
Abstract
Objective
The modern era of cognitive intelligence in clinical space has led to the rise of ‘Medical Cognitive Virtual Agents’ (MCVAs) which are labeled as intelligent virtual assistants interacting with users in a context-sensitive and ambient manner. They aim to augment users' cognitive capabilities thereby helping both patients and medical experts in providing personalized healthcare like remote health tracking, emergency healthcare and robotic diagnosis of critical illness, among others. The objective of this study is to explore the technical aspects of MCVA and their relevance in modern healthcare.
Methods
In this study, a comprehensive and interpretable analysis of MCVAs are presented and their impacts are discussed. A novel system framework prototype based on artificial intelligence for MCVA is presented. Architectural workflow of potential applications of functionalities of MCVAs are detailed. A novel MCVA relevance survey analysis was undertaken during March-April 2023 at Bhubaneswar, Odisha, India to understand the current position of MCVA in society.
Results
Outcome of the survey delivered constructive results. Majority of people associated with healthcare showed their inclination towards MCVA. The curiosity for MCVA in Urban zone was more than in rural areas. Also, elderly citizens preferred using MCVA more as compared to youths. Medical decision support emerged as the most preferred application of MCVA.
Conclusion
The article established and validated the relevance of MCVA in modern healthcare. The study showed that MCVA is likely to grow in future and can prove to be an effective assistance to medical experts in coming days.
Keywords
Introduction
The thought processes of humans are complex and beyond imagination, and in such a scenario, designing a computational system that exhibits such reasoning capability with the least human intervention is the real challenge. 1 In recent times, high-level experts have been trying to achieve this.
Their main purpose is to simulate human thought processes and model them into a computerized framework. This results in cognitive intelligence, which can be viewed as a combined functionality of information technology and cognitive theory. 2 This cognitive intelligence denotes self-learning models which use predictive analytics to impersonate the working of a brain. 3 In due course of time, this approach will pave the way for the development of automation-driven models which can solve problems without manual interference.
Cognitive intelligence focuses more on structured knowledge enrichment rather than detailed reasoning as it assumes that commonsense presides over knowledge representation complexity. 4
Comprehension is the underlying denotation of cognitive intelligence and is present as narrative content in cognitive psychology. In context to this intelligence, comprehension is represented by integrating the input explicitly by the user, which is found in the profile of the user, which forms a set of inputs denoting the task. 5 This narration then collaborated with data that the system recorded about the commonsense information and its user's personalized data, which leads to the building of the input narrative with new inferences, thereby getting hold of the real intention of the context. 6 Ironically, this comprehension-specific approach is cohesive and involves relevant inferences for precise interpretation, thus dropping out unstructured information. 7 As an example, if a user queries about a more personal event celebration, then it is important for the model to display the inference which includes only specific close contacts. The primary hypothesis of the cognitive intelligence framework lies in the fact that the presence of a comprehension model permits the system to assist its users in a requested activity. The structural framework for cognitive intelligence inferred from this hypothesis is depicted in Figure 1.

General architecture of a cognitive system.
In the current space of cognitive intelligence, its main functionality can be successfully utilized in playing the role of a virtual advisory agent. Siri, Alexa and Google Assistant are good examples of such agents. Experts are working on implementing these personal advisor agents in diverse domains.
8
These virtual agents possess the capability of learning, adapting and eventually finding solutions on their own.
9
To use cognitive intelligence in various applications, some basic learning capabilities of these virtual agents are highlighted in Figure 2 and in the text, it is discussed here as follows:
Adaptive: Solutions are supposed to imitate the human brain's capability to reason and adapt in different settings. The system needs to be non-static in data aggregation and understanding the objectives of tasks. Interactive: Identical to the functions of a brain, a cognitive intelligence model should interact in a bidirectional manner with the entire system, including its devices, processing unit, cloud server and user. Iterative: The system should remember past interactions and return informative data appropriate for a specific domain at any instant. It should define the problem by querying or determining alternate sources. Contextual: The system should understand and retrieve context-based data like syntax and semantics of a defined problem in hand. They may infer from different information sources including sensory data too.

Basic capabilities of a cognitive agent.
Emergence of medical cognitive virtual agents
The increasing digitization of medical applications and the rise in advanced computing technologies have enhanced the design of different assistive tools for the medical domain. These helping technologies strive to support varying user categories in the healthcare zone, ranging from medical experts to patients. Though various literature exists on assistive interfaces for the medical sector, 10 few discuss cognitive agents. 11 The majority of the existing works aim to review modern assistive models for medical applications rather than discussing important technological challenges and research gaps to facilitate cognitive intelligence in the medical field. Hence a knowledge gap exists in determining prime concerns and modern technologies suited to develop effective cognitive virtual agents in the medical domain. However, cognitive virtual agents in the medical field are a topic of relevance in present scenarios. 12 A comprehensive discussion of medical cognitive virtual agents (MCVAs) is presented in this study to deal with the knowledge gap in the current healthcare domain. Vital domains of health care where these virtual agents can be deployed include robotic domain, machine intelligence, cyber secure systems, human–computer aided systems and connected digital healthcare systems.13,14 MCVAs are inspired by integrating together related concepts like intelligent systems, cognitive advisors and virtual healthcare agents. In a simple analogy, an MCVA can be defined as an interactive context-aware cognitive assistive agent which is equipped with computational abilities on the basis of massive data models and facilitates cognition capability to enhance health care through augmenting human intelligence. 15 This improvement in health is achievable by giving cognitive support to all people involved in the medical domain. Hence, enhancing healthcare effectiveness is one primary objective of MCVA. Also, intelligence ability is based upon machine learning, machine vision, automated reasoning and natural language processing. The environment includes a series of situations, resources, contexts and users with which the cognitive agents interact.
Categorization of medical cognitive virtual agents (MCVAs)
MCVAs may be categorized into patient engaged, patient outcome and tutoring driven on the basis of the advanced augmented functionalities of these agents which not only involve both patients and medical experts but also the training techniques used to assist them. These types of MCVAs are discussed as follows:
Patient-engaged MCVAs: to offer prevalent cognition suggestions irrespective of the availability of medical experts. Some applications related to it are shown in Table 1. Patient outcome MCVAs: to offer cognition suggestions to medical staff to provide more reliable and scalable health care, as shown in Table 2. Tutoring-driven MCVAs: to train patients and clinical experts. Some relevant prototypes are depicted in Table 3.
Different types of applications for patient-engaged MCVAs.

MCVA: medical cognitive virtual agent.
Types of cognitive assistance to patient outcome MCVAs.

MCVA: medical cognitive virtual agent.
Types of cognitive assistance to tutoring-driven MCVAs.

MCVA: medical cognitive virtual agent.
MCVAs and their impact

MCVA: medical cognitive virtual agent.
The major contribution of the research analysis includes the following:
The manuscript provides a precise and application-driven analysis of cognitive virtual agents in the healthcare domain. A cognitive functionality-enabled categorization of MCVAs is presented for better interpretation. A novel and computationally intelligent integrated system framework for an MCVA is designed to highlight the generic workflow of a cognitive agent in a multi-phase manner. Different potentially feasible technically advanced applications of MCVAs and their relevance to health care are discussed in the study. Critical technical constraints of MCVAs are also included in this article for better understanding. An analytical survey of the societal perception of MCVAs is presented in comparison to conventional health care is discussed and its outcome is presented. The benefits of MCVAs are established.
Methods
System framework concerning MCVA
A solution design framework for cognitive agents in the medical domain is shown in Figure 3. There are four concurrent phases of the design model, which include system modelling, semantic modelling, system design and development. The system modelling phase is denoted by context-aware medical data where multiple abstract models of the healthcare functionality are developed where each model depicts a distinct perspective of that system. The entity-specific information and the features of the concerned domain are represented in graphical patterns using data flow diagrams or modelling language.
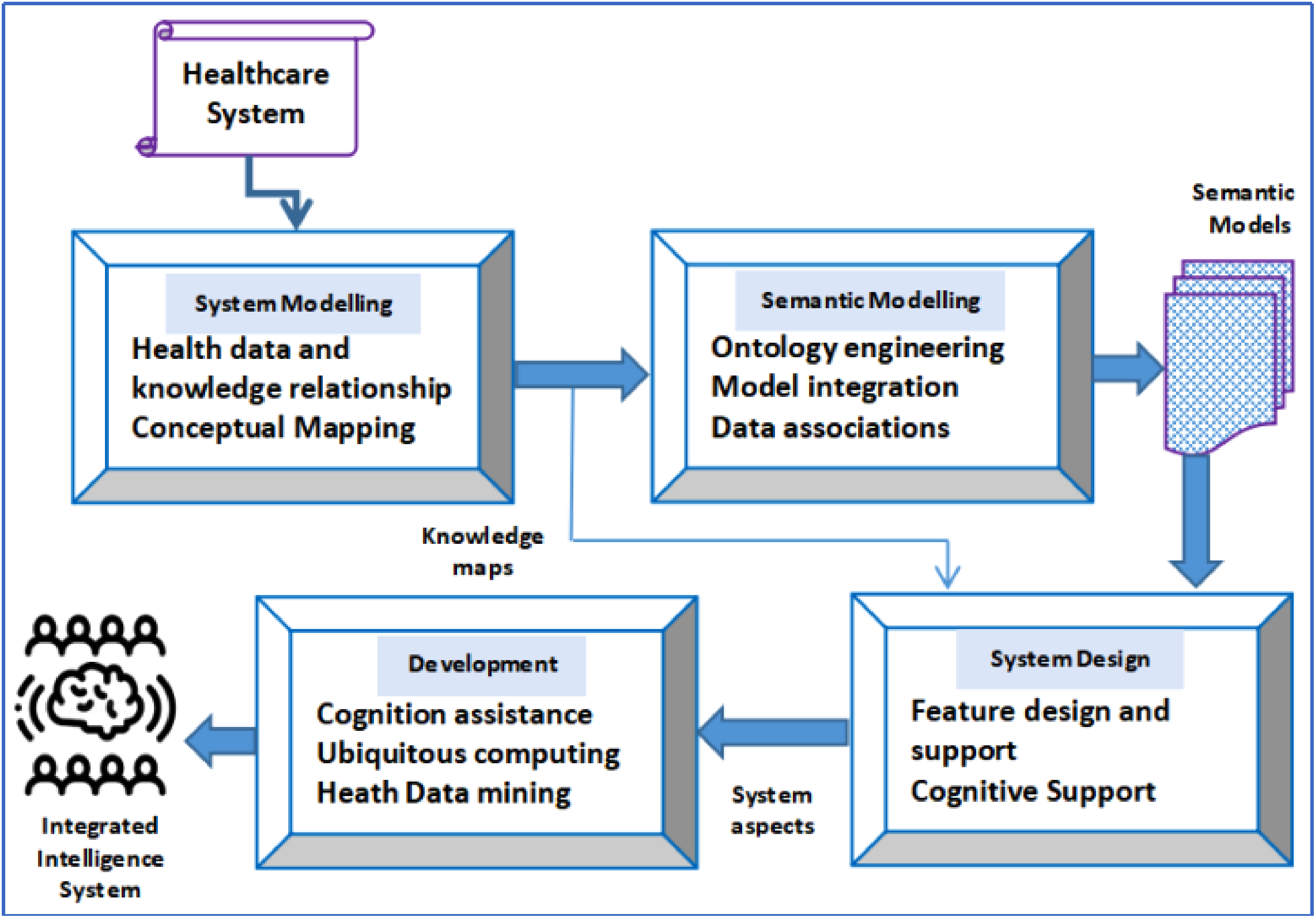
System design model using MCVAs.
Conceptual model is a common abstract representation used in this phase to denote real-world objects which the software architects intend users to understand. It works well if the prototype built in the user's mind is identical to the one which the architects desired.
The second phase is semantic modelling which involves an interpretation of entities used in the data repository (DR) along with their associations with each other in medical application-specific scenarios. It highlights the existing relations among specific data values of entities and their relationships. Ontology engineering is useful to map semantic modelling. Ontologies address the kind of entities in the system and their categorical grouping method. This engineering provides guidance to deal with software interactivity concerns observed in semantic problems in the context of defining medical-related terms and application module objects. This results in creating emergency medical alert notifications and recommendations that retrieve health information from the dataset and react like a decision support module that maps the idea upon health task-specific rules.
System design is the third phase which defines the architectural framework, interfaces and data concerning a system to suit the requirements specification. Here features design is taken care of which includes ambience, structure, navigation, attributes, capabilities and overall sequential organization of features in the healthcare system. Cognition functionality is also integrated in this phase which acts as a tool to generalize, learn, abstract, reason and plan scenarios of medical applications. This phase denotes interrelated requisites related to capabilities, a platform that interconnects the functionalities with the community. It also communicates with devices like mobile phones and tablets.
System development is the final phase of the framework which defines, designs, tests, implements and deploys a novel healthcare information application software. Here ubiquitous technologies related to the clinical domain are studied to develop medical cognitive agents. These intelligent agents are integrated into manual tasks by analysing collaborative models toward collective intelligence. Thus, these phases ultimately lead to the development of an intelligent MCVA.
Functional applications of MCVAs
Medical cognitive agents find many diverse and critical uses where they may be applied with care. In this section, the MCVAs are categorized according to the functionalities of users, different scenarios and associated purposes, as these elements figure out the deployment needs of these virtual agents from other use cases. These virtual agents have been used in different domains encompassing ICU monitoring, educating patients, decision support systems, symptom checkers and many more.37–40 Figure 4 shows some of the modern applications of cognitive healthcare agents.

Advanced applications of MCVAs.
ICU-centric MCVA
MCVA are widely used in ICU for monitoring patients. Cognitive computing is making it possible for digital healthcare assistants to take care of patients even in ICU successfully. These systems are complex and require high-speed streaming information to be analysed.41–44 The major component of the system consists of:
Data Integrator Knowledge extraction component Deployment server Medical/sensor devices Interface for these devices Medical data hub
Programming language processing streaming data from different medical devices/sensors is generally SPADE (Stream Processing Application Declarative Engine). It allows flexibility to the end users to specify which data streams should be incorporated, operators and connections between different streams. These data streams are generated through different sensors on the patient's body. They are responsible for measuring blood pressure, oxygen saturation, heartbeat rate and different parameters of the patient's body.25,45
These devices require an interface to be connected to the healthcare assistant system. These devices could be hundreds in number. The interface device converts the data stream into an internet protocol (IP) stream. These IP streams from hundreds of devices are forwarded to an interface server. Using an application program interface, selective data streams are filtered from the server.46–48 Conventionally these cognitive virtual healthcare assistants process streaming data almost in real-time, and concurrently storing of data is done.
The Data integration manager (DIM) constitutes operators to communicate with the database interconnectivity unit. There is a need for the storage of unprocessed data in the integrated repository. Data from the DIM database is moved to a DR at regular intervals. This repository is mostly placed inside the knowledge component. The knowledge component uses a data analysis and mining framework capable of processing multidimensional, temporal data. 49 The patterns detected from the knowledge component and clinical rules stored in the database are both used to develop an ontology. The deployment server is used to deploy the SPADE application program for stream computing to function smoothly. Figure 5 depicts the scenario.
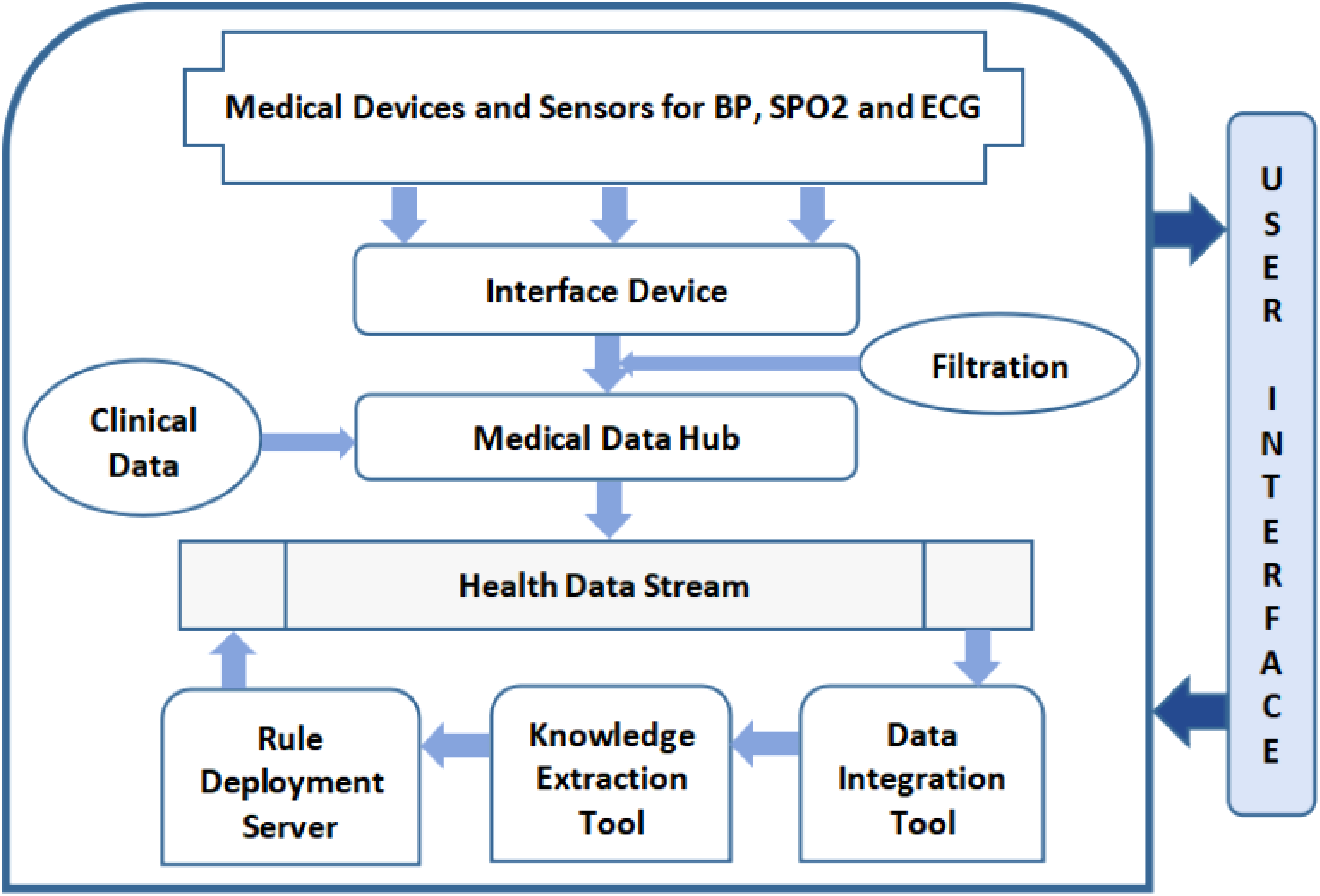
Framework of an ICU healthcare assistant.
Patient education-centric MCVA
All around the world, millions of people die due to chronic health conditions like diabetes, hypertension and heart disease.
50
Healthcare assistants are widely used to train and educate patients to maintain a lifestyle that would improve their health conditions. These systems equipped with sensors are capable of analysing patients’ health parameters and accordingly suggest interventions through a dialogue. The natural language processing (NLP) unit consists of two components NLP comprehension and NLP generation unit, as shown in equation 1.
The architecture of the healthcare agents (HCA) is shown in Figure 6. These HCA systems are generally installed through smartphones. The objective of this system is to monitor the patient's vital parameters. It also engages in a dialogue with the patient and assists him to enhance his/her knowledge and cope with the medical condition. Parameters like heart beat rate, oxygen saturation and blood pressure can be monitored by the add-on devices connected to the smartphone or by the smartphone itself.52–55 These healthcare-assisting applications installed on the smartphone encourage patients to monitor their vital parameters regularly. It helps in comprehending the results of this measurement. It makes an analysis and suggests interventions based on the severity of the case. In some cases, the system suggests a more active lifestyle. In moderate cases, it suggests medicines in consultation with doctors, and in emergency cases, it would suggest immediate hospitalization. Atrial fibrillation virtual agent is one such application that is capable of analysing patients’ heart rhythm patterns and suggesting interventions. 56

Framework of MCVAs to educate patients.
Physical therapy-centric MCVA
MCVA have now been developed which are able to provide physical therapy to patients.
57
These systems are highly in demand as the requirement to provide physical therapy to patients has increased manifolds. In remote places where medical support is not in reach, physical home therapy would greatly benefit patients. In several cases, patients require post-surgery at-home physiotherapy sessions. Several sessions are required for patients to return to normal life. These physiotherapy sessions are expensive. However, smart systems these days provide customized at-home physical therapy. KinoHaptics is one such smart device.
58
This device consists of different sensors. The system can pick up feedback from haptic (touch) vibrations. It can accurately track a patient's body motions. A physiotherapy session directed by a doctor can be configured into the system. The system architecture consists of:
Kinect Armband Doctor Patient Bluetooth modem
The interface of the system is designed to be user-friendly and generally has both patient's and physician's interface.
59
An armband can direct the patient and deliver feedback on the physiotherapy session. In each session, a patient is expected to lift a body part at a required angle. Each vibrohaptic feedback created by the hand band is an encoded message from the device. The frequency, intensity and duration can be customized by the physician. The patient coordinates with the medical assisting device and armband as shown in Figure 7. This smart healthcare assistant reduces the dependency on physiotherapists.

Framework of MCVA to provide physical therapy.
Elderly assistance-centric MCVA
Technology advancements have enabled us to take care of the elderly generation's cognitive skills in a better way. Elderly people often suffer from loss of memory, linguistic impairment, motor skill loss, etc.60–62 The focus is on elderly people without severe deficits in cognitive skills and aim to retain their skills for a longer period. Technology-driven suggested exercises have succeeded in addressing the mental stimulation of the elderly. Figure 8 displays the framework of such a healthcare assistant. These healthcare systems include novel board games, which include a system of bonuses and penalties based on the execution of tasks to be accomplished by the players. These games can be played by a couple of players simultaneously even remotely. The outcome of these games is game scores. These scores are analysed and further provide the health status of the end user. Based on the end user's health condition, the smart healthcare assistant suggests customized games that will further help in maintaining the cognitive skills of the elderly. The tasks assigned to the players are designed in such a way that they ensure training to improve memory, reasoning, focus and categorization. 63

Framework of MCVA to assist elderly in retaining cognitive skills.
Based on the score attained by the players, a diagnostic score is generated. This score throws an insight into the user's current mental abilities and health status. The smart healthcare assistant would provide a customized set of tasks for users depending on their existing health status. Accomplishing the given set of tasks would enhance and help users to retain their mental faculties. 16 These tasks are customized based on the diagnostic score in each cycle. Several cognitive algorithms are used to manipulate the suggested tasks based on each diagnostic score in a cycle.
Decision support-centric MCVA
Healthcare assistants are widely used to support doctors in suggesting treatments and therapies to patients. However, these healthcare assistants can improve their decision-making by processing this huge voluminous data with more information and better analytics techniques. Using big data along with cognitive computing techniques would result in better therapy suggestions by the MCVAs. This would result in effective cost reduction by not providing the wrong treatment and avoiding the detrimental side effects of the associated treatment.64–66
Doctors now use several such healthcare assistants. IBM's cognitive computing healthcare assistant is also widely being used. The decision support systems extract knowledge from available guidelines, books, research articles and journals. They are also data-driven and learn by finding patterns and trends in the existing medical data using cognitive computing techniques.27,67
The physical assistants can read and understand concepts, learn therapies, recollect information, enhance their performance through machine learning techniques and understand the effect of prescribed treatment on the patient. This system suggests treatments based on studies and patterns discovered in data.
The knowledge encapsulation module extracts and builds a knowledge base from clinical guidelines and evidence. The medical domain knowledge is built into the system as a set of ontological rules, as highlighted below.
If Health Disorder = pancreatic beta cells & 7 symptom is polydipsia + elevated blood glucose, then disposition = diabetes mellitus
The retrospective analysis module analyses the patients based on clinical guidelines and generates patient similarity metrics. This could be used to assess the patients’ therapy outcomes. The cosine similarity metrics between two non-zero vectors X and Y is given in equations 2.

The Jaccard coefficient of similarity measure is shown in equation 4.
The prospective analysis module uses machine learning and cognitive techniques on similar patients’ data. Based on the patterns discovered it helps in recommending better therapies and effective decisions.68–70 It requires an understanding of natural language processing to comprehend queries. Processing queries require semantic analysis, speech translation and generating hypotheses, parsing, answer searching, lexical matching, and machine learning techniques including logistic regression, similarity learning and deep learning techniques. A skeleton structure of a decision support model-based MCVA is shown in Figure 9.
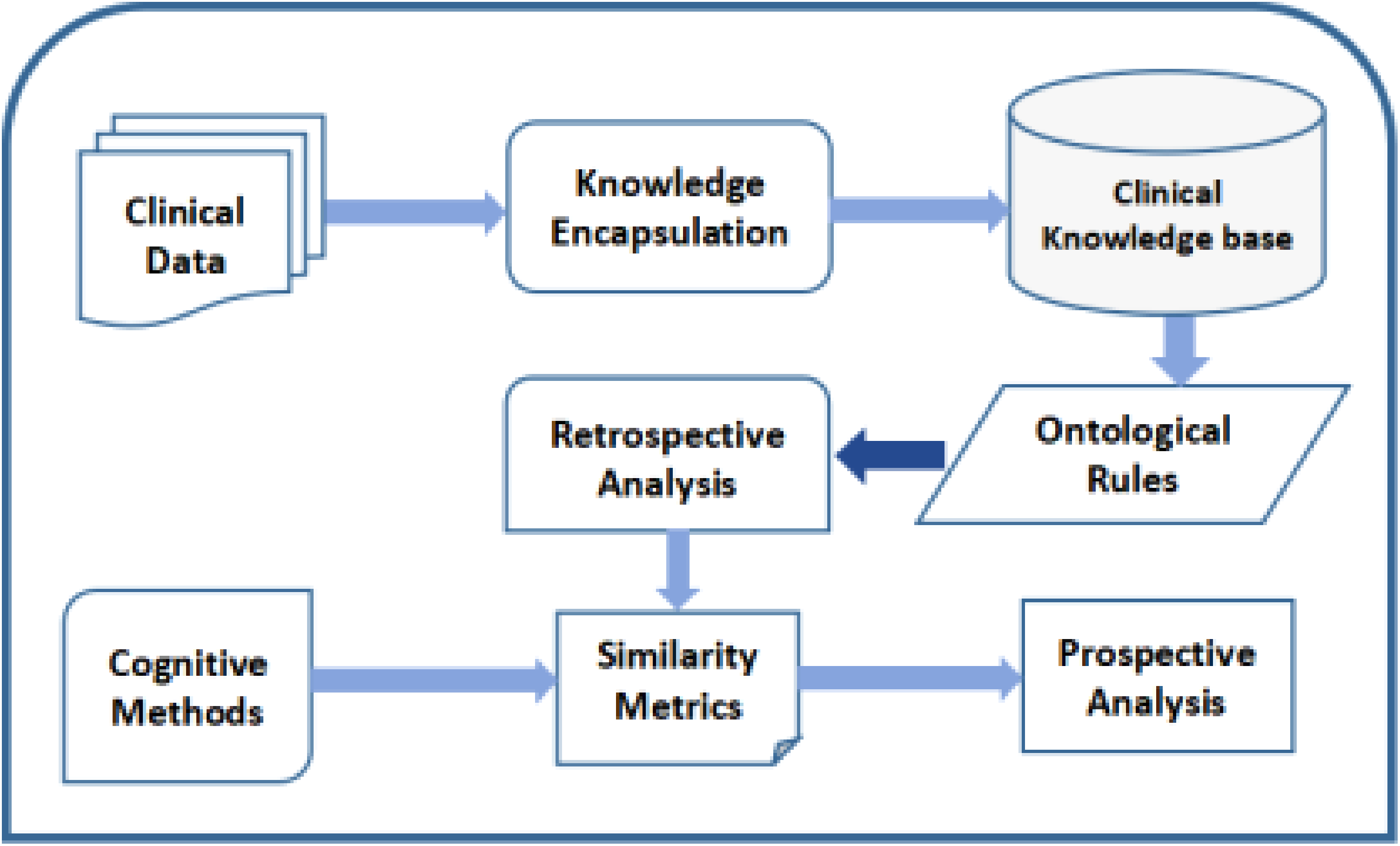
The framework of a clinical decision support system based on MCVA.
Personalized chatbot-centric MCVA
The use of automated conversational agents in the medical domain has increased profusely. These chatbots have access to medical knowledge and could be extremely useful to patients who have been discharged from the hospital or patients having ailments that require regular medical screening of symptoms. 18 With the development of cognitive computing techniques and their proven effectiveness, has resulted in it being used in different domains. Medical chatbots powered by cognitive computing provide simple symptom analysis and a conversational mechanism to predict the health condition and recommend corrective steps if any.
The chatbot establishes a dialogue with the user. The purpose of the dialogue is to extract and assess the health condition of the user. Based on the answers received from the user the chatbot further engages in symptom-specific health condition queries. 71 Based on the inputs received from the end user the chatbot further recommends lifestyle changes or refers immediate doctor's screening. However, the conversational agents face issues with responses received in non-medical terms which are sometimes ambiguous. For example, an end user may reply with stomachache for a multiple symptom. He may not be able to specify the health condition in medical terms.72–74 To address this issue natural language text is split into sentences. Parsing is done. Noun phrases are extracted. Medical terms are detected using ontologies. Unified medical language systems, disease ontology, symptom ontology, etc. are used. These chatbots are evaluated using different performance evaluation metrics and have been extremely efficient.24,75,76 Figure 10 demonstrates a simple personalized symptom-checked chatbot.

Framework of a MCVA based personalized symptom checker chatbot.
Customized monitoring-centric MCVA
Patients with cognitive disabilities are becoming over-dependent on healthcare assistants. Doctors and nurses are overburdened with the huge number of patients they have to attend to. Medical practitioners can attend to several patients remotely. These medical assistants need to be customizable so that with progress in disease or recovery from disease the technology-enabled treatment can be updated. For example, in Alzheimer's disease, with the progress of the disease the requirements of the disease change. These systems use several sensors. The medical practitioner is the controller of this healthcare assistant. The controller can change the parameters of the system and can provide customized assistance to the patient. Based on the reading from the sensors’ input mapping is done and it provides inputs to the machine learning component. The customization interface helps to settle the right parameters for the learning algorithms. It comes up with a set of actions/policies best suited for the patient. It is mapped as output mappings and communicated to the patient.77,78
Figure 11 demonstrates the customizable healthcare assistant consisting of an environment layer, customization layer and AI layer. The machine learning component consists of sophisticated algorithms like convolution neural networks, support vector machines, and decision tree as mentioned below.
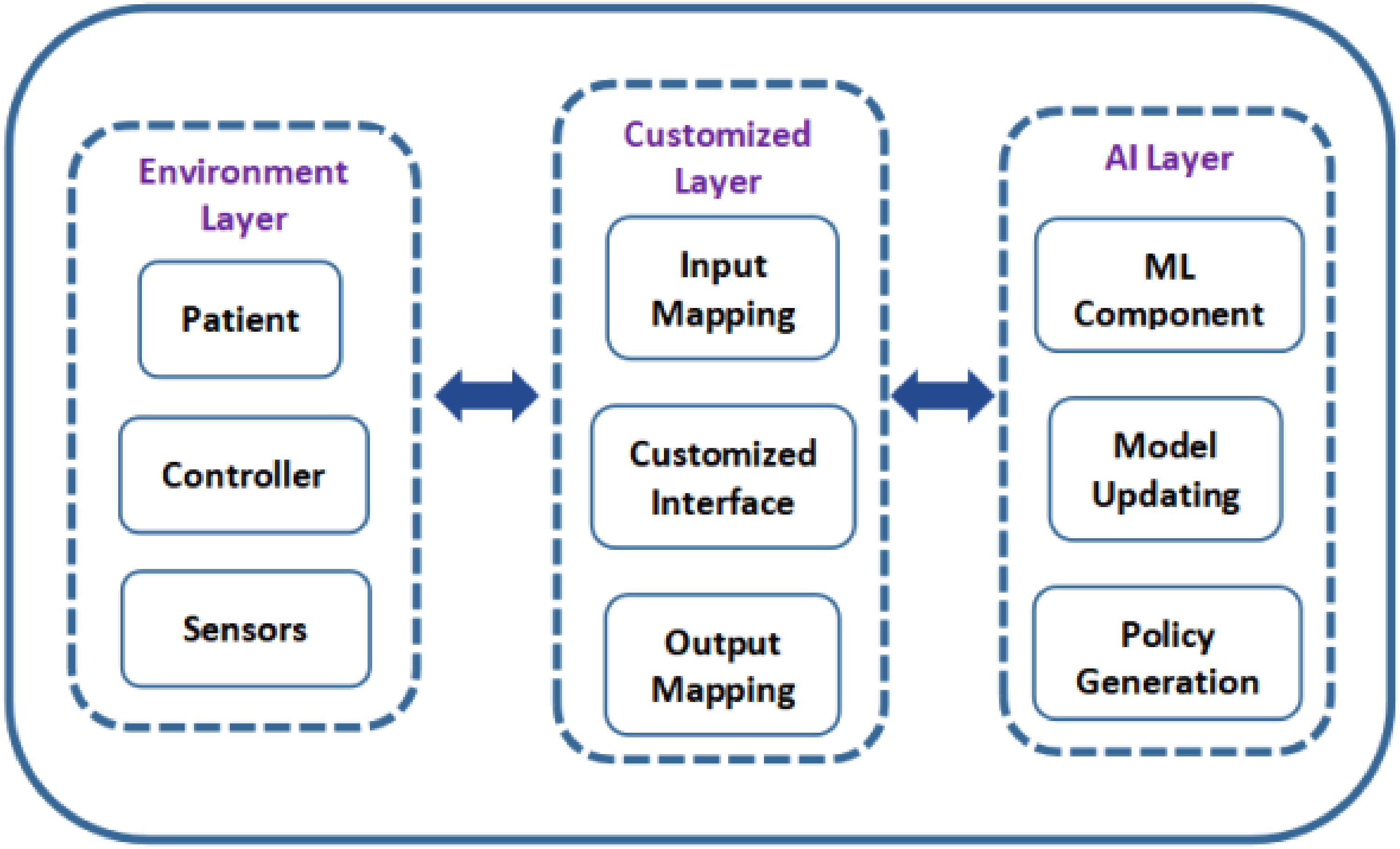
Framework of a customizable monitoring of MCVA.
The radial basis function (RBF) kernel function used in support vector machine (SVM) is shown in equation 5.


MCVA relevance analysis
An analytical survey through Google Forms was undertaken in different parts of India regarding the importance of MCVA in today's scenario. This survey was termed as ‘MCVA Relevance Survey’. Various metrics and features were taken into consideration during the analysis. As many as 5412 participants voluntarily took part in the survey. The MCVA relevance survey process was conducted in online mode during March 2023. The set of survey questions was prepared through Google Forms in consultation with experts. This question set has queries in the form of multiple-choice questions along with a small space provided to record the reason for selecting a specific option.
These questionnaires were forwarded to the pool of participants to get responses from them. The participant team mainly constitutes many medical experts, patients and technologically skilled staff. This team is formed through personal contacts, email broadcasting, volunteers and a network chain. The filled-out responses of the participation team are aggregated in .csv file. There may be a few of these responses with missing values either in the option part or in the reasoning space provided. Some reasoning notes may seem incomplete. Also, the respondent details are visible in the collected file. Thus, a preprocessing procedure is followed where the missing values and the incomplete reasoning are dropped while the respondent columns are also deleted. This preprocessed response file is sent to the validation team. The main job of the validation team is to evaluate the correctness and suitability of the answers provided by the participation team. This team also has a similar composition as that of the participation team. To maintain transparency and impartiality in evaluation, there are no persons who belong to both teams. Also, the respondent details from the response sheets are dropped out in the preprocessing stage before passing to the validation team to maintain the privacy and authenticity of the process. After successful validation by the validation team, the processed output is the filtered response sheet in .csv format which is retrieved by authors for performance analysis. The overall process is illustrated in Figure 12.

Stepwise process of MCVA relevance survey.
Results
This section presents the results analysis of the impact of MCVA in modern society and the outcome of MCVA relevance analysis. Different survey-based questionnaires are designed to capture society's opinion. A diverse section of society which includes medical staff, patients, technology experts and other miscellaneous professionals became part of the survey. Around 51% of volunteers included medical staff and patients while the rest 49% comprised technological experts and individuals from other professions as shown in Figure 13.

MCVA relevance analysis survey participants division.
In another analysis, a concrete equal ratio subdivision between urban and rural populations was studied. Their preference level for MCVA was surveyed and it was noted that there was a sharp rise of 80% of people preferring MCVA over conventional health services in urban society. On the contrary, only 32% of volunteers in the rural population gave MCVA a chance in this modern health care as highlighted in Figure 14. An age group analysis was conducted with respect to the acceptance of MCVA over conventional health care in different age groups. It was observed that elderly people and senior citizens found MCVA more acceptable than today's youths. An approximate population of 60% of participants of the age group beyond 50 years found the service of MCVA more relevant than traditional medicine. Figure 15 shows the outcome of the analysis. MCVA finds scope in many diverse healthcare applications as shown in Figure 16. In this survey, participants ranked the order of priority of the use cases of MCVA as per the requirements of society. Medical decision support application was recorded to be most relevant with 20% relevance while patient education application with 9% relevance is found to be the least significant use case in the present healthcare scenario.
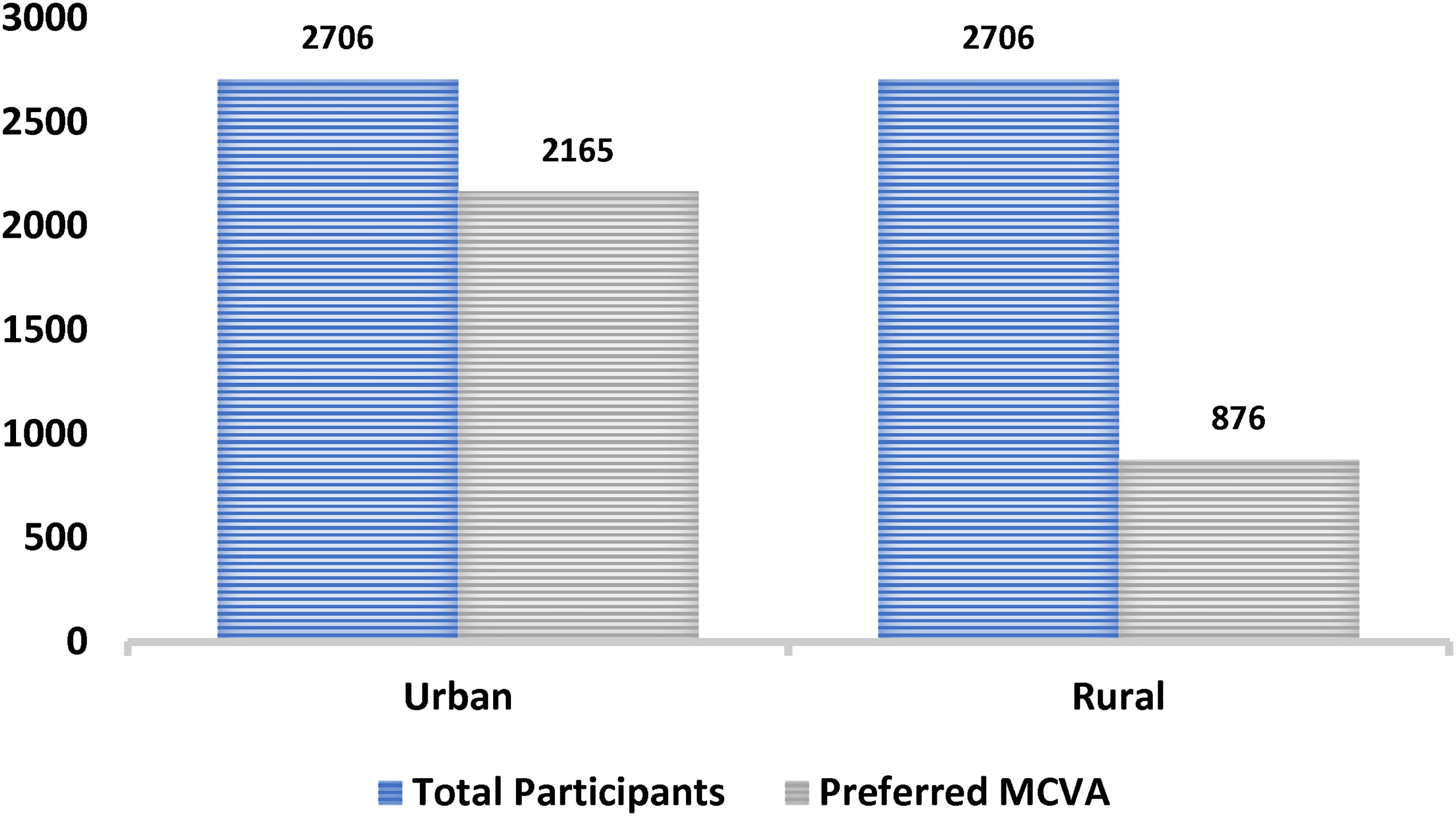
MCVA preference in urban–rural domain.

MCVA relevance analysis in context to age groups.
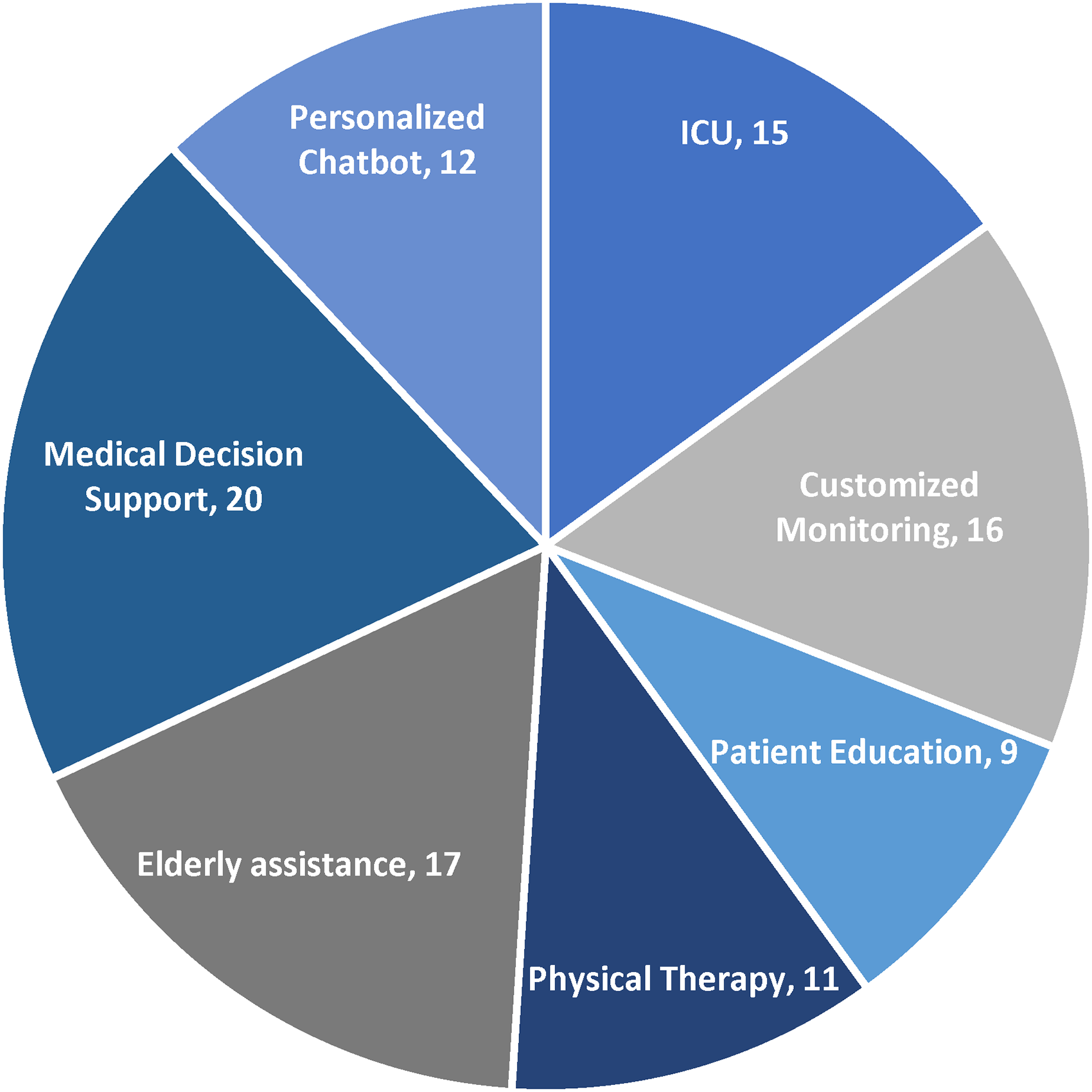
MCVA relevance analysis in context to different use cases.
The analytical survey in the context of MCVA was undertaken where diverse sections of various communities took part in the survey. The majority of the participants belonged to the healthcare sector as the topic in discussion is related to the health sector. Again, the survey was carried out with both urban as well as rural populations altogether to understand the requirements and comfort level of each section of society. Though a large section of urban society showed their inclination towards the adoption of MCVAs still the rural population stuck with traditional medical services. This divide is due to the fact that rural people are less exposed to modern technological innovations and their reluctance to change. This scenario will change over a period of time with the gradual emergence of MCVAs. Also, an age group-wise analysis of the application of MCVAs was carried out and it was observed that elderly citizens gave more constructive feedback to MCVAs as compared to youths. This can be attributed to the fact that MCVAs provide more precise results, easy to operate and less prone to errors. Finally, a relevance analysis of different applications of MCVA is done through a survey. It was found that a large section of people found medical decision support as the best application of MCVAs because these virtual agents are equipped with advanced cognitive abilities that help them in instantaneous decision-making. Though at present MCVAs are very much in the inception stage, gradually it is likely to emerge as a reliable assistive tool for medical experts and patients in forthcoming days as a good decision support interface.
Discussion
This research studies MCVAs. A novel cognitive integrated system framework was designed for virtual medical agents. In this study, an extensive study was done on the different types of MCVAs and their application. An analytical survey ‘MCVA relevance analysis’ was conducted to find out the perception of people on MCVAs versus the traditional healthcare system.
Though these virtual assistants are of great help to healthcare experts in various domains still there exist some gaps in these MCVAs that need to be addressed to make them more productive. Some visible limitations identified from existing literature are as follows:
System–user interactivity
These medical virtual agents have to interact with humans in a natural setting through natural languages. Thus, it is very important to augment the capabilities of library modules in natural language processing with cognitive intelligence. 79
Commonsense reasoning
The basic template of MCVAs is dependent upon the discourse of commonsense knowledge. Based on this, the real challenge is automated learning and how to populate the commonsense dictionary. 80
Content-aware memorization
MCVAs are required to recognize previous interactions and accordingly respond to application-specific use cases. 32 Besides, these agents must be capable enough to differentiate among a variety of anomalies to provide accurate cognitive suggestions.
Ambiguities and uncertainties
MCVAs should be dynamic and adapt well to uncertain clinical situations. 81 These agents should be able to find solutions by using additional medical resources to resolve incompleteness in health data. At present, almost all such medical agents fail to address this ambiguity.
Privacy preserving
In most of the MCVAs, the privacy element is overlooked. Protecting confidential data from malicious usage is a vital challenge for MCVAs. Besides abnormal attacks like errors in robotic surgery or wrong drug dosage can result in fatal consequences for users.82–84
Multi-modal interaction constraints
Modern MCVAs are providing multi-modal facilities thereby offering cognitive virtual assistance for many functions using virtual simulation-based platforms. Still, at present, these MCVAs lack meaningful and frequent user interactions. 85 Also, they are prone to privacy attacks.
Adaptability concern
Adapting to varying situations and use cases is another issue since these agents possess the power to discover naturally like humans. 86 As a result, humans are scared as these agents may replace humans in the near future.
High-speed streaming and data processing
Several MCVAs have to process huge amounts of real-time data and implement complex algorithms to make quick decisions and provide effective medical support to the patients.30,87,88 This would require sophisticated high-speed computing devices and servers. Several hospitals and patients are not able to afford such expensive MCVAs.
Complex user interface
Many of the MCVAs have complex user interfaces which require the knowledge of smart devices. Several patients due to age and physical difficulties may not be able to use such complex applications thereby reducing the scope of virtual healthcare assistants. 87
Low acceptance of MCVA among patients
Patients are reluctant to use these devices as the absence of a real medical practitioner reduces the credibility and acceptance of MCVAs. Patients world over prefer to interact personally with a medical practitioner than interact with a virtual agent.88,89
Complex customization of MCVAs
Though it is possible to customize MCVAs but requirements of the patients are diverse. Patients having different medical conditions and symptoms require different treatments and therapies. Therapies suggested by the MCVAs may not be able to customize them precisely as per the requirement of patients automatically. 90 Human intervention may be required.
Convoluted symptom checking
As viruses and diseases evolve it has been found that several diseases have similar symptoms.91,92 Symptom checkers used in MCVA might use mining algorithms or suggest lab tests to do a proper diagnosis of the disease.
Conclusion
MCVAs are likely to be a recognized force in modern times to make the future medical more practical enabled, precise, scalable, consistent and efficient. The primary purpose of this study is to highlight the current stature of these virtual assistants in the healthcare space and explore their unique features. Different use cases of MCVAs have been highlighted with examples. A novel framework for MCVAs has been presented in this study. Different applications-based novel architectures have been designed taking inspiration from existing works. The impact of MCVAs is presented. Towards the end, the study presents the outcome of the MCVA relevance survey thereby demonstrating the significance of MCVA in modern health care. Overall, the research study addresses the rise of these healthcare agents which can be a reliable assistive tool to medical experts in various medical applications in future.
Though extensive work is undertaken in the context of MCVA in this article, still further enhancements may be made in future. The MCVA classification may be done in a different way on the basis of achievable outcomes. The MCVA relevance analysis survey can be made more global involving a wide range of participants throughout the globe. The outcome of the survey can fetch more accurate results and further strengthen the evaluation if more queries with minute technical details can be included in the questionnaires would.
Footnotes
Acknowledgements
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through large Research Groups Project under Grant number (RGP.2/127/44).
Authors contribution
Conceptualization, Sushruta Mishra, Pamela Chaudhury, Hrudaya Kumar Tripathy, Kshirasagar Sahoo, N.Z. Jhanjhi; formal analysis, Pamela Chaudhury, Hrudaya Kumar Tripathy, Kshirasagar Sahoo, N.Z. Jhanjhi, Asma Elnour; funding acquisition, Hrudaya Kumar Tripathy, Kshirasagar Sahoo, N.Z. Jhanjhi, Asma Elnour, Abdelzahir Abdelmaboud; investigation, Sushruta Mishra, Pamela Chaudhury, Asma Elnour, Abdelzahir Abdelmaboud; methodology, Sushruta Mishra, Pamela Chaudhury, Hrudaya Kumar Tripathy; Supervision, Hrudaya Kumar Tripathy, Kshirasagar Sahoo, N.Z. Jhanjhi, Asma Elnour, Abdelzahir Abdelmaboud; writing – original draft, Sushruta Mishra; writing – review and editing, Sushruta Mishra, Pamela Chaudhury, Hrudaya Kumar Tripathy, Kshirasagar Sahoo, N.Z. Jhanjhi, Asma Elnour, Abdelzahir Abdelmaboud.
Author's Note
Abdelzahir Abdelmaboud is also affiliated with Department of Information Systems, King Khalid University, Muhayel Aseer, Saudi Arabia
Data availability statement
Will be furnished on request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP2/319/45.
Guarantor
N.Z. Jhanjhi is the Guarantor 0000-0001-8116-4733.