
Abstract
Background
The prevalence of heart failure (HF) is increasing in Uganda. Ugandan patients with HF report receiving limited information about their illness and associated self-care behaviours. Interventions targeted at improving HF self-care have been shown to improve patient quality of life and reduce hospitalizations in high-income countries. However, such interventions remain underutilized in resource-limited settings like Uganda. This study aimed to develop a digital health intervention that enables improved self-care amongst HF patients in Uganda.
Methods
We implemented a user-centred design (UCD) process to develop a self-care intervention entitled Medly Uganda. The ideation phase comprised a scoping review and preliminary data collection amongst HF patients and clinicians in Uganda. An iterative design process was then used to advance an initial prototype into a functional digital health intervention. The evaluation phase involved usability testing of the intervention amongst Ugandan patients with HF and their clinicians.
Results
Medly Uganda is a digital health intervention that allows patients to report daily HF symptoms, receive tailored treatment advice and connect with a clinician when showing signs of decompensation. The system harnesses Unstructured Supplementary Service Data (USSD) technology that is already widely used in Uganda for mobile phone-based financial transactions. Usability testing showed Medly Uganda to be both acceptable and feasible amongst clinicians, patients and caregivers.
Conclusions
Medly Uganda is a functional digital health intervention with demonstrated acceptability and feasibility in enabling Ugandan HF patients to better care for themselves. We are hopeful that the system will improve self-care efficacy amongst HF patients in Uganda.
Keywords
Introduction
The prevalence of cardiovascular disease (CVD) is on the rise in Uganda, 1 with CVD now accounting for roughly 10% of deaths in the country. 2 This increasing prevalence of CVD places an immense burden on cardiac clinics, specifically given that African patients with CVD often present with various structural and haemodynamic complications, such as heart failure (HF), that require both acute and long-term management. 3 In the chronic phase of HF, patients require complex treatment plans involving a myriad of medications, lifestyle recommendations and self-care behaviours. 4 These management plans can be burdensome for both HF patients and clinicians, given the necessity for follow-up appointments to monitor patient health, the financial costs associated with medications, the need for adherence to stringent self-care instructions and the overall impact of HF on patient quality of life. 5 Ugandan patients with HF describe receiving limited information about their illness, its management or appropriate self-care behaviours. 6 These challenges necessitate novel solutions aimed at mitigating the burden of HF, improving the patient experience and offloading overburdened clinics.
Amongst the potential solutions to these challenges is the promotion and improvement of HF self-care. Such patient-centred care strategies aim to empower patients with skills and behaviours that will improve illness management and health outcomes. 7 Self-care interventions have been found to enable patients to better manage their own condition, and have been successfully implemented in other resource-limited settings.8–11 Various technological and non-technological methods of improving chronic disease self-care have been investigated in low- and middle-income countries (LMICs), with digital health interventions appearing to be the most common modality. 12 Various factors make digital health interventions favourable for improving self-care in resource-limited settings, such as the near-ubiquity of mobile phone penetration in LMICs, 13 the ability to automate simple tasks with minimal oversight from oft-overburdened clinical staff, and the functionality to algorithmically triage patients in order to optimize resource allocation. 14 One communication modality well-suited for digital health interventions in LMICs is Unstructured Supplementary Service Data (USSD) – a signalling protocol universally available in both smartphones and non-smartphones that is commonly used for mobile banking transactions in resource-limited settings. An interaction with a USSD-based system is initiated by dialling a service provider's USSD code (e.g. *123#), which opens a microbrowser in which users can navigate through a decision-tree menu using numbers on their keypad to perform a specific task (e.g. transfer money and check balance). This technology differs from short message service (SMS) (i.e. text) messaging, as it allows for a live user-to-server connection in which information can be quickly exchanged. 15 Despite the potential benefits of self-care tools in general and digital health interventions in particular, HF-specific self-care remains underutilized globally, with one of the greatest performance gaps coming from LMICs like Uganda. 12
Our research team previously developed a digital health intervention (Medly) for use in Canada, which features a validated rules-based algorithm to triage patient symptoms, deliver tailored self-care advice to patients and alert clinicians of signs of regression in patient health. 16 Medly has been shown to reduce HF-related hospitalizations and to improve patient self-care ability.17, 18 As an extension of these positive results, as well as the aforementioned need for improved HF self-care in LMICs, our team recently performed formative research with the goal of adapting Medly for use in the Ugandan context. This formative research included a scoping review of previous self-care interventions deployed amongst patients with non-communicable diseases in LMICs, 12 as well as a mixed-methods study to explore the lived experiences and technological literacy of HF patients and clinicians at a cardiac care centre in Uganda. 19 In the latter study, we concluded that (a) Ugandan HF patients and clinicians could benefit from an intervention that empowers patients to better care for themselves and (b) that such an intervention should incorporate USSD technology that is already familiar to Ugandans as a result of its use in local mobile money services. 19 Accordingly, we implemented a user-centred design (UCD) process 20 to develop a USSD-based self-care intervention called Medly Uganda. The UCD process and the resulting digital health intervention are described in this manuscript.
Methods
Study design
This study used a UCD process for the conceptualization, design and development of Medly Uganda. Design activities were based primarily at the Uganda Heart Institute (UHI), a cardiac care centre located in Kampala, Uganda. As a design philosophy, the UCD process directs the creation of technologies with consistent consideration of end-user needs throughout three main stages of design: ideation, design and development, and evaluation (Figure 1). 20 Guided by this philosophy, our multidisciplinary team of patients, clinicians, researchers, engineers and designers worked to develop an intervention that was both effective and contextualized to the local population. All research activities were approved by the Uganda National Council of Science and Technology (HS 2364), the Makerere University School of Medicine Research and Ethics Committee (REF 2017–076), the University Health Network Research Ethics Board (ID# 14-7510) and the Yale Human Research Protection Program (ID# 2000025338).
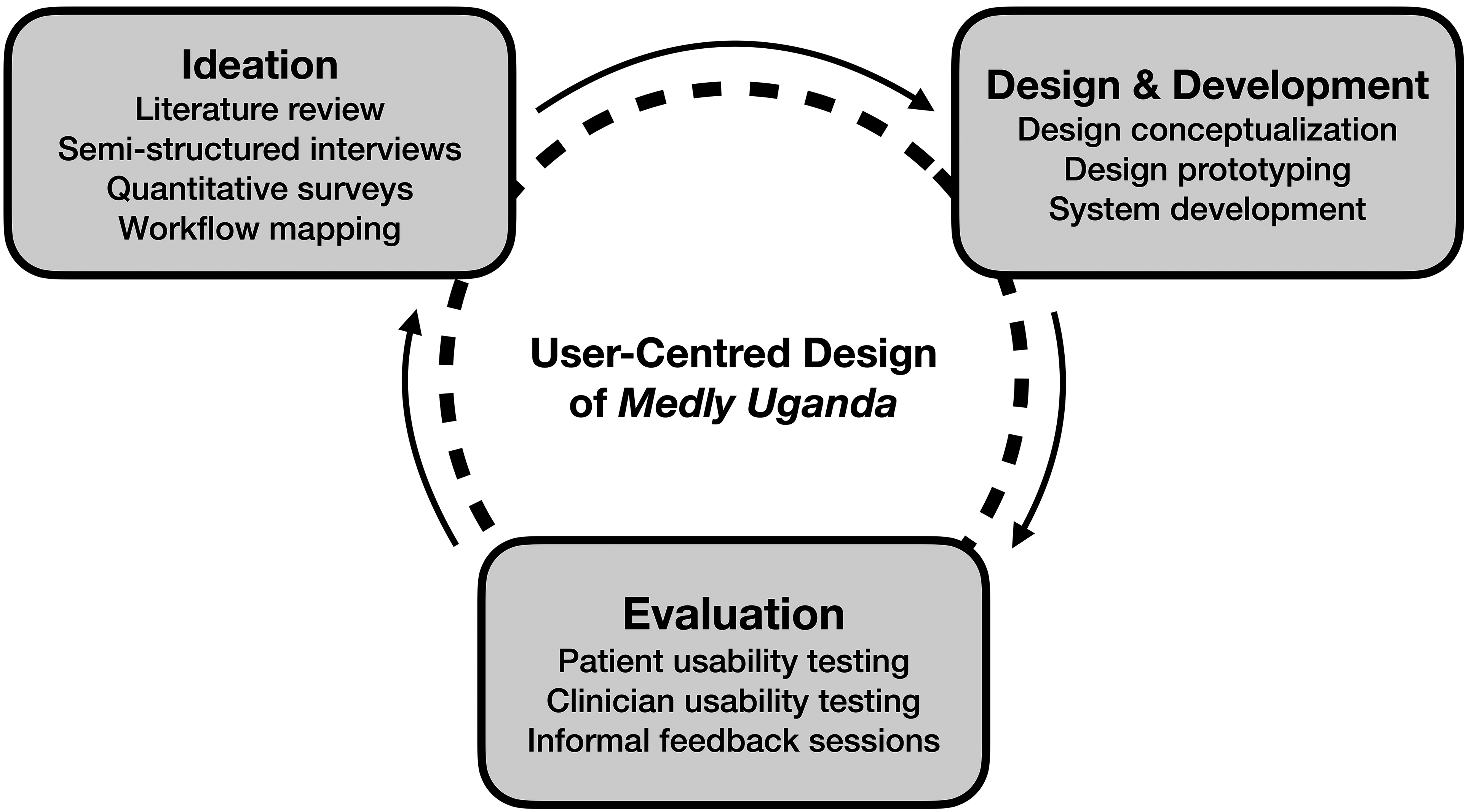
User-centred design (UCD) framework (adapted from McCurdie et al. 20 ).
Phase 1: Ideation
The aims of the first phase of the UCD process were (a) to obtain a baseline understanding of the use of chronic disease self-care in LMICs, (b) to work with Ugandan HF patients and clinicians to define the specific needs and functionalities of a potential digital health intervention and (c) to gain an understanding of the technical resources and on-the-ground personnel available to support the delivery and implementation of the intervention. We first conducted a scoping review on the use of self-care for non-communicable diseases in LMICs, with the goal of summarizing the nature and effectiveness of past interventions that have enabled chronic disease self-care in resource-limited settings. 12 To better understand the HF-related needs and available technological resources in Uganda, we then conducted a mixed-methods study focused on the experiences and technological literacy of HF patients and clinicians at UHI. 19 Based on the key findings in this preliminary research, a list of design principles was defined to guide the development of a digital health intervention.
Phase 2: Design and development
The aim of the second phase of the UCD process was to utilize the elicited feedback from patients and clinicians to design an intervention prototype. A preliminary design, consisting primarily of schematics, sketches and mockups describing the main components of the intervention, was created to allow for members of the multidisciplinary research team to provide feedback and suggest refinements to the system design in a series of iterations. Sketches of the various dashboard screens were created in conjunction with a user interface designer using Keynote, and subsequently used to create an interactive wireframe using inVision. Similarly, a smartphone application was developed to simulate the expected functionality of the patient-facing USSD application. These mockups were then presented to Ugandan patients and clinicians by a member of our research team to elicit informal feedback that could be used to refine both the patient- and clinician-facing aspects of the intervention. We continued to iterate the intervention in this manner until minimal suggestions for improvement were elicited by the end-users, at which point we proceeded to develop the prototype into a fully functional digital health intervention.
During this design and development phase, our research team (based at the Uganda Initiative for Integrated Management of Non-Communicable Diseases) also developed strong relationships with key stakeholders in Uganda. Namely, the team fostered connections with united nations children's fund (UNICEF), the Uganda Ministry of Health and a Ugandan technological consulting firm entitled GoodCitizen. These relationships facilitated the development and local deployment of the intervention, as each of the three organizations had previously collaborated in the creation of a USSD-based system entitled FamilyConnect. 21 Accordingly, existing infrastructure and experiential knowledge were able to be harnessed for the deployment of the USSD-based component in our digital health intervention.
Phase 3: Evaluation
The aim of the third phase of the UCD process was to evaluate the design of the digital health intervention to help ensure that the system could be effectively implemented in practice. Both HF patients and clinicians were invited to participate in moderated usability testing of the patient- and clinician-facing components of the system, respectively. A moderated approach was implemented to allow for in-depth information regarding user behaviours and identified areas for improvement. Participants were recruited from UHI. Patient eligibility criteria included a diagnosis of HF by a clinician at UHI and the ability to communicate in English, Luganda or Runyankole. Clinicians were considered eligible if they were a physician or nurse with direct experience caring for HF patients at UHI.
At the start of each usability test, the study protocol was discussed and written informed consent was obtained. Next, a high-level overview of the Medly Uganda system and the long-term vision for its deployment at UHI was provided. Participants were then asked to follow a series of simulated scenarios on their own device to test the functionality of the system. Examples of simulated scenarios for patients included reporting current symptoms and reporting a specific set of symptoms (e.g. ‘Report to the system as if you have pain in your chest’). Similarly, clinicians were asked to complete specific tasks such as looking up provided patients, reviewing a patient's symptom history and onboarding new patients using the dashboard. The goal of these scenarios was to capture the manner in which the participant interacted with the system in various situations, allowing for the isolation of key areas for improvement. Specifically, both the patient- and clinician-facing systems were assessed in terms of perceived complexity, consistency, learnability and user confidence. Usability sessions took place at UHI and lasted between 30 and 60 minutes for patient participants and between 20 and 45 minutes for clinician participants. All participant interactions with the system were video recorded for subsequent analysis by the research team. For the patient interviews, an interpreter capable of speaking English, Luganda and Runyankole was present to allow patients to participate and interact with the system in their language of preference. Patients that were accompanied by a caregiver were given the option of (a) using the system themselves or (b) having their caregiver use the system on their behalf.
Results
Phase 1: Ideation
Detailed results of both the scoping review and mixed-methods research amongst HF patients and clinicians at UHI are summarized elsewhere.12, 19 Table 1 correlates the key findings that emerged in this formative research with the associated design principles that were formulated to guide the development of Medly Uganda.
Summary of design principles for Medly Uganda.

HF: heart failure; USSD: Unstructured Supplementary Service Data.
Phase 2: Design and development
Overview of Medly Uganda
Guided by the design principles and consistent feedback from a multidisciplinary team, an iterative process was used to develop, refine and contextualize a digital health intervention named Medly Uganda. The digital health intervention is accessible to HF patients using any mobile device (i.e. smartphone or non-smartphone). Patients can dial into Medly Uganda using a USSD code and subsequently respond to a series of yes-or-no questions pertaining to their HF symptoms. Patients are asked to complete this symptom questionnaire on three pre-specified mornings per week. Upon receiving the patient's symptom data, the system autogenerates self-care advice and/or educational information that is immediately sent to the patient via an SMS message. By sending this advice in a separate SMS message (as opposed to including it at the end of the temporary USSD interaction), the patient can refer back to the provided information as necessary. For patients reporting symptoms in keeping with potential decompensation, the system also sends an SMS message to an assigned clinician containing a brief summary of the patient's symptoms and a number at which the patient can be reached. The clinician can then review the patient's demographic information, previous symptom reports and past clinician notes in a web-based dashboard, either on their computer or smartphone. After reviewing the patient's file, the clinician can call the patient to discuss their symptoms and subsequently decide whether a visit to the clinic is necessary, or whether the patient's issue can be managed remotely. Figure 2 offers a high-level overview of the Medly Uganda system.

Overview of Medly Uganda.
Patient-facing system
The patient-facing portion of Medly Uganda involves a symptom questionnaire and tailored self-care advice, both of which are guided by an inbuilt algorithm. The decision-tree algorithm was designed to take responses to a symptom questionnaire as input, and return appropriate self-care advice and/or educational content based on the inputted symptoms. The algorithm also uses the reported symptoms to triage the patient with a current disease state. The algorithm was initially based on the Medly system currently deployed in Canada, 17 with modifications being made to contextualize the algorithm based on feedback from our Ugandan colleagues. After applying an iterative design process, the final algorithm includes seven yes-or-no symptom questions and six potential disease states (see online Appendix S1). Based on symptom responses, patients can be triaged as either low risk, moderate risk, moderate risk with fluid overload, high risk, high risk with fluid overload or critical. Each of these disease states corresponds to a specific self-care message that is sent to the patient. Patients triaged as low risk receive one of several educational messages rooted in the various domains of HF self-care. 22 Moreover, moderate- and high-risk disease states trigger a second message that is sent to a clinician for potential follow-up.
To access the symptom questionnaire, patients dial a USSD code on their mobile device (e.g. *123#). Upon accessing the system, patients are asked to enter a four-digit password that they set during their registration to the system. Upon entering the correct password, the user is presented with a series of symptom-related questions in the language that they selected during the registration process (i.e. English, Luganda or Runyankole). In situations where a patient forgets their password, they can contact technical support to reset their password. Similar to USSD-based mobile money services commonly used in Uganda, patients can then respond to the yes-or-no questions using the keypad on their device. Specifically, patients are asked to respond with ‘1’ for Yes, ‘3’ for No or ‘9’ to repeat the previous question. The selection of numeric responses that are physically separated on the keypad (e.g. 1, 3 and 9) minimizes the risk of an accidental entry of the wrong response. Once the patients complete the questionnaire, the USSD session is terminated and an SMS message is sent to their device containing tailored self-care advice. Figure 3 demonstrates two screens in the USSD workflow as well as the resulting SMS message.

Simulated screenshots of the USSD workflow and resulting SMS message.
To operationalize the above interaction between the patient and Medly Uganda, an open-sourced software entitled RapidPro was used. RapidPro was chosen over similar platforms due to the ease with which modifications could be made to the system, its compatibility with Ugandan USSD channels and its previous use by collaborators at UNICEF and the Uganda Ministry of Health for their USSD-based FamilyConnect system 21 into which Medly Uganda was being integrated. Using RapidPro, a digital health system was developed comprising two components. An interaction with the system begins with a USSD workflow (i.e. the symptom flow), where patient responses to the symptom questionnaire and the developed decision-tree algorithm are used to determine the patient's disease state on a given day. Completion of the USSD flow then triggers the start of an SMS workflow (i.e. the message flow), where the system uses the determined patient disease state to send the appropriate SMS message(s) to the patient and clinician (if required). A high-level overview of this workflow is shown in Figure 4.

Overview of RapidPro system.
A final consideration that is integrated into the patient-facing system is adherence reminders. Instead of prompting every patient three times per week, the RapidPro system automatically sends SMS reminders to patients who have not reported their symptoms by midday on days on which a symptom report is expected.
Clinician-facing system
The clinician-facing system comprises autogenerated SMS alerts sent directly to the clinician's mobile device, as well as a web-based dashboard accessible from the clinician's smartphone or computer. The SMS alerts are triggered in response to a patient-submitted symptom report that is triaged as either moderate or high risk. These SMS messages include a brief overview of the patient's symptoms, as well as a phone number at which the patient can be reached. The phone number can also be used to query the patient's file in the web-based dashboard.
The web-based dashboard is a simple and secure platform that enables clinicians to access additional information relating to their presenting patient. The web application uses React JavaScript library for the front end, Express JavaScript library for the back end and PostgreSQL for the database. The application is hosted using the cloud platform Heroku, while the PostgreSQL database is stored on a cloud server hosted by UHI. Clinicians access the web application by navigating to a UHI-hosted web address on their internet-enabled device. After entering their credentials on the home page (Figure 5(A)), the clinician is provided with the option of querying their patient using a phone number, browsing all of their patients by name or adding a patient to the system (Figure 5(B)). Adding a new patient requires simple demographic information including a name, phone number, date of birth, sex and preferred language (Figure 5(C)). A clinician may also choose to add credentials that will allow another clinician to access the system (Figure 5(D)). If the clinician queries a patient using the patient's phone number, they will be taken directly to the patient's file. If they choose to browse all of their patients, they are taken to a page where they can search patients using their first name, last name or phone number (Figure 5(E)).

User interface for clinician dashboard as seen on a smartphone.
Once the clinician has accessed a specific patient file, they will see simple demographic information at the top of the page, a panel summarizing the patient's symptom history (Figure 5(F)), a panel including clinician notes relating to past symptom reports (Figure 5(G)) and a legend for the symbols used in the symptom history panel (Figure 5(H)). The symptom history is presented as a block chart, with the y-axis representing the various items included in the symptom questionnaire (e.g. chest pain, fainting) and the x-axis indicating the report dates. For a specific symptom question on a given date in the chart, a blue square denotes a ‘Yes’ response, a light grey square signifies a ‘No’ response and a dark grey square indicates that the corresponding symptom question was not asked on the specific date. In addition to the symptom responses, the patient's assigned status for each report is included at the bottom of the chart. Risk status is represented using a stoplight model already used by clinicians at UHI (i.e. green for low risk, yellow for moderate risk, red for high risk), with an ‘H’ being added to critical reports where the patient has been instructed to report to a hospital. To increase the accessibility of the dashboard to clinicians with colorblindness, risk status is also denoted with an increasing number of dots (i.e. 1 for low risk, 2 for moderate risk and 3 for high risk). Below the symptom history, clinicians are provided with a space to add notes for each symptom report submitted by the patient. These note fields save automatically as the clinician types, further increasing the usability of the dashboard.
Phase 3: Evaluation
Patient usability testing
In-person usability tests were performed with six HF patients and four informal caregivers at UHI. Six participants opted to use the system in Luganda, whereas four participants completed the testing in English. No users performed usability testing in Runyankole. Overall, participants were extremely satisfied with both the usability and usefulness of the intervention. There was strong agreement amongst patients that the system was straightforward, easy to learn and contextual to the user. Participants appreciated the similarities between the developed system and mobile money services with which they were already familiar. The patients also exhibited a strong interest in future use of the system as part of their daily self-care regimen. Even patients who self-identified as having low technological literacy were able to learn and use the system. For these participants, the research team allowed them to experiment with submitting different sets of symptoms until they reached a point where they felt confident that they could use the system independently at home. By the end of the usability testing, every participant indicated that they were able to reach this level of comfort with the system.
Several informative cases emerged in the usability study. For example, we found that certain participants were interested in their caregivers using the system on their behalf. One caregiver, who assisted his mother frequently but did not live with her in the village, stated that he would be willing to call his mother three times per week, and ask her the various symptom questions that would be asked by the system. He stated that he would then dial the USSD code, report the symptoms on her behalf, receive the self-care advice and call her back to discuss what the system recommended. Despite the apparent inconvenience of using the system in this manner, the son felt confident that his actions would be worthwhile given the benefits he expected from Medly Uganda.
A second interesting case involved a Luganda-speaking patient who had recently acquired her first smartphone but had accidentally left the device at home. At the time of the study, the patient described her technical capabilities on her new phone as being able to swipe between screens and to place a call. The patient agreed to complete the usability test using a smartphone provided by the research team. Despite the patient's lack of familiarity with the smartphone, she quickly became proficient at using the various components of the system. By the end of the session, she was completing the questionnaire without assistance and retrieving the self-care advice with ease. The patient appeared empowered by the fact that she could use the system independently, and even noted that she would ‘get even better’ at using the system with more experience.
Despite the overall patient satisfaction with the developed system, various usability considerations emerged in the patient testing. Most notably, the usability tests highlighted the importance of appropriate training when patients are first introduced to the system. Certain individuals, particularly those that opted to use the system in Luganda, initially had difficulty completing the USSD interaction in the allotted time. These patients often took increased time to read, comprehend and respond to the questions posed by the system. After a brief introductory discussion with the research team regarding each question, however, these patients quickly adjusted to the time requirements of the system.
Clinician usability testing
Usability tests were also performed with five cardiologists and two nurses. Clinicians reported a high degree of usability, simplicity and consistency for the dashboard. Participants also described the system as straightforward and easy to learn. Following a brief overview of the dashboard by the research team, clinicians quickly mastered the dashboard and its various functions. Based on the time taken to complete the typical interaction of logging in, querying a patient, reviewing the patient's history and subsequently recording a note, it was estimated that responding to a single patient alert could take as little as two-to-four minutes of in-dashboard interaction (i.e. not including clinician-patient telephone communication).
Qualitative assessment of the clinician usability tests helped identify important usage patterns and elements of the dashboard that limited usability. For example, clinicians would often affix a leading zero when entering a phone number into the dashboard (e.g. 0720123456); thus, the dashboard was updated to omit zeros located at the beginning of a phone number. Other minor issues included the requirement to click a patient's last name to access their file from the complete list of patients, rather than the expected functionality of clicking the row associated with their name. Again, the dashboard was modified to accommodate the expected functionality.
Discussion
This article presents the UCD and development of a digital health intervention, Medly Uganda, for HF patients and clinicians living in Uganda. Medly Uganda is designed to empower HF patients to improve their HF self-care through a simple symptom-focused questionnaire, an autonomous triage algorithm and self-care advice sent directly to the patient's device. Moreover, the system supports the remote management of HF patients by alerting clinicians to moderate- or high-risk patients and enabling clinicians to review patient information in a web-based dashboard.
The importance of self-care amongst patients with HF is well-documented in the literature, with effective HF self-care being associated with improved quality of life, reduced mortality and lower readmission rates.23–25 With Medly Uganda, we aim to improve the three domains of HF self-care described by Riegel et al.: maintenance of physiologic stability, identification of HF-related symptoms and symptom management. 22 To optimize self-care maintenance, Medly Uganda sends educational messages regarding important everyday behaviours to patients who – based on the inbuilt algorithm – have been triaged as stable (or low risk). Identification of HF-related symptoms is facilitated through symptom questionnaires that prompt patients to regularly reflect upon the physical signs of HF and their physiologic relevance. Finally, self-care management is encouraged through tailored and timely self-care advice specific to the symptoms and disease state elicited from the questionnaire on a particular day. By strategically targeting each of the key areas of HF self-care, we are hopeful that Medly Uganda will enhance self-care efficacy amongst Ugandan patients with HF in the future.
The strengths of the presented intervention are numerous. The UCD process enabled the development of a contextualized system designed specifically to address patient- and clinician-raised concerns regarding HF management in Uganda. This end-user input informed several major design characteristics, such as the use of the USSD platform, the focus on addressing information needs amongst patients and the semi-autonomous nature of the eventual design. Similarly, the iterative feedback elicited from Ugandan patients and clinicians led to fine adjustments that optimized system usability, such as rephrasing questionnaire items to align with locally accepted terminology (on the patient side), as well as adding the ability to query patients by both phone number and name (on the clinician side). The involvement of Ugandan HF patients and clinicians at all stages of design and development will also help support the adoption, acceptability and scalability of Medly Uganda in the long term.
Several potential benefits are also associated with the autonomous triage algorithm. The autonomous nature of the algorithm will enable clinics to efficiently manage a larger number of HF patients. By autonomously triaging patients in terms of their risk status, clinics can prioritize the care of high-risk patients while continuing to remotely monitor individuals that remain asymptomatic. This triage system presents potential benefits towards clinic operation, as it should reduce the number of unnecessary visits to the clinic and increase availability for patients with acute concerns. An additional strength of the algorithm is the potential impact that the resulting self-care advice will have on patient quality of life. When patients are triaged as low risk, they will receive positive reinforcement to maintain their current self-care behaviours. When a patient has signs of decompensation, they will be reassured through tailored self-care advice and timely intervention by their care provider (if required).
An additional strength of Medly Uganda is that the patient-facing portion of the system harnesses a technology that is both familiar and accessible to Ugandan HF patients. The USSD platform is ubiquitous in Uganda as a result of its use in local mobile money services. Our formative research amongst the HF population at UHI found that a significantly larger proportion of patients identified as comfortable using their phone for mobile money services when compared to both SMS-based services and interactive voice response systems. 19 Because USSD is compatible with any network-enabled device (i.e. smartphone or non-smartphone), the platform is accessible to individuals with varied economic means. USSD also enables the system to be provided to patients free of charge, as USSD-associated costs are incurred by the service provider. Accordingly, the USSD-based design increases both the familiarity and accessibility of the intervention to HF patients in Uganda.
The final strength of the design is the sustainable and collaborative approach that was used in all phases of development. In addition to the aforementioned involvement of HF patients and clinicians, early stakeholder engagement with UNICEF and the Uganda Ministry of Health provided crucial support in the development and deployment of the intervention. As UNICEF had already deployed a government-endorsed USSD-based system for pregnant and postpartum women entitled FamilyConnect (based on the South African MomConnect), 21 we were able to leverage a breadth of experience and infrastructure to realize Medly Uganda. Moreover, the ongoing collaboration with UHI, Makerere University and the Uganda Ministry of Health will help to further solidify the long-term acceptability of Medly Uganda amongst key stakeholders.
Despite its promise, the Medly Uganda system is not without limitations. In its current form, the developed system requires patients to have access to a mobile device. Though our preliminary research indicated that 98% of patients at UHI have access to a mobile device with 89% owning their own device, 19 we acknowledge that the minority of patients without a mobile phone will be unable to access the system. Access may also be limited by patient literacy levels and technological capabilities. Our formative research suggested that nearly 30% of patients at UHI self-identify as illiterate; 19 however, we attempted to mitigate the effect of this limitation by offering the service in three local languages. Given that our preliminary data indicated USSD was a trusted communication modality amongst our participants, we developed Medly Uganda within a USSD-SMS hybrid platform. 19 A future innovation to the design could include the option for an interactive voice response system for patients unable to engage with the current USSD-based system. Another possible concern regarding the system design is the risk of health-related information (i.e. self-care advice) being stored on a personal (or shared) mobile device. To lessen the impact of this drawback, we ensured that all self-care messages were devoid of identifying information and encouraged users to only register with a mobile device that they felt to be secure. An additional limitation is the time restriction placed on a USSD interaction, which can vary between 90 and 180 seconds depending on the cellular provider. Though our usability testing suggests that most patients will be able to complete the seven-item questionnaire in the allotted time, this time constraint could prohibit some patients from effectively submitting their symptoms. The final potential limitation of the system is that responding to patient alerts could eventually become burdensome for the assigned clinician(s) as the number of patients using Medly Uganda increases. We expect that the semi-autonomous design should mitigate this final limitation; however, it is possible that designated staff members will eventually be required to remotely manage the Medly Uganda users. Such implementation and service design considerations will be addressed in upcoming phases of validation and deployment.
Medly Uganda is currently being tested in a pilot hybrid implementation/clinical effectiveness trial amongst HF patients and clinicians at UHI. This pilot study will shed light on technical and human resource challenges involved in deploying and managing the system. It is important to recognize that we have designed the Medly Uganda system alongside a population of patients based at UHI, where access to care is relatively more available than more remote regions across Uganda. Therefore, our future work will build upon the results of this pilot trial with the goal of broadening the geographic and sociodemographic reach of the system through further collaborations with nursing stations throughout Uganda. As a long-term goal, we also hope to expand the scope of chronic conditions that can be managed using Medly Uganda.
Conclusions
Ugandan HF patients and clinicians stand to benefit from digital health interventions that enable patients to better care for themselves. We used a UCD process to develop a USSD-based self-care intervention named Medly Uganda that allows HF patients to report daily symptoms, receive tailored treatment advice and connect with a clinician when showing signs of decompensation. Usability testing showed Medly Uganda to be acceptable and feasible amongst clinicians, patients and caregivers. As we move towards the deployment of Medly Uganda, we are hopeful that the system will improve self-care efficacy amongst HF patients in Uganda.
Supplemental Material
sj-png-1-dhj-10.1177_20552076221129064 - Supplemental material for A digital self-care intervention for Ugandan patients with heart failure and their clinicians: User-centred design and usability study
Supplemental material, sj-png-1-dhj-10.1177_20552076221129064 for A digital self-care intervention for Ugandan patients with heart failure and their clinicians: User-centred design and usability study by Jason Hearn, Sahr Wali, Patience Birungi, Joseph A Cafazzo, Isaac Ssinabulya, Ann R Akiteng, Heather J Ross, Emily Seto and Jeremy I Schwartz in Digital Health
Footnotes
Acknowledgements
The authors would like to acknowledge the patients, caregivers and clinicians that participated in the co-development of Medly Uganda. We would also like to thank Rebecca Gillman for her thoughtful review of this manuscript.
Contributorship
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All research activities were approved by the Uganda National Council of Science and Technology (HS 2364), the Makerere University School of Medicine Research and Ethics Committee (REF 2017–076), the University Health Network Research Ethics Board (ID# 14-7510) and the Yale Human Research Protection Program (ID# 2000025338).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ted Rogers Centre for Heart Research, Wolfond Chair in Digital Health, Fogarty International Center (grant number R21TW010998-01A1).
Guarantor
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.