
Abstract
Objective
Virtual reality (VR) has become increasingly popular in clinical and health settings where it has been used for a wide range of purposes. A recent scoping review explored VR applications to assist pregnant women and found that VR was a useful method to be used for a range of different purposes in both pregnancy and labour. However, no such review exists for the period after birth.
Method
We aimed to search for studies that used VR to support parents during birth and in the first year postpartum (Population) in different settings (Context), and finally provided data on the characteristics, reported effectiveness and experience of VR interventions (Concept). Two hundred and fifty-one studies were identified, of which ten were eligible. Two authors independently extracted data including study design, participants and results.
Results
Findings indicate that VR has been used effectively in this context to alleviate depression anxiety, and multiple domains of pain and to improve childbirth satisfaction. The majority of the studies explored the use of VR technology on outcomes such as pain and anxiety during labour and birth. The studies included used a broad range of VR hardware and software. All of the studies reported positive experiences of using VR.
Conclusions
Across these studies, VR was found to be effective in terms of both physiological and psychological outcomes. There are many unexplored maternal and infant focused applications of VR which warrant further investigation as emerging evidence indicates this is becoming an increasingly accessible method to improve maternal and infant health outcomes from pregnancy through to parenthood.
Introduction
Virtual reality (VR) is a computer-based technology that has seen an exponential surge in popularity due to increased affordability. 1 There are three primary categories of VR simulations used today: non-immersive, semi-immersive and fully-immersive simulations. 2 Non-immersive VR uses a computer or video game system and users interact with the virtual environment (VE) with devices such as a mouse or a joystick. Semi-immersive VR provides users with a partially VE simulating via 3D graphics. Immersive VR uses VR glasses or a head-mounted display providing the user with high-resolution content and a wide field of view. The VE is the simulated scenario generated by the computer or device which is designed to be explored, so users can interact with their environment. 3 In multi-user or collaborative virtual environments two or more users can share the same simulation and communicate and/or interact inside it. 3 Augmented reality is a newer technology which combines adding virtual objects into real life, in real time. 4
VR provides opportunities to create and recreate simulated environments ‘where the testing, training, teaching, and treatment of cognitive, emotional, and sensorimotor processes can take place under stimulus conditions that are not easily deliverable and controllable in the physical world’. 5 As a result of this, VR technologies are increasingly used in different settings including sports, 6 the arts, 7 the military, 8 industry, 9 education, 10 entertainment 11 and healthcare. 12 VR has become increasingly popular in clinical and health settings 1 where it has been used for a wide range of purposes including medical simulation, 13 remote and live surgery, 14 training health care professionals, 15 facilitating pain management, 16 improving psychological health 17 and exercise rehabilitation. 18
A recent scoping review explored VR applications to assist pregnant women and found nine studies which demonstrated that VR was a useful method to be used for a range of different purposes in both pregnancy and labour. 19 Four studies had used VR technology to reduce the anxiety of pregnant women, four studies had applied VR for decreasing pain during labour, and one study used VR to support physical activity in pregnancy. However, no such review exists for the period after birth which makes this an important and necessary undertaking to add to the literature base on utilisation of VR in maternal health settings. The postnatal period is a complex period in a woman's life with a multitude of unique biopsychosocial transitions during which VR may have the potential to support. Furthermore, the prenatal review used a small number of databases (n = 3), search terms regarding labour and birth were limited, and the search strategy was restricted (keywords were searched only in the Titles/Abstract fields). The authors acknowledge this may have lacked sensitivity and omitted relevant work. While our focus was on the postnatal period, we deemed it relevant to include studies relating to birth and delivery and overcome the limitations of the previous review. Therefore, this scoping review has the research question of ‘What are the characteristics, reported effectiveness, and experiences of VR interventions designed to support parents during and throughout the first year after birth?’ It therefore aims to synthesise the existing literature about the characteristics, reported effectiveness and experience of VR interventions designed to support parents during and throughout the first year after birth.
Method
A protocol was developed using the scoping review methodological framework proposed by Arksey and O’Malley 20 and further refined by the Joanna Briggs Institute. 21 The draft protocol received feedback from the research team, including methodologists and a creative artist involved in VR intervention development. The final protocol is available upon request from the corresponding author. The PRISMA extension of scoping reviews (PRISMA-ScR) checklist was used to report information throughout the article.
Eligibility criteria
Published studies were included if they reported data on the reported effectiveness and/or experience of VR interventions designed to support parents during birth and in the first year postpartum. This included all interventional, observational and qualitative study designs that provided information on outcomes (e.g. reduction in anxiety) and/or experiences (e.g. satisfaction with the intervention). Any outcome or experience were considered eligible. All types of VR were considered including non-immersive VR, fully-immersive VR, semi-immersive VR, augmented reality and collaborative VR. Studies that did not use VR as an intervention to support birth or the first year of life, that used VR to train healthcare professionals, that used VR for parents with children > 1, or that focused on the infant rather than the parent, were excluded. We further excluded study protocols, reviews, books, periodicals, and articles with a full text in a language other than English.
Information sources
Databases searched included: The Cumulative Index of Nursing and Allied Health Literature (CINAHL), MEDLINE (Ovid), PsycArticles, Embase, Web of Science and Global Index Medicus. Additional methods involved author runs, backward and forward chaining. The population, concept, and context (PCC) structure was used to identify search terms. We aimed to search for studies that used VR to support parents during birth and in the first year postpartum (Population) in different settings (Context), and finally provided data on the reported effectiveness and/or experience of using VR technology (Concept). Search terms were refined following a priori scoping exercises and modified for specific databases as appropriate. Keywords included: ‘virtual reality’, ‘VR’, ‘virtual intervention’, ‘augmented reality’ and ‘labor’, ‘labour’, ‘birth’, ‘postnatal’, ‘postpartum’, ‘maternal’, ‘mother’, ‘parent*’. A copy of the full electronic search strategy is available upon request. A manual search of reference lists of included studies and relevant reviews was also conducted.
Study selection
A three-stage screening protocol was followed. Titles were first assessed and any articles that were evidently unsuitable were excluded at this stage. Abstracts were then screened and excluded where appropriate with written justification. Finally, the full text of each eligible article was read thoroughly by two authors (VF and SMD) to determine inclusion in the review.
Data extraction
Two review authors (VF and SMD) extracted data from the included studies. Any inconsistencies were resolved by discussion or, where necessary, LC was consulted. For each study, general characteristics extracted included authors, year of publication, country, study design, sample size and characteristics, study objective. Specific characteristics of the intervention were also extracted including VR components (software and hardware), data collection, results and pertinent methodological details. Where necessary, authors were contacted to identify/confirm any missing or ambiguous data.
Data analysis
Descriptive summaries were provided for general study characteristics and characteristics of the VR hardware and software. Results were then synthesised and reported based on physical and psychological outcomes. A summary of the experiences of those using VR was also provided.
Results
Following searches using CINAHL, MEDLINE (Ovid), PsycArticles, Embase, Web of Science and Global Index Medicus, 485 studies were identified. Two additional studies were identified via reference list searches. Two-hundred fifty-one studies were remaining after 234 duplicates were removed. These studies then underwent title and abstract screening. Twenty-six full text articles remained and were reviewed for eligibility resulting in 10 studies meeting the inclusion criteria for this study (see Figure 1).
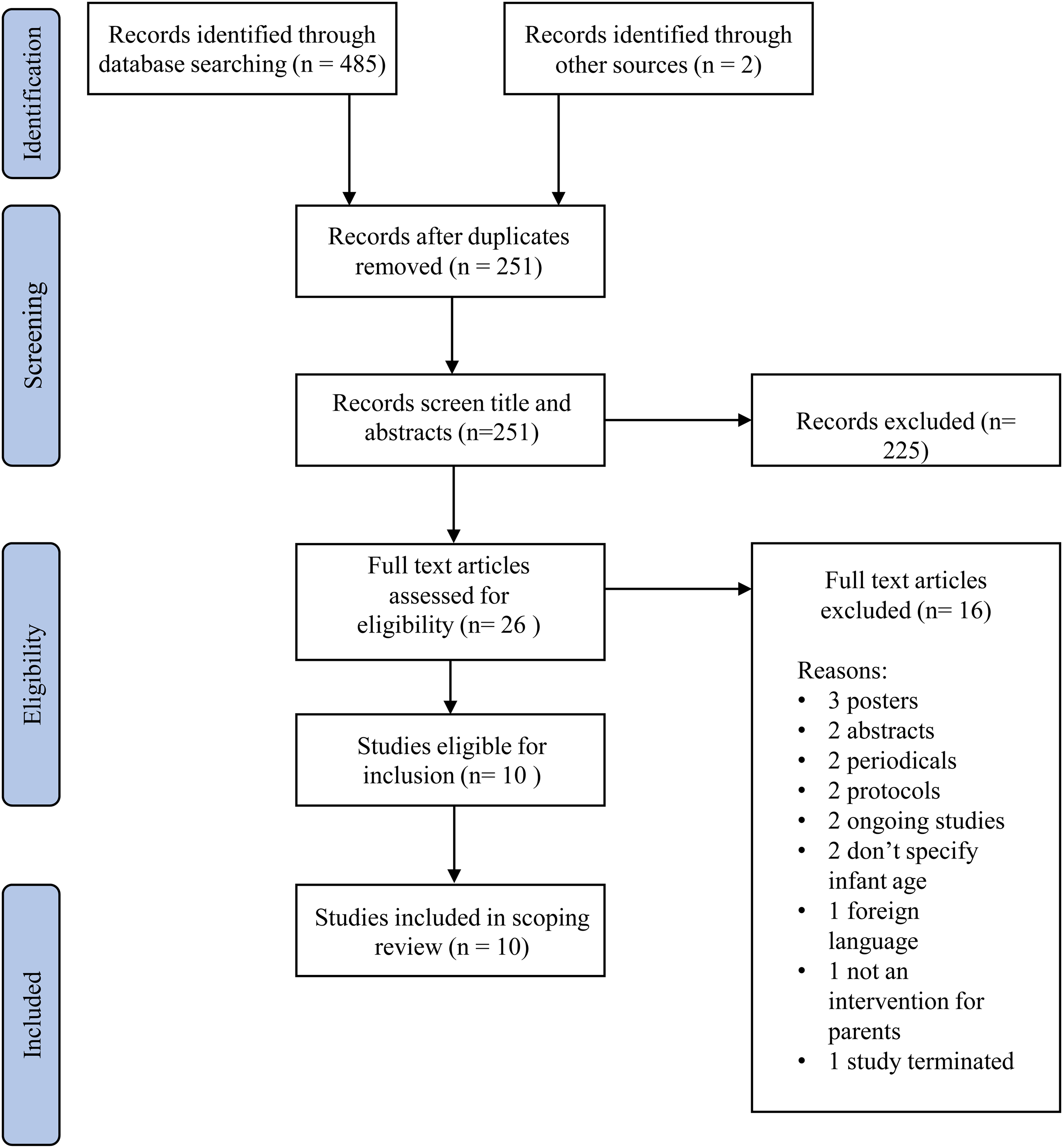
PRISMA scoping review flowchart.
General study characteristics
Ten articles met inclusion criteria and were included in this review.22–31 The majority of the studies (n = 8) were published between 2019 and 202122–25,27,28,30,31 with the exception of one study published in 2015 26 and one published in 2016. 29 Four of the studies were conducted in Iran,23,26,27,29 two in Turkey,22,25 and one in the US, 24 Mexico, 28 New Zealand 30 and China. 31 Nine of the included studies were randomised control trials22–29,31 and one study was a single case-study trial. 30 A total of 726 participants were included in the 10 studies, with sample size ranging from 4 28 to 273. 25 Two studies aimed to reduce pain25,26 and one study aimed to reduce anxiety. 29 Some studies (n = 5) reported multiple outcomes (e.g. pain and anxiety)22,24,27,28,31 and one study reporting both depression and anxiety. 30 One study examined childbirth satisfaction. 23 The majority of the studies (n = 7) explored the use of VR technology on outcomes such as pain and anxiety during labour and birth.22–25,27,28,31 Five studies were identified that examined VR during labour that were not identified in the previous prenatal scoping review.22,23,25,27,31 Two studies investigated the use of VR technology following birth during episiotomy26,29 and one study examined the role of VR technology postnatally (see Table 1). 29 All of the studies used immersive VR.
General characteristics of the included studies.

Characteristics of the VR
The studies included used a range of VR hardware used in varying combinations. Three studies implemented the VR technology via a smartphone22,24,25 and three studies implemented the VR technology via a computer or DVD player.26,29,30 Five studies utilised a head mounted display participants wore24,27,28,30,31 and four studies provided VR glasses/goggles for participants to wear.23,25,26,29 One study additionally provided a joystick for participants to use during the VR program. 30 Similarly, a range of VR software was employed, Akin et al. 22 displayed foetal ultrasound images taken antenatally to participants. Ebrahminian at al. 23 presented 360° views of nature scenes. Frey et al. 24 displayed simulations of ocean scenes and animals alongside relaxing music. Gur et al. 25 used VR to show participants digital photographs of content infants accompanied by classical music. Jahani et al. 26 provided participants with a 3D film of ocean animals. Momenyan et al. 27 displayed 360° videos of peaceful landscapes. Mosso et al. 28 provided participants with the option to select one of three VR nature scenarios. Shourab et al. 29 displayed VR videos of ocean animals. Stamou et al. 30 provided participants with a virtual household environment to navigate containing various stressors. Wu at al. 31 showed participants VR programs such as ocean scenes (see Table 2).
Intervention characteristics of the included studies.

Reported effectiveness according to physical and psychological outcomes
VR and physical outcomes
Seven of the studies included demonstrated the VR intervention groups having a significant analgesic effect on pain during labour22,24,27,28,31 and episiotomy repair26,29 compared to the non-VR groups.
VR and psychological outcomes
Eight studies demonstrated lower anxiety22,24,27–31 and depression 30 scores in the VR intervention groups compared to the control groups. Additionally, one study found that maternal childbirth satisfaction scores were higher in the VR groups in comparison to the control group. 23
Experiences of those using VR
Six studies reported data on the experiences of participants while using the VR.22,24,25,29–31 Two of these studies reported quantitative survey data24,31 and four reported qualitative data.22,25,29,30 Five of the studies reported on VR experience during labour,22,24,25,29,31 and one reported on VR experience during combined treatment for postnatal depression. 30 All of the studies reported positive experiences of using VR. Childbirth was considered less painful in one study 22 and less anxiety provoking in two studies22,25 while using VR. VR aided focus, control, relaxation and satisfaction with childbirth. VR was also well accepted, recommended and enjoyed by women during childbirth in three studies.24,25,30
Discussion
This scoping review was conducted to identify and review the studies that used VR to help mothers during birth and the first postpartum year. Findings indicate that VR has been used effectively during and immediately after birth to alleviate depression anxiety, and multiple domains of pain, and to improve childbirth satisfaction. There was also preliminary evidence in one study that VR was effective in treating symptoms of postnatal depression. Anxiety and fear during childbirth have been consistently linked to a number of adverse objective and subjective birth experiences 32 and contribute to higher levels of pain experienced during birth. 33 The relationship between anxiety and pain is cyclical with anxiety increasing perceptions of pain, and the experience of pain exacerbating anxiety. 34 It is well documented that difficulties during labour are associated with a range of birth complications which have negative implications for health and wellbeing in the postnatal period for both mother and infant. 32 Therefore, the use of VR has the potential to disrupt the anxiety-pain feedback loop and reduce the risk of longer-term adverse maternal and infant outcomes.
VR was used predominately during labour and birth, but also for episiotomy repair and postnatal mental health. Furthermore, mothers reported positive experiences of using VR across many of the studies which indicates it is an acceptable intervention across diverse settings in the intrapartum and postpartum period. However, there has been very limited use of VR outside of an intrapartum context with only one study in the review exploring its use further into the postnatal period. 30 There is potential for VR to be applied as a preventative tool to other psychological and social domains of perinatal health such as supporting the mother-infant relationship, infant feeding, routine infant care and perinatal wellbeing. Furthermore, it has yet to be applied to other settings within maternity care such as the operating room, postnatal ward or Neonatal Intensive Care Unit. This is similar to the prenatal review where the vast majority of studies were also conducted during labour. 19 There are also numerous applications for VR in the antenatal period that have yet to be explored including virtual tours of the labour and delivery suite to prepare women for birth, to alleviate anxiety in the early pregnancy assessment unit and pregnancy monitoring. Alleviating childbirth-related anxiety during the antenatal period may also improve birth experiences and subsequent postnatal health and wellbeing. 32
There was preliminary evidence in one study that VR was effective in treating symptoms of postnatal depression, although this was in combination with CBT. 30 Further investigation of the efficacy of VR for supporting perinatal mental health is necessary, and studies should consider other conditions (e.g. anxiety, PTSD, stress, adjustment disorders) and constructs (e.g. resilience, wellbeing, self-efficacy, psychological flexibility). VR should be explored as both as a standalone tool, and in combination with other therapies, to fully understand its potential. There is evidence for the efficacy of VR for supporting mental health in general adult populations with a recent systematic review reporting that VR was an effective treatment for a range of mental health conditions. 35 However, while a meta-analysis found that VR-based interventions were more effective than control conditions, they did not perform better than other therapeutic interventions for anxiety and depression. 36 VR has also been demonstrated to be effective for specific phobias in general adult populations, 37 which indicates that it may hold potential in a perinatal context for treating maternal phobias, obsessive-compulsive disorders and breastfeeding aversion.
Finally, while undertaking screening, we noted there were two study protocols with research both planned and in progress in perinatal populations, which was encouraging. This included a planned RCT exploring the utility of VR for assisting with perinatal loss and grief, 1 and a study in progress which examined the efficacy of VR for reducing pain and anxiety during labour. 38 Given the number of studies which investigate the potential of VR during childbirth, there may be scope to meta-analyse this literature and draw more robust conclusions regarding its use in this context.
Strengths and limitations
The majority of the studies included were randomised control trials which are considered gold standard in terms of design due to limiting bias and therefore providing high-quality evidence. Furthermore, all of the studies included used inferential statistics which allows generalisability of findings. However, there was heterogeneity across the studies in terms of aims, VR software, outcome measurements and timing of measurement which limits the ability to draw firm conclusions. Furthermore, there were no qualitative studies included in the review specifically exploring the experiences of those using VR during labour or the first year after birth, which is important to consider in future research. Seven of the studies included used generic, pre-designed relaxation software including dolphins, whales, curious manatees, oceans and mountains.23, 24,26–29,31 The remaining three studies used bespoke software tailored specifically to the study aims and population.22,25,30 While generic software may be cost-effective, it may lack specificity to childbearing populations, therefore co-design of future VR software with experts by experience would be a good method to improve acceptability. In terms of real-world application of VR in this context, considering safety in postnatal populations who may be caring for a baby is also of importance. The studies included in this review used immersive VR with mounted headsets which limits the ability to carry out routine tasks while using the software. Future studies should also examine the ecological validity of using VR in this context, to see whether it translates into the natural maternal environment. It is important to note that scoping reviews can only provide information on the reported effectiveness, but cannot determine actual effectiveness, of interventions. Future research should consider a full systematic review with meta-analysis to establish actual effectiveness.
Conclusion
Our scoping review found that VR technology has been used during childbirth and the postnatal period in a range of ways, including reduction of pain, anxiety, and stress in labour, and coping with the symptoms of postnatal depression. Across these studies, VR was found to be effective in terms of both physiological and psychological outcomes. Furthermore, mothers reported positive experiences of using VR which indicates acceptability in this population. There are many unexplored maternal and infant focused applications of VR which warrant further investigation as emerging evidence indicates this is becoming an increasingly accessible method to improve maternal and infant health outcomes from pregnancy through to parenthood.
Footnotes
Abbreviations
Contributorship
LC and VF conceptualised and designed the study. VF and SMD conducted the searches, screening and data extraction. VF and SMD wrote the manuscript. LC and SAS critically revised the manuscript. VF, LC, SMD and SAS approved the final version of the study to be published.
Consent statement
Participant consent was not necessary in this paper as it is a review article and not primary research.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LC is a visual artist with an interest in developing a virtual reality application using her art to support breastfeeding mothers. She commissioned VF and SMD to conduct the current scoping review from an Arts Council funded grant. This was to enable an understanding of the existing literature about virtual reality interventions designed to support parents during and throughout the first year after birth prior to developing her application.
Ethical approval
No ethical approval was required for this study as it was a scoping review of the literature.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LC commissioned VF and SMD to conduct the current scoping review from an Arts Council funded grant.
Guarantor
Dr Victoria Fallon.