
Abstract
Background
The use of immersive virtual reality, wearing head mounted display, has recently increased for people with chronic pain, with no definitive conclusion of its efficacy on pain-related outcomes.
Objective
To map the available evidence on the use of immersive virtual reality as intervention for adults with chronic primary pain, illustrating gap in knowledge and direct future research.
Methods
The search was performed with a range of study designs, but only those written in English language. A search was created in CINAHL Plus, Medline, AMED, Embase, PsycINFO, ASSIA, Scopus, TripPro, CENTRAL and EmCare.
Results
Thirty-two studies were included. Several chronic conditions were identified including chronic musculoskeletal pain and fibromyalgia. The immersive virtual reality mechanisms included distraction, physical exercises, mindfulness/biofeedback, graded exposure, hypnosis, neuromodulation, and multi-mechanisms, and all these mechanisms were associated with varied dose. The use of customised software, with wide range of head mounted displays were common in clinical setting with some degree of supervision. Motion sickness, head mounted display discomfort and technical issues affect the usability of immersive virtual reality leading to poor engagement and dropouts.
Conclusions
The use of immersive virtual reality for chronic primary pain is in early stages with lack of consensus regarding the mechanisms and associated dose. Future research needs to address the need of customisation, clinical usability of head mounted display as well as safety strategies to enhance the uptake of immersive virtual reality technology in healthcare practice.
Introduction
Chronic pain (CP) is one of the primary causes of disability worldwide.1,2 CP is defined as the pain lasts or recurs for more than 3 months. 3 The recent definition of pain in 2020 by the International Classification of Disease (ICD-11) classified CP into chronic primary pain (CPP) and chronic secondary pain (CSP) based on the etiology of pain. 3 CPP is labelled as a disease which associated with emotional distress and functional impairment that cannot be described by another chronic condition, while CSP is defined as a symptom which is caused by underlying disease or injury. 3 Acknowledging the complexity inherent in the treatment of CPP as a disease, the National Institute for Health and Care Excellence (NICE) recommended pharmacological and non-pharmacological interventions including physical exercises and psychological therapy. 4 Although a wide range of non-pharmacological intervention have been supported, limited access to multi-disciplinary rehabilitation and lack of providers remain challenging.4–6 Further, the harmful effect of pharmacotherapy encourage exploring alternative interventions. 4 Thus, promising new pain management strategies such as virtual reality (VR) have emerged. 7
VR is a technology system that enables users’ interaction with computer-generated virtual environment (VE). 8 The system setup produces multi-sensory experience (e.g., visual, auditory, and haptic) to create ‘sense of presence’, described as an illusion of being in virtual world.8,9 Depending on the system sensory inputs and user's isolation from real world, VR is divided into non-immersive (non-IVR), semi- immersive (semi-IVR) and fully immersive (IVR). 10 In non-IVR and semi-IVR, the users interacted with the two-dimensional VE through computer desktop and large monitors, respectively, to visualise the real world outside the screen. 10 on the other hand, Immersive VR delivers three dimensional VE, enveloping user's view with head mounted display (HMD), generating full immersion and high sense of presence.11–14 The utility of VR as an intervention in pain conditions has significantly increased over the last decade with 39.8% in acute pain and 34.3% in CP conditions.8,14 Distraction was hypothesised to be the leading mechanism underlying the analgesic effect of VR, attributing analgesia to occupying attention, emotion, and memory resources and blocking the pathway of pain stimuli.15,16 Whilst the distraction mechanism is aligned with short-term pain relief, VR assumed to induce analgesia in CP conditions through neuroplastic changes in brain regions with long term use. 17
The efficacy of VR as an analgesic tool has been strongly supported across several reviews in acute pain settings, such as burn care, dental procedure and other related medical procedure and it has been recommended as a non-pharmacological intervention for pain management.13,18–22 However, recent systematic reviews between 2019–2022 reported that no definitive conclusion can be drawn about the efficacy of VR on pain, function, mental health or disability in CP conditions.23–30 This was recently emphasised in 2023; an umbrella review discussed that VR can effectively reduce acute pain during medical procedures, but it appears to be insufficiently effective for CP. 31 The lack of consensus about the effect of VR in CP management has been attributed to heterogenous application of VR associated with different methods, type of VR software or hardware, dose and the measured outcomes.24,25,28–30
The heterogenous nature of VR field in CP management indicates the gap in knowledge and lack of consistency in the body of evidence. Therefore, we conduct a scoping review, which is practically relevant design when the literature has heterogenous nature to address the gap in knowledge and direct future research. 32 This review aims to explore the use of IVR in adults with CPP, identifying patient characteristics, the underlying IVR mechanisms, intervention characteristics, setting and adverse effects. These aspects have not been explored in previous reviews, yet they are crucial to address the gap in IVR application and identify relevant key factors. While other reviews included a range of non-immersive and immersive technology, this review focuses on immersive technology (IVR) using portable and easy-to-set up (HMDs) for adults to highlight promises and inform future research.
Methods
Review design
This scoping review was conducted following the recommendations of Arksey and O’Malley32 and Levac et al. 33 The recommendations consist of five stages: 1) Clear identification of the review question, 2) Identifying relevant studies, 3) Eligibility criteria for the study selection, 4) Data charting, 5) Summary and report of the results. These recommendations were followed to map the literature and achieve overall results. In accordance with PRISMA guidelines, a checklist of essential items has been included (Supplementary File 1). 34 Ethical approval and consent are not applicable, as this article does not involve any human or animal subjects.
Stage 1: identifying the review question
To align with the aim of this scoping review, the review question is: How has immersive virtual reality (IVR) been utilized as an intervention for adults with chronic primary pain (CPP)?
Stage 2: identifying relevant studies
The search strategy was adapted with consultation of health science librarian and research team. The terms and keywords of search were adapted from previous VR literature and ICD-11 classification of CP 3 (see example in Appendix 1). The studies were extracted between February 2023 and May 2023 from the following databases: CINAHL Plus, Medline, AMED,Embase, PsycINFO, ASSIA, Scopus, TripPro, CENTRAL and EmCare. All studies were exported into Mendeley (version 1.19.8), and duplicates were removed. Additionally, manual search of reference lists within systematic reviews was performed.
Stage 3: eligibility criteria
The selection criteria were restricted to full text, English language articles with no date limitations. Studies including adults greater than 18 years old, with CPP as defined by ICD-11 (i.e., pain lasting more than 3 months including chronic musculoskeletal pain, widespread CP, and chronic visceral pain) or non-specified CP were eligible. Studies in which the effect of IVR was evaluated in healthy participants, acute pain or CSP were excluded. For the IVR intervention, studies which use HMD to view three dimensional VE were included, while those who use non-IVR to view VE on a computer screen or projector were excluded and these included video games, Nintendo Wii, Xbox, PlayStation for example. Studies that did not use IVR as intervention or measure the effect on CPP were excluded. There were no restrictions in the outcomes that were used. To aid the scope of the literature and direct future research, all experimental designs were included (e.g., feasibility, pilot studies, RCT, pre-post trails, case serious, single case study). Study protocols, reviews or conference abstracts were deemed not suitable for inclusion. Two reviewers independently screened the titles and abstracts to identify relevant studies based on the eligibility criteria. A discussion meeting was held including all the research team to decide on the full text. Discrepancies were discussed between reviewers to reach final agreement on the study selection.
Stage 4: data charting
All relevant information was extracted and synthesised, as follows:
Article details: author, publication year, country, study design. Sample size, characteristics of patients (age, type of CP condition, specific exclusion criteria). Mechanisms and the effect on all relevant intended outcomes. IVR Intervention characteristics including software, hardware, and dose of the intervention (i.e., number of sessions, duration, and frequency). Comparator intervention if found. Setting of the intervention (e.g., hospital, home) Adverse effects.
Stage 5: summary and report of the results
The summary and the report of the results included numerical counts of the studies. In addition, the included studies were analysed to see if any information was reported to have a negative/positive effect within the intervention to give meaning to the summary results presented and direct future investigation.
Results
The literature search identified 1975 references of which 896 were screened for relevance after duplicates were removed. Seventy-four relevant studies were eligible for full text inspection. From these, 42 studies were excluded because they used non- IVR, or did not indicate the type of pain as acute or chronic, or included only chronic neurological underlying condition. Thirty-two studies were included in this scoping review. Figure 1 presents the flowchart of study selection, following PRISMA guidelines 35 and Figure 2 presents the summary findings of this scoping review.

PRISMA flow chart for study selection 35 .
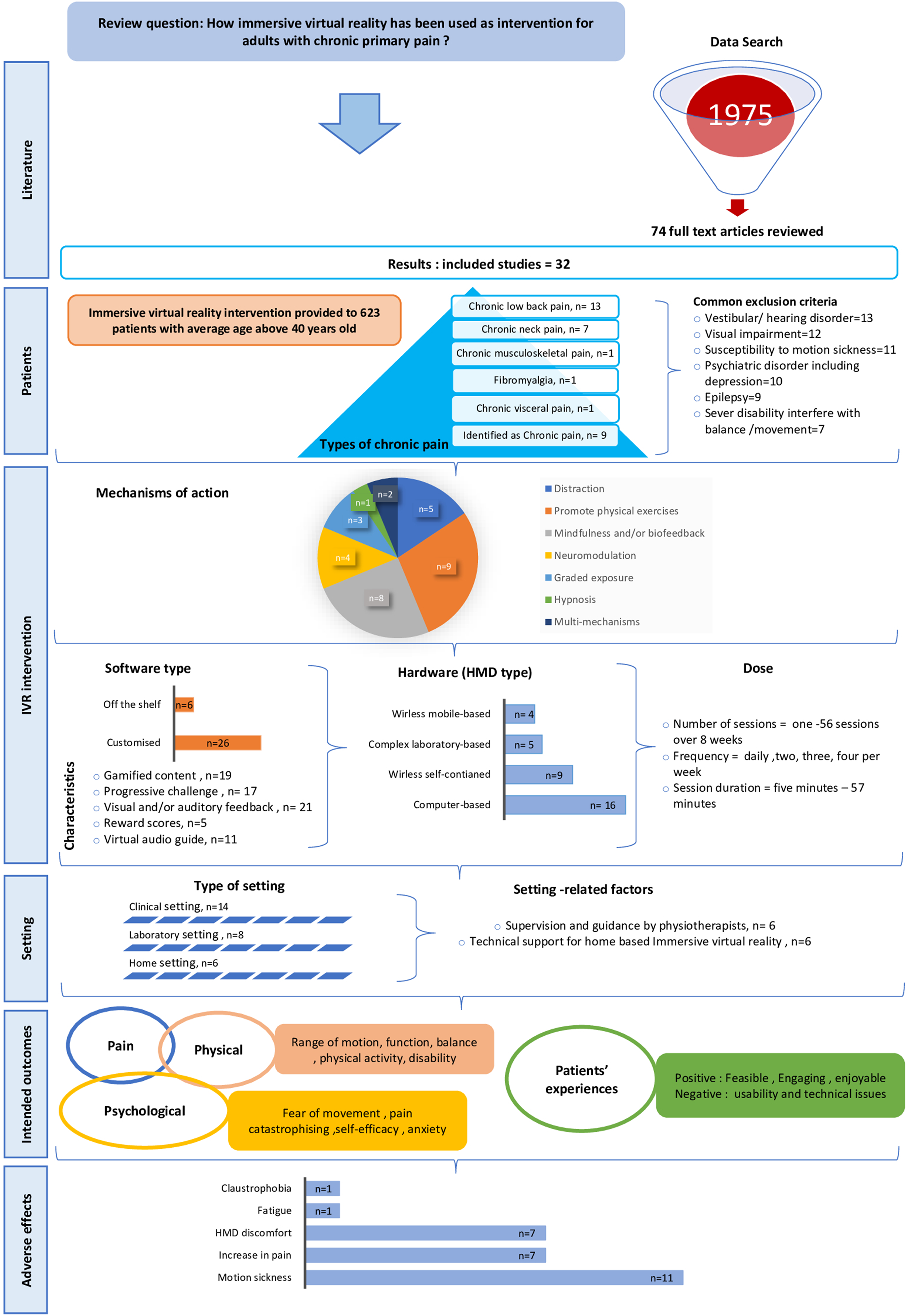
Summary of the key findings.
Study characteristics
The included studies were mostly conducted in United States of America (USA) (15/32) and as pilot or feasibility studies (15/32) (Table 1). There were 19 controlled study design of which were randomised control trials (RCTs)36–51 with two controlled trials52,53 and one RCT of cross over design. 54 In the controlled trials, the IVR in the intervention was compared to either standard rehabilitation,36–39,46,48,49,51,52,54,55 sham VR (HMD with two dimensional video),41–45 audio intervention50,51 or had control groups with no intervention.40,45,47,48 Study designs also include seven pre-post trials,55–61 five case studies62–66 and one randomised cross over. 67 Alongside side the experimental data, four studies present qualitative data on patients’ experiences and suggestions to improve IVR system.48,55,57,67
Study characteristics including authors, year, country, design, comparator and characteristics of patients.

N. n
Patient characteristics
The studies included 1037 patients, with 623 patients receiving IVR intervention (Table 1). More than half of the studies involved patients with average age above 40 years old, with two studies46,47 purposely evaluating the effect of IVR intervention on older adults (over 60 years old). Twenty-two studies were conducted on specific clinical conditions including chronic low back pain (CLBP) (13/32),40–47,58,59,62–64 chronic neck pain (CNP) (7/32),36–39,55–57 chronic musculoskeletal pain (1/32), 48 fibromyalgia (1/32), 49 chronic visceral pain (1/32). 65 The remaining nine studies were conducted on conditions identified as having non-specific CP (Table 1).50–54,60,61,66,67
There were common exclusion criteria of CPP conditions noted across studies including susceptibility to motion sickness (11/32),41–46,54,56,62,66,67 epilepsy (9/32),37,41–45,56,64,66 vestibular or hearing disorder (13/32)36–39,41–44,46,49,55,60,64 and visual impairment (12/27).40–44,46,47,49,56,58,60,64 Also, other studies excluded patients who reported to have psychiatric disorder or severe symptoms of depression (10/27)41–45,48,56,57,61,64 as well as those with medical condition or severe disability that interfered with movement and /or balance in CNP, CLBP and fibromyalgia (7/27) (Table 1).36–38,45,46,49,59
Mechanisms of action and associated effect on the intended outcomes
Six distinct mechanisms of action (see details Appendix 2) were employed in the identified studies including distraction (5/32),52,54,60,66,67 promotion of physical exercises/activity (9/32),36–39,47–49,55,57 mindfulness and/or biofeedback (8/32),41–44,50,51,53,64 neuromodulation (4/32),56,58,62,63 graded exposure (3/27),40,59,61 hypnosis (1/27) 65 as well as multi-mechanisms (2/27).45,46
Distraction. Five studies utilised distraction, focusing on alleviating pain during and/or immediately after using IVR. It was argued that IVR distraction could have the potential to work as an alternative to opioids to control acute episodes associated with CP. Two types of distractions were implemented: active distraction which required patients to play interactive games, while passive distraction immersed patients in 3D relaxing VE without interaction. A single session of passive distraction by Wiederhold et al. 52 for 15 min revealed significant reduction of pain and stress level only during IVR. However, Jin et al., 54 Jones et al., 60 and Amin et al., 67 asked patients to play interactive games called ‘Cryo-slide’, ‘Cool’, ‘In-Mind’ for 5, 10 and 10 min respectively. These distraction games reduced the pain significantly during a single session of IVR, but the analgesic effect continued immediately after the session only in two studies.60,67 Both passive and active distractions were delivered by Garrett et al. 66 using relaxing games, and interactive (exploring VE and puzzle games) for 30 min over 4 weeks. However, no significant pain reduction was seen after 6 h, 24 h or after 4 weeks.
Promote physical exercises/activity. Nine studies integrated IVR with motor control, mobility/balance exercises and general physical activity, arguing that IVR gaming motivate patients to practice exercises.36–39,47–49,55,57 Six studies utilised VE that enable patients with CNP to practice motor control exercises such as range of motion (ROM), sensorimotor (SM) and stability exercises as well as head-eye movement control.36–39,55,57 Being immersed in VE was assumed to distract patients from pain and induced visual feedback of neck movement which was proposed to enhance performance of the neck control exercises. Two subsequent studies by the same research group utilised gamified VE as adjunct, where patients controlled the virtual airplane using neck movement to practice kinematic training exercises (ROM, accuracy, velocity, stability) over 4 weeks.36,37 Some advantages were seen by Sirag-Bahat et al. 36 in pain and disability after 4 weeks and by Sirag-Bahat et al. 37 in pain, ROM, and some kinematic measures (accuracy, velocity) after 4 weeks and 3 months follow up. However, IVR showed no significant differences compared to conventional kinematic training using laser pointer.
In Tereja et al., 39 the use of two gamified VE to train cervical ROM revealed significant reduction in pain, neck rotation, disability, catastrophizing and anxiety post 4 weeks, 1 month, and 3-months follow-up. Although this improvement was not statistically significant when compared to standard ROM exercises, IVR showed significantly greater improvement in FOM in 3 months follow up. 39 Three studies38,55,57 investigated the effect of IVR as an adjunct to standard rehabilitation (SR), using VE, where a virtual object controlled by neck movement to practice SM exercises. Nusser et al. 38 reported that 6 IVR sessions showed significant increase in neck flexion/extension compared to standard SM and SR, however, no significant differences were seen in pain, FOM or disability. Similarly, Zauderer et al. 55 found no significant change in pain, ROM, disability following 5 sessions or in 3 months follow up. In Glavare et al., 57 the use of IVR over 6 weeks showed significant improvement in FOM, depression and quality of life (QOL) with no significant change in pain, disability, or anxiety.
In addition, two studies by Yalfani et al. 47 and Gulsen et al. 49 utilised gamified VE to practice mobility/balance exercises over 8 weeks in patients with CLBP and fibromyalgia, respectively. Yalfani et al. 47 utilised eight IVR games as a stand-alone intervention, showing significant reduction in pain and improvement in QOL compared to no intervention. However, Gulsen et al. 49 delivered two IVR games as adjunct to aerobic/Pilates exercises and reported a significant improvement in pain, FOM, fatigue, physical activity level and QOL compared to aerobic/Pilates exercises alone. Tuck et al. 48 evaluated the effect of IVR over 6 weeks, utilising 10 IVR games that induce general body movement. The IVR effect was superior to no intervention with moderate change in pain intensity and daily activity (e.g., number of steps, walking), but was equivalent to the standard rehabilitation. 48
Mindfulness and /or biofeedback. Eight studies examined the effect of IVR using mindfulness and/or biofeedback.41–44,50,51,53,64 In Gromala et al., 50 the VE called ‘Virtual Meditative Walk’ was employed as a relaxation tool and was found to bring about a significant pain reduction after a single session. In contrast, IVR was utilised as a coping skills tool to deliver mindfulness and biofeedback in Darnall et al. 51 and Gracia et al., 41 biofeedback in Jones 53 and mindfulness in de Vries et al. 64 The VE of Darnall et al. 51 and Gracia et al. 41 included pain education, mindfulness, relaxation, and biofeedback training of breathing exercises (Appendix 2). Darnall et al. 51 reported that daily IVR sessions over 3 weeks resulted in greater reduction in pain, pain interference (with mood and sleep) compared to audio instructions, and both had significant improvement in pain self-efficacy and catastrophising. Gracia et al. 41 results agreed in part and revealed that daily IVR sessions over 8 weeks produced significantly greater reduction in pain, pain interference (with activity, mood, stress) and improvement in physical function and sleep disturbance compared to sham VR (two dimensional VE), but no change in pain self-efficacy or catastrophising was shown in either group.
The research group of Gracia et al. conducted other studies to follow up the effect of IVR at three, 42 six 43 and 18 months. 44 These studies showed sustained reduction in pain intensity, pain interference (with activity, sleep, and stress) compared to sham VR over three, six and 18 months.42–44 Pain interference with mood showed sustained reduction in three and six months, but not greater than sham VR.42,43 The improvement in physical function was sustained at three and six months compared to sham VR,42,43 but equal improvement was shown in 18 months. 44 Sleep disturbance had no significant change at three months, 42 but improvement was shown in six and 18 months.43,44 The study by Jones 53 utilised VE called ‘Pain care’ to learn relaxation using biofeedback of breathing exercises and gave patients the freedom to explore ‘off the shelf’ games with no prescribed dose over four weeks. Although Jones 53 showed significant reduction in depression and catastrophising, no change was found in pain interference with activity. The recent study by de Vries et al. 64 used ‘Reducept’, a developed IVR containing five VE (Appendix 2), focusing on pain education and visualisation to control pain through breathing, mindfulness and changing negative thoughts. The five IVR sessions over 4 weeks showed significant pain reduction and increase in active coping strategies, however, no change was found in FOM, pain catastrophising, psychological compliant and QOL. 64
Hypnosis. One study employed IVR in 2 sessions for a single patient diagnosed with chronic visceral pain. 65 The VE which consists of hypnotic suggestions to feel relaxed, breath comfortably and think positively, reduced pain and anxiety significantly post 1 h of the 1st and 2nd session. 65
Neuromodulation. Two IVR technology advancements were reported in four studies: virtual embodiment62,63 and visual manipulation,56,58,63 which are believed to enhance analgesic effect through neuroplastic changes within the brain processing system. Virtual embodiment is the perception of owning a virtual body by giving an illusion that the real body is being replaced by a virtual avatar and technology sensors allow movement coordination of the real and virtual body.62,63 In visual manipulation, the visual feedback of a virtual body can be altered in shape or range of movement.56,58,63 The study by Trujillo et al., 62 involved CLBP patients in a game that facilitated lumber flexion, extension and rotation while embodying a virtual hand and another game that encouraged anterior, posterior, and lateral pelvic tilts while embodying the back region and found significant pain reduction after each of the 7 sessions. Another VE utilised by Harvie et al. 63 for CLBP patients was to play 3 different games while embodying head and hand movement in a visually manipulated athletic avatar (i.e., boxer, superhero, rock climber) which was assumed to improve distorted body image (i.e., reduced perceived strength, and the sense of body vulnerability). The body image and pain self-efficacy improved significantly after 4 weeks and at 3 months follow up, with great reduction in disability in the 3 months follow up. 63 There are two studies utilising visual manipulation, implemented games developed for CNP 56 and CLBP 58 to visually manipulate feedback of the neck and back rotations respectively, by giving an illusion of lesser degree (45 degrees) within VE, while performing larger degree (50 / 90 degrees) in the real world. Although the after effect on pain, rotation and FOM was not measured, the rotations of neck and back were increased with manipulated visual feedback.56,58
Graded Exposure. Three feasibility studies utilised IVR that adopted the graded exposure mechanism to gradually expose patients with CLBP to movement, aiming to reduce FOM.40,59,61 Thomas et al. 40 assessed the effect of ‘Dodgeball game’ which was designed to catch or block a virtual ball to enhance lumber flexion gradually of 15, 30 and 60 degrees within 3 sessions. Although lumber flexion increased during the game, no change was shown in pain, FOM or lumbar flexion after the sessions. In contrast, a hierarchy of games was built and rated by Fowler et al. 61 and Hennessy et al. 59 to provide graded challenges starting from low intensity, moving to medium intensity, and ended with high intensity. Fowler et al. 61 examined the effect of daily IVR using mindfulness (low intensity) and gradually progressed to game required head/neck movement (medium intensity) and upper limb/ trunk movement (high intensity) over 3 weeks which resulted in significant improvement in pain, pain interference with mobility, pain catastrophising, and function, but no change was seen in FOM. Hennessy et al. 59 developed ‘Lucid’ game to practice functional activities of reaching, bending, and carrying weights during walking on treadmill, where each activity increased in difficulty progressively over 3 sessions. Although the validity of the hierarchy was supported by the included patients with significantly higher avoidance and pain expectancy of the high intensity game compared to the low intensity one, no change was found either in pain or in FOM after exposure. 59
Multi-mechanisms. Recent IVR integrated two different mechanisms within VE for patients with CLBP aiming to reduce fear and increase level of physical movement.45,46 Stamm et al. 46 delivered multi-model VE, including 12 physical exercises (i.e., warm up, core strengthening exercises, core stretching exercises and stretching exercise for cool down) as well as psychoeducation (pain physiology, management of pain and stress) and reported significant improvement of function after 4 weeks, but no change was detected in pain and FOM. Eccleston et al. 45 designed an embodied VE consisting of 24 tasks based on behaviour change principles including goal setting, goal-value discrepancy, pacing, homework setting in real world, reflection on movement and reward which change every 5 days over 8 weeks. A virtual mentor guided the patients through two VE: ‘inside space’, where patients were instructed on problem solving tasks, social and cognitive difficulties, pain and avoidance behaviour, and ‘outside space’ where they were encouraged to play fruit picking game while embodying virtual hand to accomplish a set of pre-defined fearful movement by the research group that increases in intensity and range upon accomplishment. 45 Pain, FOM and disability significantly improved after 8 weeks and 3 months follow up, with superiority of IVR in disability and FOM compared to sham IVR and no intervention within 8 weeks. 45
IVR intervention characteristics
In Appendix 2, the details of intervention characteristics including software, hardware and dose were shown.
Software. Customised software (26/32) was commonly implemented.36–46,49–51,53–60,62,64,65,67 Alternatively ‘off the shelf’ software was rarely used (6/32).47,48,52,61,63,66 Most software shared the following features: gamified VE (19/32),36,37,39,40,45–49,54,56,58–63,66,67 progressive challenge of different forms including the range of movement, speed, direction, duration, and complexity of the exercises and/or skills (17/32),36–45,47–49,57,59,61,62 visual and/or auditory feedbacks including biofeedback on breathing rate (21/32),36,37,39–45,47,49–51,53,54,56–58,60,62,67 reward scores (5/32),40,45,49,54,62 and virtual audio guide (11/32).41–46,50,51,53,64,65The gamification with the progressive challenge, visual feedback and rewards on task completion were reported to be a positive factor in patient motivation.39,45,47,48,57 Additionally, eight studies personalised the progressive challenge in level of movement or skills, and exercise duration to individual patient performance.36–38,41–44,49,57,61,62 A virtual audio guide was integrated to guide patients through VE and instruct them on the required tasks, mainly in the software for mindfulness and/or biofeedback, pain education and hypnosis.41–46,50,51,65 A virtual audio in Eccleston et al. 45 guided the patients to explore VE, offered pain education and behavioural instructions as well as reinforcement cues and rewards.
Hardware. The type of HMDs was varied including non-wireless (computer-based and laboratory-based) and wireless, either with or without interactive devices (e.g., hand controllers, cameras, motion tracking sensors or physiological sensors). The computer-based HMDs (i.e., Oculus Rift, HTC Vive, Sensics zSight) were commonly used (16/27),37,38,46–49,54,56,58–63,66,67 with Oculus Rift being the most frequently reported (9/27).37,49,54,56,60,61,63,66,67 The laboratory-based HMDs (5/32) involved the use of complex technology where HMDs attached to a 3D TV or robot-like articulated arm.36,40,50,55,60 The wireless HMDs were either self-contained (9/32) (i.e., Oculus Quest,Pico G2, Oculus Go)41–45,51,53,63,64 or mobile-based (4/32) (i.e., Samsung Oculus gear, Google cardboard, VR vox).39,57,61,67 Five studies utilised two types of HMDs, and some reported essential clinical considerations for the use of specific HMD.45,60,61,63,67 Two studies reported that computer-based HMD (Oculus Rift) provided greater immersion and pain reduction compared with the mobile-based HMDs (Samsung Gear, Google Cardboard).61,67
Dose. The number of sessions, frequency and duration were varied across the studies, with discrepancy even in the studies which employed the same mechanism of action. The number of sessions ranged between a single session to 56 sessions over 8 weeks, and a duration ranged between 5 to 75 min. The frequency reported a range between daily to two sessions per week.
Delivery setting and related factors
IVR was commonly used in clinical settings (14/32)38,39,48,50,54,55,57,60–65,67 (i.e., hospital, clinics, and rehabilitation centres) and laboratory setting (8/27).36,40,46,47,49,56,58,59 The implementation of IVR as a home-based intervention was rarely reported (6/32),37,41,45,51,53,66 but it was common across studies which were conducted during Covid pandemic. Supervision and guidance by physiotherapists, as well as the technical aspect of IVR were frequently reported across the included studies. In the clinical and laboratory settings, six studies reported that IVR intervention was supervised and represented the physiotherapist's role in guiding patients during exercises performance, and providing instructions as needed.39,46–48,57,63 Of these, physiotherapists in Stamm et al. 46 and Tuck et al. 48 had direct access to the software, they monitored performance, safety and pausing the game when needed. Supervision and guidance were also reported to play a role in safety, engagement, and adherence to IVR intervention, particularly those associated with physical exercises.37,46,47 The technical aspect was highlighted in the studies, which implemented IVR as home-based intervention.37,41,45,51,53,66 This includes specific eligibility criteria such as familiarity with technology, the ability to wear the HMD, and the availability of resources such as WIFI, computer, and space and the need of remote technical support.37,41,45,51,53,66
Intended outcomes, patients’ experiences and adverse effects
The intended outcomes were varied across the studies in relation to the IVR mechanisms. However, three major outcomes were evaluated including pain, physical (ROM, function, balance, physical activity, and disability) and psychological (FOM, pain catastrophising, pain self-efficacy and anxiety). Pain, FOM and disability were the most frequently assessed outcomes across the studies. The outcomes were assessed in short and intermediate terms of post one session and a maximum of 3 months follow up. The long-term follow up of 18 months follow up was limited to one study. 44 Patients’ experiences were investigated by 13 studies, in which positive and negative aspects were reported.40,41,45,46,48,51,53,55,57,59–61,66 Based on patients’ feedbacks, these studies concluded that IVR games and /or experiences were feasible, enjoyable, and engaging, but some studies reported the negative aspects of IVR with regards to its usability including technical issues (e.g., e.g., connection problem, unexpected stop of the game or hand controller),45,46,53,66 difficulty in understanding the game instructions, 48 and several adverse effects that impacted patient's engagement.
The adverse effects were reported in 15 studies: symptoms of motion sickness (MS) (i.e., dizziness and nausea) (11/15),36,37,41,45,51,53,54,57,60,61,66 HMD discomfort (i.e., headache, neck pain, eye strain) (7/14),37,38,45,53,57,58,61 increase in pain (7/14),37,40,45,57,59,65,66 fatigue (1/14), 53 and claustrophobia (1/14). 66 Symptoms of MS were the most common, of which four studies reported that patients developed MS even though those with susceptibility to sickness were excluded prior to the study.41,45,54,66 The symptoms of sickness were reported as a main reason for poor engagement and dropouts.41,51,54,57,66 Whilst most studies did not provide specific reasons of pain exacerbation during the intervention period, two studies attributed that to challenging tasks as the physical limitations of the patients was not considered.40,59 The HMD discomfort was a major complaint of the patients in five studies,38,53,57,58,61 in which other five studies excluded patients who could not tolerate wearing HMD prior the intervention.41,54,55,66,67
Discussion
This review aimed to map studies using IVR intervention for adults with CPP. The search yielded 32 studies, mainly of pilot and feasibility studies. The IVR utilised for chronic musculoskeletal pain, fibromyalgia, chronic visceral pain and other conditions identified as CP. Several mechanisms of action were identified: distraction, physical exercises and activity, neuromodulation, graded exposure, mindfulness and/or biofeedback, hypnosis, and multi-mechanisms. The integration of these mechanisms was varied, primarily addressing pain, physical (e.g., ROM, function) and psychological (e.g., FOM, self-efficacy) attributes in short and limited long terms. Customised software was frequently used, with varied wireless and non-wireless HMDs. The IVR interventions were widely implemented in clinical/laboratory settings and the usability of the intervention was adversely affected by MS, discomfort wearing HMDs and technical issues.
Patient characteristics
Across the studies, the exclusion of patients with susceptibility to MS, epilepsy, visual or hearing impairments and psychiatrics conditions suggests that they may be at risk of adverse effects when receiving IVR intervention. The symptoms of MS (nausea or dizziness) have been a common disadvantage of IVR, however it is rarely associated with seizures.68–70 Additionally, patients with visual or hearing impairment as well as those with psychiatric symptoms may face challenges in tolerating the intense visual and auditory stimuli of the VE, as it may induce their symptoms.68,71 Although IVR has been utilised for anxiety and psychotic disorders,72–74 precautions should be considered for those with severe symptoms.41,45,48,56,57,61,64 Patients with balance problems were excluded when the VE enhance physical interactions in standing position,45,46,59 as maintaining balance is essential in fully immersive VE to prevent falls. 71 Hence, these exclusion criteria seem critical to promote safety of IVR intervention.
IVR mechanisms of action and intended outcomes
In line with previous reviews, the IVR mechanisms of action included distraction and other mechanisms beyond distraction.8,24–26,28,75–79
Distraction. The reviewed studies found that IVR distraction resulted in pain reduction during and /or immediately after the session, with a lack of long-lasting analgesic effect.52,54,60,66,67 Distraction is a well-discussed mechanism by gate control theory of pain to divert attention away from pain stimuli.15,16,80 Distraction may be more appropriate to explain the effect of IVR in acute pain rather than CP, typically considered as a complex biopsychosocial disorder, requiring focus on function and quality of life.4,7,21
Mechanisms beyond distraction. IVR as means of providing physical exercises and activity, mindfulness and/or biofeedback, hypnosis, neuromodulation, and graded exposure may lend itself better to describing how IVR is likely to address CPP. The use of physical exercises, mindfulness, biofeedback, hypnosis and graded exposure has been recommended in CPP management as they are not meant to treat pain directly, but to change behaviour and improving the ability to cope with pain.4,81 In addition, neuromodulation is a type of supported intervention in CP management to stimulate cortical remapping and enhance pain reduction.82,83 Whilst several reviewed studies delivered these mechanisms using IVR, limited attempt was found to align the intended outcomes to support any underpinning theories.
For instance, the studies proposed that gamified physical exercises within VE would motivate patient's engagement.36–39,47–49,57 However, the evaluation of engagement and adherence was limited to two studies, which reported that adherence to IVR exercises was equal or lesser compared with standard exercise.36,37 Assessing adherence to VR rehabilitation is crucial to validate its added benefits over standard rehabilitation. 84 This indicates that IVR as a mean for physical exercise in CP management holds potential but requires further investigation. Applying IVR mindfulness and biofeedback as a home-based intervention showed some promises in reducing pain intensity, pain interference with mood and activity, pain self-efficacy, catastrophising.41,51,53,64 However, limited information were reported on how patients practised these skills via IVR.41,51,53 A detailed intervention description, particularly for remote interventions, is considered critical for future replication,85,86 thus emphasizing the need of better reporting to determine the benefits of such mechanisms.
The neuromodulation mechanism was assigned to address the disruption of body perception and movements, that contribute to pain and disability in CLBP.58,62 However, pain reduction and improvement in back movements were found either after a single session or while inside VE.58,62 These positive findings could be attributed to the distraction nature of IVR and may not reflect the neuromodulation. Based on neuroplasticity theory, delivering the neuromodulation interventions (e.g., mirror therapy) daily over 4 to 6 weeks, can potentially provide analgesic effect by reversing the neuroplastic changes in the brain related to body mis-representation, as these effects are highly dependent on the frequency of practice over time.17,87–89 The reviewed studies are at early development stage and the results may not support the proposed neuromodulation mechanism.
In the CLBP studies, the graded exposure mechanism was applied in two different ways. Thomas et al. 40 facilitated only lumbar flexion, whereas the research group in Hennessy et al. 59 and Fowler et al. 61 developed and predefined a hierarchy of fearful movements. The standard graded exposure requires developing individualised hierarchy, where each patient rank their own fearful movements.90–92 This may explain the lack of significant improvement in the primary outcome of FOM across the studies.40,59,61 The distraction element of IVR games is believed to mitigate the anxiety-provoking nature associated with standard graded exposure, 93 however, the technology needs solutions to enable patients to define their own virtual hierarchy during VE development.
The review found recent study of multi-mechanisms, combining embodiment and behaviour change. 45 This recent development shows potential to address the avoidance behaviour associated with CLBP, employing VR elements (immersion, interactivity, and embodiment) to facilitate behaviour change principles including goals setting, repetitive tasks, feedback, and reward. 45 These principles have been well-established in psychology to foster behaviour change, 94 thus, their integration within VE may contribute to intervention success. Further studies are needed to validate this mechanism for future replication.
The IVR intervention characteristics
This review focused on the IVR intervention characteristics (software, hardware, dose), aiming to identify common features that may play a role on maximising the benefits of the intervention.
Software. Customized software was prevalent in the reviewed studies compared to off-the-shelf options to tailor movement progression, addressing the heterogeneity of CPP.36–38,41–44,49,57,61,62 This customisation would be essential, given that non tailored progression of movements was acknowledged to correlate with pain exacerbation.40,59 Previous reviews reported the need of customisation for enhancing the IVR intervention effectiveness, considering individual differences in usability.76,77 Integrating visual and auditory feedback as well as rewards have been also suggested as key engaging factors in VR rehabilitation.95,96
Hardware. Non-wireless computer-based HMDs (e.g., Oculus Rift) were frequently used, emphasizing the demand of high performance computer with controllers and motion sensors for immersive experience to influence patient's perception of movement.75,76 Furthermore, the feasibility of Oculus Rift were reported in the reviewed studies for providing greater immersion and longer pain relief compared to mobile-based HMDs.61,67 Notably, the recent studies between 2020 and 2023 showed the emergence of wireless-self-contained HMDs (e.g., Pico), potentially offering easier options for clinical population, although their superiority in changing clinical outcomes is yet to be established.
Dose. The variation in duration, number of sessions and frequency of IVR interventions have no clear consensus, however it may depend on the mechanism of action to achieve its intended outcomes. For example, the IVR for graded exposure may need 8–12 sessions to address FOM and the physical or psychological limitations in CPP patients.91,92 In addition, other factors such as immersion, interactivity or embodiment may need to be considered as technology-based interventions become more available.
Delivery setting and adverse effects
The IVR interventions in the reviewed studies were commonly implemented in clinical setting38,39,48,50,54,55,57,60–65,67 with fewer instances of home implementation.37,41,45,51,53,66 In clinical setting, the practitioner's supervision was seen essential for patient engagement when VE induced physical exercises,37,46 although it was rarely reported. Previous reviews highlighted the significance of supervised setting in improving the engagement and exercises effectiveness in chronic musculoskeletal conditions. 97 Alongside engagement, the high potential of associated adverse effects including symptoms of MS, discomfort of wearing the HMDs, and technical issues across the reviewed studies cannot rule out the need of supervision and practitioner support. Motion sickness characterised by nausea and dizziness, as well as discomfort from HMDs heavy weight have been major concerns in IVR research, stressing the need of monitoring during and after the intervention.26,69,76,98,99 Despite the encouraging findings on patients’ enjoyment and engagement, the risk of the adverse effects and the need of technical support remain challenges in adopting IVR for CP management.
Future research
The scope of the literature indicates the need to focus on the development stage and adopting a framework to improve the developed intervention. The complexity of developing IVR intervention for CPP increases the demand to use a rigorous framework. For instance, the Medical Research Council Framework has been validated for development and implementation of new intervention in healthcare. 100 Exploratory studies, engaging stakeholders have been suggested to enhance the development prior moving to pilot or feasibility studies. 100 This includes the use of theoretical basis in the development stage to understand how the mechanisms of action and associated dose can achieve change in the intended outcomes. 100 Multidisciplinary co-designing research engaging healthcare providers, technology developers and patients are recommended to better address customisation and usability of HMDs. In addition, IVR companies need to provide innovative healthcare solutions, designing patient-friendly HMDs. The prevalence of adverse effects requires further research on safety measures to mitigate risks and enhance patient's experience.
Strengths and limitations
The contribution of this scoping review to the field of IVR in CPP management was a strength, identifying the patients’ characteristics, the mechanisms of actions as well as the key features of software, hardware, and delivery setting. This aids in understanding the gap in development and implementation of IVR intervention. However, the current review has some limitations including the exclusion of non-English studies, which may provide additional insights into the use of IVR intervention for CPP. Also, the quality of the included studies was not critically evaluated due to the pre-defined heterogeneity of the studies. Although limiting the search to CPP and un-specified CP was seen necessary by the reviewers as substantial body of literature in CPP, this may be criticised for narrowing the scope of literature. Future reviews are encouraged to broaden the search scope to encompass both CPP and CSP, presenting in depth discussion about mechanisms of action based on CP classification and its effect on intended outcomes.
Conclusion
The use of IVR technology for CPP is rapidly emerging, creating interventions with diverse range of mechanisms including physical exercises, neuromodulation, and graded exposure, yet these mechanisms are not well established. Customised software associated with visual feedback and rewards on performance need to be considered to enhance the effect of the intervention. The MS, HMD discomfort and technical issues pose major challenges, directly impacting the uptake of IVR intervention. As technology advances, further investigation is warranted on IVR mechanisms, related dose and strategies to enhance uptake, using co-designing research.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241254456 - Supplemental material for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241254456 for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review by Anfal Astek, Valerie Sparkes and Liba Sheeran in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241254456 - Supplemental material for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review
Supplemental material, sj-docx-2-dhj-10.1177_20552076241254456 for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review by Anfal Astek, Valerie Sparkes and Liba Sheeran in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241254456 - Supplemental material for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review
Supplemental material, sj-docx-3-dhj-10.1177_20552076241254456 for Exploring the use of immersive virtual reality in adults with chronic primary pain: A scoping review by Anfal Astek, Valerie Sparkes and Liba Sheeran in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank Cardiff university librarian for assistance in search strategy of this research.
Contributorship
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval and informed consent are not applicable, because this article does not involve any studies with human or animal subjects.
Funding
This work is a part of PhD thesis funded by Saudi Arabia Cultural Bureau in London
Saudi Arabia Cultural Bureau in London,
Guarantor
AA
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.