
Abstract
Background
Electronic patient-reported outcomes (ePROMs) enhance symptom management and patients’ engagement in palliative cancer care. However, integrating them into this setting brings challenges, including patients’ familiarity with technological devices and declining health status. Prioritizing the patient's acceptability and feasibility is crucial for their adoption. However, more knowledge is needed about patients’ perspectives on the adoption of ePROMs in the community, especially for home-based palliative care.
Aim
Explore patient viewpoints on utilizing ePROMs for symptom reporting in home-based oncology palliative care.
Design
A qualitative interpretative approach was used to evaluate patients’ points of view on using ePROMs in this specific care setting. Semistructured interviews were carried out. Data were analyzed using a reflexive thematic analysis.
Setting/participants
A total of 25 patients receiving oncological home palliative care from the advanced palliative care unit of the Fondazione IRCCS Istituto Nazionale dei Tumori in Milan, Italy, were invited to participate. Twenty interviews were conducted, as five patients declined due to deteriorating health.
Results
Four themes were identified: (1) strategic value of ePROMs and subjective appreciation; (2) enhancing patient centeredness through ePROMs; (3) exploring and addressing concerns about the use of ePROMs and (4) intersecting factors influencing the efficacy of ePROMs
Conclusion
Despite initial reticence, home palliative care patients consider ePROMs as potentially valuable allies monitoring symptoms, enhancing their quality of life, and amplifying their voices on less explored aspects of care. Continuous dialog between healthcare professionals and patients is crucial for addressing patient skepticism about ePROMs and their impact on the human aspect of care.
Keywords
Background
The World Health Organization has reported an increase in cancer incidence worldwide. 1 Annually, approximately 17 million people are diagnosed with cancer, and 9.6 million die, underscoring the need for adequate palliative care and end-of-life care. 2 Home-based palliative care is preferred by most advanced cancer patients, as it aligns with their desire to receive care and spend their final days in the comfort of their own homes. 3 Opting for home-based end-of-life care enables patients to preserve their autonomy, privacy, and sense of normalcy, 4 resulting in heightened satisfaction and improved quality of life for them and their families.1,5 Gathering patient voice on home-based cancer palliative care is crucial for a holistic understanding of their health status and care outcomes. 6
Patient information may be captured using patient-reported outcome measures (PROMs), questionnaires reporting health conditions directly by patients, bypassing interpretation by healthcare professionals or anyone else. 7 PROMs can help healthcare professionals make informed decisions, foster effective communication with patients/families, monitor symptoms and the effectiveness of treatments and prioritize patient needs.8–11 The most commonly used PROMs in palliative care are the Edmonton Symptom Assessment System (ESAS) 12 and the Integrated Palliative Care Outcome Scale (IPOS). 5
In a recent systematic review, patients’ experiences with PROMs showed empowerment through self-reflection and valuable information for clinical planning, assessment, diagnosis, personalized treatment, decision-making, and monitoring. However, barriers to their engagement were identified, including concerns about their purpose and how gathered information is used in clinical settings. 13
Digital versions of PROMs (ePROMs)14–16 offer advantages such as increased accuracy and efficiency of data collection, reduced data entry errors, prompt availability of recorded symptom data for healthcare professionals14,17–22 and complete PROMs at any time and place convenient to patients. 23 Nevertheless, the literature also highlights that healthcare professionals are concerned that digital PROMs might reduce personal interaction and result in inadequate, limited, and one-dimensional symptom assessment.24,25
Utilizing ePROMs in cancer palliative care can enhance a patient-centered approach25,26 and patient engagement in healthcare delivery.25,27–30 They gather symptom data such as anxiety, drowsiness, fatigue, nausea, and pain, enabling clinicians to prioritize patients’ needs based also on their questionnaire scores. 9 However, the integration of e-PROMs into oncological palliative care is challenged by a myriad of factors such as cultural and socioeconomic influences, familiarity with technological devices, 24 care settings, deteriorating functional health status9,24 and emotional symptoms that are perceived as burdens and may even overshadow physical manifestations. 11
The adoption of ePROMs must prioritize patient acceptability and perspectives and thoroughly assess feasibility.31,32 However, despite this evidence, there is still a need for more knowledge regarding patients’ perspectives on ePROMs in the community setting, particularly concerning patients undergoing home palliative care.
Aim
This study was designed to uncover and understand patients’ viewpoints on utilizing ePROMs for symptom reporting in the context of home-based palliative care.
Methods
Design
The aim of this study was achieved by employing a qualitative interpretative approach through interviews. For this qualitative investigation, we used Braun and Clarke's reflexive thematic analysis method.33–35 We reported this study under the Consolidated Criteria for Reporting Qualitative Research (COREQ) 36 guidelines to ensure transparency and enhance rigor.
Setting
This single-center study was part of a larger project titled “Impact assessment of a system e-Patient Reported Outcome Measures on home palliative care: Mixed-methods study of feasibility and intervention.” This project aimed to promote the utilization of e-PROMs in palliative cancer care at home within the Fondazione IRCCS Istituto Nazionale dei Tumori of Milan (INT), a comprehensive center. The study was conducted within the INT's Palliative Care—Hospice, Pain Therapy, and Rehabilitation Complex Unit, including the service of Home Palliative Care.
Annually, approximately 100 patients access home-based palliative care, receiving consistent support from a dedicated couple of physicians and nurses. At the time the data were collected, none of the healthcare professionals used e-PROMs or PROMs as a standardized method of assessment. Before the study started, all healthcare professionals were required to participate in a comprehensive training program focused on ePROMs. This training was designed to equip them with a thorough understanding of how ePROMs are applied within palliative care settings, highlighting their significance and detailing the PROMs that are most commonly used in this context.
Participants and recruitment
To be considered for inclusion, participants were required to be under the care of the home-based oncology palliative care service at the INT, be adults aged 18 or older, have a diagnosis of metastatic or advanced neoplasms (stage III or IV), have an estimated prognosis of less than three months, and not have any clinical conditions that would impair their ability to self-assess. A purposive sampling method aimed at achieving maximum variation was utilized to select patients undergoing palliative care for cancer, ensuring a diverse sample in terms of age, gender, diagnosis, and educational background. 37 The recruitment phase spanned from May 2022 to April 2023, during which healthcare professionals referred eligible patients to the research team. IB, a researcher with experience in palliative care, was responsible for screening and recruiting participants, detailing the study's objectives and providing written consent during individual patient meetings.
Study procedures
After providing their signed informed consent, participants underwent a training session at their homes, led by researcher IB. Subsequently, they engaged in two separate testing sessions of the e-PROMs during their appointments at home with healthcare professionals. In the meeting with IB, patients were introduced to prototype ePROMs on a tablet provided by INT through Ticuro Reply software, an innovative application used for telemonitoring and telecounseling at INT. Patients tested the usability and utility of the Italian version of two types of PROMs (IPOS and ESAS) on the tablet, ticking multiple-choice questions and manually typing the answer to open-ended questions, with IB and the healthcare professionals available to address their questions. Participants were guided through the process of entering data and interpreting the results within these tools, with special attention given to the nuances of each of the two PROM types, providing a real-world context for using the ePROMs. The data from the ePROMs collected during the training sessions were not formally integrated into the medical records as the aim was not to immediately apply the data for clinical decision-making.
The IPOS is a patient self-report and staff proxy-report outcome measure for advanced illness patients in palliative care that assesses physical symptoms, emotional symptoms, and communication/practical issues through ten questions (17 items),38,39 focusing on symptom burden. 5 It is available at https://pos-pal.org.
The ESAS, which measures perceived symptom severity, is a brief and versatile screening tool with ten items covering many physical and emotional symptoms, including pain, fatigue, drowsiness, nausea, dyspnea, depression, anxiety, well-being, and sleep. 40
Patients underwent training sessions with their assigned healthcare professionals to grasp the benefits of PROMs and their applicability to their health conditions.
Data collection
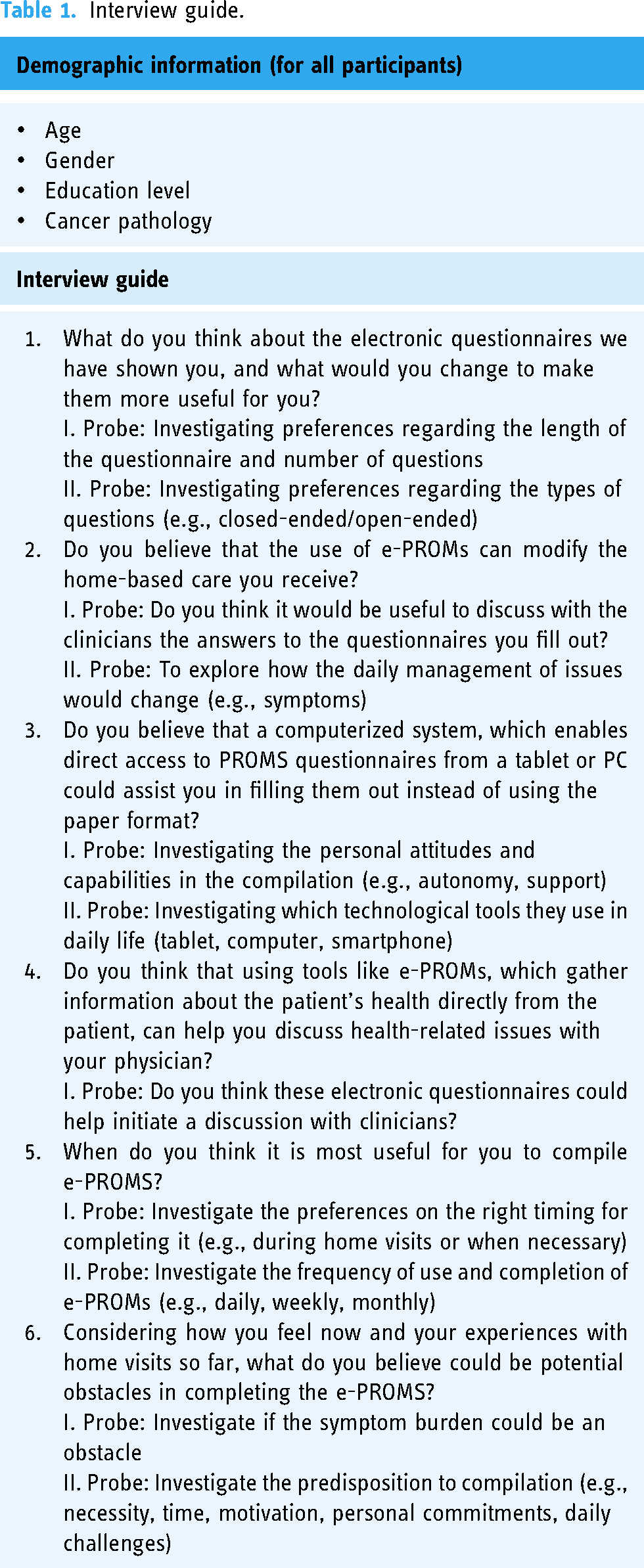
LC, a PhD student in nursing and public health, and ML, an experienced senior researcher in qualitative research, conducted a comprehensive literature review to shape the guiding questions for semistructured interviews (Table 1). These face-to-face interviews in Italian, although flexible in prioritizing patients’ unique perspectives, covered all research areas thoroughly. Data were collected at the patients’ homes from June 2022 to May 2023. Initially SC, a nurse with expertise in cancer care and qualitative studies, conducted with LC collaborative interviews. These initial interviews prompted minor revisions to the interview guide for a more comprehensive understanding of patients’ perceptions. To stimulate respondents to produce more information, researchers have developed additional probe questions, which are supplementary questions aimed directing the discussions and not leading the discussion. Subsequent interviews were then conducted individually by LC and SC the week following the training session with healthcare professionals. At the start of each interview, participants were given a refresher on the ePROM through the same tablet used in the training sessions. This was done to confirm that participants fully understood the study's goals and to answer any of their questions. The caregivers of the participants were at home with the patients at the time of the interview but the study did not involve their participation. Detailed notes were taken during the interviews. The decision to halt recruitment was guided by repeated team discussions in conjunction with the study objective. Recruitment continued until we achieved adequacy (richness, complexity) of the data for addressing the research question. 41
Interview guide.
Data analysis
The audio-recorded interviews were transcribed verbatim by SC and managed using NVivo V1.6.2. 42 To protect anonymity, any mentions of the participant's identity in the transcript were modified. SC extensively reviewed the interviews, with all authors thoroughly reading the transcripts for a comprehensive understanding. The qualitative data were independently coded line by line by LC and DR, an author experienced in cancer care. The entire research team then discussed the codes concurrently to identify emerging themes and add or modify questions. The reflexive thematic analysis approach was employed to analyze the data 34 using an inductive method. Initially, the data were categorized into multiple smaller groups, but as the analysis progressed, these groups were merged to form the final results. As the analysis progressed, it fostered a deeper understanding of the data, leading to the discovery of new patterns of meaning. 40 Consensus meetings with ML ensured agreement on the coding process. To enhance credibility, the authors adhered to interpretive description principles. This involved a thorough review of prior research, selecting a method recognizing human experience complexity, testing the interview guide for credibility, employing triangulation in the analysis phase, and maintaining open-ended analysis to present multiple quotes that clarify the results’ rationale. 43
Ethical considerations
The participants in the study gave their written consent. They were also guaranteed that their identities would remain anonymous and that the confidentiality of the collected data and audio files would be maintained. Strict data protection procedures were followed, and further assurances of confidentiality were provided. All collected data and audio were stored using a two-level password protection file that the researchers had sole access to in an encrypted computer. The study received ethical approval from the INT Ethics Committee [Ref: 187/21].
Results
Five of the 25 invited patients declined due to health deterioration, resulting in 20 interviews. The baseline characteristics of the sample are presented in Table 2. The interviews averaged 25 min, with an average participant age of 72.57 years. Half of the patients were between 50 and 70 years old, and most were female (n = 13), with various cancer types.
Characteristics of interviews participants.

The coding process identified 408 codes, leading to 13 subthemes and four main themes: (1) strategic value of ePROMs and subjective appreciation; (2) enhancing patient centeredness through ePROMs; (3) exploring and addressing concerns about the use of ePROMs; and (4) intersecting factors influencing the efficacy of ePROMs. Figure 1 illustrates a thematic summary of the themes and subthemes.
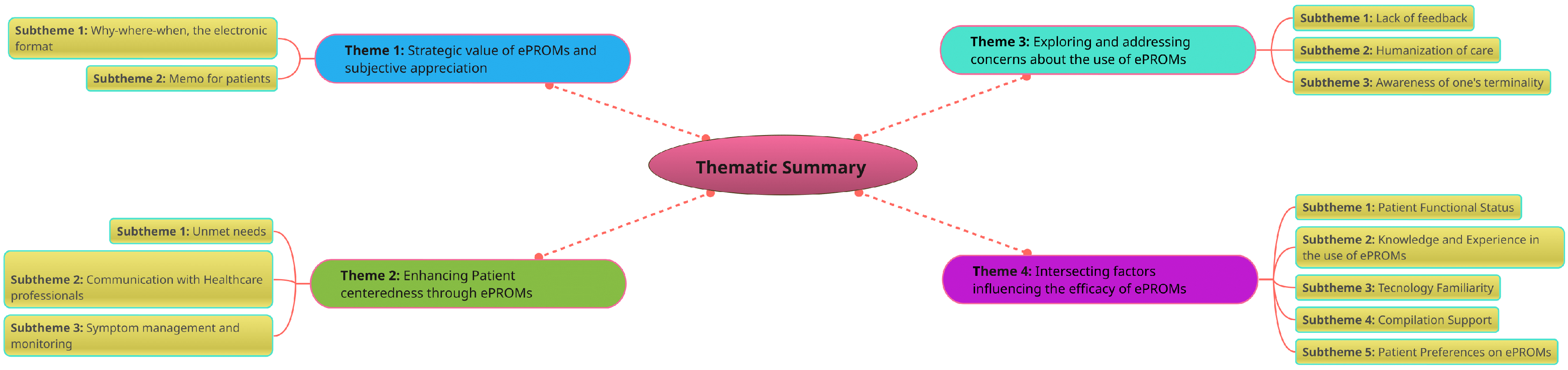
A thematic summary of the themes and subthemes.
Theme 1: strategic value of ePROMs and subjective appreciation
Patients perceived the potential value and advantages of integrating an ePROM system, seeing it as a transformative tool that could elevate the standard of their health management and potentially enrich the therapeutic experience throughout their home-based clinical care trajectory. This theme includes two subthemes: why-where-when, the electronic format and memo for patients.
Subtheme 1: why-where-when, the electronic format
Patients regard ePROMs as accessible tools that seamlessly integrate into their lives due to their availability around the clock and in any setting. They particularly value the straightforwardness and efficiency of its utilization, which allows them to engage without the onset of fatigue or the cumbersome requirement of securing an appropriate setting for completion. This appreciation underscores the strategic value of ePROMs, as it highlights the technology's ability to meet patient needs in a flexible and user-friendly manner: Then, I could do it wherever and whenever I want, without fatigue, without–you know, without even looking for a place to write. I just pick up and press the end. Interview n°6 But so the information still remains written down and visible to all. It provides a tangibility of what we're going through on those days when thoughts fly to the worst places. Interview n°14
Subtheme 2: memo for patients
According to participants, EPROMs provide a tangible reminder to address and articulate specific experiences such as the acute pain at a distinct moment, in the context of consultations with healthcare professionals. It is especially valuable in environments where the hustle of medical discussions can lead to the omission or oversight of critical details, ensuring that nothing significant is missed or forgotten: During meetings with clinicians, it's possible to miss or forget important pieces, and sometimes we need help remembering what happened the previous week. That's where this serves as a helpful reminder. For instance, I need to discuss the pain I experienced in that moment rather than the struggles I faced in another. …That therapy was beneficial; it helped me through a time when I couldn't eat…in short. Interview n° 3 I think they could help me remember all my issues; the more time passes, the more there are, or maybe I'm so used to having to manage them that I don't even think it's a problem anymore. Interview n° 20
Theme 2: enhancing patient centeredness through ePROMs
Patients outlined their views on the potential outcomes that could be achieved using ePROMs. When patients articulate their own health outcomes, they foster a sense of ownership and empowerment which can lead to improved quality of care. This theme includes three subthemes: unmet needs, communication with healthcare professionals, and symptom management and monitoring.
Subtheme 1: unmet needs
Patients often overlook certain needs when talking to their healthcare professionals. Comprehensive ePROMs covering various relevant issues and symptoms in this healthcare setting help patients voice unaddressed needs. These questionnaires, tailored for personalized and in-depth assessments, empower patients to express needs that require further exploration, facilitating a more thorough understanding for healthcare providers: Having a questionnaire that provides me with an orientation to address all the topics, all the knowledge, could be useful for me. That's what I need at this moment[…]. Interview n°5 Some things are being explored in depth that maybe I hadn't even considered. Interview n°12
Subtheme 2: communication with healthcare professionals
Patients believe that the use of ePROMs can capture the most significant symptoms they suffer from daily, thereby enabling the initiation of discussions about each of these symptoms during home visits. Consequently, patients view ePROMs as potentially valuable tools that not only aid in structuring their conversations but also promote open communication, acting as a bridge between them and healthcare professionals: I believe that it can definitely be a tool that further enhances and strengthens the relationship, as long as it is managed properly. The checkmark you put is the stimulus to open the conversation. They could be the questions from the questionnaire that encourage you to speak and discuss verbally with your doctor in an open way. Interview n°3 It could help build a relationship with the physician and the nurse. This is because initially, I think any patient or person feels they need more confidence about overexposing themselves, asking questions, or confronting issues. So maybe… yes, this questionnaire at the beginning could break the ice […]. Interview n°19
Subtheme 3: symptom management and monitoring
Patients regard ePROMs as valuable tools for the vigilant monitoring of symptoms and evolving healthcare needs. By methodically tracking fluctuations and transformations of symptoms over time, they are empowered to identify specific triggers that have a profound impact on their mental and emotional well-being: To monitor so many aspects of myself, such as emotional fluctuations over time, perception of pain, quality of life, and more […]. Interview n°3 Maybe to better identify what I have, but also to see how things are going. Interview n°12
Theme 3: exploring and addressing concerns about the use of ePROMs
This theme delves into the uncertainties raised by patients regarding adopting ePROMs, encompassing a range of issues that reflect the complexities and challenges of integrating digital tools into health management. It includes three subthemes: lack of feedback, humanization of care, and awareness of one's terminology.
Subtheme 1: lack of feedback
Patients emphasize the importance of receiving constructive feedback from healthcare professionals after completing ePROMs to collaboratively address issues. They consider regular discussions and comparisons during clinical home visits crucial for enhancing adherence to ePROMs usage. Furthermore, patients believe that such feedback ensures that they feel thoroughly understood and actively listened to: Feedback is crucial; if the clinicians don't provide any, it feels like a waste of time, leading to reluctance in filling it out again. However, with constructive feedback, the system becomes valuable, functional, and empowers us to be better heard. Interview n°12 In the end, what matters is that the answers I give here must be seen by the doctor or the nurse. They need to be seen. Interview n°16
Subtheme 2: humanization of care
The interviewers revealed concerns regarding the deployment of ePROMs within the realm of home-based palliative care. A significant concern raised was the fear that the introduction of a technology-centric data collection system could potentially reduce the level of direct human engagement with healthcare professionals. This apprehension stems from the possibility that an over-reliance on electronic data might erect an inadvertent barrier between patients and their care team, thereby impacting the traditional personal and empathetic nature of palliative care interactions: I fear that the human aspect comes a little less. I think anything mechanical is cold. Interview n°1 It depends on how the technology is managed; if there's an intention to limit the contact between doctor/nurse and patient, then I think it's harmful, that it diminishes the relationship and connection. However, if it's used in a utilitarian way with the aim of facilitating a process, a management but the doctor or my nurse, and I know they are very humane, would never let slip this precious moment of care. Interview n°19
Subtheme 3: awareness of one's terminality
Awareness of terminal illness raises doubts about the utility of ePROMs. This skepticism is rooted in the belief that if the progression of their illness cannot be halted or reversed, the act of constantly charting their health may seem futile or even burdensome. However, this awareness prompts patients to respond with heightened consciousness to ePROMs questions: Then I can express what I highlight as problems, I don't know if then they can be solved …I think then they cannot be solved. I'm throwing it out here, that is, I answer; however, I don't know if those problems can be solved, so why make them?. Interview n° 16 Of course, if I am aware I answer all the questions without problems, I accept what comes without problems. Interview n°17
Theme 4: intersecting factors influencing the efficacy of ePROMs
Despite highlighting potential facilitation factors in the use of ePROMs, participants expressed legitimate concerns about their use. In fact, there is often apprehension about reporting health results in a digital format due to their clinical condition. This theme includes five subthemes: patient functional status, knowledge and experience with the use of ePROMs, technology familiarity, compilation support and patient preferences on ePROMs.
Subtheme 1: patient functional status
Patients reported that variations in health status present significant challenges to the completion of ePROMs, citing these fluctuations’ substantial effects on their capacity to engage in daily activities. Specifically, functional impairments, including diminished visual acuity and restricted strength and coordination, are identified as key factors that hinder the ability of patients to interact with and complete ePROMs effectively: The obstacle is when the person just does not feel well when the state debilitating state is such, then access to computerization may appear more exhausting compared to paper, but only because of a physical aspect. Interview n°5 Fatigue, without a shadow of a doubt. I feel very weak, sleep little, eat even less. So, when you're feeling this bad and exhausted, you just don't have the strength. Interview n°12
Subtheme 2: knowledge and experience in the use of ePROMs
Some patients exhibit reservations toward integrating this novel technology into their everyday healthcare routines, a sentiment that can largely be attributed to their limited familiarity and hands-on experience with these advanced tools. This apprehension is further compounded by the fact that their introduction to these innovations came solely from training sessions conducted by their healthcare professionals at home:
I wouldn't know… I wouldn't know why… I've never had experience with specific questionnaires until now. There's more of a practice of using satisfaction surveys that only serve to say ‘oh, how well I was treated…’ rather than ‘I really had a bad experience.’ Interview n°9
I don't know, having lack of experience and knowledge with them and having now started to use them, I don't know if I would really do it and if they could help me in this respect. Interview n°19
Subtheme 3: technology familiarity
Despite the widespread use of technology, mastering digital tools and navigating the online world continue to be a formidable challenge for some people. This challenge emerged especially among participants who grappled with complex health issues or navigated precarious situations and who found themselves at a significant disadvantage, discouraging them from embracing digital solutions. This emphasizes the importance of ensuring technology truly facilitates healthcare without acting as an obstacle. It makes me a bit anxious, the fear of making a mistake on the tablet… of pressing something wrong. Interview n°1 No look, on the computer or tablet, I'm really bad, I'm really bad. Because given my age and everything, I'm not capable […]. Interview n°10
Subtheme 4: compilation support
Some patients view the support of clinicians and caregivers as a crucial facilitator in the adoption of ePROMs, recognizing them to play a pivotal role in helping them overcome potential challenges associated with digital tools. This suggested that the integration of technology in healthcare requires more than just user-friendly design; it necessitates a supportive human network to bridge the gap between patients and digital innovation. Yes, I would fill it in; maybe first you explain to me how it works, you know, tell me well what I have to press, when I have to fill it in and how. Interview n°19 I would have my daughter do it without a doubt […] I would have my daughter help me, I don't want to disturb anyone. My daughter is here with me; she reads the questions, and then I can answer them. But I don't use those things. Interview n° 20
Subtheme 5: patient preferences on ePROMs
Regarding ePROMs characteristics, determined by what patients tested in the training session, patients expressed a variety of preferences in terms of the length of the questionnaires, the types of questions asked, and a strong desire for the tools to be highly useful and tailored to their individual needs as much as possible. The shorter, the better. Faster and less fatigue. Interview n°2 So maybe I would prefer to fill in closed questions because maybe it is quicker, but I would leave the space for a statement in short…if someone wants to, like if someone wants to add, it's only fair that there be a possibility. Interview n°15
Discussion
In this study, we explored patients’ perspectives on integrating ePROMs into home palliative cancer care, acknowledging the known challenge of introducing them in this context.10,24 Despite facing certain challenges associated with the use of ePROMs, such as limited familiarity with the technology and their deteriorating functional state, which are also highlighted in the literature,9,24 this study revealed patients’ positive expectations regarding ePROMs implementation.
Indeed, consistent with the literature, most of the interviewed patients prefer ePROMs over paper forms.9,14 The advantages they perceive are mainly associated with the electronic format, which enables them to complete questionnaires whenever and wherever they wish to monitor their health status, bridging the physical distance with the care team, as reported for other care settings. 23
The results obtained in this study emphasize how systematic ePROMs usage can enhance to prompt availability of recorded symptom data for healthcare professionals.14,17–22 Patients believe that the use of ePROMs may improve symptom management and communication with healthcare professionals, particularly in the early stages of care when confidence in sharing concerns may be lower. This insight enables healthcare professionals to formulate early strategies for improving quality of life, personalizing care.
Patients also consider ePROMs valuable for tracking symptom progression, increasing their awareness of the disease's development over time. However, they often face uncontrollable symptoms that disrupt daily activities and hinder their ability to self-assess and complete ePROMs. Those with the worst functional status among palliative care patients had the lowest device compliance.9,24,27 Healthcare professionals, in previous studies, have also expressed similar issues about the use of ePROMs by this population due to their potential decline.24,25
In fact, in our study, some patients with irreversible conditions did not see ePROMs as a solution because their problems persisted as the disease and its symptoms inevitably progressed. The inability of 5 out of 25 individuals to engage with ePROMs due to the severity of their conditions raises questions about the accessibility and applicability of such technologies in capturing the full spectrum of patient experiences and needs during this most vulnerable phase of life. It is important to consider the perspective of some patients who see ePROMs as futile in an unstoppable terminal state.
However, the interviewed patients found ways to complete ePROMs by seeking help from healthcare professionals or caregivers. Patients delegate the task of physically completing ePROMs to them when they are unable to do so, addressing technological skill barriers and fostering their involvement.14,20,31,33
Using a tablet for data collection instead of discussing it with a clinician in person raises concerns that these data may not be discussed but rather remain stored on the device. Patients expressed the need for healthcare professionals to provide feedback on their ePROMs responses during home visits. De Jel et al., in a different care context, underscored that when healthcare professionals do not discuss ePROMs results, their significance decreases and patient skepticism increases, lowering completion rates. 32
As expressed by our sample, ePROMs help patients recall and discuss specific issues during clinical visits that might fade from memory over time. They also provide a means to address issues that might otherwise go unattended due to reluctance or time constraints during clinical visits,5,9,30 preventing potential oversights in addressing their concerns with the care team. 9 Therefore, study participants viewed ePROMs as tools capable of reordering their thoughts about their situation and fixing them; it is a way to continue trying to maintain control over themselves as much as possible.
Another barrier to patient ePROMs completion might be patients’ lack of knowledge and experience, leading to an unawareness of potential outcomes. 22 Nevertheless, patients prefer ePROMs that are easy to fill out, with a limited number of questions, aligning with their clinical condition. 13 Indeed, according to the literature, patients should play a central role in designing and implementing ePROMs systems to align these tools with the needs of those receiving home-based oncology palliative care. 44 Moreover, technological tools designed for this frail and mostly elderly population must be easy to use, bypassing technology familiarity.
A further concern expressed by patients is that improper use of ePROMs could deteriorate the human aspect of care. Human contact and proximity are “the absolute value” that people look for in healthcare professionals. They fear that technology might hinder sincere human relationships, reducing interactions to data collection on a device. Healthcare professionals-patient meetings should be considered to highlight ePROMs’ outcomes and continuous dialog is crucial to address patient skepticism and concerns about ePROMs potentially eroding the human aspect of care. EPROMs should enrich the healthcare professionals -patient relationship beyond merely standardizing home visits.
Future longitudinal studies could investigate the adherence rate to completion and the association between ePROMs monitoring and disease trajectory in home-based oncology patients, assessing whether such tools can effectively assist patients in symptom self-management, thereby impacting perceived quality of life.
Strengths and limitations
A notable strength of this study is its integration within a larger mixed-methods project and the use of a rigorous methodology and robust data collection and analysis since an integrated approach can ultimately provide more comprehensive and fundamental solutions to the addressed problems, with a greater probability of influencing professional practices. Another strength is interviewing patients in their homes, especially considering their vulnerability during this critical phase of life. Nevertheless, recruitment was restricted to a single-home palliative care setting, potentially limiting the generalizability of the findings to other healthcare settings. The aim of this study was to delve into patients’ perspectives regarding the future integration of an ePROM system in the context of palliative care at home; however, this limits knowledge about their prospects to an early stage of use. Moreover, the results might have been influenced by additional probe questions due to their specificity.
Conclusion
This study highlights the extreme frailty of home-based palliative care patients who believe that ePROMs can help monitor symptoms, enhance their quality of life and communication with healthcare professionals. EPROMs have the potential to amplify patient voices, especially regarding less explored aspects of care. In fact, patients believe that ePROMs can help keep a tangible trace in the medical records of their palliative pathway at home, allowing them to explore their thoughts and concerns beyond physical symptoms and deepening their understanding of their end-of-life condition through reflection on their own terminality. Patients expressed concern that the improper use of ePROMs could diminish the human aspect of care, valuing human contact and fearing technology may reduce interactions to mere data collection. Meetings between healthcare professionals and patients should be prioritized to discuss the answers gained by ePROMs, and maintaining ongoing dialogue is essential to tackle patient skepticism. Despite different challenges, patients view these tools as allies, offering crucial support.
Footnotes
Abbreviations
Acknowledgments
We express our profound gratitude to the patients who generously participated in this study, as well as to their families who graciously welcomed us into their homes. Our heartfelt thanks also go to the dedicated palliative home care team at INT for their support throughout this project. A special acknowledgment is extended to nurses Salvatore Benenati, Daniele Pezzera, and Gianmarco Sorace for participating with the researchers in the process of instructing patients in the use of the device and software.
Availability of data and materials
Due to a potential anonymity compromise within the full interviews, the datasets generated and analyzed during the current study are not publicly accessible.
Contributorship
All authors contributed to writing and reviewing the manuscript; LC, ML, and LP contributed to the study conception and design. IB screened and recruited the participants, explained the study's purpose, obtained written consent and introduced patients to the e-PROM prototype on a tablet. LC and ML developed the guiding questions for semistructured interviews. LC and SC conducted before collaborative then individually interviews. SC transcribed all the interviews verbatim, and the entire team critically read the transcripts. LC and DR independently coded line-by-line qualitative data. The entire research team discussed the codes and identified semantic themes; final agreement on the coding process was reached during consensus meetings with the senior researcher (ML). ML, AC, and TC commented on previous versions of the manuscript. All the authors have read, commented on, and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Dr Letteria Consolo.