also deter adoption among patients. 4
Perspectives on integrating technology into healthcare are varied. Many studies, predominantly from high-income regions, reveal some patient scepticism towards technological rehabilitation methods.21,22 This hesitation often stems from limited familiarity and understanding of tech-based rehabilitation.21,23 Concerns also arise over reduced effectiveness due to diminished personal interaction. 24 In contrast, scepticism in lower-income areas is primarily about data accessibility and costs. 25 For technology to be effectively adopted in rehabilitation, comprehending user perspectives is essential to foster acceptance.
Therefore, this study aimed to explore perceptions of TR use among primary care patients in South Africa to guide implementation and optimisation. Although, the recent study that assessed the organisations and health professionals’ readiness to integrate TR into service delivery reported that TR is feasible for expanding access, 19 there is minimal research on user readiness to accept these platforms in the South African context. 26 Patient feedback can inform larger implementation decisions and necessary training to support adoption across diverse patient populations and public health settings. Therefore, this study aims to explore the perspectives of patients with OA on the use of digital technology as part of their rehabilitation at a public community healthcare centre with specific focus on awareness, views on accessibility/affordability and willingness to engage in TR and describe the sample with respect to their functioning status, quality-of-life and self-efficacy.
Methodology
Study design
A qualitative descriptive design with an interpretive approach was used to explore patients’ awareness and willingness to use digital technology in rehabilitation at a South African primary care facility. This approach, suited to situations with limited existing knowledge, 27 aimed to understand patients’ perspectives on accessibility and experiences with complex factors influencing their healthcare. 28
Study setting
The study took place at the Bishop Lavis Community Healthcare Centre (CHC) in Cape Town, South Africa. This community faces high unemployment and limited internet access (69.6% of households), potentially impacting telehealth adoption.29,30 The CHC offers various medical and rehabilitation services, making it a relevant setting for exploring telehealth's potential within this population.
Researcher characteristics
All interviews were conducted by the lead author, who is a qualified female physiotherapist. The researcher has three years of clinical experience as a physiotherapist in treating a variety of conditions (neurological, NMS, cardiopulmonary), ranging from acute to chronic, in the primary to tertiary healthcare settings. The researcher has never worked at BL CHC and the participants have not received any physiotherapy treatment from the researcher. The participants from this facility had no prior contact or relationship with the researcher. The occupation of the researcher was shared with the participant and they were informed that the researcher was conducting this research in pursuit of a postgraduate degree. The researcher is fluent in the participants’ home language which was mainly Afrikaans and used it for conducting the interviews.
The researcher received guidance from her supervisor and co-supervisor, who possess considerable expertise in qualitative research methods. All of the supervisors have extensive backgrounds in carrying out, analysing, reporting, and publishing qualitative research studies, having been involved in more than 15 studies and publications. Additionally, they have supervised numerous master's and doctoral students.
Sample
All adults on the waiting list for rehabilitation services were eligible to participate if they were referred by the medical officer and/or professional nurse for confirmed or suspected OA of all joints. Inclusion criteria: Adults diagnosed with OA, regardless of the presence of other concurrent medical conditions, such as diabetes or tuberculosis. To ensure effective participation, the study required participants to be able to communicate independently and complete questionnaires with or without minimal assistance. Exclusion criteria: Individuals with significant verbal or auditory impairments that hindered their ability to engage in the interview were excluded from the study. Participants were recruited using convenience sampling 31 from the OA waiting list patients at the Bishop Lavis Rehabilitation Centre (BLRC) (rehabilitation unit of the BL CHC). Additional participants were recruited from newly referred patients during the data collection time period. Stratified randomised sampling 32 was originally intended but proved unfeasible as the majority (90%) of waiting list patients were uncontactable. For the initial exploration of a relatively under-researched topic within a specific community, ten participants were considered a sufficient sample size. 33 The data collected from these participants allowed the main research objectives to be satisfactorily addressed, achieving data saturation. 34 Data saturation was met with the minimum requirement of 10 participants. However, if data saturation had not been met after the initial data collection and analysis, the research plan was to recruit additional participants for further interviews.
Data collection procedures
Following ethical approval, the principal researcher consulted with BLRC management to secure logistical support for conducting on-site interviews in terms of scheduling and facilities. A BLRC volunteer contacted the waiting list patients telephonically to provide a brief introduction about the study and researcher. The researcher followed up with the potential participants to explain the study purpose and procedures in further detail and schedule interviews if the individual was willing to enrol. All participants received remuneration for their time to acknowledge the potential inconvenience.
Data collection instruments
Five instruments were used to gather data on functioning, self-efficacy and quality of life. A sociodemographic questionnaire collected information on age, gender, OA diagnosis date, employment, comorbidities and medications. The Patient Specific Functional Scale (PSFS) quantified activity limitations. 35 The individual self-reports three to five functional activities that they have difficulty completing or are unable to complete. The activities are rated on an 11-point score, where 0 being unable to complete the activity and 10 being able to complete the activity without difficulty. 36 Arthritis Self-efficacy Scale – 8 item (ASES-8) is a self-reporting questionnaire which measures a patient's belief in their confidence when managing the pain and symptoms of arthritis. 37 It consists of eight questions covering pain, other symptoms and physical function. 38 Each question is scored on a numeric rating scale ranging from one to ten. One being the patient is being very uncertain, five to six being moderately uncertain and ten being very certain. 39 The EuroQol EQ-5D-5L is a self-rated health-related quality of life (HRQoL) questionnaire that comprises of five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 40 Each domain consists of five levels: no problems (1), slight problems (2), moderate problems (3), severe problems (4) and extreme problems (5). The individual must indicate the most appropriate statement for their condition. 40 The literature did not provide any information about using public domain resources in the items or scoring methods of the instrument. This lack of transparency regarding the PSFS and ASES-8 development reduced its validity within the specific context of this study. The EuroQol Group was contacted to obtain permission to use the EuroQol 5D5L for research purposes. The PSFS,41–43 ASES-844–46 and EuroQol 5D5L47,48 have not been validated in the South African Context but has been used in various other arthritis, rheumatic and musculoskeletal populations.
A semi-structured interview guide explored perspectives on using digital technology during OA rehabilitation. The interview schedule was developed in English and was informed by the research objective and previous information found in similar published literature.1,49–54 All data collection tools were tested in two pilot interviews. All interviews were held at the BL CHC and were conducted in a private, locked room. Non-participants were not allowed in the room during the interviews. No data contained any personal information and was coded to ensure privacy. A pilot study was conducted with two participants before the main interviews were held. Following the two pilot interviews, no changes were needed to any procedures for the main interviews. Instruments were translated into Afrikaans and isiXhosa. Written informed consent was obtained at the beginning of each 45-minute interview session. Interviews were conducted in the participant's preferred language of English, Afrikaans or isiXhosa. Sessions were audio recorded and supplemented with observational notes by the interviewer. The interviewer-built rapport by providing a brief presentation that explained the study purpose and procedures. Data collection instruments were completed before interviews were conducted. Member checking occurred throughout interviews to verify understanding of responses. The interviewer would repeat statements back to participants and confirm the intended meaning was accurately captured. This enhanced authenticity of perspectives in transcripts and supported data collection rigour. No repeat interviews were needed.
Data processing and analysis
An external transcription company transcribed and translated the anonymous data. The translation was validated by the researchers (GP, QL and DE) during the coding process to ensure accurate meaning reflection. Quantitative data from the sociodemographic questionnaire, PSFS, ASES-8 and EuroQol EQ-5D-5L was analysed using descriptive statistics like means, standard deviations, medians and interquartile ranges depending on normality. Qualitative data underwent thematic analysis based on Braun and Clarke's 6-step approach 55 to identify, analyse and report themes and patterns. The qualitative data was coded using the ATLAS.ti (version 22.2) coding software. Inductive coding was performed to allow relevant codes to emerge directly from the data itself. These codes were examined to derive a conceptual framework for drawing conclusions. Two independent reviewers (QL and DE) verified codes and modified the framework through collaborative discussions. Code names were reviewed by the same reviewers for adequate brief descriptions. The researcher (GP) created a narrative explaining how each code provided unique insights into the research questions. Codes were analysed to identify common themes representing participant perceptions as subthemes. Themes and data extracts were reviewed by the researcher and two independent reviewers to confirm appropriate theme identification and fit. An audit trail documenting the analysis supported interpretation trustworthiness. The final report included descriptive narratives and representative quotes illustrating the identified themes and subthemes. No feedback was obtained from participants as member checking was done during the interview for clarity.
Ethics
This study received ethical approval in February 2023 from the Stellenbosch University Health Research Ethics Committee (Ref no. S22/11/253) and the Western Cape Government Department of Health (Ref WC_202301_026). The authors confirm that all study procedures adhered to relevant national and institutional ethical standards, as well as the Helsinki Declaration of 1975 (revised in 2013).
Results
Demographic information of the participants
Table 1 provides an outline of the sociodemographic information of the participants. Ten participants were recruited and participated in the study over a period of 2 months. The participants were mostly female and Afrikaans speaking. Most participants (9%) were not employed at the time of the study, of which 4% are pensioners.
Summary of participant characteristics.

The information obtained from the three data collection tools that assessed participants’ function, self-efficacy and quality of life are reported narratively below.
The PSFS gauged activity limitations across categories such as personal hygiene, domestic chores, transfers, and mobility. On average, participants scored 3/10 for personal hygiene and domestic chores, indicating moderate limitations, while scoring slightly higher at 4.8/10 for transfers and 4.4/10 for mobility. The ASES – 8 aimed to capture participants’ perceptions of their OA symptoms, with lower scores reflecting lower levels of self-efficacy. In this study, participants achieved an overall mean score of 33.3, suggesting a generally low level of self-efficacy in managing their OA symptoms. For assessing quality of life, the EuroQol EQ-5D-5L was utilised. Results indicated that participants reported the highest scores in mobility, self-care, usual activities and depression categories, with mean scores ranging from 1.9 to 2.5. Pain emerged as the lowest scoring category, with a mean score of 3.00, indicating significant discomfort and impact on daily life. Overall, these measures collectively paint a comprehensive picture of the challenges individuals with OA face in various aspects of their lives, including physical functioning, self-efficacy in managing symptoms, and overall quality of life.
Themes and subthemes identified from interviews
The quotations from interviews were used to convey the perceptions and feelings of the study participants. The quotations were labelled using the participant number, age and gender (e.g. P1, Female, 49). Figure 1 provides an overview of the main themes and subthemes of the results of the study.
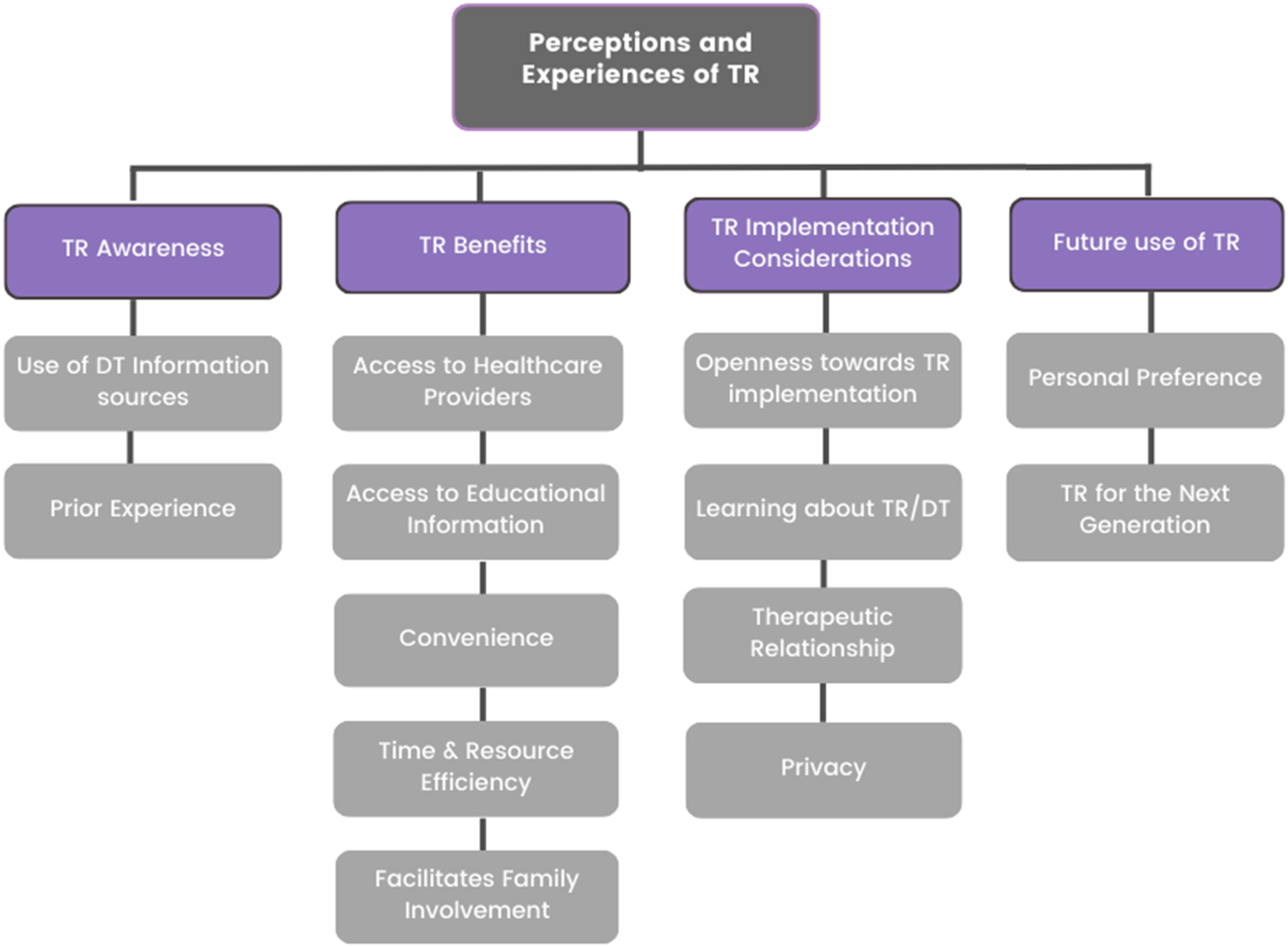
Main themes and subthemes of study. TR: telerehabilitation; DT: digital technology.
Theme 1: telerehabilitation awareness
TR awareness involves knowledge of digital technology options as well as experience using these options. The subtheme ‘use of digital health information’ relates to seeking and engaging with online content, reflecting general digital literacy and openness to technology-based methods such as TR. The second subtheme, ‘knowledge, skills and experience with TR’, evaluates familiarity and competency applying telehealth tools in rehabilitation.
Use of digital technology information resources
Participants had varying knowledge of digital information resources for their health conditions. Most had minimal experience using online sources like search engines or social media videos. Instead, they primarily learned about their conditions through peer sharing.
‘… I’ve never looked at that… because I’ve … gone to look, but I’ve never Googled it because I'm still in denial myself’. P1, Female, 49
‘Not actually. We just talked among ourselves and so on about arthritis, so on, because I am a diabetic, I understand why I also got arthritis, because it is also part of diabetes and so on’. P2, Female, 53
Participants’ responses also reflected that their limited digital health literacy could be due to their preference for more traditional methods of learning about their condition. These quotes are relevant as it is indicative of their digital skills and literacy
‘It's not that I don’t want to use the phone, but it's better to see it on paper, read it and then do it. I'm still an old person’. P8, Female, 67
‘Because I tried to do it (stating the participant has used YouTube before for assistance with arthritis)’. P10, Male, 58
Knowledge, skills and experience of telerehabilitation
Only one participant had previous TR experience which was received at a private hospital in the Cape Metropole area. This participant provided a positive experience in receiving TR, especially due to not having to travel to the health care centre. The potential of TR in providing guidance and exercise prescription was also highlighted by the participant. It showed how much value the participant placed on the continuous guidance and feedback within their TR sessions. ‘It was a video … on the phone, video, then once she talked to me and she said what must I do, and I don’t need to go in, you see’. P10, Male, 58
‘Then I do it, then because when you go back or when she video call you, she can check how are you. She will say, put your arm at the back, she will see how far your arm will go and she will tell you, you didn’t … you didn’t do the exercise what I told you to do, you understand. So, you must put again, you must do it’. P10, Male, 58
In contrast, the majority (1–9) of the participants have not had any TR experience before or were aware that technology can be implemented as a method of providing rehabilitation. Most participants expressed their lack of knowledge and awareness of TR. ‘I don’t know, man, I don’t have knowledge about this’. P7, Female, 61
Theme 2: telerehabilitation benefits
TR benefits refer to the potential advantages of using TR services as perceived by patients. The subthemes relate to different types of benefits experienced by the participants: Access to healthcare providers describes the ability through TR to remotely connect with rehabilitation staff or any health professional. Access to educational information refers to the accessibility of online resources, self-management tools and instructions through digital platforms. Convenience includes benefits such as receiving services from home and flexible scheduling made possible by TR. Time and resource efficiency relates to reduced travel time/costs and optimisation of clinical resources facilitated by TR delivery methods. Facilitation of family involvement describes how TR could allow family members to participate in and support patients in the rehabilitation process remotely.
Access to health care providers
Participants recognised the direct and immediate communication that TR provides, bypassing the need for intermediaries such as other health professionals. TR was seen as improving accessibility due to the possibility of it removing any intermediaries for booking rehabilitation appointments. The participants were keen to have direct access to the therapist during their rehabilitation journey.
‘It will be fast because then you send her a message, straight to her, then you don’t come via a sister or a doctor, speak to her’. P10, Male, 58
‘Like I said now, you react faster to a call where, if you’re here, like for instance, if you’re here you have to go through this chain or that then, just to get to that person’. P4, Female, 49
Access to educational information
One participant mentioned the potential benefits of early exposure to information and resources through TR. By providing education and guidance remotely, the participant felt that TR could empower them to better manage their conditions. The accessibility to information was seen as particularly valuable for individuals who may have limited access due to restricted mobility or who reside in remote areas. ‘I mean, for myself with this … I wouldn’t call it a disease, but this illness, would I say it, not being able … I think if I would have known way before what I can use or … I wouldn’t been at this phase already. Maybe I would have been exposed to ways to make it easier, like now. How to sleep easier, what to eat, how to sit and all of those things. Maybe … I know it could have been maybe different’. P4, Female, 49
Convenience
Some participants emphasised the convenience of using technology, particularly video calls, for accessing rehabilitation services. TR was seen as being beneficial due to the discomfort of travelling to the facility. Participants felt that TR can provide a solution for people who are unwell and unable to travel, ensuring that they still have access to the necessary rehabilitation care and support. ‘Yes, it would be, because with me being uncomfortable half of the day, walking and to walk … getting here, having it there at home would be better than coming here to the clinic and having it here’. P4, Female, 49
‘… The persons will not be able to go because they are not feeling well today’. P8, Female, 67
Time and resource efficiency
Participants thought that TR could overcome the barriers of time constraints when they need healthcare. TR was thought to be potentially more flexible and time-efficient option for receiving healthcare services, eliminating the need for travel and reducing time constraints. However, participants noted to gain access to the benefits of TR, one would need access to a mobile phone. ‘There is not always the time to come here’. P6, Female, 56
‘Okay, number one, they don’t have to come in, they don’t have to spend money to get to the facility. The video call, depending on the time when it will be done, because there are other things that you have to do at home and so on. So, it will actually help a little, yes. If you also have access to a mobile phone’. P2, Female, 53
Facilitate family involvement
The findings suggest that TR may facilitate engagement with family members to support patients who have limited ability to travel to the healthcare facility. These findings also suggest that the older population have the confidence in the younger population to assist them with their technology use. ‘As I say now, if I say yes now then I just have to ask my children’. P7, Female, 61
‘Yes, I’m sure they will be able to do it because these phones from like … as I tell you, many can’t get here. Because many have leg problems and such. It's a lot … and there's a lot of bedridden … where they can get it on the phone and then the kids can show it to them and the grandkids … we can do that now, grandma, or we can do that now, and there are many old people who sit with those problems. But they can’t get here. So, the phone would be the best option because then the children can look it up for the grandmother, or the child can look it up for the mother, then they can see it, but that's what we can do for grandma now. See grandma, so’. P6, Female, 56
‘I don’t have that much experience, as I said, then I would always ask the children, or their children … the grandchildren. I say listen here, look, I want to get into the thing now, help me’. P6, Female, 56
Theme 3: telerehabilitation implementation considerations
TR implementation considerations relates to factors that shape willingness and readiness to adopt TR services. The subtheme ‘Openness towards TR Implementation’ reflects patients’ receptivity and interest in using remote rehabilitation methods. Learning about TR discusses the necessary needs around education and training to build knowledge and skills for effective TR use. The therapeutic relationship covers the perspectives on the ability to develop quality patient-provider connections through the various online and in-person service methods. Privacy during TR involves concerns around secure data handling and confidentiality when using technology platforms.
Openness towards telerehabilitation implementation
Mixed views were communicated on the future of TR, with some optimistic about its’ potential to improve access and efficiency, while others preferred the face-to-face interaction of traditional rehabilitation. Most participants showed an openness to this rehabilitation approach. Participants noted that TR will be a learning curve for them, and it will take some adjustment when implementing a system like TR in their context. ‘It will take some time because we are all not aware of it’. P6, Female, 56
‘Yes, in the beginning it might … it might take time to get the system as expected now’. P8, Female, 67
‘I think it will be the same. No, not really the same, it would be better, I think’. P8, Female, 67
Some participants expressed their reluctance for TR as they did not think that rehabilitation service received would be of the same quality and effectiveness as in-person sessions. ‘No, for me it won’t be the same. That's why I would prefer to come here’. P7, Female, 61
‘I think face to face will be better’. P10, Male, 58
Learning about telerehabilitation
Participants indicated that they would be open to using TR if they received the necessary support and instruction prior to accessing the service. This suggests that their hesitance is primarily due to a lack of familiarity with or knowledge about the technical aspects of TR. ‘If somebody shows me how to do it’. P4, Female, 49
‘If you don’t know how to use it, it will be a challenge. Like I was a bit stupid, but I trained myself how to use it’. P10, Male, 58 (Previous TR experience)
‘Then I have to help myself … Yes, I will surely learn’. P8, Female, 67
While one participant had a positive TR experience, others conveyed strong disinterest in the technical aspects, preferring the traditional in-person approach. Their lack of interest or comfort with technology suggests challenges related to digital skills, confidence, or familiarity. This response from some participants indicates not all may be immediately receptive to TR. ‘No man, I’m not interested in this technical stuff. Really’. P7, Female, 61
‘I’m not into apps …’ P4, Female, 49
The therapeutic relationship
Participants highlighted that therapeutic relationships are important, whether using TR or in-person format. The one participant who had prior TR experience highlighted that the personal connection he formed with the therapist was important to the success of his TR experience. ‘… like I did it before, with my shoulder, I was in a car accident last year, August, and after the operation they sent me to a physio … then a few sessions I was there, like three or four, then I … we know each other … then afterwards she video called. … And then it worked lekker. Because I know her mos now…’ P10, Male, 58
For some participants, it was important to have eye contact or to have personal contact with the therapists. The participants felt that telephonic or computer-based interactions could create an impersonal atmosphere which would hamper explanations or understanding. This highlighted their personal preference for in-person rehabilitation due to the perceived benefits of in-person communication. ‘To see eye to eye… this is very important to me. Eye to eye’. P2, Female, 53
‘It's first time being exposed to something like this, because I’m old-fashioned, one on one is always better because then you can see the person, they can explain it to you more in detail than on … telephonically or a computer … it feels so impersonal. How do I say it?’ P4, Female, 49
Privacy during telerehabilitation
Participants recognised the need to balance privacy with family support when using TR. They stressed advance preparation, such as informing others or leaving notes when unavailable, to maintain privacy and avoid interruptions during TR sessions. ‘so my children know they shouldn’t just walk in, or they have to [indistinct 0:17:19.6] okay, if they see I’m on the phone, say okay, then they’ll go out first. So, yes, we have that privacy that no one will be there and sit and eaves drop or whatever’. P8, Female, 67
‘That is where the preparation comes in. Because if you make preparation and you know there's people that make a nuisance of themselves and so on, you tell them, or put a note on your door, I am not here, but you are there’. P5, Male, 66
Other participants had a different view as they preferred open communication and transparency regarding their health status. They believed that open communication with their family would allow them to receive the necessary support and assistance from family and health care practitioners. ‘No, I have… when it comes to my health, everyone should know. So, if I overcome anything, then they only know that … I’m not there hiding my health, everyone knows, it's my ailment and where they can help me, there they help me’. P6, Female, 56
Theme 4: future use of telerehabilitation
Future use of TR explores patients’ perspectives on continued adoption and potential scale-up of TR services in the future. The subtheme ‘Personal preference’ describes the individual receptivity and intention to use of TR options for one's own rehabilitation needs. TR for the next generation considers the attitudes towards promoting TR for broader community access, especially among the younger demographics adapting to the advances of technology in healthcare.
Personal preference
Participants preferred in-person rehabilitation over TR for their personal treatment. They valued the familiarity and personal interaction of in-person sessions. While acknowledging TR's potential benefits for those with physical limitations, participants felt uncomfortable using it themselves and believed it may not be suitable or accessible for everyone. ‘That's me now. That's mine now. As I say now, sorry for those who can’t walk now, sorry now for those who can’t use the phone… because, the phone is also a bit difficult man. Understand? And I would prefer to come here’. P1, Female, 49
‘Let me tell you what, it's not going to happen now… So, I won’t be able to say yes or no, because my option is, I won’t take it’. P7, Female, 49
Other participants again expressed their willingness to try TR for accessing services despite any reservations or uncertainties felt. ‘I will try it out. I will try it out because I’ve got nothing to lose’. P5, Male, 66
‘Yeah, I will try it out. I’m open for situations’. P4, Female, 49
Telerehabilitation for the next generation
Participants expressed that they think the implementation or TR would be beneficial for their community since they recognised that advancements in technology can lead to positive changes for the community's rehabilitation services. They were aware of the needs and skills of the future generation to access and use TR. ‘… I wouldn't think it's bad for our people’. P1, Female, 49
‘And … but either or, I will say, because of the new generation and the new things that comes out, it will definitely benefit, yes…’ P5, Male, 66
Discussion
This study is the first to explore the perspectives of OA patients on technology use in rehabilitation in South Africa. OA prevalence in South Africa is as high as 83% in rural areas and about 55% in urban settings. 36 The study specifically explored the use of technology to deliver rehabilitation for OA management in a SA primary care setting. OA was used as it is a common chronic musculoskeletal condition seen in South Africa and this will allow the findings to be applicable to the broader population with chronic musculoskeletal conditions in this context. Our findings suggest that individuals with OA presenting at primary care in South Africa are not aware of TR and strategies will be needed to facilitate adoption of TR as a rehabilitation service mode. Add OA/TR
The lack of awareness of TR among our participants may be attributable to several factors. South Africa's past legislative restrictions as transcribed by the national health regulatory council hindered the use of TR in South Africa.56,57 Consequently, health care providers and patients were never or rarely exposed to TR as a service delivery method.57,58 However, during the COVID-19 pandemic, the local regulatory restrictions were eased to facilitate access to healthcare using remote or electronic methods as a relatively safe mode compared to face-to-face consultations. 59 During the pandemic, rehabilitation professionals also benefitted from the opportunity to use TR. 60 However, many of the TR opportunities were limited. 61 to the private sector clients whilst our study was conducted in the public sector. Therefore, governance related factors influenced awareness of TR among our participants.
Factors related to digital literacy may also explain the lack of awareness and willingness to engage in TR. We found that all (except one) of participants did not consider smartphones as an avenue to gain health information sources. Mobile phones are seen as assistive technology (AT), defined as ‘assistive products that contain electronic information and communication’. 62 Participants also expressed unease about altering their familiar face-to-face rehabilitation service mode. As OA is a chronic musculoskeletal condition that requires continuous maintenance, 10 these participants have become used to the norm of in-person rehabilitation. The findings underscore the necessity to raise awareness among patients, especially older individuals and chronic musculoskeletal condition users, to improve digital literacy and promote equitable care.
In our study, participants’ literacy was limited to telephone calls and the knowledge and skills to search for health information on the internet was not evident. The poor digital health literacy skills are potentially also linked to a lack of confidence in using technology. This finding may be linked to the published evidence on a passive attitude towards healthcare among South Africans using the public health care sector. 63 Similarly, as our study participants viewed health care professionals as the primary source of health information, another study conducted on PHC patients in South Africa showed that the patients looked at the health care provider to decide on providing health information or how their treatment will be conducted. 63 Investing in digital literacy is needed for improving the accessibility to health facilities and empowering patients to access health information, although users in the public sector will also need strategies to assist them in using technology confidently. Engaging with digital sources can be a cost-effective way to promote health, provide access to reliable information, and facilitate information exchanges between patients and healthcare providers. 64 These strategies could improve functionality in daily life, independence, and societal participation. Moreover, it could lead to significant health cost savings, which is particularly crucial in South Africa, where healthcare resources are limited. This stands in stark contrast to the participants’ strong dislike for complexity.
Our findings also showed mixed views among OA participants on the acceptance of TR as a service delivery mode. The study was conducted in a lower-resource community setting, which may explain why some participants were not keen to accept TR. A previous study found that wealth disparities among communities, leading to a wider range of educational profiles, can influence acceptance rates of TR. 65 Additionally, in a study conducted by Kessel et al. 66 revealed that various factors, such as age, gender, socioeconomic status, health status, and urban versus rural home environments, can influence patients’ digital health literacy. 67 In both HICs and LMICs, digital literacy has become increasingly crucial for active participation in modern society.68,69 The lack of digital literacy and exposure to technology in such settings could contribute to hesitancy or resistance towards adopting TR as part of their healthcare. However, openness towards learning and training expressed by our participants were positive. In a study done by Intan and Irma 70 also showed that acceptance rates may increase with strategies addressing barriers such as limited funding for the required devices and TR software needed, underdeveloped policies, poor data security measures, inadequate infrastructure, limited availability of TR facilities, and staff shortages in health facilities70,71 Appropriate and context specific strategies are indicated to positively influence acceptance of TR so that users of the public sector can benefit from TR, which has been shown in be effective in increasing access and outcomes in many conditions. 72
We found that patients did not perceive TR as an effective way to receive rehabilitation. A study conducted among the general public of Brazil also showed that patients have concerns about lacking hands-on treatment with TR. 24 Similarly, a Swedish study reported building rapport and trust can facilitate the outcomes of TR 73 positively. The effect of TR has been shown to be equally effective as using the traditional face-to-face in patients with OA 74 in which outcomes such as pain, function, self-efficacy improved. The participants in our study reported high levels of pain and low self-efficacy which affected their daily functioning or ADLs. Implementing TR could enhance their quality of life by offering better access to healthcare providers when support and guidance on symptom relief are needed. TR presents an opportunity for therapists at well-resourced healthcare facilities to provide remote support and services to understaffed, resource-constrained, or geographically isolated facilities, thereby enhancing access to rehabilitation care.
Multi-faceted strategies are needed to raise awareness among patients and providers. 70 Unless barriers are addressed by providers, senior management and policymakers, exposure likely won’t change. Effective adoption requires a thoughtful approach to drive organisational change. South African healthcare organisations aiming to integrate TR should advocate for funding to invest in technology, IT support and operating costs for long-term sustainability. 70 Training health professionals is equally critical to foster buy-in and develop quality TR service competencies rather than directives. 70 A collaborative, holistic process engaging leadership and staff is key to meaningful culture change that expands equitable access through TR.
Limitations
The sampling method had to be changed from probability sampling to convenience sampling during data collection due to participants being uncontactable. The original participants were recruited from the physiotherapy OA waiting list. Only 3.6% of the waiting list of 60 were contactable. The rest of the participants were recruited from patients that arrived with new referrals during the data collection time period.
The study only included one condition (OA) and PHC facility in an urban area. The results were based on a small sample size and limited to one facility in one province. Therefore, the data cannot be compared between rural and urban facilities and among different provinces. The data could not be compared to other different health conditions affecting cardiorespiratory or neurological systems. OA is also a chronic MSK condition. All this makes it difficult to draw conclusions on the different population groups in South Africa.
The questionnaires used in the study have not been validated in the South African context. The PSFS, ASES-8 and EuroQol 5D5L have been used in various musculoskeletal conditions.41,46,48 Research should be done to obtain validation on these questionnaires specifically in musculoskeletal conditions seen in the SA context.
Conclusion
The aim of this study was to understand OA patients’ perspectives regarding the use of technology as part of their rehabilitation. We found that there was a strong lack of interest in learning new methods of accessing rehabilitation as well as a general lack awareness and acceptance of using technology for rehabilitation. Patients also felt that TR might not be as effective as the traditional face-to-face consultations. These views are possibly due to the limited digital literacy found which is a big factor for incorporating technology in healthcare. This implies that the SA population might not be ready for implementing TR in the public sector specifically at PHC level. Various strategies will be needed to bring awareness on technology use and TR as a mode of service delivery. The next steps are to conduct further research with different population groups at various levels of care within the South African context to explore the feasibility of implementing TR. Many older adults in South Africa lack the necessary educational background and digital literacy skills to fully understand and provide informed perspectives on the use of technology and TR. Therefore, prior to widespread implementation of TR services, it is crucial to provide adequate education and training across diverse populations, including patients, caregivers, and healthcare professionals. This education should aim to enhance their understanding of TR and foster acceptance of these technological approaches in healthcare delivery. Additional research is also needed on the behavioural and educational interventions required to address perceptions and attitudes toward TR among patients in the South African context. Furthermore, research should investigate the feasibility of delivering TR at different levels of care within the local context, as well as explore the various TR service design and delivery models available globally.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241282230 - Supplemental material for Perspectives of patients with osteoarthritis for using digital technology in rehabilitation at a public community centre in the Cape Metropole area: A qualitative study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241282230 for Perspectives of patients with osteoarthritis for using digital technology in rehabilitation at a public community centre in the Cape Metropole area: A qualitative study by Gabriela B. Prins, Eugene Nizeyimana, Dawn V. Ernstzen and Quinette A. Louw in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241282230 - Supplemental material for Perspectives of patients with osteoarthritis for using digital technology in rehabilitation at a public community centre in the Cape Metropole area: A qualitative study
Supplemental material, sj-docx-2-dhj-10.1177_20552076241282230 for Perspectives of patients with osteoarthritis for using digital technology in rehabilitation at a public community centre in the Cape Metropole area: A qualitative study by Gabriela B. Prins, Eugene Nizeyimana, Dawn V. Ernstzen and Quinette A. Louw in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank, Ms Marisa Coetzee, Ms Thandi Conradie and Dr Maria Charumbira for their assistance in this research.
Authors contributions
QAL conceived the study and obtained funding. GBP wrote the first draft of the manuscript. QAL, DE, and EN reviewed and edited the manuscript for intellectual content. All authors contributed to the design of the work, read, and approved the final version of the manuscript.
Declarations
© EuroQol Research Foundation. EQ-5D™ is a trademark of the EuroQol Research Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The health research ethics committee of Stellenbosch University approved this study (S22/11/253).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation Chair Initiative (Grant number UID 115461).
Guarantor
Gabriela Babette Prins.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.